
Abstract
This qualitative study explores perspectives of community health workers (CHWs) on family functioning among Sri Lankan Tamil refugees in India. Focus groups with 18 CHWs explored the impact of transmigration stress on family dynamics and the mitigating role of CHWs. Thematic analysis revealed three themes: parenting/family practices, services for addressing family conflicts and challenges, and solutions to enhance family well-being. Findings highlight the importance of culturally responsive interventions, increased access to counselling services and building trust. This study contributes to limited research on psychosocial experiences of refugees during transmigration and emphasises targeted support to promote family functioning and overall well-being.
Introduction
In the aftermath of the Sri Lankan Civil War (1983–2009), the Tamil population was compelled into a journey of survival and displacement. Historically, this has resulted in over 300,000 Tamil refugees being dispersed across approximately 100 camps in Tamil Nadu, India, and beyond (George, 2010). This exodus, characterised by more than just physical relocation, has led to profound psychosocial upheaval for the refugees (George & Jettner, 2016). Refugees face a complex array of challenges, including statelessness (Majewski, 2021), acculturative stress (Berry, 2008) and the struggle to adjust in a prolonged state of displacement (George, 2017; Kuttikat & Jettner, 2015). This study explores the multifaceted impact of transmigrational stress on family functioning within the Tamil refugee community in India, with a particular focus on the crucial role of health workers in mitigating these challenges.
The case of Tamil refugees represents the global refugee reality. The United Nations High Commissioner for Refugees (UNHCR) revealed in 2023 that an estimated 29.4 million refugees worldwide are living in similar protracted states of displacement, paralleling the experiences of the Tamil refugees (UN High Commissioner for Refugees [UNHCR], 2023). With India housing the largest concentration of Sri Lankan refugees—over 125,000 individuals—an in-depth exploration of their challenges, particularly through the lens of health workers’ roles in these camps, becomes critical (de Silva, 2007). This study not only focuses on the immediate needs of Tamil refugees in India but also offers a valuable framework for understanding the role of refugee health workers in the global migration context. The reality of Tamil refugees and the contribution by the health workers add to a global conversation for those working with refugees living in low-resourced host countries, while highlighting the role of qualitative research in informing the creation of pragmatic policies that address the needs of both global refugees and health workers.
The impact of the Tamil refugee displacement has been particularly profound on the familial structures and mental health of these refugees (Kuttikat & Jettner, 2015). Parental roles and responsibilities have undergone significant transformations due to the weight of transmigration stress, as highlighted by De Vries (2001). The term ‘transmigrational stress’ in migration studies is interpreted diversely, encompassing psychological, social and cultural difficulties encountered by individuals adapting to different societal structures during transit (Betancourt et al., 2015; Brun, 2001); the cumulative and interconnected nature of stress throughout the migratory journey (Beiser et al., 2011), including pre-migration and post-arrival challenges (Kuttikat et al., 2018); and the unique vulnerabilities of irregular migrants due to legal status issues, such as risk of deportation and limited resource access (Betancourt et al., 2015; Yusoff et al., 2018). This article adopts George’s focus on familial structures and the negotiation of strain as a mediator of familial mental health (George & Jettner, 2016; Kuttikat & Jettner, 2015).
Transmigrational Stress and Family Functioning
In refugee camps, where trauma symptom levels are typically higher than those among resettled refugees, the effects of migration are compounded by the loss of material resources, diminished coping mechanisms and limited access to healthcare and other social resources (Maneesh et al., 2021). The trauma associated with forced migration profoundly impacts family dynamics, notably by diminishing parental emotional and mental capacities. This decrease directly influences the relationship between transmigration stress and mental health outcomes, affecting both parents and their children (Betancourt et al., 2015). Such challenges are exacerbated in environments where refugees often face severe and complex health needs due to inadequate financial and material support. This scenario not only strains individual mental health but also disrupts the fabric of family functioning, particularly in the context of prolonged displacement in refugee camps.
