
Abstract
To systematically evaluate the effects of Pain Coping Skills Training (PCST), both as an isolated intervention and in combination with other therapeutic approaches, on the quality of life in individuals with osteoarthritis (OA). A systematic and meta-analyses were performed using review manager (RevMan) version 5.4. Search was conducted using the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, PubMed, and Web of Science (WoS) databases. Selected articles comprised randomized-controlled trials (RCTs) which evaluated PCST alone or in combination with other treatments measuring quality of life (QoL) as a primary or secondary outcome. Only articles which had study populations with a mean age ≥50 years, with knee or hip osteoarthritis (OA) were included. Data were extracted, minimal detectable change (MDC) and effect sizes were calculated, meta-analysis was performed using random effects models, and heterogeneity was assessed with the I2 statistic. Of the 12,284 titles identified initially; only seven full text articles met the inclusion criteria and were selected. Selected articles varied in type of intervention and methodological quality. The average quality assessment score was 13, implying good overall quality. Significant improvements in pain and QoL in favor of PCST were reported by all included studies. PCST improves QoL-related outcomes in individuals with OA, particularly when combined with complementary therapies. However, inconsistent findings across heterogeneous studies highlight the need for larger, standardized trials to confirm its effectiveness and long-term impact.
Plain Language Summary
This study looked at whether a type of mental health treatment called Pain Coping Skills Training (PCST) can help people with osteoarthritis (OA) feel better and enjoy life more. PCST teaches people ways to deal with long-term pain by changing how they think and respond to it. Researchers reviewed many earlier studies to find out if PCST works, either on its own or when used along with other treatments. They focused on people aged 50 and older who had knee or hip osteoarthritis. Out of over 12,000 studies they found, only seven met their strict standards and were included in the final review. These studies showed that people who took part in PCST reported less pain and a better quality of life. The overall quality of these studies was good. Conclusion: PCST helped people with osteoarthritis to improve their quality of life. It can be a useful treatment option that supports both the body and the mind.
Introduction
Osteoarthritis (OA) is a degenerative condition resulting from the gradual progressive breakdown of joint cartilage over time. It is often referred to as the “wear and tear” of the joints, and can affect the knee, hip, or other joints (Loeser et al., 2012). The risk of developing OA increases with age, and other risk factors including female gender, obesity, hypertension, and having a lower level of education (Fu et al., 2022; Lee et al., 2019). The global prevalence of knee OA in individuals aged 40 years and above, from 2017 to 2020, is 22.9%. The global incidence of hip osteoarthritis is also rising, with the total number of cases increasing from 0.74 million to 1.58 million between 1990 and 2019 (Graham et al., 2022). This growing incidence poses a significant burden to the healthcare resources, as the utilization of healthcare services is reported to be high in this population (Hunter et al., 2008; Kamsan et al., 2021).
Pain is the primary symptom of OA, while swelling, reduced range of motion, and muscle weakness are other possible symptoms. Managing pain is, therefore, required to improve physical function and mobility and promote an overall better quality of life (QoL) for individuals living with OA (Kamsan et al., 2020). Recent study revealed that coping strategy for OA is crucial in avoiding functional dependency (Ismail et al., 2017). Pain coping skills training (PCST) is a non-pharmaceutical method of pain management which helps the individual develop cognitive and behavioral skills, hence promoting their sense of pain control. This allows individuals to be more engaged in their own pain management when used in tandem with standard treatment. Bennell et al. (2016) describes PCST as a well-organized cognitive behavioral treatment for disease-related pain disorders which focuses on the self-management approach. Despite the promising nature of PCST, there is a limited number of studies specifically evaluating its effectiveness among individuals with OA. This systematic review aims to address this gap by focusing exclusively on PCST and its effects on knee and hip OA, as these joints are among the most affected.
Numerous interventional studies and systematic reviews have identified PCST as an effective intervention for managing pain. Most review articles on PCST have selected pain and function as their primary outcomes (Bennell et al., 2017). However, limited studies reviewed the impact of PCST among OA individuals. This review study, therefore, systematically evaluated all eligible studies which included QoL-related outcomes following PCST in individuals with knee or hip OA.
Methods
Inclusion and Exclusion Criteria Considered for This Systematic Review
This review study was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO); CRD42021295342. Protocol was not prepared. There were slight changes in the title as none of resilience outcomes were found during the search. Thus, we changed the title from the effect of pain coping training on resiliency and quality of life among individual with osteoarthritis: A Systematic Review to the effect of pain coping training on quality of life-related outcomes among individuals with osteoarthritis: A systematic review and meta-analysis.
