
Abstract
Background
Burnout and work-related stress in health-care professionals (HCPs) is a growing concern to the optimal functioning of the health-care system. Mindfulness-based interventions may be well-suited to address burnout in HCPs.
Objective
The purpose of this study was (1) to quantitatively evaluate the effect of a mindfulness-based intervention for interdisciplinary HCPs over time and at a long-term follow-up and (2) to explore perceived benefits, facilitators, and barriers to the practice of mindfulness at the long-term follow-up.
Design
A mixed-method, repeated measures, within-subjects design was used to investigate Mindfulness for Interdisciplinary HCPs (MIHP) at baseline, post-MIHP, and a follow-up (6 months to 1.5 years after MIHP). MIHP is an 8-week, group-based course for interdisciplinary HCPs and students, with weekly meditation training, gentle yoga, and discussions on the application of mindfulness to common stressors faced by HCPs. Main outcome measures were the Maslach Burnout Inventory—Health Services Survey and the Five Facet Mindfulness Questionnaire. A semistructured interview was used to explore participants’ perceptions of sustained effects and practice in the context of HCP work at the long-term follow-up. The study protocol was registered with ClinicalTrials.gov (NCT02736292).
Results
Eighteen HCPs (88% female) participated in the study. Significant reductions were found after the intervention for 2 subscales of burnout: depersonalization, F(2, 17) = 5.98, P = .01, and emotional exhaustion, F(2, 17) = 2.64, P = .10. Three facets of dispositional mindfulness showed significant increases at long-term follow-up, act aware: F(2, 15) = 4.47, P = .03, nonjudge: F(2, 15) = 4.7, P = .03, and nonreactivity: F(2, 15) = 3.58, P = .05. Continued practice of skills long term was facilitated by the use of informal practice and perceived improvement in work and personal life.
Conclusion
In sum, MIHP improved subscales of burnout and mindfulness. These findings should be further explored with a larger, controlled study. Interventions should focus on developing mindfulness practice that can be integrated into the work of HCPs.
Keywords
Introduction
Burnout in health-care professionals (HCPs) is conceptualized as a state of emotional exhaustion, depersonalization toward patients, and impaired sense of personal accomplishment due to work-related stress. 1 Extensive research shows that burnout is related to cognitive dysfunction, 2 poor physical and mental health outcomes,3–6 and the use of more sick days. 7 Described as an epidemic in health care,8,9 burnout has increasing prevalence in HCPs and, given its negative sequelae, imparts increasing cost to the health-care system from job turnover, impaired job performance, and exacerbation of health conditions. 8 The rise in attention to burnout in HCPs was solidified in 2014 when Bodenheimer and Sinsky established the Quadruple Aim, calling for improvement of HCP burnout and work life as essential for the functioning of the health-care system overall. 10
Mindfulness-based interventions have been the focus of many recent studies investigating ways to reduce burnout and improve functioning in HCPs.11,12 Mindfulness can be defined as “nonjudgmental moment-to-moment awareness.” 13 It is important to note that definitions of mindfulness vary and are the topic of conceptual, theoretical, and empirical debate.14,15 Due to this lack of conceptual clarity in the face of a burnout epidemic, research is needed to test interventions alongside refinement of theoretical foundations within the field.
In the past 5 years, the number of pilot studies or pre-/postintervention investigations of mindfulness-based interventions for HCPs have grown substantially.16–21 Several theory papers and a recent review have been published discussing the potential for mindfulness and mindfulness-based interventions to improve HCP burnout and work, including findings that mindfulness may improve patient care and patient safety.22–27 However, the current body of literature does not define what practices and components of such interventions may be best suited for HCPs in the long term. Long-term qualitative investigations may provide a wealth of information to inform intervention development and underlying theory.
The current study investigates a newly developed intervention (Mindfulness for Interdisciplinary Health-care Professionals, MIHP), which is based on the empirically supported structure of mindfulness-based stress reduction 28 (MBSR; eg, group meetings each week for 8 weeks with introductions to a variety of mindfulness exercises) and has been tailored to the specific stressors of interdisciplinary HCPs. Preliminary pilot findings on MIHP have been published elsewhere and demonstrated significant short-term reductions in burnout, perceived stress, and anxiety. 29 Qualitative findings confirmed feasibility and acceptability of MIHP. 29 However, whether these improvements in psychological symptoms can be maintained at a long-term follow-up has not been established.
