
Abstract
This study explores the relationships between resource utilisation, transmigration stressors, physical and mental health problems, and family dysfunction of Sri Lankan Tamil camp refugees during their transmigration period. The study aims to (a) describe the types of stressors experienced by Sri Lankan Tamil refugees, and their levels of adjustment and family functioning; (b) conduct a preliminary assessment of associations between parental daily stressors, mental well-being and family functioning; and (c) analyse the extent to which refugees rely on formal and informal resources and their impact on adjustment and family functioning. A quantitative longitudinal study was conducted over 4 years with a systematic random sample of 120 camp refugee parents. Statistical analyses examined the effects of transmigration stress on mental well-being and family functioning. Findings from Phase I indicated significant associations between transmigration stress and somatic complaints, depressive symptoms, hostility and family functioning. Improved family functioning was reported in Phase II, which could be attributed to a reduction in overall transmigration stress. Refugees who accessed informal support from friends in Phase I reported better family functioning, and those using formal support from non-governmental organisations and informal support from families showed improved family functioning in Phase II. Our findings underscore the importance of emphasising transmigration stressors in understanding health outcomes, family dynamics and resource utilisation among transmigratory refugees.
Keywords
Introduction
The United Nations High Commissioner for Refugees (UNHCR) reports that there are currently over 108.4 million people experiencing forced displacement globally, with 35.3 million of them categorised as externally displaced refugees. Forcibly displaced persons often undergo an intense migration journey, marked by exposure to physical and psychological traumatic experiences. Chronic exposure to such stressors has been shown to heavily impact the long-term health of refugees, particularly within the unstable ecologies that are common among displaced populations (Bhui et al., 2003; Kulandai, 2021; Silove et al., 1998).
Refugees displaced in camp settings are among the most vulnerable category of refugees due to factors such as their prolonged displacement, uncertain legal status, lack of proper documentation, forced encampment, chronic discrimination, and poverty and criminalisation within unfavourable socio-legal conditions (Amrutkar, 2012; De Vries, 2001; Rogers et al., 1998; Weaver, 2016). UNHCR reports that a significant proportion of camp refugees consist of children who have either migrated to the camps alongside their parents or were born in displacement (Lustig et al., 2004). Prior research indicates an association among forced displacement, adverse family dynamics and parenting capabilities (Al-Simadi & Atoum, 2000; Herath, 2012; Morantz et al., 2012; Somasundaram, 2010; Steel et al., 2006). Resource utilisation has been previously documented to alleviate the negative mental health outcomes associated with deteriorated family functioning (Fadhlia, 2023; George et al., 2016; Siriwardhana & Wickramage, 2014; Sahoo et al., 2024). However, despite these findings, there exists a noticeable gap in the literature regarding the role of resource access in mitigating the adverse effects of transmigration stress experienced by camp refugees, presenting a barrier to the development and implementation of effective mental health interventions within camp settings.
In this study, transmigration refers to the process of forced displacement and the experiences of refugees during their stay in refugee camps, which often involve multiple stages of migration (Al-Baldawi, 2002; Kirmayer et al., 2011). This term encompasses the various stressors and challenges faced by refugees during their time in camps, such as poor living conditions, limited access to resources and future uncertainties (Morantz et al., 2012; Silove et al., 2017). The concept of transmigration is distinct from the pre-migration phase, which involves the events and experiences that lead to forced displacement, and the post-migration phase, which refers to the resettlement and integration process in a new country (Bhugra et al., 2011).
Background on Sri Lankan Refugees in India
Beginning in 1983, the civil conflict in Sri Lanka led to the involuntary displacement of approximately 150,000 Tamils. A majority of these refugees sought refuge in neighbouring India (Acharya, 2007; Jayawardena, 2020; Shastri, 1999; UNHCR, 2021). This mass exodus was driven by both long-standing ethnic tensions and through violent outbreaks, which were rooted in the marginalisation and discrimination of the Tamil population (Bahu, 2019; Bentz & Goreau-Ponceaud, 2020; Jayawardena, 2020; Kulandai, 2021). This conflict was exacerbated by the anti-Tamil pogroms of 1983, which is commonly known as Black July. This was a fundamental factor that forced many Tamils to flee their homeland (de Silva, 2001, 2010; Kanagaratnam et al., 2020; Kuttikat et al., 2018).