The Participants, Intervention, Comparison, Outcomes, and Study Design (PICOS) framework guided the development of the objectives and search strategy. Inclusion criteria for this review specified that all randomized controlled trials (RCTs) published in English were required, evaluating pain coping mechanism interventions, including Pain Coping Skills Training (PCST) either alone or in combination with other interventions, with objective QoL-related outcomes. These outcomes included self-efficacy (ASES), psychological status (depression, anxiety, and stress), coping strategies questionnaire (CSQ), assessment of quality of life (AQoL), and other related measures as either primary or secondary outcomes. Only studies reporting a mean age of participants of 50 years and over were included. Studies that included participants with wrist or spine OA were excluded from this review.
Search Strategy
The Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, PubMed, and Web of Science (WOS) were systematically searched using the keywords: (Pain Coping Skills OR Pain Coping Skills Training OR Pain Coping Mechanism OR Pain Management Skills OR Self-Management Skills) AND (Knee Pain OR Osteoarthritis OR Osteoarthritic Pain OR Knee Osteoarthritis OR Hip Osteoarthritis OR Joint Pain) AND (Resilience OR Quality of Life OR Psychological Resilience OR Cognitive behavioural OR Psychological Distress OR Kinesiophobia). We also manually screened the reference lists of the selected articles and relevant publications for potentially relevant articles.
Data Extraction and Analysis
The title, abstract, and descriptors of identified research were evaluated for inclusion by one review author (SSN). Two authors (SSN and SM) thoroughly examined potentially eligible RCTs for inclusion from the null text, as well as any disagreements were resolved through discussion. Titles and abstracts were first screened by one author (SSN). The full text of articles of potentially suitable articles was then examined by two authors (SSN and SM) and any disagreements resolved through discussion. Data from selected articles were extracted independently by two authors using a standardized data extraction form. Conflicts of the articles were resolved by discussion with a third person (DB). To evaluate the effect of the interventions, the change in outcome scores was compared against the estimated minimal detectable change (MDC) which has been published in previous validation studies. If this was not available, MDC was calculated using the formula: The standard error of the mean (SEM) multiplied by 1.96 and √2 for 95% CI (Supplemental Figure 1.0).

or

Effect sizes were manually calculated using formula: taking the difference between the two groups; (the mean of treatment group minus the mean of the control group) and dividing it by the standard deviation of control groups, such as below:

Meta-analysis of Quality-Of-Life Related Outcome Measure
The meta-analyses that examined the effects of PCST on QoL were performed using review manager (RevMan) version 5.4. Analysis of changes in quality of life-related outcome measures generated from AQoL, CSQ, and ASES data as improvement in quality of life was also conducted. The difference in change score between the intervention and control groups for each relevant outcome measure was calculated and divided by the pooled standard deviation using the random effects model. The standard mean difference (SMD) and associated 95% confidence interval were used to calculate the mean differences for all the data. The I2 statistic was used to examine heterogeneity in particular chosen studies. To make sure that all scales are pointing in the same direction, adjustments were made to negative values by multiplying by 1.
Minimal Detectable Changes (MDC)
MDC was calculated using the standard error of mean of random samples drawn from the original population (SEM) and interclass correlation coefficient (ICC) in formula mentioned above. Minimal Detectable Change (MDC): The MDC values were calculated for various outcome measures. The MDC represents the smallest amount of change in a measurement that can be considered beyond measurement error. The MDC values for the different outcome measures were calculated in Table 1 below.
Effect of PCST on Quality of Life Related Outcomes.

Note. Bold indicate significant at p value < 0.05.
Paired t-test.
Independent sample t-test.
Effect size, small effect < 0.40, medium effect, 0.4–0.75, large effect > 0.75. ** Effect size calculated using formula.
Quality Assessment and Publication Bias
The actual PEDro score includes 10 items: random allocation, concealed allocation, baseline comparability, blind participants, blind therapist, blind assessors, adequate follow-up, intention-to-treat analysis, between-group comparisons and point estimates and variability. Then, seven items were added to provide further details on the quality of the research. These additional questions added in quality assessment enquired about the inclusion of sample size calculation using multivariate estimation calculation, use of repeated measures multivariate analysis with planned post-hoc testing, adequacy of sample size, medium to large statistical power, use of validated outcome measures which were responsive to change, use of targeting interventions to measure outcomes, sufficient dose of intervention delivered, and reporting of clinical significance of statistically significant results. Publication bias was assessed using funnel plot.