Quantitative and qualitative exploration of long-term outcomes would inform the current literature about whether MIHP and its association with reductions in burnout 29 can be maintained following the end of a mindfulness-based intervention. This may be especially important to explore given the need to develop sustainable stress management techniques in a population for whom chronic work-related stress is prevalent. This study addresses these gaps in the literature by investigating MIHP across time and at a long-term follow-up (at 6, 18, or 24 months of follow-up) along with a qualitative investigation of HCP-perceived benefits, barriers, and facilitators (eg, factors that enable) of mindfulness practice at the follow-up. We hypothesized maintained decreases in psychological distress measures (burnout, depressive symptoms, perceived stress, rumination, and state anxiety) and increases in dispositional mindfulness at the follow-up.
Methods
Participants
Participants were interdisciplinary HCPs who had completed MIHP between September 2014 and March 2016. A total of 3 cohorts completed the intervention during this time (n = 38) and were recruited for participation in this study. The first cohort was comprised of faculty and staff who completed the intervention in 2014; the following 2 cohorts were comprised of students enrolled in the intervention as course credit in 2015 and 2016. A total of 38 HCPs from the 3 cohorts were eligible to participate in the current investigation based on previous indication of willingness to be contacted for future studies. Participants who had completed the intervention, elected to participate in the previous associated study, and agreed to be contacted for future studies (total of 38 HCPs and students) were recruited via e-mail to participate in the study. The study was approved by the Virginia Commonwealth University Institutional Review Board and the protocol was registered with ClinicalTrials.gov prior to participant recruitment (NCT02736292).
Procedure
A within-subjects, repeated measures design was used to investigate the outcome of MIHP on measures of psychological functioning. In addition, all participants were asked if they would be willing to participate in a phone interview, of which 8 agreed. Qualitative data were collected using a semistructured interview to explore participants’ experiences with mindfulness in the context of HCP work and the perceived strengths and weaknesses of the intervention.
Intervention
MIHP was developed for interdisciplinary HCPs and students by the authors (P.K.: nurse scientist and nurse practitioner; S.E.B.: clinical psychology doctoral candidate; and an oral surgeon) using the evidence-based format of MBSR, review of the extant literature, and feedback from previous pilot studies. 29 The resulting intervention, MIHP, is an 8-week training with specific themes each week dedicated to applying mindfulness to the context of HCP work. Each week, MIHP met for 2 hours. The first hour was dedicated to discussion on the theme of the week and often included guest speakers from relevant health-care disciplines (see Table 1 for a list of weekly themes). The second hour was dedicated to the formal practice of mindfulness, which included hatha yoga, or gentle physical movements, mindful breathing, and relaxation, followed by a gradually increasing amount of seated meditation. The rationale for a consistent practice of hatha yoga is 2-pronged. First, there is evidence suggesting that yoga and other movement-based mindfulness practices may be especially well-suited for high-stressed populations and novices to the practice of mindfulness due to their embodied nature relative to seated meditation alone.30,31 Second, given the increasing amount of time HCPs are required to perform clerical duties (eg, note writing), the effects of hatha yoga may be especially helpful in reducing stress as a form of gentle exercise and practice of cultivating body awareness in an increasingly mind-centered environment. The seated meditation that followed the movement practice was tailored to the theme of the week (eg, loving-kindness meditation was introduced in the session titled Mindfulness in the Presence of Suffering).
MIHP Themes and Practices.

Abbreviation: HCP, health-care professional.
Measures
Burnout
The Maslach Burnout Inventory—Human Services (MBI) 1 was used to assess burnout. It is a 22-item questionnaire of burnout symptoms with 3 subscales: Depersonalization, Emotional Exhaustion, and Personal Accomplishment (reverse scored). Respondents rate items on a 7-point scale from “not at all” to “everyday.” This is the gold standard of burnout measurement in HCP samples.32–34 For HCPs, scores on the Depersonalization subscale from 7 to 12 are considered moderate and scores >13 are considered high; Emotional Exhaustion scores from 17 to 26 are considered moderate and >26 are considered high. The Personal Accomplishment subscale is often considered a distinct dimension from burnout 35 and was therefore not interpreted categorically in this study. The 3 subscales of the MBI demonstrated acceptable to excellent internal reliability (α = .75–.91).
Perceived stress
The Perceived Stress Scale (PSS-10)36,37 is a 10-item survey with a 5-point scale assessing symptoms of stress over the last month with scores ranging from “never” to “very often.” The PSS-10 demonstrated good internal reliability (α = .85) in the present sample.
