
Abstract
Improved menstrual hygiene management (MHM) is key to socioeconomic empowerment of women through improved well-being. However, Safe MHM remains a challenge in developing countries particularly in rural and low-income settings. This study assessed the influence of a pilot project that adopted nurturing care group approach to improve MHM in rural communities of Ghana. Four (4) communities each from Savelugu Municipal and Sekyere East District Assemblies were selected for a qualitative study using 16 focus group discussions. Data was analysed inductively using content analysis. Findings from 162 study participants showed satisfactory MHM awareness and practices among beneficiaries. MHM awareness and education sources included close relatives, friends, NGOs, public and social institutions (e.g., health centres, churches, schools). The intervention improved MHM behaviour and personal hygiene practices. Persistent challenges included menstrual taboos and stigma, limited availability and prohibitive cost of commercial sanitary pads, burden of managing menstrual pain, and inadequate knowledge of menstrual complexities. Menstrual stigma was comparatively lower in intervention communities than controls, but no differences were observed regarding menstrual taboos which were largely sustained by religious and superstitious beliefs. Promoting local production and use of reusable menstrual pads from fabrics was considered an innovation to reduce the cost burden and address non-availability of commercial alternatives. Overall, the intervention positively influenced understanding of personal hygiene practices and contributed to reducing stigmatisation. Future interventions would require extensive collaboration with key stakeholders in facilitating change processes, particularly in addressing entrenched menstrual taboos.
Plain Language Summary
Improving menstrual hygiene management (MHM) leads to healthy life for socioeconomic development of women. Yet, safe MHM remains a challenge in developing countries especially in low-income settings. This paper focused on understanding the influence of a piloted project that used nurturing care group approach to improve MHM in rural communities of Ghana. The study surveyed eight communities with 16 focus group discussions from two District Assemblies. The findings from 162 study participants showed satisfactory MHM awareness and practices among participants with most MHM information sources listed as family members, friends, NGOs, public and social institutions (e.g., health centres, churches, schools etc). Also, participants claimed improved MHM behaviour and personal hygiene practices from the intervention. Persisting challenges reported by participants included the non-availability and prohibitively high cost of commercial sanitary pads, the burden of managing menstrual pains, inadequate knowledge of menstrual management, as well as menstrual taboos and stigma. Menstrual stigma was perceived to be comparatively low among intervention communities than controls, unlike menstrual taboos which remained prominent across all communities–largely due to religious and superstitious beliefs. Championing the local production and use of reusable fabric-based menstrual pads was seen as an innovation to improve access and reduce the cost of sanitary pads. Project intervention positively enhanced participants' understanding of personal hygiene practices, and contributed to reducing stigmatization. Future interventions will require extensive collaboration with key stakeholders to facilitate change processes especially in addressing menstrual taboos.
Introduction
Menstrual hygiene management (MHM) is critical to achieving several Sustainable Development Goals (SDGs), including SDG 3 – good health and well-being, SDG 4 – inclusiveness and quality education, SDG 5 – gender equality and women’s empowerment, SDG 6 – clean water and sanitation, and SDG 8 – decent work and economic growth. These goals are key to addressing the needs of women and girls, especially those in vulnerable situations. Meanwhile people who menstruate face multiple challenges in managing MHM at home, schools and workplaces (Sommer et al., 2016). These challenges are compounded by factors such as long distances between home and school, poverty, and inadequate facilities (including water, toilets and changing rooms), especially in rural areas (Montgomery et al., 2012; Oruko et al., 2015; Rossouw & Ross, 2021). Other key barriers include limited access to MHM materials, menstrual stigma and taboos, period pain, and associated illnesses such as distress, dysmenorrhoea, headache and excessive bleeding (Maqbool et al., 2022; WHO/UNICEF, 2024).
The dignity and well-being of menstruating women in low-income settings are affected by the aforementioned MHM challenges (Sychareun et al., 2020). Moreover, many women and girls have inadequate knowledge about menstruation and/or lack information on safe menstrual hygiene practices (MacLean et al., 2020). This is partly linked to the fact that menstruation remains shrouded in silence in many cultures. For instance, the stigma associated with menstruation has been observed universally whether in Asia, Africa, Australia and America (Patkar, 2020). In some cultures, such as those in Nepal and the Pacific, women are still required to stay in secluded locations like menstrual huts during menstruation (Joshi & Acharya, 2022; Mahon & Fernandes, 2010). Among the Akans in Ghana, women face multiple restrictions during menstruation, including prohibitions against visiting shrines, attending palace hearings, and cooking for husbands and/or male household members (Agyekum, 2002). These practices emphasise the persistence of social seclusion of women during menstrual periods. At times, restrictions such as avoiding household chores are perceived to be desirable by women (Robinson & Barrington, 2021); however, they may also reinforce negative stereotypes (Tomlinson, 2025).
Urgent attention is needed to address the challenges of MHM including stigma and taboos (and the fear they generate), poor hygiene practices, and the lack of effective antidote for menstrual pains and other illnesses (Armour et al., 2019; Rubinsky et al., 2020; Shah et al., 2019). MHM constraints contribute to menstrual poverty compounded by inadequate education and training (Mohammed & Larsen-Reindorf, 2020), as well as the teasing of adolescent girls for period stains and/or odour (Benshaul-Tolonen et al., 2020). Menstrual poverty restricts socio-economic empowerment among women in low- and middle-income countries (Miiro et al., 2018). Addressing these concerns will not only promote a healthier and more productive lifestyle but also safeguard women’s dignity (Mchenga et al., 2020). Recent campaigns for improved MHM emphasise positive menstruation and female empowerment (Campbell et al., 2021). Efforts to change the narrative around MHM are driving interventions aimed at breaking menstrual stigma and taboos by providing relevant knowledge, skills, and resources (Hennegan & Montgomery, 2016). Such interventions create opportunities for girls, women, and communities to openly discuss menarche and period myths, which are often intrinsically linked to local menstrual taboos (Mohammed & Larsen-Reindorf, 2020; Robinson & Barrington, 2021).
World Vision piloted a Nurturing Care Group (NCG) approach project in Ghana to improve MHM using community-based care groups. The project components, MHM and animal faeces management (AFM) with the later component recently published (Dwumfour-Asare et al., 2025) – were grounded in behaviour change approach that empowered volunteer care group leaders to create a multiplying effect by reaching households through neighbour-to-neighbour contacts, home visits and group meetings (Borger & Davis, 2019; World Vision [WV], 2020). The project aimed to address menstrual hygiene and animal faeces management challenges at both household and the community levels through collective action for improved environmental health, safe water, sanitation and hygiene practices (WV, 2020). By integrating MHM and AFM concepts, the initiative leveraged community collective effort to strengthen these often neglected but critical components of environmental sanitation interventions.