Ethics Approval
The study is a systematic review study and requires no ethics approval from university.
Result
Literature Search
The initial keyword and cross-referencing detected 12,387 published documents, of which 12,355 were eliminated following removal of duplicates through title and abstract review. A total of 32 papers were found to be relevant for full text analysis. Twenty-five papers were excluded as the mean age of participants were below 55 years, lacked focus on pain (n = 4), addressed secondary illnesses not related to OA (n = 3), evaluated treatment that was not PCST (n = 10), not reported in the English language (n = 2), protocol paper (n = 1) and qualitative design (n = 1). A total of seven full-text articles were, therefore, retained and included for subsequent data extraction and meta-analysis (Supplemental Figure 1).
Participants
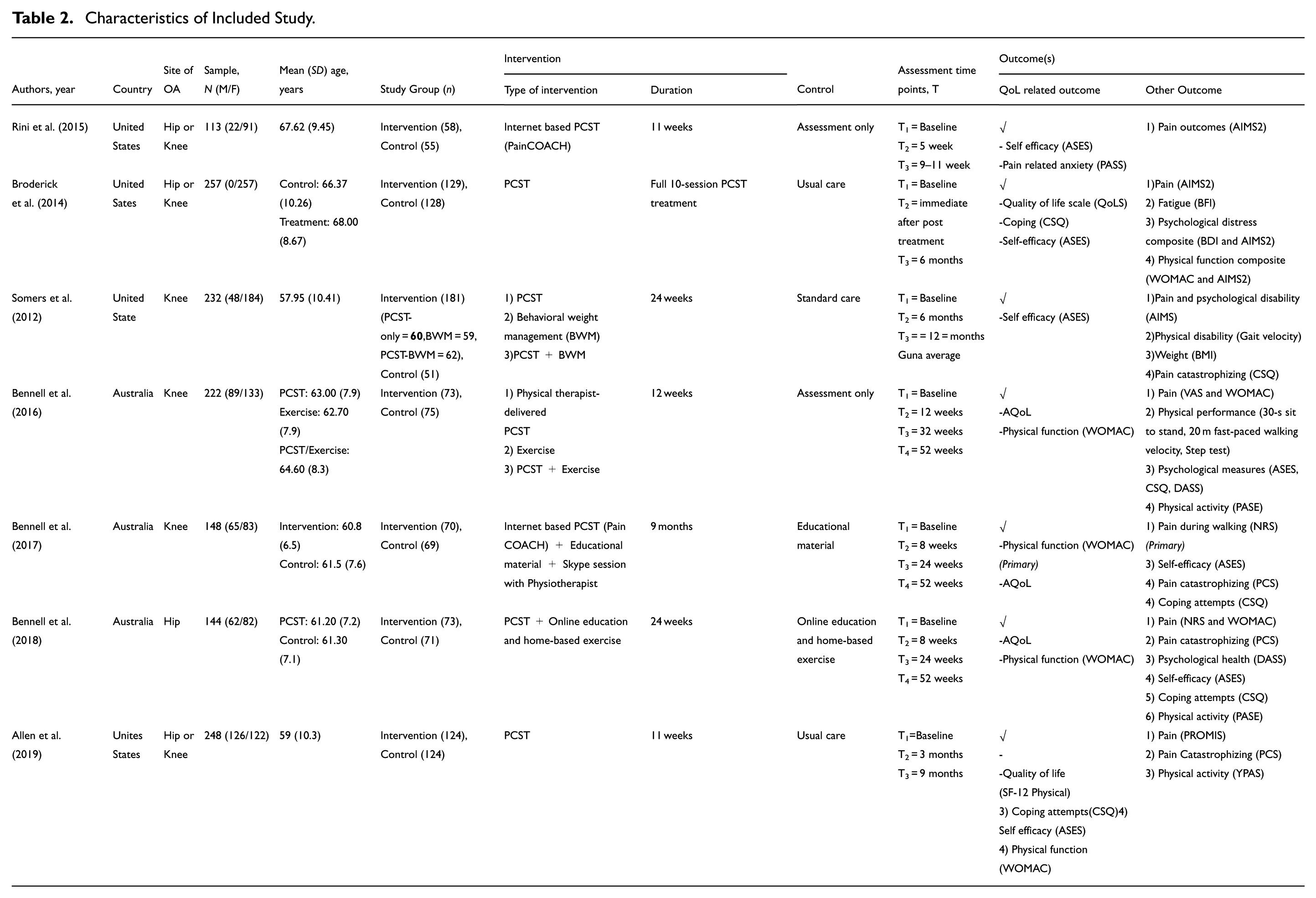
The seven selected articles published between 2012 and 2019 included a total of 1,364 participants (range = 144–257) with either hip or knee OA and mean age of 55 years old and above. Included studies were conducted in the United States (n = 4) and Australia (n = 3).