Depressive symptoms
The Patient Health Questionnaire (PHQ-9) 38 was used to measure depressive symptoms. Its 9 items ask respondents to rate symptoms of depression over the last 2 weeks in frequency on a 4-point scale ranging from “not at all” to “nearly everyday.” It is well-validated and widely used. 39 The PHQ-9 demonstrated good internal reliability (α = .87) in the present sample.
State anxiety
Current levels of anxiety were measured using the State-Trait Anxiety Inventory, Form Y (STAI). 40 This investigation was only interested in state anxiety, as trait anxiety is unlikely to change in an 8-week period; 41 furthermore, research suggests that traits are frequently experienced states; therefore, changes in state anxiety may have gradual effects on changes in trait anxiety.42,43 The STAI presents 20 statements and respondents rate them based on how they feel in the present moment on a 4-point scale from “not at all” to “very much so.” The STAI demonstrated good internal reliability (α = .86) in the present sample.
Dispositional mindfulness
The Five Facet Mindfulness Questionnaire (FFMQ) 44 is a 39-item survey assessing one’s tendency to be mindful in daily living with a 6-point scale ranging from “Never, or very rarely true” to “Very often or always true.” The scale is comprised of 5 facets or subscales: Observe, Describe, Acting with Awareness, Nonjudging of Inner Experience, and Nonreactivity to Inner Experience. The 5 subscales of the FFMQ demonstrated acceptable to excellent internal reliability (α = .75–.95) in the present sample.
Study-specific questions
Respondents were asked to answer 2 forced-choice questions and 5 open-ended questions (listed in Table 2) developed specifically for this study and used to guide and inform the qualitative exploration. These questions asked respondents what mindfulness practices they continued to engage in and what barriers and facilitators existed for the continued practice of mindfulness. These questions were used to inform the subsequent qualitative interview. For example, 1 open-ended question asked participants, “What makes it easier for you to practice mindfulness and how?” A participant responded to this question with, “Being committed to seeing a drop in my anxiety level and knowing mindfulness helps that.” Therefore, during the interview with this participant, they were asked to describe how mindfulness benefited their anxiety and to recall a situation in which mindfulness mitigated their anxiety including what practices were helpful.
Open-Ended Study-Specific Questions.

Data Analytic Plan
Quantitative aims
Descriptive statistics were used to analyze the 2 forced-choice questions developed for this study. Repeated measures analysis of variance was used to test for differences across the 3 time points for all measures. Post-hoc pairwise comparisons were adjusted for using Tukey’s Honest Significant Difference test. Significance level for this pilot study was set at 0.10/SAS EG v.6.1 was used for all analyses.
Qualitative aim
Semistructured interviews were performed with open-ended questions about participants’ experience with the intervention, use of mindfulness skills in their personal and professional lives, and barriers and facilitators to practice. A descriptive, phenomenological data analysis lens was used to analyze the data.45–47 Two authors (S.E.B. and P.K.) used an iterative process to independently and collaboratively read all individual interview transcripts to get an overall sense of the data, group quotes into categories based upon similarities, re-read the data, and ultimately identify themes to examine and interpret. The themes that arose were used to construct a coherent picture of participants’ general experiences with the intervention and with barriers/facilitators to mindfulness practice.
Multiple methods to ensure rigor were implemented during the data analysis process. First, the authors independently analyzed the data to enhance dependability and consistency of findings, during the analysis process. Second, documentation about decisions regarding themes was maintained in order to ensure confirmability of findings. Third, an intervention participant who expressed interest in continued engagement with the research activities and a colleague unrelated to the study reviewed the data and confirmed themes, in order to enhance credibility of findings.
Results
Sample
The respondents consisted of 18 interdisciplinary HCPs and trainees (see Figure 1 for study flow). This represents a 53% response rate. Most participants were nursing students (n = 6; see Table 3 for a complete demographic breakdown). Participants were predominantly white (n = 13, 81%) and female (n = 14, 88%).