There is increasing policy attention on menstrual hygiene management (MHM), shown in the National Guidelines for MHM in Schools and the Ghana WASH Sector Development Programme (GWASHSDP 2021–2030). However, these policies remain largely school-focussed (Ministry Of Sanitation & Resources, 2023), with limited emphasis on the community-level interventions – particularly in rural areas where poverty, stigma, inadequate WASH infrastructure and related challenges disproportionately affect women and girls (Gbogbo et al., 2025; Kpodo et al., 2022). Meanwhile, community-driven and peer-led approaches like the Nurturing Care Group model, have proven successful in promoting positive outcomes in maternal and child health (Borger & Davis, 2019). Yet, such approaches remain scarce in WASH interventions including MHM and this gap presents an opportunity to develop sustainable, family- and community-centred interventions led by caregivers and peer leaders. Such initiatives could help shift social norms (using Social Norms Theory) and foster behaviour change (grounded on the Health Belief Model) (Castro & Czura, 2021; Warlenda & Marlina, 2024).
This qualitative evaluation of the Nurturing Care Group (NCG) project is presented in two separate papers – this paper and another on animal faeces management, already published (Dwumfour-Asare et al., 2025). They are separated due to the conceptual complexities involved. Again, the contrasting scope and themes with distinct attributes, made it nearly impossible to produce a single, integrative article that maintained digestible for readers (Fine & Kurdek, 1994). This paper, which focuses on the menstrual hygiene management (MHM) component of the intervention, highlights participants' experiences with knowledge transmission, behaviour change practices, and shifting social norms – particularly efforts to break stigma and taboos.
Methodology
Brief Description of the Study Area and the Pilot Project
The study was undertaken in the two districts – Savelugu Municipal and Sekyere East District Assemblies in Ghana. While Savelugu Assembly is dominated by the Mole-Dagbani (88.4%) ethnic groups, and Moslems (95%), the Akans are the majority tribe (85%) with most worshippers (76%) being in Sekyere East District (Ghana Statistical Service [GSS], 2014a; GSS, 2014b). A brief overview of the project is shared here. The project areas were namely Savelugu Municipal and Sekyere East District Assemblies. The project used the Nurturing Care Group (NCG) approach, an adopted version of Care Group model from WHO/UNICEF Nurturing Care Framework. The project was implemented in selected communities from June 2019 to January 2021.
For menstrual hygiene management (MHM) component of the project, two main lessons were emphasised for beneficiaries:
(1) Menstrual hygiene management behaviour, targeting women and girls above the age of 10 years; and
(2) Breaking the stigma and taboos surrounding menstruation, achieved by involving household members within the communities.
The pilot project has been described in detail in an earlier publication on the animal faeces management component of the intervention (Dwumfour-Asare et al., 2025); therefore, only a summary of the key themes is provided here for readers. The project focussed on integrated behaviour change using groups of 10 to 15 community-based volunteers as change agents (leader mothers) whom the project trained to cascade down behaviour change messages and activities to caregiver groups (mothers and pregnant women and ladies) at the neighbourhood and household levels throughout the community (Dwumfour-Asare et al., 2025; Perry et al., 2015). Thus, building social support and cohesion, and linking neighbourhoods with community leaders, and government services/staff (where possible) to create a multiplying effect for equitable reach of beneficiary households through neighbour-to-neighbour contacts, home visits and group meetings (Borger & Davis, 2019). The project used collective action to enhance behaviour change through peer support and redefining community norms for the improvement of private and communal wellbeing (Borger & Davis, 2019; Dwumfour-Asare et al., 2025).
Study Approach and Data Collection
A qualitative content analysis study was carried out in selected communities with and without the NCG project intervention. The sampling strategy was convenience because the target was female participants who had lived in the community during the intervention, who were readily available, and also capable of sharing experiences from the NCG project (Elo et al., 2014; Moser & Korstjens, 2018). Thus, we targeted a homogeneous sample of females with menstrual hygiene experience in rural communities (Bornstein et al., 2013; Palinkas et al., 2015). The data collection campaign took place between 22nd November 2021 and 11th December 2021 in 8 communities: 4 each from Savelugu Municipal and Sekyere East District Assemblies. The study used 16 focus group discussions (FGDs) with 2 female groups (those above 25 years, and those below 25 years i.e., 15–25 years) in each selected community. In each district, two intervention communities and two control (non-intervention) communities were randomly selected. Females who had been in the community at the time of the project intervention were conveniently recruited as study participants with the support of community Care Group Leaders based on age groups, not a group leader, and available to participate in the study.
The FGD sessions were facilitated by the first two authors using FGD guide with questions based on the key themes: background of the NCG programme, participants’ sources and kind of information on MHM before and after intervention, specific knowledge acquired/lessons recall, and existing barriers to MHM. The FGDs were held using the two local languages of participants. In overcoming a language barrier at Savelugu, two experienced community development officers were recruited as translators with the support of the World Vision Area Programme Office to co-facilitate FGDs with the lead researchers on the field. The FGD sessions with 6 to 15 participants took between 1 and 1.25 hr to complete with audio and field notes recorded. Large size participants were allowed for sharing of wide range of experience and shared narrative in addition to achieving efficiency with available participants within time constraints (Dwumfour-Asare et al., 2025; Krueger & Casey, 2014).
All protocols including FGD guide (see Supplemental material 1) approved by an institutional review board (IRB) for ethical clearance with reference CHRPE/AP/418/21 were followed including seeking of informed consent and assent from participants after reading and explaining information about the study to them (in English and the local dialects). Verbal informed consent from participants was witnessed by the leaders who led participants’ recruitment, and the consent was documented as part of the field recordings. The same was done for assent procedure for participants below 18 years (15–17), in addition to using proxy parental informed consent from the leaders who recruited them with permission from parents. The non-invasive qualitative study design of this research limited the risk of potential harm to participants by employing voluntary participation, informed consent, and focus group discussions conducted within community settings to reduce inconvenience, discomfort, and related stress. Ethical standards approved by a nationally recognised institutional review committee were upheld, including strict confidentiality, anonymity, and respect for the human rights of all participants, including minors and young persons. The potential benefits of the research to society far outweigh the risk of potential harm to study participants. Valuable insights were gathered from participants on an emerging community-driven and peer-led behaviour change approach to shifting regressive social norms such as menstrual stigma and taboos in rural communities. Participants’ contributions generated relevant evidence-based knowledge that could inform future programmes and policies for the benefit of wider society in the long term. In addition, the research provided an opportunity for participants to interact with the research team for information sharing, including sources of available support systems.