Intervention
Intervention and follow-up periods occurred from between 11 weeks to 13 months. PCST or PCST along with physical therapy were used in the research. Four studies evaluated PCST alone, whilst the rest delivered PCST in combination with exercise therapy or behavioral weight management in the other three studies. Four studies evaluated PCST delivered face-to-face while the remaining three delivered PCST virtually either through a web-based application or through telephone calls (Table 2).
Characteristics of Included Study.
Assessment tools
The outcomes included were pain, symptom severity, pain anxiety, arthritis self-efficacy, physical activity, and arthritis impact. Two studies used an 11-point numerical rating scale (NRS; Bennell et al., 2017, 2018) for osteoarthritic pain, six studies used the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC; Allen et al., 2019; Bennell et al., 2016, 2018; Broderick et al., 2014; Melo et al., 2023; Somers et al., 2012), all studies used the Arthritis Self-Efficacy Scale (ASES; Allen et al., 2019; Bennell et al., 2016, 2018; Broderick et al., 2014; Lee et al., 2019; Melo et al., 2023; Somers et al., 2012), one study used the Pain Anxiety Symptoms Scale (PASS; Fu et al., 2022), two studies used Physical Activity Scale for Elderly (PASE; Allen et al., 2019; Melo et al., 2023), one study used the Brief Pain Inventory (BPI; Somers et al., 2012), one research used Arthritis Impact Measurement Scales (AIMS; Bennell et al., 2016), two studies used the Arthritis Impact Measurement Scales 2 (AIMS2; Fu et al., 2022; Somers et al., 2012), and one study used the 100 mm Visual Analog Scale (VAS; Melo et al., 2023). Quality of life were measured using the Assessment of Quality of Life (AQoL) tool by three studies (Allen et al., 2019; Bennell et al., 2018; Singh et al., 2018), while the Quality of Life Scale (QoLS; Somers et al., 2012), the 12-item short form health survey (SF-12; Broderick et al., 2014) and the Yale Physical Activity Survey (YPAS; Broderick et al., 2014) were employed by one study. Coping ability was measured using the Coping Strategies Questionnaire (CSQ; Allen et al., 2019; Bennell et al., 2016, 2018; Broderick et al., 2014; Melo et al., 2023; Somers et al., 2012) (six studies) and the Pain Catastrophizing Scale (PCS; Allen et al., 2019; Bennell et al., 2018; Broderick et al., 2014; Melo et al., 2023) (four studies). Psychological status was measured by three studies with two studies using the Depression, anxiety, and stress test (DASS21; Allen et al., 2019; Bennell et al., 2016; Broderick et al., 2014; Melo et al., 2023; Somers et al., 2012) and one study utilized the Brief Fatigue Inventory (BFI; Somers et al., 2012).
Intervention Effects
PCST Alone
Allen et al. (2019) showed that 9 months after training, ASES score and CSQ total coping attempts of the PCST group were significantly improved with p = .032 and p = .016 respectively compared to the control group (waiting list control group) which has p-value of p = 1.00 and p = .198 respectively (Broderick et al., 2014). Although ASES was significant, the change over time did not met the MDC and also have a small effect size of 0.33. In contrast, the CSQ exceed the MDC despite the small effect size of 0.34. Study by Rini et al. (2015) showed no significant improvement in pain anxiety outcome but PCST participants showed higher self-efficacy (ASES) for pain management with p = .012, moderate effect size with 0.43 and did not met the MDC (Fu et al., 2022). While Broderick and colleague reported significant impact on the outcome of quality of life (QoL) and arthritis self-efficacy (ASES) with p < .01 and p = .082 respectively. However, only QoL exceeded the MDC with a small effect size of 0.11. Bennell et al. (2018) found that PCST has no significant impact on the QoL of individuals with OA on the hip with p = 1.00 in both intervention and control group in the Standardized Education and Exercise Program for People with Persistent Hip Pain (HOPE trial). It also did not met the MDC with a small effect size with 0.00 (Allen et al., 2019; Bennell et al., 2017; Table 1).