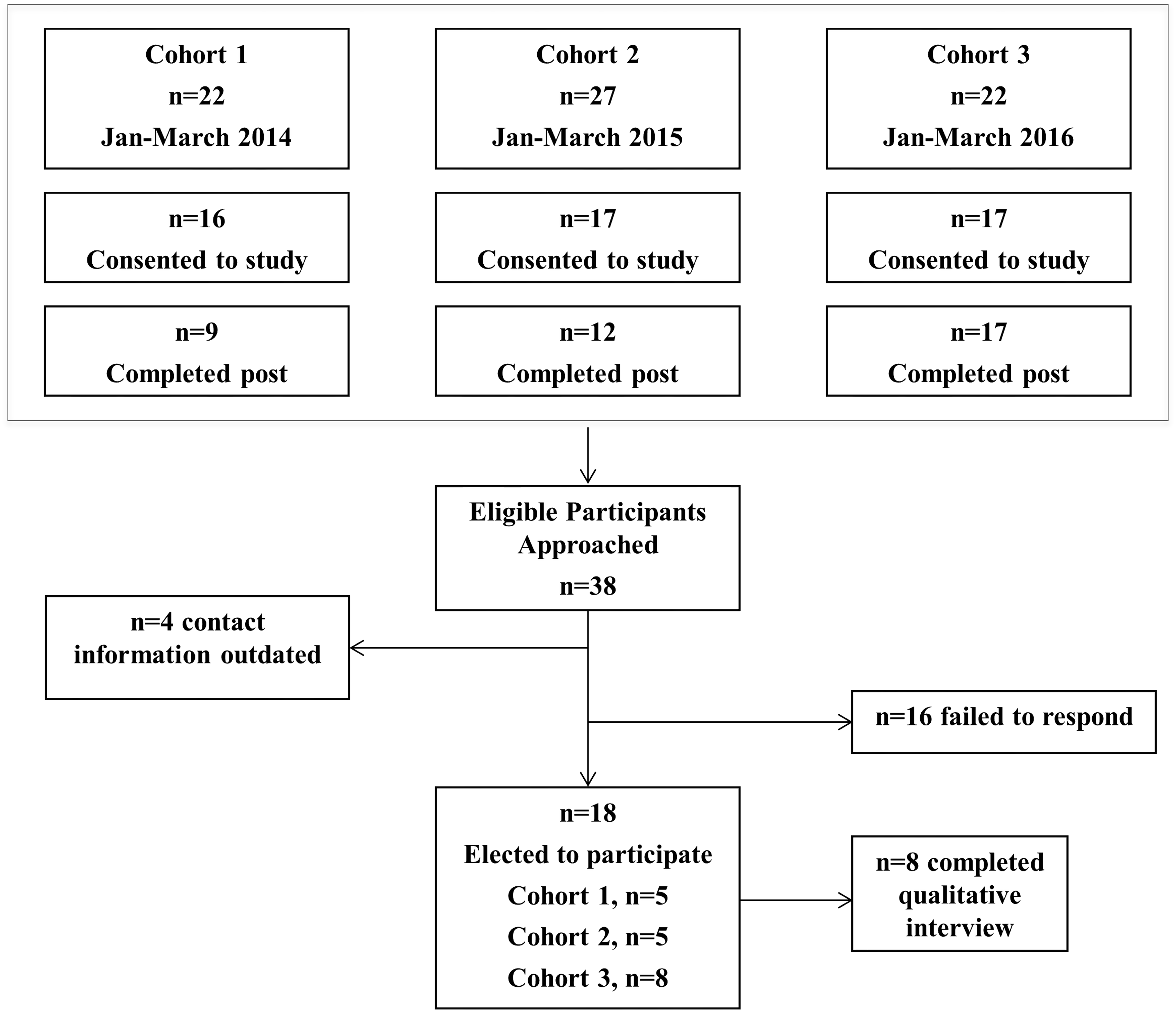
Study Flow Diagram.
Participant Demographics.

Abbreviation: SD, standard deviation.
Two participants did not respond to demographics.
Quantitative Findings
Significant changes across the 3 evaluations were found for several measures. For burnout, there were significant changes in depersonalization (P = .01) and emotional exhaustion (P = .10; Table 4). Specifically, there was a significant reduction in depersonalization from baseline to postintervention (average difference: 3.08; standard error [SE] = 1.05; Tukey’s adjusted P = .02) and baseline to follow-up (average difference: 4.36; SE = 1.38; Tukey’s adjusted P = .02) For emotional exhaustion, there was a significant reduction from baseline to follow-up (average difference: 7.21; SE = 3.14; Tukey’s adjusted P = .08) and a nonsignificant reduction from baseline to postintervention (average difference: 4.23; SE = 2.49; Tukey’s adjusted P = .23). Pairwise comparisons for measures that demonstrated significant changes are given in Table 4.
Comparison of Measures Across Time.

Abbreviations: FFMQ, Five Facet Mindfulness Questionnaire; M, mean; MBI, Maslach Burnout Inventory; PHQ-9, Patient Health Questionnaire—9 item; PSS, Perceived Stress Scale; STAI, State Trait Anxiety Inventory; SE, standard error. Items noted with different letters are significantly different (Tukey’s adjusted P < .10).