Data Management and Analysis
First, data from FGDs were transcribed and organised using Microsoft Word by adapting the three-stage approach to minimise errors – using audio recording and field notes together by careful listening before transcriptions (Barker et al., 2016). All transcribed data were finally transferred to Microsoft Excel database for data analyses by following the structured themes outlined in the interview (FGD) guide. The analysis was done by reading through transcripts under each structured themes and synthesising narrative summaries of main findings based on descriptive categories derived from terms (e.g., MHM education source, challenges, taboos, stigma, behaviour changes etc.) in the main structured themes (Moser & Korstjens, 2018). This inductive content analysis described the content of categories under the structured themes (Elo et al., 2014) and was opened to careful identification of emerging subthemes and supporting synthesis with peer debriefing and member checking, and verbatim quotes (Antwi-Agyei et al., 2020; Onwuegbuzie et al., 2009). During manuscript revision, Microsoft Copilot (Microsoft Corporation, Redmond, WA, USA) was used for grammar check and style suggestions after which final editing was reviewed and approved by the authors.
Limitations of the Study
The findings are limited by the small sample size drawn from few selected communities with convenient sampling and voluntary participation by respondents – risking selection biases and limiting generalisability yet provided insights into the context. We also acknowledge limitations such as cross-sectional design’s inability to establish causality, potential social desirability bias in self-reported data, and the absence of male voices in exploring stigma dynamics. This study is not an impact evaluation of the pilot intervention but rather a qualitative assessment aimed at understanding the intervention’s immediate influence, lessons and experiences from beneficiaries’ perspective. These findings may be subject to recall bias, satisficing, observer bias and the Hawthorne effect (Dwumfour-Asare et al., 2025). Although the behaviour change intervention employed a controlled before-and-after trial design (Tidwell et al., 2023), this paper draws solely on post-intervention field data collected by the research team. The authors were unable to return to the field for participant feedback on the findings and instead relied on internal peer review, revisiting the transcriptions, notes and audio recordings sequentially (Noble & Smith, 2015).
Results
Study Participants
The study communities and participants were mainly subsistence farmers. Table 1 presents the two (2) main FGD categories – women under 25 years, and those above 25 years from four (4) intervention and four (4) control communities. The group sizes ranged from 6 to 15 participants, with an average of 10 members per focus group. The total participants involved in the study were 162 women including 78 and 82 respectively from control and intervention communities.
Number of Participants for the FGDs in the Study.

Key Themes From Focus Group Discussions
Table 2 presents the results of thematic analyses of responses on participants’ experience including menstrual stigma, taboos and myths based on the structured thematic FGD facilitation tool used.
MHM Education and Existing Challenges From Focus Group Discussions.
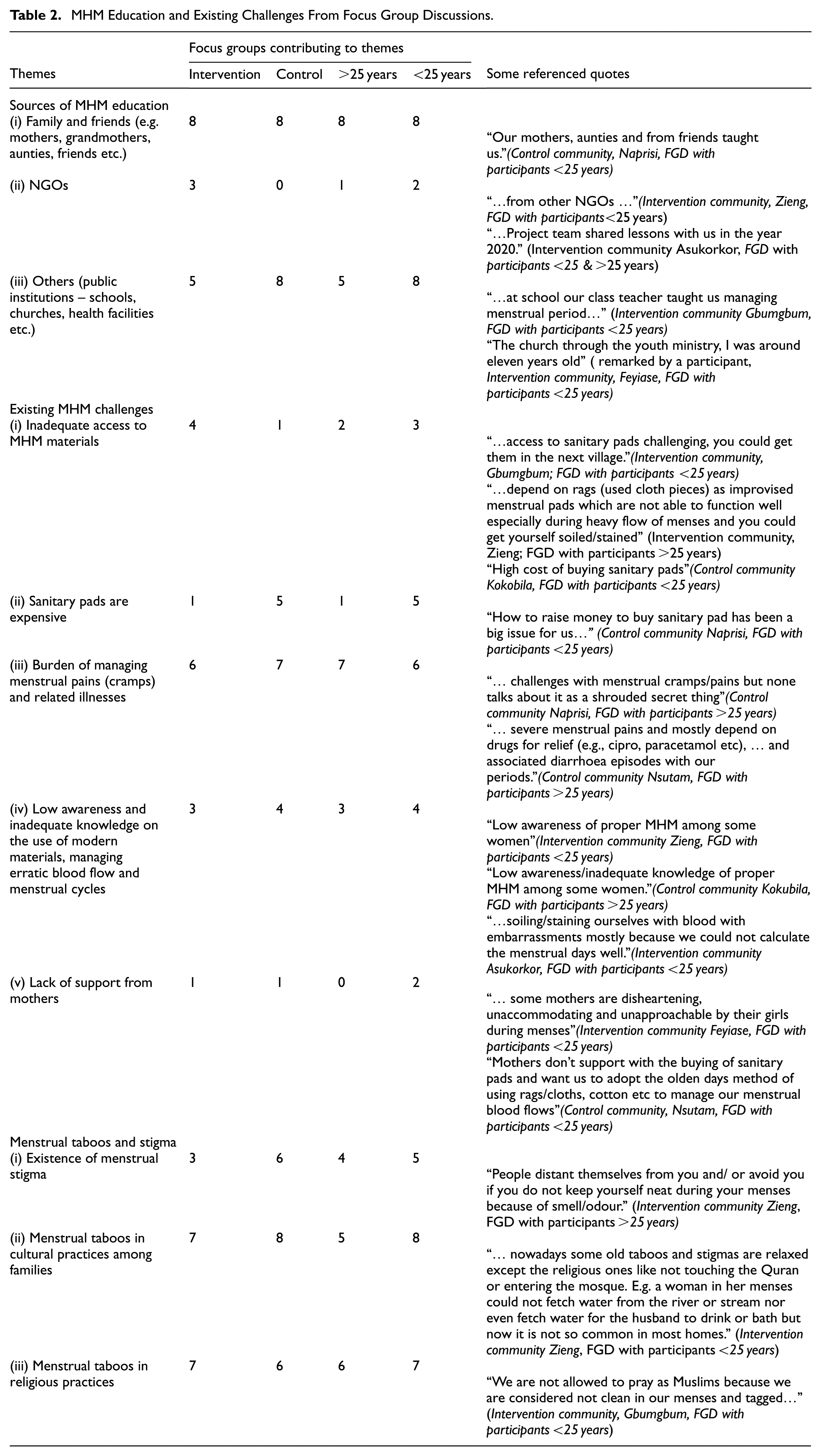
Participants primarily received awareness and education on MHM, especially for first-timer learners, from relatives and/or friends, and later from NGOs, and other public institutions. The challenges associated with MHM were largely linked to period poverty, stemming from limited access to menstrual materials and inability to afford them including the burden of managing menstrual pains and related illnesses. Menstrual stigma and taboos were also prevalent in the study communities, embedded directly or indirectly within religio-cultural beliefs, practices and myths. The findings revealed mixed trends in terms of differences between intervention and control communities as well as across age groups.