Tamil refugees arrived in India in three distinct waves: 1983–1987, 1990–1995 and 1995–2002 (Acharaya, 2007; Bradimore & Bauder, 2011; Brun, 2003; Jayawardena, 2020; Shastri, 1999). Upon arrival, refugees were placed in government-run camps, primarily located in the state of Tamil Nadu (Kulandai, 2021). These camps provided basic amenities but were often characterised by overcrowding, poor living conditions and limited access to essential resources (George, 2013; Kulandai, 2021). The abrupt nature of their displacement, coupled with their lack of resources, categorised them as ‘acute refugees’ (Kunz, 1973, 1981), underscoring their heightened vulnerability to various social and economic challenges (George, 2013; Jayawardena, 2020).
Specific Stressors Faced by Sri Lankan Tamil Refugees in Indian Camps
Sri Lankan Tamil refugees in Indian camps face a multitude of stressors that significantly impact their mental health and family functioning (Hans, 1993). These stressors are interconnected and often compound one another, creating a complex web of challenges for refugees to navigate. One of the most immediate and persistent stressors is unstable housing (Krishna & Howard, 2022). As Kulandai (2021) notes, the camps are frequently overcrowded, with living conditions that fall far short of adequate. Refugees often report a lack of privacy, poor sanitation and insufficient space for families (Krishna & Howard, 2022). These conditions not only contribute to physical discomfort but also create a constant source of psychological stress.
The adaptation to refugee camp life generally follows three phases: pre migration, transmigration and post migration, each presenting distinct stressors (George & Jettner, 2015a,b; Kirmayer et al., 2011). Transmigrational stressors occur during the displacement in refugee camps and are amplified by unstable housing resources, family conflicts and economic stressors (Affleck et al., 2022; Bahu, 2019; Byrow et al., 2022; Krishna & Howard, 2022; Minihan et al., 2018). These stressors intersect with the Tamil refugees’ historical disenfranchisement in primary industries, adding a unique layer of socio-historical stress to Tamil families in India (Bradimore & Bauder, 2011; George, 2015).
Post migration, Tamil refugees in India have continued to experience the adverse effects of statelessness, discrimination and limited access to education, healthcare and employment opportunities (Kulandai, 2021; Samuel et al., 2018). India’s non-ratification of the United Nation’s 1951 Refugee Convention as well as the omission of having a national refugee policy have also contributed to the challenging situation of Tamil refugees in India (George, 2013; Jayawardena, 2020; Shastri, 1999). Due to these facts, understanding how refugee resource utilisation within camps in alleviating transmigration stress is crucial for implementing effective mental health interventions as well as improving the well-being of refugee families (Fadhlia, 2023; George, 2017). This research provides insights into the challenges of Sri Lankan Tamil migrants (Kulandai, 2021), underscoring the importance of continuous research to understand the evolving nature of refugee experiences and the impact of migration policies on their lives.
Current Study
Given the dearth of information about the adjustment of Sri Lankan Tamil refugees in Indian camps (Kuttikat et al., 2018), this research team implemented a large mixed-method longitudinal study that aims to inform future evidence-based intervention development to significantly improve the dynamics of refugee families. Using a sample of Sri Lankan camp refugees displaced in the Trichy refugee camp in India, the purpose of this study was (a) to comprehensively characterise the stressors encountered by the refugees, assessing their levels of adjustment and family functioning; (b) to conduct preliminary assessment of associations between parental daily stressors, mental well-being and family functioning; and (c) to assess the extent of refugees’ utilisation of formal and informal resources while simultaneously evaluating their levels of adjustment and family functioning. Given the literature substantiating the impact of migration stress on individual and family well-being (Byrow et al., 2022; De Vries, 2001; Minihan et al., 2018; Siriwardhana et al., 2013; Somasundaram, 2010, 2013; Steel et al., 2006), it is crucial to investigate similar trends among Sri Lankan refugees and eventually inform implementation of potential interventions to mitigate these associations.