P value from repeated measures analysis for difference across 3 time points.
On the FFMQ, there were significant improvements on 3 of the 5 subscales: acting with awareness (P = .03), nonjudging (P = .03), and nonreactivity (P = .05). On the acting with awareness subscale, there was a significant improvement from baseline to postintervention (average difference = 2.38; SE = 1.02; Tukey’s adjusted P = .08), and a further reduction, though not significantly different, at follow-up (average difference = 3.75; SE = 1.51; Tukey’s adjusted P = .65). On the nonjudging and nonreactivity subscales, there were significant improvements from baseline to postintervention (Tukey’s adjusted P = .03 and P = .06, respectively), these improvements were maintained at the follow-up relative to baseline. For nonjudging, the average difference from baseline to post-intervention was 3.39 (SE = 1.15) and for nonreactivity, improvement of 4.66 (SE = 1.84).
The PSS, PHQ-9, RRS, and STAI showed trends towards improvement but were not statistically significant (see Table 4).
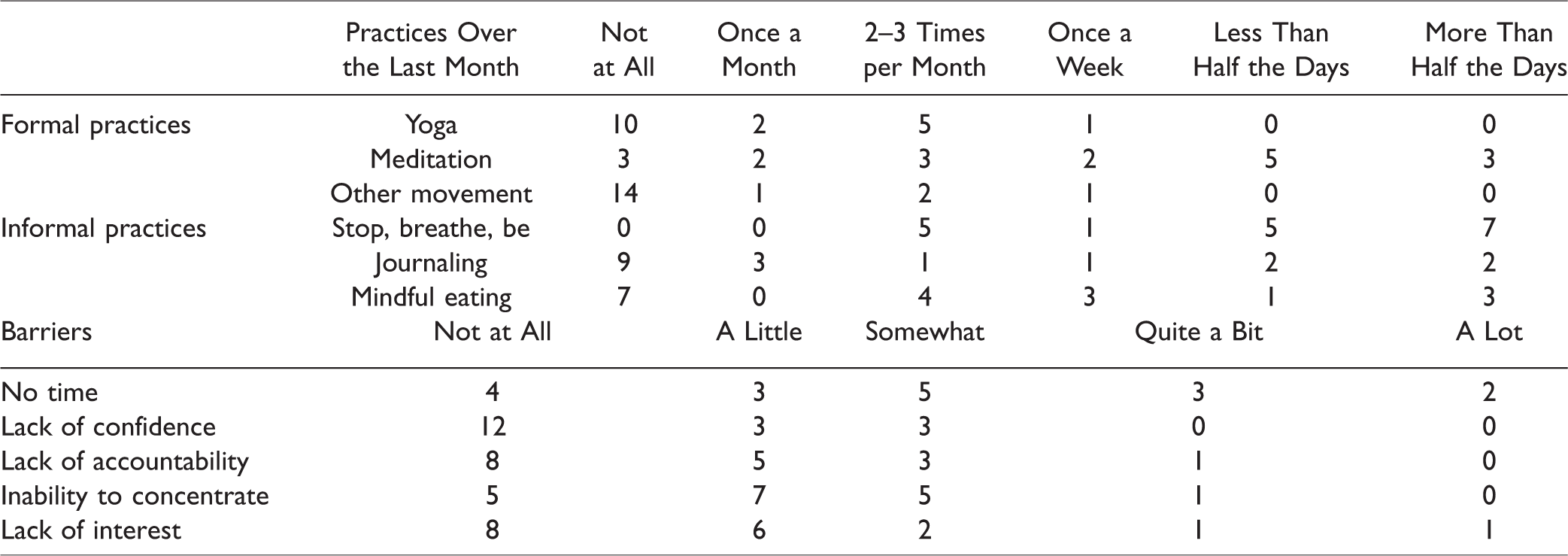
Participants were asked to rate the frequency with which they engaged in informal and formal mindfulness practices over the last month. All participants had practiced an informal practice called “stop, breath, be” (n = 18). Most participants (n = 10) had not practiced yoga in the last month. Eight participants reported practicing meditation more than once a week over the last month. Meditation and “stop, breathe, be” were the most frequently endorsed practices (see Table 5). “No time” and “inability to concentrate” were the highest rated barriers to practice. Most participants (n = 12) denied “lack of confidence” as a barrier to mindfulness practice (see Table 5).