Sources of Menstrual Education
Study participants reported that menstrual education was predominantly spearheaded by females. The sources of education included social institutions such as families and friends, community neighbours, schools, health centres and churches (Table 2). Within families, menstrual education was typically provided by grandmothers, mothers, older female siblings, and other close relatives who had personal experience with menstruation. Information from health centres was considered particularly useful, especially regarding the management of menstrual pains and the maintenance of personal hygiene. The findings largely reflected collective responses or similar experiences shared by individuals which were subsequently confirmed among group members.
Some participants disclosed the following: “My mother discussed it with me”“… my senior sister discussed it with me” (A participant from intervention community, Gbumbum; FGD with participants <25 years)
For some participants, MHM was learned by paying attention to the practices of older people as cited: “I learnt from siblings especially by observing my older sisters’ practices” (A participant from intervention community, Feyiase; FGD with participants <25 years). “I learnt through attentive listening from one lady who mostly sent me to buy sanitary pads and cotton wool” (A participant from control community, Nsutam; FGD with participants <25 years).
Unlike the majority of participants, two young women were not privileged to learn about MHM practices from anyone including adult female relatives. Instead, they relied on their own challenging personal experiences beginning at menarche. One participant, who lived alone with her father, recounted that she never informed the Dad about her menarche because she felt too shy.
“I was shy to tell my father because I was living alone with him as single parent” (A participant from an intervention community, Feyiase; FGD with participants <25 years). “I never had the opportunity to be taught by anyone close to me. I learnt it on my own in a hard way – I had to do something the first time and afterwards by personal experience.” (A participant from an intervention community, Asukokor; FGD with participants <25 years).
Meanwhile, some responses indicated that the transfer of MHM knowledge from adults to the young was generally low, and some mothers did not intentionally share menstrual information with their female wards.
“Some of us have discussed MHM with our children but others have not because they believe or assume their children already know it, and they hide it from them.” (Intervention community, Asukokor; FGD with participants >25 years) “Attitude from some mothers is disheartening; they are unaccommodating and unapproachable by their daughters” (Intervention community, Feyiase; FGD with participants <25 years). “Mothers don’t support with the buying of sanitary pads and rather want us to adopt the olden days method of using rags/cloths, cotton wool etc. to manage our menstrual blood flows” (Control community, Nsutam; FGD with participants <25 years) “We need to be supportive to our children (young girls) when in their menses” (Control community, Tetekaso; FGD with participants >25 years)
After the intervention, some participants reported that mothers related better with their young girls regarding MHM issues. However, some young participants did not perceive any significant paradigm shift among adult women (mothers).
Participants of one of the young groups had these to say: “We see our mothers holding books and making rounds, but they never reach us with any education or information. …. we see that the mothers only take their books when they hear that the Project team is coming around.” (Intervention community, Feyiase; FGD with participants <25 years)
Menstrual Hygiene Management Challenges
Study participants expressed a range of views across groups regarding the challenges they faced during menstrual periods. However, the challenges identified were largely similar (Table 2), including low awareness and limited access to modern MHM materials (e.g., sanitary pads), difficulty in managing menstrual cramps, reduced self-confidence during menstruation. Stigma and taboos surrounding MHM also emerged as challenges and these are addressed in the section. Notably, the incidence of all challenges was more pronounced in the control communities and among younger participants.
For control communities, key challenges reported by participants were as follows:
low awareness and inadequate knowledge of proper MHM,
erratic and inconsistent menstrual cycles and associated management difficulties,
menstruation related health conditions such as menstrual cramps, diarrhoea, skin rashes and others are unfortunately shrouded in secrecy without open discussions,
high cost of MHM materials such as commercial sanitary pads and alternative products,
overuse of painkillers (e.g., cipro, paracetamol etc.),
improvisation of rags and toilet tissue papers as sanitary pads, and
lack of parental support, particularly from mothers, in providing MHM materials.
“The challenge is how to manage menstrual cramps/pains but unfortunately people don’t talk about it because it’s considered a secret thing. … challenges with menstrual cramps/pains but none talks about it as a shrouded secret thing.” (Control community, Naprisi; FGD with participants >25 years) “…my experience is frequent visits to the toilet – diarrhoea episodes when in I am in my menses.” (Participant, Control community, Nsutam; FGD with participants >25 years). “… severe menstrual pains and mostly depend on drugs for relief (e.g., cipro, paracetamol etc), … and associated diarrhoea episodes with our periods.” (Control community, Nsutam; FGD with participants >25 years)
In the intervention communities, the main MHM challenges identified were as follows:
Low awareness and limited access to modern MHM materials, such as sanitary pads with some participants noting discomfortable in their use,
Menstrual cramps and headaches, often accompanied by bodily weaknesses and other related illnesses,
Reduced self-confidence during menstruation,
Erratic blood flows and difficulties in predicting menstrual cycle which sometimes led to public embarrassment from unexpected blood stains, and
Inadequate parental support, particularly for young females, in accessing MHM materials.
“Getting access to a sanitary pad is challenging. Pad is not sold in our village, so we have to travel to a nearby town to get one.” (Intervention community, Gbumgbum; FGD with participants <25 years) “We largely depend on rags (used cloth pieces) as improvised menstrual pads which were not able to function well especially during heavy flow menses and you could get yourself soiled/stained.” (Intervention community, Zieng; FGD with participants >25 years) “…menstrual pains and headaches are common with young girls in this community during menstrual periods.” (Intervention community, Feyiase; FGD with participants <25 years). “…soiling/staining ourselves with blood with embarrassments mostly because we could not calculate the menstrual days well.” (Intervention community, Asukorkor; FGD with participants <25 years).
Among the older female groups, the main challenge was menstrual cramps and the inability to manage the condition or receive adequate support. This often led to frustration, stress and depressions, especially when combined with overburdened domestic chores. These factors negatively affected self-esteem and confidence meeting public expectations.
“…how to behave comfortably in public during menstruation.” (Intervention community, Gbumbum; FGD with participants >25 years). “… any challenges are hardly talked about, if any at all, except menstrual pains.” (Intervention community, Asukokor; FGD with participants >25 years). “Sometimes the menstrual period changes, and you may miss the timing, which could lead to unexpected blood stains and public embarrassment. Mostly this happens when we are not able to do the calculations well.” (Intervention community, Asukokor; FGD with participants < 25 years).