Materials and Methods
Setting
The principal investigator (PI) has been engaged in research at the Trichy refugee camp since 2008. The study was overseen by a collaborative board comprising refugees, service workers, staff from the Organisation for Eelam Refugee Rehabilitation (OfERR) and community elders. This board also played a crucial role in guiding the current study, working in partnership with OfERR at the refugee camps in Trichy, India. The entire research spanned four years, with recruitment and data collection occurring over three years, specifically from June 2014 to April 2015 (Phase 1) and from June 2016 to April 2017 (Phase 2). The investigation adhered to the latest guidelines of the Declaration of Helsinki. The study design underwent ethical review by an appropriate committee, and informed consent was obtained from all participants after thoroughly explaining the study procedures.
Sampling
At the time of data collection, the Trichy refugee camp had 1,500 families with approximately 4,500 individuals. The researcher conducted the study with a random sample of 120 parents. The research team presented critical information, such as study details, criteria for participation and the voluntary nature of the study during Sri Lankan refugee community events organised by OfERR. A systematic random sampling method was used to select a representative sample of 40 families from each subdivision. A random number between 1 and 1,500 was generated to determine the initial starting point, after which every eighth house was selected. This approach yielded a total of 120 families, each consisting of children and parents residing together, who were willing to participate in the study. Study participation was limited to Sri Lankan Tamil refugee families in which parents lived with their adolescent children.
Data Collection
The PI, along with a team of 12 locally trained female healthcare workers, conducted the initial screening and provided an overview of the study to those expressing interest. Each participant received an information letter about the study in either Tamil or English, depending on their language preference. Following this, the researchers contacted those selected for the study to schedule a convenient time for the participant to sign the consent form, which had been translated into Tamil, and to attend a face-to-face interview. During the screening process, the researchers ensured that all refugee parents were willingly participating in the study. The team thoroughly explained the study’s purpose and the methods of data collection to all participants, securing informed consent before proceeding.
To complement the informed consent process, the mental and cognitive status of participants was evaluated using the MINI Mental Health exam. The PI had established prior connections with the refugee families by leading earlier studies and frequently visiting the Trichy camp through OfERR community events, which helped foster trust and rapport. Additionally, the research team underwent training in linguistic and social communication techniques to effectively interact with the families. By spending time with families outside of the formal data collection process, the research team was able to create a more comfortable and engaging environment, enhancing the families’ willingness to participate when data collection began.
The interviews were held at the OfERR office, chosen for its convenient location near the study participants. To maintain privacy, each parent was interviewed separately, with the research team ensuring their comfort throughout the process. In keeping with cultural norms, an elderly woman was present during interviews with male participants to provide a sense of security. At the conclusion of each interview, a debriefing session was conducted, during which participants had the opportunity to ask any follow-up questions before receiving a compensation of $50 (₹2,500). Phase II of the data collection occurred approximately two years later, during which the research team used contact information from Phase I to reach out to potential participants. Of the 120 initial participants, 96 took part in Phase II, following the same procedures as in the first phase. Participant attrition was attributed to the natural movement of refugees between camps, driven by factors such as family reunification, rehousing or changes related to employment, healthcare or other family dynamics.