Frequency of Practices and Barriers to Practice at Follow-up.
Qualitative Findings
The following 3 themes arose during the interviews with participants: (1) Personal Integration; (2) Importance of Informal Practices; and (3) Mindfulness Fosters Connection with Self, Others, and Patients.
Theme 1—Personal integration
The theme of “personal integration” arose frequently, in which participants reported the importance of integrating mindful practice into one’s personal life, before it could be a focus in one’s professional life. The concept of “integration” was described with varying language among participants. For some, successful integration meant that one uses mindful practices regularly, whether formal or informal, that is, “to just make it part of the day” and to be “aware that there are other choices in how you can handle stress and life . . . you have a variety of tools.” For others, the concept of integration meant to live mindfully irrespective of the specific formal/informal practices, for example, “staying in the present moment . . . as a way of life.” Equating the experience to muscle memory, participants repeatedly suggested that there was a positive feedback loop, whereby regular mindfulness practice creates “a positive effect—makes me realize that I need to keep doing this more.” Small integrated practices would inform participants’ general experiences: “be patient but just start making small little shifts [that] can add up to huge, huge benefit,” hence, they would experience larger integration into living mindfully.
The theme of personal integration also underlay discussions of self-care. Several participants noted that, since taking the course, they had become aware of the benefits of self-care and that having self-awareness through a regular integrated mindfulness practice is a key component of that self-care. One stated that “to have self-love . . . is very important and I do that through self-awareness.” Participants reported that integration of mindfulness into daily life allows one to pay attention to reactions to stress and act with acceptance and recognition of difficult thoughts and feelings. Often participants suggested that “just learning to be quiet” and “a sense of acceptance and being present in the moment” were a key component of the personally integrated mindfulness. For some participants, having a crisis situation became a tipping point to realize the importance of living mindfully. One participant with a cancer diagnosis said “tremendous adversity was actually helpful in really integrating mindfulness because . . . you really need to change your perspective or else you’re going under.” She continued to underscore the relevance of integrating mindfulness in one’s persona: My whole pattern used to be, as soon as I would get stressed I would go sit in the “dumpster”—be negative and just “oh everything’s horrible.” Now I start laughing, realizing you can get out of the “dumpster” at any time you want, you don’t have to sit in there. I think slowly over the past year I’ve been able to kind of really get that at my core and kind of understand yeah I’m the only one that can take away my joy, I can stop doing that.
Theme 2—Importance of informal practices
In order to obtain a sense of integration (theme 1), participants consistently described the importance of informal mindfulness practices to do so, whereas formal meditative practices were not cited to be as relevant. Examples of informal practices that were most consistently used included “Stop-Breathe-Be,” meditation while walking, and gratitude exercises. For example, one participant stated “my most consistent mindfulness practice is every time I hit fresh air. The minute I step outside, and feel the sun on my face, or feel the breeze, I try to come to the present moment.” Several participants suggested that informal practices done in conjunction with regular occurrences during daily life facilitated integration. Participants suggested the class helped them realize that “micro-practices, as opposed to sitting down for a long time and doing a meditation” could allow a “reset button,” particularly during stressful times. “‘Stop, breathe, and be’—that’s just so easy, you can do it anywhere, nobody knows that you’re doing it.” Participants reporting using these informal practices in the “moment to respond rather than react” and also to start the day in a calming way: “I will try in the morning when I get up to just stop and be grateful for everything that I can think of.” Several participants commented that the course provided insight that “a little goes a long way” and were pleased they learned how to integrate mindfulness when they previously perceived to be too busy. Another participant commented that stress, anxiety, and “lack of clarity [are] a signal where I know I need to take a step back, take a breath, focus on the moment, and then move on and tackle things,” reflecting the common sentiment that participants developed reminders for using informal practices.
Many participants expressed gratitude for and interest in more formal practices, such as seated meditation, yoga, and tai chi, but they expressed difficulty with incorporating those into their daily lives. Instead, participants repeatedly stated that informal practices provided a tool to interrupt a stressor in a realistic, less time-intensive way: “I’m in lab and have a huge long to-do list, I can’t just bust out my yoga mat and meditate for an hour . . . so the ‘Stop, Breathe, Be’ has been great because it is a shorter amount of time.” Participants provided positive feedback about the course formatting which allowed participants to experiment with different types of formal and informal mindfulness practices, as described by one participant: “what works for one person doesn’t work for another, so you have to find what works for you and what fits into your life . . . by doing that homework each week you could really experiment with that.”