The forced displacement and resettlement experiences during and after the civil war have posed challenges to Tamil families, affecting their ability to adapt to new environments. Challenges include navigating different cultural norms, overcoming language barriers and finding employment. Additionally, the trauma of war and migration has impacted familial bonds, often leading to changes in parenting styles and family dynamics. One study evidenced synchronous acculturation processes, transmigrational PTSD and stress of daily life in refugee camps, all of which have profound impacts on family dynamics (Hazer & Gredebäck, 2023). These factors, alongside differences in family structure and roles, challenges in adaptation, acculturation stress and intergenerational conflict, are cited as specific strains impacting refugee mental health and family well-being (Kuttikat & Jettner, 2015). Research has shown that family well-being can be improved with increased parent support and lower levels of parent–child conflicts (Taraban & Shaw, 2018). Health workers play a crucial role in activating resource management and allocation, supporting parents and minimising parent–child strain.
The Role of Health Workers and the Importance of Family Functioning
Transmigrational stress has led to altered family dynamics and increased mental health challenges within the refugee community (George, 2012). Amidst these challenges, health workers in refugee camps have emerged as a critical element of support and care (Ehiri et al., 2014).
Refugee camp health workers are trained, professional workers who offer social support and link camp refugees to services, such as materials and resources for social welfare, family support and counselling, as well as legal resources pertaining to migration status and governmental records (Miller et al., 2020; Perry et al., 2014; Scott et al., 2018). Their role extends beyond providing medical assistance; they are a crucial link to resources and psychosocial support (Maneesh et al., 2021). Often being refugees themselves, these health workers are uniquely positioned to provide culturally responsive care. Health workers play a pivotal role in addressing the community’s unique challenges, supporting both the resettlement process and the adaptation to new realities (Miller et al., 2020; Somasundaram & Sivayokan, 2013).
While the nature of forced migration results in the deterioration of many psychosocial factors and resources—such as loss of material resources, coping and mental health—preliminary research has identified family functioning as being especially impacted. Health workers in refugee camps, often refugees themselves, are crucial in providing culturally responsive peer support (Maneesh et al., 2021). They link camp refugees to essential services, offering support for social welfare, family support, counselling and legal assistance (Miller et al., 2020; Perry et al., 2014; Scott et al., 2018).
Health workers emerge as pivotal figures in mitigating daily challenges, offering resources to enhance family functioning, supporting overall well-being (El-Khani et al., 2018; Maneesh et al., 2021) and offering social support services (Miller et al., 2020; Perry et al., 2014; Scott et al., 2018). Access to healthcare and other social resources inside refugee camps is immensely limited as a result of the lack of financial and material resources available to camp refugees, especially given that 85% of the world’s refugee population is hosted in lower-middle income countries (UNHCR, 2023). The lack of resources presents challenges for camp refugees who often have serious and complex health needs (Maneesh et al., 2021). These unique needs have led to a variety of innovations to promote health and psychosocial well-being inside refugee camps, including the use of health workers as resource allocators and cultural support that is clinical in nature (Perry et al., 2014).
Compared to resettled or internally displaced refugees, refugees undergoing the transmigration process experience commonality with resettled populations as well as unique sets of stressors, specifically statelessness and uncertainties regarding resettlement or repatriation (Frounfelker et al., 2020; Radhakrishnan et al., 2022; Yusoff et al., 2018). The trauma associated with forced migration results in decreased parental emotional and mental capacities (Eruyar et al., 2018) and mediates the relationship between transmigration stress and mental health outcomes for parents and, consequently, their children. Additionally, levels of family functioning have been linked to the development of various mental health symptomatology in children (George & Jettner, 2016).
For those who are parents during this process, these problems become especially pronounced, as parenting capacities become impeded (Bloch, 2018). Studies conducted on Syrian refugee populations have underscored the need for parenting resources in refugee camps (El-Khani et al., 2018). In particular, El-Khani et al. (2016) have identified three themes in this area: parental desire for parenting guidance and support seeking, perceived barriers to support and the value of discussing parenting issues.