Aside from these challenges, young participants in the intervention communities expressed their dissatisfaction with the attitudes of their immediate family members, including mothers. In some cases, mothers encouraged their daughters to use improvised MHM materials such as rags and tissue paper instead of modern sanitary pads.
“…the attitude of some mothers is not the best, they are unaccommodating and unapproachable by us their daughters.” (Intervention community, Feyiase; FGD with participants <25 years) “Mothers don’t adequately support us daughters with the purchase of sanitary pads and rather want us to adopt the old-aged method of using rags/cloths…” (Control community, Nsutam; FGD with participants<25 years)
Menstrual Taboos and Stigma
Menstruation-related taboos and stigmas were present in both control and intervention. These were largely driven by religious beliefs, cultural traditions, lapses in personal hygiene practices, and to some extent, exposure to modernisation. These taboos and stigmas appeared similar across communities, regardless of demographic differences (north vs. south, and young vs. old). For example, in Savelugu (northern Ghana), where Muslim communities are dominant, restrictions on women during menstruation – such as exclusion from religious activities congregational prayers or and mosque attendance, limitations on making contacts with or serving male family members (e.g., husbands, fathers, sons) all existed. These observations were comparable to practices reported in Sekyere East (southern Ghana) where similar forms of seclusion were reported within spiritual churches, shrines and fetish priests, and traditional norms observed in some households.
FGD participants from the north shared these views: “We women are not allowed to pray as Muslims at the mosque because we are considered unclean during our menstrual periods” (Intervention community, Gbumbum; FGD with participants >25 years). “… women in menses could not touch the Holy Quran and could not join prayers at the mosque too because we are considered unclean at that time.” (Intervention community, Zieng; FGD with participants <25 years) “… women can’t have sexual intercourse or any intimacy with partners during our periods.” (Intervention community, Gbumbum; FGD with participants >25 years). “We are not allowed to pray nor have sexual intimacy with our partners.” (Intervention community, Kukobila; FGD with participants >25 years). “…women in menses do not enter their husband’s room, can’t cook, not allowed to touch the Quran, pray nor enter the mosque as a Muslim. You’re not allowed to share toilet with men and other people. People distance themselves from those without proper MHM especially when there is odour/smell to that effect.” (Control community, Naprisi; FGD with participants >25 years).
In the Sekyere East communities (southern Ghana), some experience were shared as follows: “… women cannot go to a fetish priests’ houses or shrines in their menses, even very daring to pass by such houses/shrines or greeting them.”(Intervention community, Feyiase; FGD with participants<25 years) “Some churches don’t allow you to enter the church, especially the spiritual churches/movements.” (Intervention community, Asukokor; FGD with participants <25 years) “… we do not cook or hold/touch our father’s food.” (Intervention community, Asukokor; FGD with participants <25 years). “You dare not cook for your father nor touch his drinking cup.” (Control community, Tetekaso; FGD with participants <25 years).
Older participants expressed concern that menstruation-related taboos affected women’s daily life, including domestic chores. For instance, restrictions often prevented them from fetching water, cooking and serving food to husbands and male household members, visiting certain farmlands, or crossing certain rivers and streams for socioeconomic activities. In some cases, menstrual taboos even prohibited women from using the only available riverine transport route, further limiting mobility and participation in community life.
“… we are not allowed to fetch water from the dam.” (Control community, Kukobila; FGD with participants <25 years). “…you don’t cross certain rivers nor attempt to access or fetch water from such rivers in the community.” (Intervention community, Feyiase; FGD with participants <25 years). “…you don’t have to commute across certain rivers in the community, including going to farms and markets.” (Intervention community, Asukokor; FGD with participants >25 years).
Menstrual taboos were observed due to the belief in severe repercussions for women who violated them. In both Savelugu and Sekyere East, some participants shared personal experiences that reinforced the fear surrounding menstrual taboos, citing consequences such as prolonged or heavy menstrual bleeding.
“…one time, I bled continuously for almost two weeks after I crossed that river down the community to my farm, although I didn’t know about the taboo.” (A participant from Intervention community, Asukokor; FGD with participants >25 years). “The taboos are real, and some of us have suffered the consequence before, that if you defiled the taboos, you will experience protracted and heavy menstrual bleeding for several days to weeks.” (Control community, Kukobila; FGD with participants >25 years).
Regarding menstrual stigma, some participants reported that teasing by boys in schools was common, although perpetrators were subject to punishment when reported to school authorities. Such disciplinary measures were intended to deter male bullies and discourage behaviours that perpetuate menstrual stigma.
“When a girl stains herself in school, they may call her names, especially by the boys, saying Osmo! Osmo! Stigmatization may happen only at school, especially when you soil yourself with blood stains – this normally comes from the boys, although they could be punished when it is reported to school authorities.” (Control community, Nsutam; FGD with participants <25 years)
Although, adults were not currently subjected to menstrual stigmatisation, they recalled past experiences from their schooldays, confirming that such ordeals have long persisted particularly within educational settings. However, adults sometimes experienced social isolation, especially in instances of accidental period stains.
“Stigmatization was common at school in those days when you got your dress stained.” (Control community, Nsutam; FGD with participants >25 years) “People distant themselves from you ….during their menses because of smell/odour.” (Intervention community, Zieng; FGD with participants>25 years)
Behavioural Changes Due to MHM Intervention
In the control communities, information and education on MHM came from sources other than the NCG intervention. Participants reported improved MHM practices by exposure to the use of modern and alternative sanitary pads, improved personal hygiene practices, and the importance of supporting others, particularly younger females.
The key improved MHM practices reported from control communities were:
✓ Using modern and alternative sanitary pads with appropriate usage practices,
✓ Improved personal hygiene such as regular bathing – at least twice a day,
✓ Avoiding the use of family planning pills during menstrual periods for effective monitoring of menstrual cycle.
✓ Preparing in advance towards menstruation episodes for safe MHM,
✓ Supporting young girls on MHM through education
“Previously we could use one sanitary pad the whole day, but now we change pads at the right time. You could get infections and sores from using one sanitary pad for a long time.” (Control community, Naprisi; FGD with participants <25 years) “… we have not changed anything much except using modern pads for improved personal hygiene.” (Control community, Kukobila; FGD with participants >25 years) “For us who improvise the use of cloth as pads, we wash the materials and iron it neatly before reuse and it has helped a lot especially when you have no money to buy sanitary pads.” (Control community, Nsutam; FGD with participants >25 years)
In the intervention communities, the list of behaviour change practices was comparatively extensive likely reflecting the additional understanding gained through sensitisation during the nurturing care group (NCG) pilot project. However, the improved behaviour changes did not address taboos directly; rather, they focussed on behaviours that could mitigate or avert stigmatisation, particularly those linked to personal behaviour hygiene practices. Most participants reported that menstruation taboos continued to exist though they were not as stringent as in earlier generations. The shift was attributed to modernisation – particularly the use of modern sanitary pads and improved hygiene that helped conceal menstruation, as well as to certain religious beliefs that contradicted traditional cultural norms and practices.