Measurements
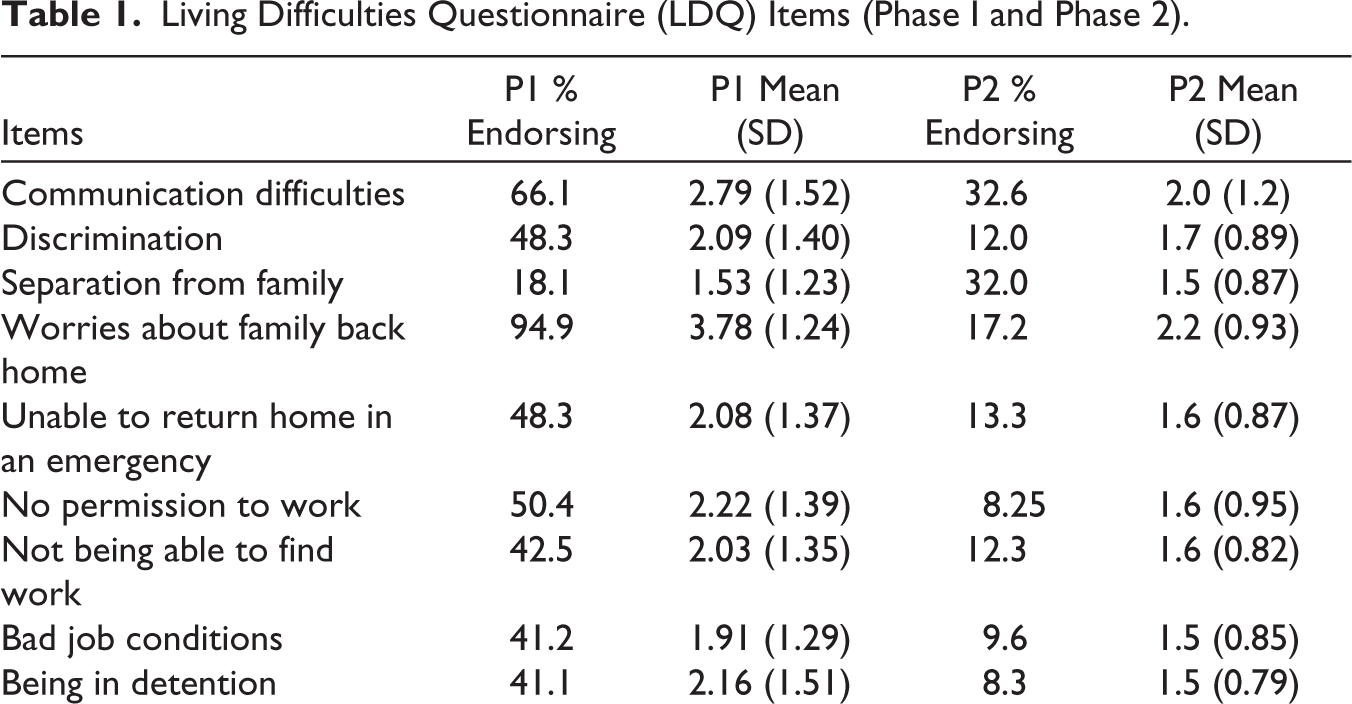
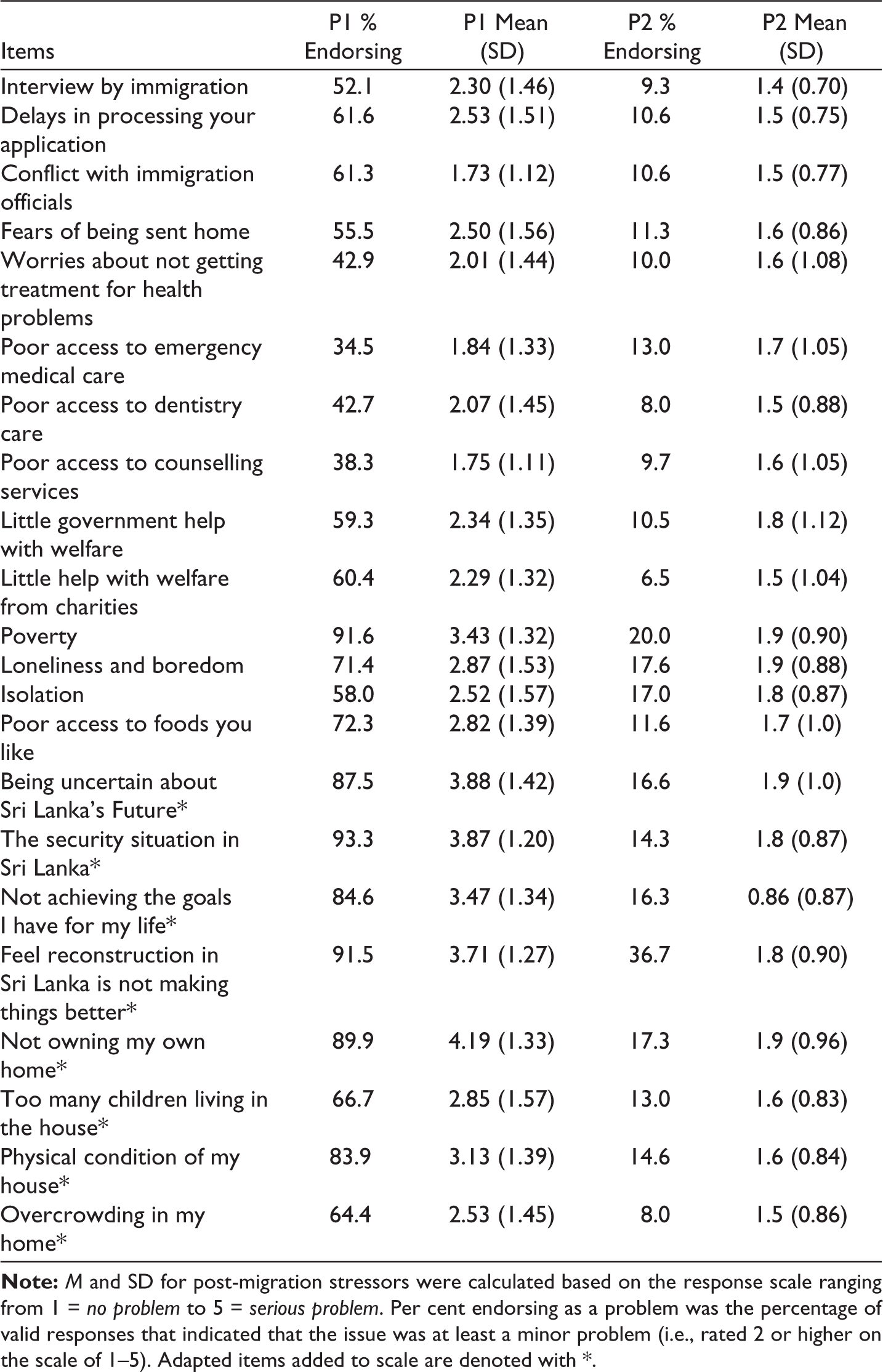
Transmigration stressors: Transmigration stressors were assessed utilising the Post-Migration Living Difficulties Questionnaire (LDQ; Silove et al., 1998). The LDQ, a self-report tool, evaluates recent adverse experiences commonly associated with migration (Sengoelge et al., 2022). This questionnaire has been effectively used in prior studies to assess transmigration and post-migration stressors in diverse refugee populations, including Tamils (Sengoelge et al., 2022). The current research team also successfully used this tool in previous research (George & Jettner, 2015a,b).
Originally comprising 24 items, the LDQ asks respondents to indicate the extent to which they are troubled by various living difficulties, utilising a 5-point scale ranging from ‘no problem at all’ to ‘a very serious problem’. In collaboration with the Tamil Community Collaborative Board (TCCB), an additional eight items were incorporated into the original scale (Kuttikat et al., 2022), resulting in a 32-item scale. This revised scale was translated into Tamil, and content comparability was ascertained through blind back-translation procedures. The revised scale, presented in Table 1, gauged the total transmigration stressor score. Internal consistency in Phase 1 was good (α = .814) and in Phase 2 was excellent (α = .990).