PCST in Combination With Other Intervention
Four out of seven studies combined PCST with other interventions with three such studies reporting significant positive impact on QoL-related outcomes. Bennell et al. (2016) showed that physical therapist delivered PCST in combination with exercise, had a greater effect on QoL measured with the AQoL-6D, self-efficacy and coping strategies compared to exercise alone at week 32 (p < .01) and week 52 (p < .05; Melo et al., 2023). The effect sizes of AQoL-6D and self-efficacy were 0.38 (small) and 1.24 (large), respectively and both had not met the MDC. Meanwhile, coping strategies with the effect size of 0.61 (moderate) met the MDC (Melo et al., 2023). Another study, Bennell et al. (2017) found that with web-based PCST delivered in combination with exercise after 3 months, both quality of life and self-efficacy (ASES) had improved in the intervention group (PCST + Exercise) with mean changes of −0.1 and −0.9, respectively, while in the control group (Exercise), the mean change was 0 and −0.3 (Allen et al., 2019). Following 9 months of therapy, QoL improved similarly, with greater improvements in, self-efficacy, mean change of −0.8 for the intervention group and −0.4 for the control group (p = .018), effect size 0.50 (moderate), while self-efficacy did not meet the MDC but QoL exceeded the MDC (Bennell et al., 2018). Somers et al. (2012) found that combining PCST with Behavioral Weight Management (BWM; M = 1.0) resulted in better improvement in physical ability than BWM-only (M = 1.5) or PCST-only (M = 1.5; Bennell et al., 2016). The effect size of self-efficacy combined with BWM were 0.55 (moderate) and below the MDC. In contrast, the effect size of PCST alone was 0.77 (large), exceeding the MDC (Bennell et al., 2016; Table 1).
Meta-analysis of Outcome Measures
Meta analyses of study results were possible for the seven studies. Three QoL-related outcome measures—the Assessment of QoL (AQoL; Supplemental Figure 2.1), the Assessment of Self-Efficacy (ASES; Supplemental Figure 2.2), and the Coping Strategies Questionnaire (CSQ; Supplemental Figure 2.3)—were the focus of subgroup analyses. The aggregated results from the five RCTs that assessed QoL revealed a substantial improvement in QoL (SMD = 1.31, 95% CI [0.46, 2.16], p = .003, p for heterogeneity < .00001, I2 = 97%). The same trend was found in the pooled results of self-efficacy outcome measures, which were reported in seven studies, and coping strategy outcome measures, which was disclosed in five studies, with (SMD = 1.36, 95% CI [0.33, 2.39], p = .010, p for heterogeneity < .00001, I2 = 98%) and (SMD = 2.49, 95% CI [1.99, 2.99], p < .00001, p for heterogeneity < .0001, I2 = 89%) respectively. The pooled results for all seven studies that used these three types of outcome measures suggested that PCST significantly improves QoL in individuals with knee OA. It is important to acknowledge that, despite the varying scales used across these studies, they measure the same construct and can be effectively pooled together for analysis.
Methodological Quality Assessment and Publication bias
Table 3 contains a summary of the quality component checklist adapted from the PEDro scale and Table 4 showed score of the additional quality assessment questions as described above. The total score for PEDro scale and the additional quality assessment was 10 and seven respectively. The average PEDro score and additional quality assessment score was eight (range = 5–10) and six (range = 5–7) respectively, suggesting that high-quality RCTs were selected. The use of the PEDro score provides a standardized assessment of the methodological quality of studies, focusing on internal validity and statistical rigor, while additional questions were included to address aspects not fully covered by the PEDro scale, ensuring a more comprehensive evaluation of study quality. The funnel plot in Supplemental Figure 3 suggests asymmetry, with more small studies showing positive effects, especially for self-efficacy, indicating potential publication bias.
PEDro Scale.

Additional Quality Assessment.

Discussion
This review demonstrates that Pain Coping Skills Training (PCST) has the potential to improve quality-of-life (QoL) related outcomes in individuals with osteoarthritis (OA), though findings were inconsistent. Improvements in pain and physical function were frequently reported, but these did not always correspond with measurable gains in QoL. Some studies further showed that greater improvements were achieved when PCST was combined with other therapeutic approaches, such as physical therapy or behavioral weight management, compared with PCST alone. Variability in study design, intervention delivery, and the QoL measurement tools used contributed to these inconsistencies.