Refugee camp health workers are trained, professional workers who offer social support and link camp refugees to services, such as materials and resources for social welfare, family support and counselling, as well as legal resources pertaining to migration status and governmental records (Miller et al., 2020; Perry et al., 2014; Scott et al., 2018). Health workers are better positioned to provide culturally responsive peer support (Maneesh et al., 2021). While the nature of forced migration results in the deterioration of many psychosocial factors and resources—such as loss of material resources, coping and mental health—preliminary research has identified family functioning as being especially impacted.
Health workers in refugee camps, often refugees themselves, are crucial in providing culturally responsive peer support (Maneesh et al., 2021). They link camp refugees to essential services, offering support for social welfare, family support, counselling and legal assistance (Miller et al., 2020; Perry et al., 2014; Scott et al., 2018). Health workers emerge as pivotal figures in mitigating daily challenges, offering resources to enhance family functioning, supporting overall well-being (El-Khani et al., 2018; Maneesh et al., 2021) and offering social support services (Miller et al., 2020; Perry et al., 2014; Scott et al., 2018). Access to healthcare and other social resources inside refugee camps is immensely limited (Maneesh et al., 2021). These barriers are a result of the lack of financial and material resources available to camp refugees, especially given that 85% of the world’s refugee population is hosted in developing countries (UNHCR, 2023). The lack of resources presents challenges for camp refugees who often have serious and complex health needs (Maneesh et al., 2021). These unique needs have led to a variety of innovations to promote health and psychosocial well-being inside refugee camps, including the use of health workers (Perry et al., 2014).
With much of the literature focused on pre- and post-migration contexts, very little is known about the psychosocial circumstances of those refugees in the transmigration phase. This knowledge gap may be a result of the limited access researchers have to refugee camps, thus hindering the understanding of the interventions needed (Maneesh et al., 2021). Still, the literature on refugee resettlement highlights the importance of interventions targeted at all levels of migration. Interventions during the transmigration phase have been shown to contribute to later, successful resettlement (Murray et al., 2010). Community health workers (CHWs) represent a vital parenting resource for a population experiencing pronounced impediments to parental capacities and susceptibility to experiencing deteriorated family functioning (El-Khani et al., 2018). Given the protracted nature of the displacement Sri Lankan refugees face, as well as the unique stressors inherent in this phase of migration, research should examine the relationship between transmigration stress and family functioning. Health workers offer unique and worthwhile perspectives, as their positionality as peer refugees offers a proximity to the psychosocial challenges and family conflict that camp refugees face.
Current Study
While existing research has examined CHWs’ effectiveness in improving access to healthcare across these settings, few studies have focused specifically on their own perspectives during the unique phase of transmigration, where families face many uncertainties, stressors and restricted resources that profoundly shape parenting, family roles and mental health. This study investigates the interplay between transmigration stress, family dynamics and the role of health workers in alleviating the adverse effects of trauma among Tamil refugees. By delving into the specific experiences and challenges faced by Tamil refugees in India, this research seeks to contribute significantly to the broader discourse on global migration crises. Due to the limited knowledge about health worker refugees in refugee camps, the primary objective of this qualitative research is to explore the perspectives of CHWs on family functioning among Sri Lankan Tamil refugees living in refugee camps in India. Specifically, we examine the impact of transmigration stress on family dynamics and the crucial role played by health workers in mitigating these challenges. By centring the voices of CHWs, this study addresses a critical gap in the literature, supporting our understanding of how frontline workers embedded within refugee camps perceive and respond to the psychosocial challenges of transmigration, and how these insights can inform more sustainable, family-centred interventions.
Methods
Setting and Participants
Our focus is qualitative and exploratory, using data collected in a larger overarching project that utilised both quantitative and qualitative methods to gather data with families from the Trichy refugee camp in Tamil Nadu, India. The original study recruited CHWs as participants via purposive sampling in March 2018. Participation was restricted to individuals in the camp who (a) worked as CHWs and (b) were Sri Lankan Tamil refugees. Two members of the research team conducted two focus groups (N = 18). Table 1 presents the descriptive characteristics of the participants. The average age of participants was approximately 45 years, and a majority (61%) identified as female. The average years of experience working as CHWs was 11 years, with the majority identifying their role as social/welfare workers or counsellors.