Sleeping difficulty: Participants’ sleep difficulties were evaluated using the Pittsburgh Sleep Quality Index (Buysse et al., 1989). Refugee participants rated their experiences over the past two weeks on a 5-point Likert scale, ranging from 0 (daily) to 4 (never), across 10 items. The scores were reversed and then totalled, with higher scores reflecting greater sleep difficulties. The internal consistency of the measure was deemed acceptable at Phase 1 (α =.796) and excellent at Phase 2 (α =.907).
Somatic complaints: The Somatization Subscale of the Brief Symptoms Inventory (BSI), a 90-item measure that evaluates current psychological symptoms of distress (Derogatis & Melisaratos, 1983) was used to measure somatic complaints. This subscale is made up of seven items on a 5-point Likert scale ranging from 1 (not at all) to 5 (extremely). Refugees rated how often they experienced each item in the last seven days. Items were summed for a total score, with higher scores indicating higher levels of somatic complaints. Reliability was good at both Phase I (α = .817) and Phase II (α = .896).
Depressive symptoms: Another subscale of the BSI (Derogatis & Melisaratos, 1983), the Depression Subscale, was used to measure the depressive symptoms. Using six items on a 5-point Likert scale ranging from 1 (not at all) to 5 (extremely) in the last seven days, refugees’ depression were assessed by summing these items with higher scores, indicating higher levels of depressive symptoms. Reliability was good at both Phase I (α = .824) and Phase II (α = .809).