Key behaviour changes reported by participants from intervention communities included:
✓ Adoption of sanitary pads to discreetly manage menstruation without detection by others. There has been a significant shift from the use of old cloths (rags) to reusable fabrics or disposable sanitary pads, accompanied by improved hygienic practices such as regular changing and bathing.
✓ Abstaining from sexual intercourse to prevent unwanted, particularly teenage, pregnancies.
✓ Enhanced personal hygiene practices, including washing clothes, underwear, and reusable pads, and ensuring they are dried in sunlight.
✓ Dispelling feelings of inferiority associated with menstruation. With improved hygiene, women reported being able to live normally and interact freely without stigma.
✓ Greater preparation for menstruation, including educating younger women on menstrual hygiene management (MHM).
✓ Improved disposal of used sanitary pads, with practices such as burying, burning, or discarding them in toilets to prevent misuse by ritualists seeking them for “rituals” or “blood money.”
✓ Increased efforts to educate and support children, especially girls, on MHM. Women reported stronger relationships with their daughters, sharing concerns and offering guidance during menstruation.
✓ Schoolgirls demonstrated improved self-management during menstruation, reducing the likelihood of accidental staining.
“Now most women wrap used sanitary pads in polythene bags and dispose into toilet or burn them. This practice has been helpful because you hardly see used pads in the streets of the community particularly where you could find dogs littering/dragging them around.” (Intervention community, Asukorkor; FGD with participants >25 years) “We still hear of taboos, but they are not as religiously enforced as they used to be some years back, especially in the olden days.” (Intervention community Feyiase; FGD with participants >25 years) “… nowadays some old taboos and stigmas are relaxed except the religious ones like not touching the Quran or not entering the mosque. For instance, a woman in her menses could not fetch water from the river or stream and even fetch water for her husband to drink or bath, but now it is not so in most homes.” (Intervention community, Zieng; FGD with participants <25 years). “… many people menstruate and go to church without the leaders being aware because of the use of modern sanitary pads.” (Intervention community Asukorkor, >25 years FGD). “We think some taboos are watered down by modernization, because of improved and safe MHM practices of modern life and educational promotion.” (Intervention community, Feyiase; FGD with participants >25 years). “…some church beliefs and modernisation have relaxed some menstrual taboos and stigma. …women in their menses could not go to farm to defile the land or soil but nowadays it is not like that.” (Control community, Naprisi; FGD with participants >25 years).
Apart from improved awareness creation from the NCG intervention, other project activities in schools: provision of toilet facilities with changing rooms, improving MHM knowledge, supply of MHM materials such as sanitary pads for emergencies contributed to improved MHM behaviour changes.
Participants shared experiences from the project intervention as follows:
✓ Increased use of sanitary pads with regular changing practices among young females reinforced through MHM education in schools.
✓ Provision of changing rooms for girls in schools, including improvised spaces such as a converted computer lab where necessary.
✓ Greater acceptance of using bathrooms at home as changing spaces during menstruation, reducing stigma.
✓ Distribution of sanitary pads to schoolgirls by some NGOs.
✓ Teachers providing MHM education directly to schoolgirls.
✓ Upgraded toilet facilities in schools, enabling girls to access changing rooms
✓ Improved knowledge among schoolgirls on proper MHM practices, resulting in fewer instances of accidental staining.
✓ Construction of latrines with urinals and changing rooms in schools by the project to support pupils, especially girls.
✓ Strengthened mother–daughter relationships, with mothers offering greater support and guidance on MHM.
Some of the quotations from FGDs are cited as follows: “Toilet and urinals in schools were provided by the project to ensure privacy especially in MHM to support schoolgirls ….” (Intervention community Feyiase, FGD with participants <25 years & >25 years) “We have changed from using old cloth as sanitary pad to using reusable and/ or disposable sanitary pads. We did not know how to use the pads properly …..we were bathing only in the evenings but now we bath 3 times daily during menstruation.” (Intervention community, Gbumbum; FGD with participants <25 years). “Schoolgirls are now able to manage themselves well without soiling themselves during menstrual periods. Improved awareness, knowledge, and behaviour in that regard has been helpful.” (Intervention community, Asukokor; FGD with participants <25 years). “Previously wastewater from washed pads(cloths) was disposed of in the open, but now it is disposed of in a pit. Clothes, underwear, and reusable pads were washed and dried in our rooms, but now we have been educated to dry them in the sun.” (Intervention community, Gbumbum; FGD with participants >25 years) “We support by educating and monitoring our young girls on MHM. Some of us now have cordial relationships with them to share and support their menstrual issues together.” (Intervention community, Feyiase; FGD with participants >25 years).
Discussions
The study revealed that the primary sources of menstrual hygiene management (MHM) education and awareness among participants were relatives and friends, spanning both younger and older groups across intervention and control communities. This finding aligns with previous studies that underscore the significant role of mothers and close relatives (e.g., older sisters and grandmothers) - as the main conveyors of menstrual knowledge (Holmes et al., 2021; Mohammed & Larsen-Reindorf, 2020). However, reliance on these informal sources may be inadequate as highlighted elsewhere (Plesons, Patkar, Babb, Balapitiya, Carson, Caruso, Franco, et al., 2021). Beyond family networks, participants also reported receiving support from public institutions including schools, churches, health facilities, and NGOs. Particularly, control communities had limited access to any NGO-led MHM education, likely due to the broader neglected of community-level interventions within WASH projects (Asimah et al., 2017). The contributions of NGOs, public institutions and local government authorities were considered highly relevant, echoing findings from other studies that institutional involvement has strengthened menstrual health initiatives (Hennegan et al., 2019; Kansiime et al., 2020). Again, our findings confirmed that Ghanaian schools educate pupils on MHM under the supervision of School Health Education Programme (SHEP) while communities are supported by health centres (Kpodo et al., 2022; Rheinländer et al., 2019). Thus, these institutional structures complement informal familial sources of MHM information, offering more opportunities to leverage a comprehensive framework for menstrual health education.