OA affects overall well-being by combining physical symptoms with psychological consequences that reduce QoL (Fonseca-Rodrigues et al., 2021; Singh et al., 2018). Pain and stiffness are closely linked to depression and anxiety, while self-efficacy serves a protective role in coping but may be weakened by catastrophizing or self-doubt (Wang et al., 2021). These links highlight the need for psychological approaches alongside physical interventions. PCST is promising because it addresses both domains; however, improvements in QoL were not consistently observed (Estoque et al., 2019). This may reflect the multifaceted nature of QoL, which extends beyond pain and coping, as well as the heterogeneity of included studies that applied diverse measurement tools with varying sensitivity and focus (Murphy et al., 2008).
It is possible that the benefits of pain coping mechanisms are transient and may not translate into sustained changes in daily life. Alternatively, while participants may have adopted healthier habits, these adjustments may not have been perceived as improvements in QoL, particularly if they required giving up previously valued but less healthy lifestyles. Moreover, the specific coping strategies employed can influence activity levels and behavioral patterns, which may inadvertently offset potential QoL gains. Previous research has also shown that different coping strategies can be associated with either greater or diminished physical activity levels and activity patterns, which may at times negate the purpose of managing pain (Estoque et al., 2019; Hasenbring & Verbunt, 2010; Murphy et al., 2008, 2012). Combination therapies may overcome some limitations seen with PCST alone by addressing multiple dimensions of QoL (physical, psychological, lifestyle factors).
Somers et al. (2012) and Bennell et al. (2016) showed that PCST combined with BWM or physical therapy exercise improved pain, physical impairment, and physiological disability. The effectiveness of combination therapy above that of the PCST alone may be attributed to the presence of core pain coping training, with additional treatment such as the provision of a BWM module that eventually led to weight loss of nearly 1 kg overall which helped reduce load-bearing at the knee joint. Additionally, physical therapy exercises present challenges that help individuals learn to cope with discomfort and eventually improve their QoL. Thus, the combination of PCST to other treatments might have greater impact than PCST alone or other treatments alone.
The meta-analysis indicated that participation in PCST was associated with a significant overall improvement in QoL among individuals with knee OA. Subgroup analyses of three QoL-related outcome measures (Assessment of QoL, Coping Strategies Questionnaire, and Assessment of Self-Efficacy) also showed positive associations with well-being, although these tools capture distinct but complementary aspects of health. The pooled results from RCTs demonstrated statistically significant improvements across QoL, self-efficacy, and coping outcomes, suggesting that PCST contributes meaningfully to patient-reported well-being (Marquez et al., 2020). Nevertheless, the magnitude of effect varied across studies, likely reflecting differences in intervention delivery, participant characteristics, and the sensitivity of the measurement tools employed. Collectively, these findings support PCST as a promising intervention for enhancing QoL in knee OA, while also underscoring the influence of study heterogeneity on outcome consistency.
Self-efficacy was the most frequently studied QoL outcome. Three out of seven studies used the health related or disease-specific QoL measurement tools SF12 and AQoL respectively. Self-efficacy reflects a patient’s perception of their function and overall QoL. This review suggests that a bio-psychosocial approach to managing uncontrolled pain, which empowers patients to engage in self-care and enhance their daily activities, may be effective. A comprehensive QoL measure should ideally balance physical health, psychological well-being, and social aspects. While tools like AQoL and SF-12 are well-rounded and validated, integrating a tool like YPAS may provide additional valuable insights into the physical activity limitations common in osteoarthritis, offering a more holistic view of the patient’s quality of life.
The included studies demonstrate varying effect sizes for outcome measures with most of them has high effect sizes exceeding the MDC calculated, indicating the potential effectiveness of certain interventions in improving self-efficacy, QoL, and coping strategies. These findings highlight the importance of considering these measures when evaluating the impact of interventions on individuals with the specific conditions studied.