Hostility: Hostility was measured using the third subscale of the BSI Hostility Subscale (Derogatis & Melisaratos, 1983), which includes five items on a 5-point Likert scale ranging from 1 (not at all) to 5 (extremely) assessed in the last seven days. The five items were summed together, with higher scores indicating higher levels of hostility. Reliability was acceptable at Phase 1 (α =.662) and acceptable at Phase 2 (α =.773).
Family functioning: Family functioning was evaluated using the Self-Report Family Inventory (SFI; Beavers et al., 1985, 2000). The SFI includes 17 items, where participants rate how accurately each item describes their family on a scale from 1 (yes, describes our family well) to 5 (no, does not describe our family well). The scores from all items were summed to obtain a total score, with higher totals indicating poorer family functioning. The internal consistency of the SFI was solid in both phases, with Cronbach’s alpha being 0.784 at Phase 1 and 0.780 at Phase 2.
Resource utilisation: Resource utilisation was evaluated through a series of structured interviews focused on both formal and informal family support mechanisms. Participants were prompted to identify significant individuals who provided support, detailing their location, relationship to the participant, institutional ties, the nature of the support offered, how accessible the support was and how often it was utilised.
Data Analysis
Demographics
The participants provided information about their age, sex, marital and employment statuses, education level and family composition. Phase I data collection included 120 parents. Parents were primarily female (96%) and married (83%) with an average age of 38 years. Thirty-eight per cent of parents also reported being employed during Phase I of the study. Every parent mentioned having children, with each household averaging about three children. Nearly 89% indicated that they departed Sri Lanka in 1990 and subsequently resided in a refugee camp for approximately 22 years. Additionally, 98 parents, or 82%, shared that they were currently living with their extended family, including members from three generations: grandparents, parents and children.
During the Phase II data collection, few of the Phase I participants moved to different camp locations; therefore, only 96 parents out of the original 120 parents participated in Phase II. Parents were primarily female (97%) and married (85%) with an average age of 40 years. Forty per cent of parents also reported being employed during Phase II of the study, and 95 parents reported that they lived with their family that included three generations: grandparents, parents and children.
Quantitative Analysis
In this exploratory analysis, we present descriptive information on all variables, followed by univariate reports of associations of both transmigration stressors (using correlations) and resources (using t-tests) with physical health, mental health and family functioning at Phase I. Comparisons of health outcomes and family functioning were also done after controlling for resource utilisation. Finally, we examine associations among post-migration stressors, health outcomes and family functioning at Phases I and II (using paired t-tests). Once again, a comparative analysis of the associations was made across different resource utilisation groups with the goal of exploring how these correlations evolve across both phases and various resource types.
Results
Results from Phase I Data Collection
As shown in Table 1, two-thirds of the 32 potential transmigration stressors were rated by more than half of this refugee sample as being at least ‘a little’ stressful. Worries about family (94.9%), poverty (91.6%), loneliness and boredom (71.4%), being uncertain (87.5%), feeling like reconstruction in Sri Lanka is not making things better (91.5%), the security situation in Sri Lanka (93.3%) and not owning my own home (89.8%) were most commonly noted as stressors within the sample. The use of available resources varied widely at Phase I, with nearly the entire sample (97%) using formal resources provided by both governmental and non-governmental organisations (NGOs). Around 76.7% of the total sample use informal family support, and 33.6% use informal support from friends.
Living Difficulties Questionnaire (LDQ) Items (Phase I and Phase 2)
We also look at correlations between parents’ transmigration stressors and their mental well-being and family functioning. With the exception of sleep quality (r = .11, P = .22), the total transmigration stressor score was significantly associated with various health outcomes and with family functioning: somatic complaints (r = .38, P < .001), symptoms of depression (r = .47, P < .001), hostility (r = .47, P < .001) and family functioning (r = –.24, P = .004). While the refugees with higher transmigration scores reported higher somatic complaints, depressive symptoms and hostility, they also reported overall better family functioning. Differences in the measure of family functioning were seen across groups based on the utilisation of informal support from friends and family. Refugees who utilised informal support from friends experienced stronger family dynamics than those who did not utilise these informal social resources. (Mused friend = 51.39, SD = 13.58; Mdid not use friend = 56.13, SD = 11.79). Conversely, refugees who received support from their families reported experiencing poorer family functioning than those who did not rely on such resources (Mused family = 56.48, SD = 11.76; Mdid not use family = 48.53, SD = 13.31). Similar analyses were not conducted for formal support because almost all refugees had access to some forms of formal governmental support in Phase I.