Participant Demographics.
Procedures
All methods were approved by the principal investigator’s university’s Institutional Review Board. The research team partnered with staff from the community board to conduct the study within the refugee camp. The community board was established as part of a larger research project and comprises the Organization of Eelam Refugee Rehabilitation (OfERR)—the local and largest non-profit agency serving the refugee camp—and several identified community elders. The two focus groups were conducted in Tamil with the CHWs. Each focus group was audio-recorded and then transcribed and translated into English. Each participant was compensated ₹500 for their participation.
Data Analysis
Two members of the research team conducted an inductive thematic analysis within Microsoft Excel following Braun and Clarke’s (2006, 2023) phases of thematic analysis. Excel was used to both organise and code data. Conducting the analysis with these guidelines allowed for methodological rigour and validity. Two coders were used in every step of analysis for increased interpretation of transcripts and to decrease bias. Following data transcription, two coders read through the transcript data to assess initial thoughts. Both coders independently coded the transcripts and then compared coding schemes, discussing and resolving differences until consensus was achieved. The research team held iterative meetings to refine the codes and then themes to ensure that they were coherent, internally consistent and distinct from each other. As themes were developed and excerpts were coded, the team met to discuss any differences or questions that came up, resolving them through each step of the analysis process. Themes were then checked against the full data set to confirm that they accurately represented participants’ accounts and responses to interview questions. Representative participant quotes were selected to illustrate each theme. These steps enhanced the trustworthiness and credibility of the findings.
Results
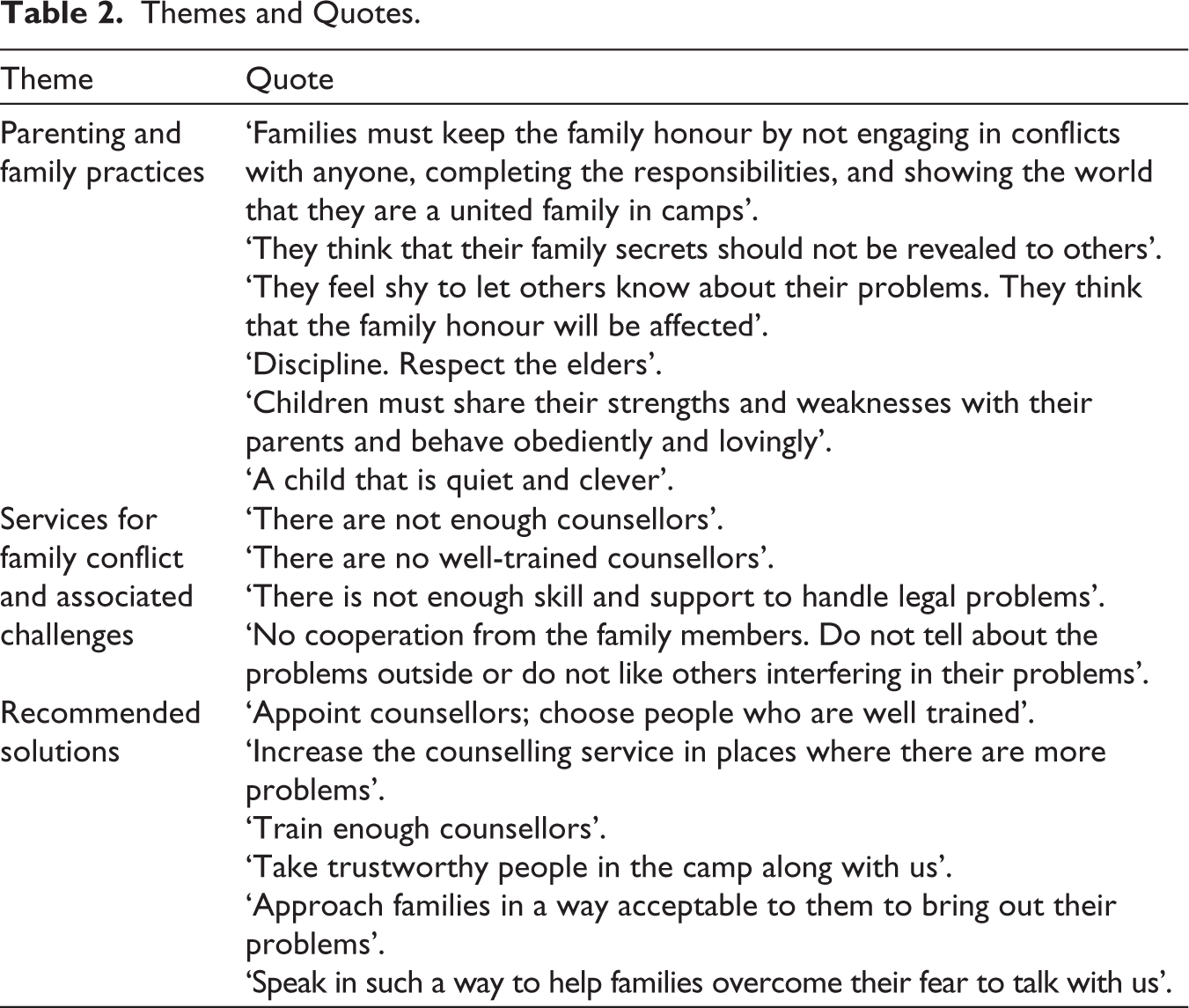
Three central themes emerged from our qualitative analysis: (a) parenting and family practices, (b) services for family conflict and challenges associated with services and (c) reducing the challenges. Table 2 presents important quotes by theme.
Themes and Quotes.
Theme 1: Parenting and Family Practices
Participants described several parenting and family practices related to the upbringing of children in the camp.
Characteristics of a ‘Good’ Family and ‘Good Children’