The main challenges with MHM reported by study participants are consistent with those reported in the literature – limited access and high cost of MHM materials (e.g., disposable sanitary pads), burden of menstrual pains (cramps), low awareness and inadequate knowledge among local women, and the perceptions among young women that mothers provide insufficient support (Kashyap & Choudhari, 2023; Kaur et al., 2018; McCammon et al., 2020). In contrast, the incidence of the first two reported challenges was lower in intervention communities compared to control, a difference that could be partly attributed to increased exposure through the NCG-led MHM education, consistent with outcomes observed in similar interventions (Hennegan et al., 2019). Menstrual cramps were common burden among the women groups who also managed that by self-medication as reported in other studies (Femi-Agboola et al., 2017). Self-medication in MHM is drug abuse partly due to misinformation to use painkillers, antibiotics and traditional herbal concoctions, local practices to numb menstrual pains (Armour et al., 2019). This could be contributing to the high prevalence of self-medication in Ghana (Opoku et al., 2023).
The intervention communities also reported being equipped with skills to produce reusable pads from fabrics towards safe MHM practices. Nevertheless, preference for modern disposable pads remained high, likely due to similar aversion to the burden of washing and reusing fabric pads (van Eijk et al., 2021). Meanwhile, no scalable local production models were available nor established to ensure sustainability. Persistent concerns regarding the affordability of MHM materials among young women undermined parental or guardian support and this could be linked to menstrual period poverty, where access to MHM materials becomes an unmet need (Boyers et al., 2022; Hennegan et al., 2019). Older women, however, appeared more accustomed to improvising fabrics as reusable pads as similarly reported in Ghana (Anaba et al., 2022) and were consequently less burdened by the cost of commercial sanitary pads. Although challenges persist among menstruating women, opportunities to voice out these concerns remain limited, similar to other studies reporting that such platforms are missing even within households and communities (Plesons, Patkar, Babb, Balapitiya, Carson, Caruso, & Chandra-Mouli, 2021; Rheinländer et al., 2019).
On menstrual stigma, awareness was high among participants but it was reported to be marginally present in communities, with about twice the incidence in control communities compared to intervention. No clear difference was observed between the younger and older women groups, suggesting that most women may have had either first-hand or shared experiences of stigma including deeply internalised perceptions (Plesons, Patkar, Babb, Balapitiya, Carson, Caruso, & Chandra-Mouli, 2021). The NCG intervention, similar to other targeted behaviour change projects may have contributed to the reduction of menstrual stigma in the intervention communities (Kansiime et al., 2020). In contrast, menstrual taboos strongly persisted across cultural and religious beliefs and practices in all communities, without notable difference between the intervention and control groups. Almost all discussion groups acknowledged the persistence of taboos as similarly reported that such restrictions are rooted in religio-cultural beliefs and practices (Barrington et al., 2021; Gbogbo et al., 2025). The intervention produced little improvement in this regard, likely because religio-cultural practices are complex, sensitive, and resistant to short-term change. Addressing these entrenched beliefs and systems may require more time and tested integrated approaches including rigorous active engagement with key stakeholders such as community leaders and religious groups (Kansiime et al., 2020; Thapa & Aro, 2021). For instance, a constructive approach could be working with existing socio-cultural frameworks – acknowledging and addressing menstruation-related myths, denial, and religious restrictions across major belief systems such as Christianity, Islam and Traditional Beliefs (Barrington et al., 2021; Thapa & Aro, 2021).
Menstrual taboos affected household practices such as exemption from domestic chores (e.g., cooking, fetching water, serving males), restrictions on sexual intimacy, and prohibitions against appearances at social gatherings. Sentiments regarding these restrictions were more pronounced in Savelugu (northern communities – mostly Muslim and traditionalist) than Sekyere (southern communities – mostly Christians and traditionalist), likely reflecting religio-cultural differences. This observation is consistent with findings from a similar study conducted in a neighbouring northern district (Mohammed & Larsen-Reindorf, 2020) and may be characteristic of predominantly Islamic communities, as noted elsewhere (Shah et al., 2019). However, Sekyere East communities exhibited relatively relaxed restrictions, partly due to modernisation and the influence of church teachings. While some menstrual taboos are increasingly regarded as outdated, they remain mystified by perceived spiritual repercussions such as prolonged menstrual episodes among women who flout them. Among traditionalists, beliefs persist regarding the mystical ability of menstrual blood to neutralise charms and spiritual powers, thereby reinforcing the perpetuation of taboos (Kpodo et al., 2022).
In these local contexts, fear of menstrual taboos persists despite the absence of scientific proof supporting the perceived consequences, although such occurrences are reported to be possible (García-Montes et al., 2008). Nonetheless, interventions have opportunities to challenge menstrual taboos by leveraging improved knowledge and modernisation, consistent with the decline of other taboos (Osei-Tutu, 2017). For instance, restrictions on sexual intercourse during menstruation may be reframed with scientific knowledge to counter traditional dogma. Such restrictions, from biomedical perspective, could help reduce risk of sexually transmitted infections associated with unprotected sex during menstruation (Hensel et al., 2016). Effective approaches may involve community-based open discussions on the consequences of menstrual taboos and stigmas including internalised stigma characterised by secrecy, shame, decreased mobility, inequity, and negative impact on confidence and self-efficacy among women (Hennegan et al., 2019; MacRae et al., 2019). Such participatory platforms could foster reflection and collective action for communities to re-evaluate retrogressive norms and promote menstrual dignity.
The consequences of menstrual stigma and taboos were associated with two key emerging themes: the mother wound, and misogyny. The mother wound is primarily associated with the absence or inadequacy of mothering or maternal care and emotional support (Gaba, 2019). This was particularly evident among younger women who reported insufficient guidance and assistance from mothers regarding the necessary menstrual hygiene and coping strategies. Such experiences are not unexpected in patriarchal settings like Ghanaian communities, where women may similarly internalise stigma and taboos across generations (Lewis, 2020). The NCG intervention’s attempt to break this social barrier by actively engaging women leaders to provide mentorship and support was notable, although it faced some implementation challenges. Such included limited community buy-in partly due to failure to engage male counterparts who are leaders of households, communities and religious institutions in typical patriarchal contexts (Dwumfour-Asare et al., 2025; Lewis, 2020).
Although, menstrual misogyny cannot be disregarded in this study, the findings appeared relatively mild, primarily linked to stigmatisation rather than the more severe forms of misogyny reported elsewhere, such as overt enforcement of sexism, collusion with racism, gender-based violence, or explicit hatred towards women (Loewen Walker, 2024). Arguably, the misogyny observed in the current study may be less intense because it manifests as episodic discrimination during menstruation rather than targeting women outside of menstruating moments including premenarchal or postmenopausal stages. Moreover, no overtly abusive treatment was reported by our study participants that aligns with common misogynistic practices of “deploying disgust to objectify and dehumanise” women (Bobel et al., 2020). Perhaps, the increasing invasion of modernism, and improved knowledge including enhanced awareness and education from the NCG intervention may have contributed to averting more misogynistic extremism. Nevertheless, persistent menstrual taboos and marginal stigma – regardless of prevalence or intensity – constitute menstrual negativity, which has historically been known as misogynistic (Tomlinson, 2025). This is particularly evident in our findings confirming that menstruation could be weaponized as an oppressive tool through bleeding shame and other menstrual burdens (Bobel et al., 2020). The persistent challenge remains taboo-driven menstrual misogyny, which poses a daunting task for rights activists and interventions such as the NCG pilot project. The difficulty arises from the complex interplay between religio-cultural systems and menstrual symbolisms. Most critically, the near inseparability of religio-cultural practices and menstrual meanings continues to (re)produce religion and culture, thereby reinforcing the cycle of stigma and dogma (Bobel et al., 2020).