Comparison Between Phase I and Phase II
In this section, we compare transmigration stressor scores, health outcomes and family functioning between Phase I and Phase II using paired t-tests. The mean transmigration score from Phase II data was 22.09 (SD = 15.01). Also, the mean transmigration score in Phase II is significantly lower than that in Phase I, indicating that the overall migration stressors had reduced from Phase I to Phase II. No significant differences were found in Phase II sleep difficulties, somatic complaints, depressive symptoms and hostility compared to Phase I; however, there was a significant drop in family functioning showing improved family functioning in Phase II as compared to Phase I (MPhase I = 54.49, SD = 12.29; MPhase II = 49.89, SD = 10.16). This can be attributed to the lowering of the overall transmigration score from Phase I to Phase II.
Comparisons of health outcomes and family functioning by resource utilisation between the two phases were also done using paired t-tests. No notable changes in somatic complaints, depressive symptoms and hostilities were seen among refugees who used the different formal and informal supports in Phases I and II. However, refugees who did not use support from formal NGOs reported lower levels of depressive symptoms in Phase II than Phase I (MPhase I = 5.22, SD = 13.58; MPhase II = 6.0, SD = 5.25). Refugees who used formal support from NGOs and informal support from families reported significantly lower family functioning scores in Phase II than Phase I, indicating better family functioning (MfNGO, Phase I = 54.95, SD = 12.2; MfNGO, Phase II = 49.72, SD = 10.32; MFamily, Phase I = 54.92, SD = 12.21; MFamily, Phase II = 51.29, SD = 9.80). Refugees who did not use these supports had no significant change in family functioning between the phases.
Discussion
Our findings are situated within a broader socio-political context that significantly influences the lives of refugees. A critical aspect of this context is India’s non-ratification of the 1951 Refugee Convention, which leaves Tamil refugees without formal recognition and protection. This legal limbo exacerbates their vulnerabilities and limits their access to essential services, including healthcare, education and employment opportunities. The absence of a national refugee policy means that refugees rely heavily on the support of NGOs and informal networks, which, while beneficial, are not sufficient to meet all their needs.
While our study does not aim to comment on specific domestic policies, our findings have implications for global approaches to refugee support. The challenges faced by Sri Lankan Tamil refugees in Indian camps highlight the need for comprehensive legal and policy frameworks that support refugee integration and well-being. Such frameworks, if implemented, could serve as models for other nations dealing with refugee populations, ideally facilitating better access to resources and services and improving the overall well-being of refugees.
Our research contributes to the global body of evidence that policy advocates can draw upon when addressing refugee issues worldwide. By emphasising the importance of addressing ongoing transmigration stressors and supporting both formal and informal support networks, our findings can inform more effective and holistic approaches to refugee support on a global scale.
The transmigration stressors such as worries about family, loneliness, poverty and being uncertain are identified as prominent stressors in refugee camps and are significantly associated with various health outcomes and family functioning. Unsurprisingly, our study revealed elevated levels of migration-related stressors—family, poverty, an uncertain future in refugee camps, not owning a home—among Sri Lankan Tamil refugees residing in Indian camps. This can be attributed to the fact that a significant portion of Sri Lankan Tamil refugees fall into the ‘acute’ refugee category, having fled their home country with little to no resources at a moment’s notice (George, 2010; Kunz, 1973, 1981). For instance, a study conducted by Silove et al. (2017) found that 85% of refugees escaping from war-affected regions were compelled to abandon their homes within a window ranging from just two days to as little as two hours prior to their departure. Given the intensity of migration-related trauma, its psychological effects and the lack of preparedness for protracted displacement, forcibly displaced refugees require a robust network of resources and global attention. Providing essential resources may help ease the challenges of forced displacement of these refugees and mitigate the difficulties of both their mental health and family functioning.