At the beginning of the interview, participants were asked to recount their perception of a good family and a good child. All participants highlighted that working hard, raising good children, helping people in need and respecting the elders are essential qualities of a good family. One participant stated, ‘A family that brings up the children well, practices good habits, moves well with other people, is hospitable and honest, helps others and the poor is a good family’. Data analysis revealed that honouring the family is a critical characteristic of a good family. Furthermore, most participants stated that not talking about the family problems with others is a way to honour the family. One participant indicated that engaging in conflicts weakens family honour, so they try to avoid conflicts with each other by demonstrating to others that they are united. Participants were also asked to elaborate on their perceptions of what being a good child means. Several participants stated that a studious child who always does the right things, fulfils parents’ desires and keeps parents safe is considered a good child. For example, one participants stated, ‘a child who does not create any problem at home through his behaviours’ which was similarly reflected by 14 additional participants.
Strict Rules/Discipline
Discipline and how parents interact with children’s behaviours were another sub-theme of the focus group interviews. Participants indicated that children must strictly obey the instructions of elders, parents and teachers. For instance, one participant shared: ‘Kids must obey the parents, obey the teachers’.
The data received from the participants revealed that most children obey and respect the rules. However, children born in the refugee camp are less receptive to the rules than children born in Sri Lanka. Participants indicated: ‘80% of the children born in Sri Lanka feel that these rules are right. Some of the children born in India (30%) cannot accept this because of the culture here’. One participant indicated, ‘children who are born in Sri Lanka are brought up with patriotism and respect for the family discipline. Children who are born here mingle with the outside society for studies, and we need to correct some of their habits’.
Participants also affirmed that children who do not accept the rules feel controlled: ‘They feel that they are controlled very much. They feel that they are not allowed to be free’. Data showed that children who accept and obey the rules do so because they believe those rules are good for them: one participant stated, ‘children brought up in the Sri Lankan culture realise that the parents make decisions for their good future only’.