Limitation and Implication
The systematic review and meta-analysis were limited by the small number of studies which fulfilled the objective and the limited information reported by individual included studies. While best practices in systematic review were followed, publication and language bias could influence its accuracy. Although measures were used to reduce biases, our search was limited to English language publications. High level of heterogeneity reflects the substantial variation in study populations, interventions, and measurement tools. Differences in patient characteristics (e.g., age, severity, comorbidities), intervention types, and cultural contexts likely drive this variability. Moreover, methodological inconsistencies, such as variations in study design and risk of bias, further complicate the comparison of outcomes. These factors underscore the challenge in drawing unified conclusions from such diverse studies, emphasizing the need for more standardized approaches in future research. Future study also should explore resilience role as a moderating factor in sustaining long-term adaptation to pain and enhancing quality of life in osteoarthritis remains underexplored despite growing evidence of its protective influence in chronic illness management.
This systematic review and meta-analysis demonstrate the effectiveness of PCST in reducing pain and QoL among individuals with OA. Clinicians should be trained in delivering PCST as part of a multidisciplinary approach, ensuring comprehensive care that addresses both physical and psychological components of pain. Based on current evidence, PCST for osteoarthritis OA should be delivered through structured programs spanning approximately 10 weeks, incorporating education, coping skills practice, and home-based exercises to support self-management. Both individual and group formats are appropriate, and telehealth delivery can be considered to increase accessibility. Clinicians are encouraged to integrate PCST with complementary therapies such as body weight management or physical therapy, which have shown additional benefits in reducing joint load, enhancing physical function, and improving quality of life. Patient selection is important, with PCST best suited for those with moderate to severe OA, significant pain, and functional limitations, who also demonstrate adequate cognitive capacity and emotional readiness to engage in behavioral change. Individuals with severe cognitive or psychiatric conditions should be carefully evaluated before inclusion. Tailoring PCST delivery and embedding it within a multimodal approach may optimize outcomes and support its integration into routine clinical practice. From a policy perspective, it is crucial to include PCST as a recognized, reimbursable intervention in clinical guidelines for OA management. This would ensure broader access to effective, non-pharmacological treatments for patients, especially those in underserved areas. Furthermore, continued research is needed to evaluate the cost-effectiveness and long-term benefits of PCST, as well as its potential for wider implementation through digital platforms. In summary, integrating PCST into routine OA care could significantly enhance patient outcomes by improving pain management and QoL, while reducing dependence on pharmacological treatments. Health policies should support the inclusion of PCST in care guidelines, ensuring accessibility and affordability for all patients.
Conclusion
This review demonstrates that PCST can improve QoL-related outcomes in individuals with OA, with the greatest benefits observed when delivered alongside complementary interventions such as physical therapy or behavioral weight management. However, inconsistencies across studies, particularly in QoL measurement tools and intervention delivery, limit the ability to draw firm conclusions. Larger, high-quality RCTs using standardized QoL measures and longer follow-up are needed to clarify the durability of benefits and the role of PCST within multimodal care. These findings highlight the growing importance of integrating psychological and lifestyle-focused approaches into OA management, supporting the shift away from predominantly pharmacological and invasive strategies toward more holistic, patient-centered care.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251396391 – Supplemental material for The Effect of Pain Coping Training on Quality of Life-Related Outcomes Among Individuals With Osteoarthritis: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-sgo-10.1177_21582440251396391 for The Effect of Pain Coping Training on Quality of Life-Related Outcomes Among Individuals With Osteoarthritis: A Systematic Review and Meta-Analysis by Siti Sarah Norman, Azianah Mohamad Ibrahim, Siti Salwana Kamsan, Sawal Hamid Md Ali, Nor Hamdan Mohamad Yahaya, Caryn Chan Mei Hsien, Dayang Balkis Md Ramli, Noorlaili Mohd Tohit, Norhayati Ibrahim, Suzana Shahar, Tan Maw Pin and Sumaiyah Mat in SAGE Open
Footnotes
Acknowledgements
The data used in this systematic review was taken from academic papers and databases that are openly accessible. In the reference section, all sources are appropriately acknowledged in the reference section.
Ethical Considerations
This is a systematic review including studies based on human participants. All the included papers had ethical approval, consent to participate and consent for publication authorized by the participants.
Author Contributions
SSN and SM conceptualized, analyzed and interpreted the data, SSN prepared the first draft of the manuscript. All authors reviewed the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Universiti Kebangsaan Malaysia Dana Impak Perdana (DIP-2024-025), which also provides salary support for Azianah Mohamad Ibrahim and by the Geran Universiti Penyelidikan, Universiti Kebangsaan Malaysia (GUP-2021-058).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.