We should emphasise that nearly the entire sample reported resource utilisation from NGOs such as OfERR (100%), Jesuit Refugee Services (JRS) (94.2%) and governmental support (100%). About 53.3% of NGO resources are from OfERR and 46.7% are from JRS. OfERR focuses primarily on providing transmigration stress support and less on family counselling support, whereas JRS primarily focuses on family counselling (George, 2012). In addition, 76.7% of the total sample uses informal family support and 33.6% uses informal friend support. The accessibility and flexibility of the support from family and the NGOs encourage camp refugees to use these resources. Refugees who used formal support from NGOs and informal support from families reported significantly lower family functioning scores and lower depressive symptoms in Phase II than Phase I, indicating better family functioning. In addition, the transmigration stressor score in Phase II is significantly lower than that in Phase I, indicating that the overall migration stressors had reduced from Phase I to Phase II.
Many refugee researchers confirmed the impact of refugee transmigration stressors on mental health challenges and intergenerational family conflicts (Miller & Rasmussen, 2010; George & Jettner, 2016; George et al., 2016). This study reveals that the levels of Phase II sleep difficulties, somatic issues, depressive symptoms and hostility remain largely unchanged from Phase I. This consistency is likely due to the ongoing absence of adequate mental health services in refugee camps. While the percentage of participants who experience loneliness and isolation and worry about family is high in the camp, there is only a monthly mobile medical clinic to receive primary medical care inside the Trichy refugee camp.
In the meantime, the refugee parents tend to avoid seeking external help until the challenges within their family become severe enough to draw attention from others (George, 2016b). Having been forced to flee their homeland to protect their loved ones, refugees often find themselves without status or material possessions during their displacement. In such situations, many refugees strive to preserve their identity by resolving issues internally rather than exposing their difficulties to the outside world. This approach can lead to significant crises, particularly when the refugees’ expectations and cultural beliefs clash with the established norms and traditions of the host countries where the refugee camps are situated (Miller & Rasmussen, 2010).
As suggested from the data in this study, families provide each other constant support to protect family status and identity until their health deteriorates. It may also mean that there is a need for more culturally based resources to address family conflict, considering the lack of openness with outsiders in South Asian culture, which may eventually address the health relapse. All study participants confirmed their utilisation of government support, such as housing in refugee camps, a monthly ration of grocery items and a monthly mobile clinic to provide primary care to the camp refugees. This government support could be the foundation for building up or expanding resources to address migration stressors, family functioning and mental well-being. Participant responses indicated a strong connection between their utilisation of support for daily stress, family conflict and health care, highlighting the need for a coordinated, collaborative approach to address these interconnected needs. Therefore, it is an urgent need to provide increased assistance to address transmigration stressors in refugee camps, which will lead to reducing the public health cost, while these refugees reach host countries for their post-migration settlement.
Conclusion
This study explored the intricate dynamics of resource utilisation, transmigration stressors, mental health issues and family dysfunction among Sri Lankan camp refugees in India. Through a longitudinal approach spanning four years, we gained valuable insights into how these factors evolve over time and impact the lives of refugees. By documenting the specific experiences of Sri Lankan refugees, this study enriches the general understanding of the migration process, highlighting the intersection of mental health, socio-economic challenges and family dynamics by examining the multidimensional nature of migration and displacement. These insights can inform public discourse and raise awareness about the complexities of refugee experiences.
Limitations of this study include data collection from a single camp, and the unavoidable attrition of the participants over the course of the data collection period. Also, while the study was designed to mitigate sampling bias, we have not considered survey biases in our analysis. Furthermore, while our study focused specifically on Sri Lankan Tamil refugees in Indian camps, future research could explore how these findings apply to other refugee populations and contexts. This could help develop more universally applicable strategies for supporting refugee mental health and family functioning.
In conclusion, our study highlights the complex interplay between transmigration stressors, mental health, family functioning and resource utilisation among refugees. It underscores the need for holistic, long-term approaches to refugee support that address ongoing stressors and leverage both formal and informal resources. As global displacement continues to rise, such insights are crucial for developing effective strategies to support refugee well-being and adaptation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute of Health (NIH) Fogarty International Center (FIC) grant number K01 TW009648: ‘Testing a refugee family dynamics model: A study with Sri Lankan Tamils in camps’.