Gender Roles
Data from the camp refugees brought to light that there are fewer gender differences in the household roles of Sri Lankan families than in Indian families; one health worker participant shared,
Comparing to the situation in India; the following things have improved in Sri Lanka: contribution of men in bringing up the children is more, gender differences between men and women is less, decision making by women in the house is more, more freedom to express our thoughts.
However, data also revealed that Sri Lankan Tamil refugee families still preserve patriarchal structures since domestic work is a woman’s task. ‘Husbands help women and wives in their household work’.
Theme 2: Services for Family Conflict, Challenges Associated with Services
All participants affirmed that the primary services available to refugees to support their family conflicts are self-help groups, Women Inclusive Network group, counsellors, religious priests, police and government officers. The data received from the participants revealed that the availability of counsellors and lack of appropriate counsellor training are fundamental challenges associated with the services offered to families in the refugee camp, oftentimes with there not being a sufficient number of trained and skilled counsellors to support the needs of the community.
Data analysis also revealed that families’ unwillingness to talk to counsellors is a crucial challenge associated with the Trichy refugee camp services. Data also show that families’ reluctance to talk to counsellors is related to Sri Lankan Tamil’s culture-specific practice of not talking to others about family problems. ‘There is no cooperation from the family. They think that their family honour will be affected’; ‘Families hide the problems’.Focus group interviews also led to discussions surrounding the need for solutions to resolve the family and service challenges the refugee camp was experiencing. Many participants highlighted that appointing more counsellors and training them is crucial to overcoming the main challenges associated with services available to refugees to support their family conflicts. Furthermore, most health worker participants affirmed that another possible strategy to reduce these challenges is building trust with families to feel more comfortable talking to counsellors about their family problems. Participants indicated that with an increased trust in the health professionals and counsellors in the community, families and individuals would be more willing and open to discussing the challenges they were experiencing. For example, one participant stated, ‘Approach families in a way acceptable to them to bring out their problems’.
Theme 3: Potential Solutions to These Challenges
The third theme that arose from focus group interviews was the need for solutions to resolve the family and service challenges the refugee camp was experiencing. Many participants highlighted that appointing more counsellors and training them is crucial to overcoming the main challenges associated with services available to refugees to support their family conflicts. Furthermore, most health worker participants affirmed that another possible strategy to reduce these challenges is building trust with families to feel more comfortable talking to counsellors about their family problems. Participants indicated that with an increased trust in the health professionals and counsellors in the community, families and individuals would be more willing and open to discussing the challenges they were experiencing. For example, one participant stated, ‘Approach families in a way acceptable to them to bring out their problems’.
Discussion and Implications
This qualitative study aimed to understand the role of health workers in these refugee camps, illuminating how they work to support the mental health and family functioning of their own Tamil refugee community. This is a critical study in the area because of its approach to exploring refugee health worker experiences working in their own community and being an integral component of interventions. In collective refugee communities, the aspect of being a known and trusted member is crucial for the role’s effectiveness. It directly influences the credibility and acceptability of these individuals within the community (Kuttikat et al., 2018). This principle is acknowledged by both the community-based participatory research team and the health workers themselves. As community members, these health workers are not just participants but are also empowered as key agents in delivering the intervention. Their unique position, rooted in their community identity, enables them to navigate cultural nuances and establish a deeper connection, thereby enhancing the intervention’s effectiveness.
Analysis of focus groups with refugee health workers highlighted how familial and gendered roles and challenges with engaging in family-based or counselling services impacted families.