Theme 3—Mindfulness fosters connections with self, with friends/family/colleagues, and with patients
A theme of “connection” was pervasive in participants’ discussion about mindfulness and participants seemed to categorize the connection into 3 areas: connection with self, connection with friends/family/colleagues, and connection with patients. With regards to connection to self, several participants gained a shift in perspective about self-awareness, self-care, and staying true to one’s needs. These shifts in perspectives provided a sense of great benefit with regards to compassion towards self. For example, one participant reflected that “before the course, I was way less kind to myself.” Another participant suggested that she was able to recognize how much energy she spends focusing on work or family that she started to prioritize mindful breaks and alone-time in the car to “use it for reflection and re-energizing.” Several participants mentioned feeling hardwired to solve others’ problems prior to taking care of self, given their chosen profession, but that the course helped them re-prioritize self-care and be “more open-minded with ourselves” in order to ultimately have a healthier relationship with others.
With regards to connection to friends, family, and colleagues, participants reflected that mindfulness allowed enhanced stress management with positive benefits for their personal and professional relationships. A participant stated that “my relationships with my family have gotten much better” and that the class had helped her clarify “what I’m feeling from what other people are feeling.” This clarification of one’s own thoughts and feelings was echoed by several participants who suggested they had learned not to take on the stress and reactivity of a family member or colleague because “that’s not my stress, that’s their stress.” By standing in one’s own experience, participants suggested they were better able to be calm and compassionate in difficult situations.
With regards to life as a health-care provider and connections with patients, the majority of participants stated their personal mindfulness practice would likely benefit their patients because they would be more open and available to patients’ needs even in stressful situations: “Practicing mindfulness, I think it helps me from becoming super stressed in clinic with patients and to be in the moment and really focus on the patients.” Further, participants identified the role of mindfulness in reducing risk of errors: “Mindfulness is, I think, a necessary thing, because you do really have to slow down at certain points and tell yourself to not work on autopilot, because you could potentially make a mistake and not realize it.” Several participants reflected that HCPs can use mindfulness to enhance true presence with their patients, as summarized by one participant: “I’ve always believed that the essence of healthcare is being present with people and meeting them where they are, and mindfulness really helps me with that.” This core value of “being present” with patients was repeated by many participants who also stated that the stress and strain of the health-care environment can often get in the way of true presence, causing decreased empathy and increased burnout. Participants perceived a mutual benefit between themselves and their patients in the use of mindfulness, as summarized by one participant: Mindfulness has direct and indirect benefits: it’s indirect in that it helps us become more kind to ourselves, which improves our care for others. It directly affects the way that we handle stress and the way that we interact with those around us, whether they be patients or coworkers, and [helps us] display more empathy.
In addition, many participants expressed pleasure at learning skills that could be taught to their patients. For example, one participant stated: “my goal for this [class] was to find healthful ways to deal with my own anxieties, and to translate that to the psychiatric patients that I work with.” Another participant reflected upon the importance of personal mindfulness practice before teaching it to patients: “if I’m gonna be able to talk the talk, I need to walk to walk.”
Discussion
The current study used mixed-method design to investigate the long-term effects of MIHP, a newly developed mindfulness-based intervention tailored to the specific stressors of HCP work and delivered in an interprofessional classroom setting. Results support the continued investigation of MIHP and demonstrated reductions in 2 domains of burnout as well as increases in dispositional mindfulness at the follow-up. In addition, it identified some characteristics of MIHP that supported long-term usefulness to participants.
The quantitative results revealed baseline levels of burnout in the moderate range on the Depersonalization and Emotional Exhaustion subscales; notably, after MIHP and at the follow-up, scores were in the low range for both subscales. These findings suggest meaningful reductions in burnout following MIHP for a group of HCPs with moderate burnout at baseline that were maintained 6- to 18 months later. State anxiety saw mean decreases post-MIHP and at the follow-up; however, these were not significant. There were virtually no changes in depressive symptoms, perceived stress, and rumination. This could be due to a floor effect (low scores on these measures at baseline) or that MIHP is especially suited for addressing symptoms of burnout rather than depressive symptoms (including rumination) and perceived stress, which may be more short-lived than burnout. Future research should continue to investigate the effect of MIHP on various psychological constructs to better understand its effects.