MHM experience and lessons learned were more pronounced in intervention than control communities. This was expected given the additional information, resource materials and support provided through project implementation beyond the general awareness and promotion activities available in communities. Available generic MHM awareness sources similarly emphasised personal hygiene practices, safe use of sanitary pads, and preparations for menstrual cycles (Hennegan & Montgomery, 2016). However, the NCG project offered beneficiaries a more in-depth experience including enhanced practices such as bathing at least thrice daily, regular changing of pads, making/sewing reuseable sanitary pads from fabrics, safe disposal of wastewater and used materials, and increased attention to supporting younger women. Overall, the NCG project fostered some expected positive attitude and behaviour change (Gneezy et al., 2011), promoted innovation, self-efficacy and confidence while dispelling known negative psychosocial attributes (Hennegan & Montgomery, 2016).
Conclusion
The study demonstrates a satisfactory level of menstrual hygiene management awareness and practices among women across age groups in the study areas. Sensitisation and education are delivered through multiple channels including relatives, peers, NGOs, health centres, churches, and schools. The NCG intervention particularly enhanced beneficiaries’ understanding of safe MHM practices and fostered positive behaviour change. Nonetheless, persistent challenges remain. Limited access to affordable sanitary materials contributes to menstrual poverty, particularly among younger women. The burden of menstrual pains and illnesses, coupled with entrenched taboos, continues to undermine women’s wellbeing. Importantly, the intervention succeeded in surfacing unspoken challenges, even though some extended beyond project scope and design. These challenges are largely systemic and institutional rather than individual, highlighting the need for broader structural responses.
Menstrual stigma was found to be relatively low and, some communities, scarcely recognised such stigma. In contrast, menstrual taboos remain widespread across both control and intervention communities, because they are rooted in religio-cultural and superstitious beliefs. Stigma typically arises from lapses in personal hygiene, such as visible blood stains or odour, especially in school settings. The promotion of sewing reusable menstrual pads from fabrics emerged as particularly effective strategy, offering affordable alternatives for women unable to purchase commercial sanitary pads. However, the absence of scalable local production models limited opportunities to institutionalise the practice.
Nurturing care group approach could be integrated into national WASH education programmes and strategies. Future interventions should expand their scope to engage directly with institutions and influential stakeholders, including community and religious leaders, to drive long-term change. Addressing deeply embedded religio-cultural taboos, that drives intergenerational mother wounds and misogyny, requires sustained and culturally sensitive approaches to challenge systemic barriers and regressive socio-cultural norms. Future research could consider long-term and rigorous impact assessment of the NCG approach - employing designs such as randomised controlled trials or quasi-experimental designs with representative sampling and gender-balanced perspectives for generalisability beyond qualitative insights.
Supplemental Material
sj-pdf-1-sgo-10.1177_21582440261418218 – Supplemental material for Understanding Nurturing Care Group Approach in Addressing Menstrual Challenges in Selected Ghanaian Communities
Supplemental material, sj-pdf-1-sgo-10.1177_21582440261418218 for Understanding Nurturing Care Group Approach in Addressing Menstrual Challenges in Selected Ghanaian Communities by Bismark Dwumfour-Asare, Eugene Appiah-Effah, James Ben Tidwell and Kwabena Biritwum Nyarko in SAGE Open
Footnotes
Acknowledgements
Authors appreciate the enormous support from World Vision, Inc. (USA) for funding this research work under the contract number SOW 33514, and the Ghana Team, especially the Area Programme Offices in the Sekyere East District and Savelugu Municipal Assemblies particularly Rachel, Georgina, and Felix and our field assistants Timothy, Gideon, and Clement.
List of Abbreviations
AFM animal faeces management
FGDs focus group discussions
IRB institutional review board
MHM menstrual hygiene management
MMDAs metropolitan, municipal and district assemblies
NCG nurturing care group
NGOs non-governmental organisations
SDGs sustainable development goals
UNICEF United Nations children’s fund
WASH water, sanitation and hygiene
WHO world health organisation
Ethical Considerations
Ethical clearance certificate was secured from the Committee on Human Research and Publications Ethics (CHRPE) of the Kwame Nkrumah University of Science Technology was sought with reference number Ref: CHRPE/AP/418/21 before field work was executed. All approved protocols and directives were dully followed.
Consent to Participate
Informed consent was sought from study participants after reading and explaining the study information to them (in English and the local dialects). Verbal consent was witnessed by the leaders who facilitated participant recruitment, and it was documented as part of the field recordings (audio and field notes). The same procedure was followed to complete the assent process for participants aged 15–17 years, in addition to obtaining proxy parental consent from the leaders who recruited them. These leaders acted as proxy parents with permission from the minors' parents.
Author Contributions
Conceptualisation: James Ben Tidwell & Bismark Dwumfour-Asare
Data curation and formal analysis: Bismark Dwumfour-Asare and Eugene Appiah-Effah
Funding acquisition: James Ben Tidwell & Bismark Dwumfour-Asare
Field investigation: Bismark Dwumfour-Asare & Eugene Appiah-Effah
Methodology: Bismark Dwumfour-Asare, Eugene Appiah-Effah, James Ben Tidwell, and Kwabena Biritwum Nyarko
Writing – drafting, reviewing & editing: Bismark Dwumfour-Asare, Eugene Appiah-Effah, James Ben Tidwell, and Kwabena Biritwum Nyarko
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was sponsored by the World Vision, Inc. (USA) as part WASH programme under the contract number SOW 33514 to BDA, EAE and KBN as independent assessors under the supervision of JBT a member of the funder’s WASH Team. All views expressed in the paper are solely those of the authors and not necessarily those of the WVI nor its WASH Team. The WASH Team provided review of research tools but had no role in the data collection and analyses, preparation of the manuscript, and publication thereof. JBT supported with research design, independent reviews and editing of the writeup.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The relevant data generated and analysed during this study is included in the article as much as possible. However, for reasons of contractual compliance, we as authors are unable to share the raw data and we believe that a reasonable request on data acquisition could be made to the funder by contacting World Vision through the Senior Programme Manager (bnorgbe@worldvision.org).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.