Authoritarian Parenting Styles and Health Workers
The data analysis emphasised that Sri Lankan Tamil camp refugees follow an authoritarian parenting style that focuses on obedience and discipline. Sri Lankan Tamil camp refugees enforced an ‘authoritarian’ parenting style to ensure suitable family environments. Cultural expectations and practices expect children to be submissively compliant, obedient and quiet. This enforcement may create (or creates?) family conflicts since children, exposed to other cultures and norms, may now perceive this as being controlled by the elders, parents and teachers. Consequently, they feel they do not have the freedom to spend time with their friends and develop social skills. This sentiment is especially true among children born in the refugee camp because they are more familiar with the Indian culture than children born in Sri Lanka. These results align with Renzaho and Vignjevic’s (2011) findings that suggest that migrant parents from countries with collectivist cultures, such as Africa, maintain their cultural beliefs that good children are those who submit to parental authority, forgoing the notion that children can be. Consequently, parents do not allow children to be independent. The authors also found that this cultural parenting practice is one of the most difficult to change, making it one of the most significant long-term challenges immigrant parents and children face when negotiating and adapting to the norms of a new camp or the new host country’s cultural norms.
The importance of the role of health workers emerges from behind the statement ‘most participants stated that not talking about the family problems with others is a way to honour the family’. Authoritarian parenting style is predicated on the notion that familial issues remain within the family system, with the implication being that people do not talk about their family publicly or to strangers. The role of the health worker emerges as a bridge builder between self-help group services, counsellors and families. In settings where this is available, participation is increased when health workers are empowered to act as cultural mediators. In addition, health workers can provide flexibility by providing individualised services at the family level, which may be more appropriate, and a way to improve communication both between counsellor familial dyads and within familial relationships.
Patriarchal Hierarchy and Health Workers
Family practices in the camp preserve their patriarchal system; therefore, women’s role in the family is relegated to family care and domestic chores, while men are the household economic providers. Moreover, women working outside the home might experience work/life imbalance since the privileged position of a father may preclude him from fully engaging with the family’s menial work.
Women’s issues and gender roles are primarily discussed in the women’s inclusive network programme; therefore, men are not part of this conversation. Research about domestic violence suggests that women’s empowerment may increase domestic violence against women when the patriarchal structures are deeply rooted, and men are not involved in the programmes (Hughes et al., 2015). Consequently, it is crucial to increase the focus on men and women in the Trychi refugee camp programmes, which aim to reduce women’s and men’s power imbalance at home.
Limitations
The current study is not without its limitations. The limited sample size of 18 health workers makes it difficult to generalise these findings. Additionally, Trichy is one of approximately 123 refugee camps, and each has different experiences with health workers and the services available to their community. Because the health workers were refugees themselves and were serving their own communities, biased responses could be another important barrier to consider. Lastly, the study asked the health workers about family dynamics, though youth and parents were not a part of this specific portion of the overall research study. Engaging with the larger community to understand their experiences with family functioning and engaging with family and counselling services could provide additional enriching, contextual information.
Implications
Health workers highlighted two key areas influencing access to care for Sri Lankan Tamil refugees: authoritarian parenting styles and patriarchal hierarchies. The analysis revealed the importance of health workers in bridging entrenched cultural norms and increasing participation in medical and mental health services. The implications of this study reveal a need for increased appointments of health workers, continuing training needed in particular on legal recourse in the area of partner violence, as well as resource allocation and parenting support.
Implications of this study extend to the training, support and sustainability of refugee health workers. Beyond expanding their numbers, investment is needed in capacity-building, particularly training in trauma-informed services, culturally responsive parenting interventions and legal advocacy. As refugees themselves, health workers face unique risks of burnout and vicarious trauma, making peer support and access to their own mental health counselling critical for their effectiveness and sustainability. Policymakers and humanitarian organisations should work to integrate health workers into camp health infrastructures due to their cultural expertise and the trust they are able to build within their own communities. Finally, interventions should work to prioritise trust-building by engaging with both men and women in their communities and positioning health workers as vital mediators to support family conflict.
Footnotes
Acknowledgements
Thank you to Dr Irudaya Rajan for mentorship to Dr Miriam Kuttikat while conducting this study in refugee camps. The authors would like to acknowledge health workers in the Sri Lankan Tamil refugee camps in India for their participation in the study of Sri Lankan Tamil refugees living in refugee camps in India.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute of Health Fogarty International Center grant number K01 TW009648.