Several themes emerged from the qualitative exploration that helps to define how a successful intervention might be structured. Participants acknowledged the utility of classroom training for introducing techniques. However, developing mindfulness as a habit long-term required integration of mindfulness practice in their daily lives. Notably, most of the participants did not endorse lack of confidence in practicing mindfulness as a barrier to continued practice at the follow-up, suggesting that—following MIHP—participants felt confident in their ability to practice mindfulness; however, most respondents noted insufficient time as a significant barrier. Participants also reported improved self-awareness. Several benefits to HCP work were also reported, including reduced “auto-pilot” and enhanced patient care. MIHP may also increase interprofessional collaboration and a shared understanding of how to approach HCP work.
Taken together, the quantitative and qualitative data demonstrate reduced work-related stress by way of integrating mindfulness into their lives, using informal practices, and fostering connections with self and others. Participants reported on the importance of integrating mindfulness into their daily lives, which aligned with significant increases in dispositional mindfulness, or the tendency to be mindful in one’s day-to-day, that were maintained at the follow-up. Informal practices were highly regarded and contributed to participants’ sense of integration. Future work could investigate informal mindfulness as a mediator of reduced burnout using ecological momentary assessment. The theme of improved relationships with self, close others, and patients could also be a mechanism by which burnout was reduced. Although the current study did not explicitly explore mechanisms, the qualitative data suggest that participants experienced enhanced relationships, which may have contributed to the significant reductions in burnout. Future research could investigate as a mechanism using measures of HCP self-efficacy, interprofessional teamwork, or patient-centered care.
Based on this mixed-methods investigation, future iterations of MIHP, as well as other interprofessional mindfulness interventions, several recommendations can be made. First, given the high reported use of informal practices, future interventions should emphasize informal practice, especially in the work setting. It is suggested that participants be introduced to a new informal practice at each session to increase participant’s access to work-relevant tools. Second, given that few participants continued practicing formal meditation/yoga, and some reported difficulty integrating formal practice into their lives, it is suggested that more time be spent encouraging formal mindfulness practice. For example, developing methods for addressing challenges to practicing, like forgetting, by setting reminders; identifying individual values that mindfulness practice may support; and developing SMART goals for behavior change. It is also recommended that participants be encouraged and supported in developing peer-led mindfulness groups following the intervention and that booster sessions be offered when possible. Finally, to investigate the participant-perceived mechanism of without informal practices, a 2-armed trial of MIHP with and without informal practices on similar outcomes of psychological functioning may be important to determine mechanisms of change and advance theory.
Based on participants’ perceived changes in patient-centered care and work functioning as a result of MIHP, several recommendations are made for measure selection in future investigations. First, studies could include validated measures of patient-care domains, examples include the patient-rated Rochester Communication Rating Scale 48 and the third-party Roter Interaction Analysis System49,50 for coding patient–provider interactions. Two studies provide initial evidence in support of the association between HCP mindfulness and patient-centered care; however, more research is needed to draw conclusions.51,52 Also, participants reported reduced reliance on automatic pilot and improved organization/planning of work priorities; these perceived benefits could be initially measured in future studies using cognitive assessments of inhibition and task switching (eg, cognitive tasks like Trail Making Test A & B or Stroop Color/Word). One study found that a mindfulness intervention for psychology students improved Color/Word performance, 53 and future research should build upon these findings. If improvements were found on these measures following MIHP, it may have bearing on HCP work-relevant functioning in the measured domains, and future studies could investigate their correlation with clinical errors or near misses.
The quantitative findings demonstrated significant and sustained reductions in burnout and increases in mindfulness at the follow-up; these findings must be qualified as preliminary. The lack of comparison group and convenience sample limits the interpretability of the findings. Differences between students and faculty/staff cannot be investigated due to low power. Furthermore, social desirability bias may be limiting to this project, as the intervention was author-led. The low response rate also limits strong conclusions from being drawn. Finally, the length of this intervention may limit generalizability to hospital settings; therefore, future studies could investigate abbreviated versions of this intervention. These findings should be used to inform future intervention development and measure selection in randomized controlled trials with participant and patient outcomes.
In conclusion, MIHP showed promise as an interdisciplinary intervention for improving burnout and dispositional mindfulness in HCPs and students. The findings here encourage future program evaluation. Participants reported on the importance of integrating mindfulness into their lives using informal practices and noted the positive effects of mindfulness on their relationships with themselves, others, and patients. MIHP may be a promising intervention to improve work-relevant functioning in HCPs, and future research should investigate this hypothesis.
Footnotes
Acknowledgments
The authors would like to say a special thank you to Andrew Harris for his work on this project. The authors would also like to thank Dr George Deeb for his initial help in the development of this intervention. Finally, the authors thank all the participants for their willingness to be mindful.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.