
Abstract
Vaccination has long been a key part of pandemic response; yet vaccine hesitancy still poses major challenges for immunization efforts. The COVID-19 pandemic exposed the world’s lack of preparedness to contain the virus and mitigate its impact. In the U.S., despite mandates and social restrictions, the goal of reaching herd immunity was not achieved. At the same time, dependence on digital media platforms—especially social media—grew, shaping public views on the pandemic and vaccines. This study explored how vaccine hesitancy was influenced by a mix of behavioral and informational factors observed during the H1N1 pandemic. Based on interviews from mid-2023, which was during the post-emergency stage of the pandemic but before big changes in public health policy, the study used a practical qualitative approach to understand the experiences of 30 social media–active participants across the U.S. Results showed that views on vaccine safety and effectiveness, personal health risk assessments, past vaccination habits, media credibility, and personal independence played key roles. While grounded in a particular moment of social and institutional flux, the study captures enduring insights into vaccine attitudes that inform both retrospective understanding and future preparedness. Its findings reflect not only the temporality of public sentiment but also the underlying behavioral drivers that persist across contexts. With the restructuring of federal public health systems and a move toward more localized vaccine communication, these insights continue to offer a valuable understanding of trust, behavior, and future pandemic planning.
Keywords
Introduction
The COVID-19 pandemic severely disrupted global health and social services, with the USA experiencing 6.3 million hospitalizations and over 1.1 million deaths, leaving a lasting impact (Kloft & López-Cevallos, 2024) and influencing public sentiment and institutional responses through 2023. The country’s economy also suffered a significant setback; many businesses shut down, and people lost their jobs. Historically, vaccination has been considered a pillar of recovery during infectious disease health crises (Lopalco & Tan, 2016), a perspective that strongly influenced early COVID-19 frameworks in 2020. The World Health Organization (WHO) estimated that vaccinations have prevented at least 154 million deaths between 1974 and 2024 (Shattock et al., 2024), based on which vaccination has been considered a safer way to accomplish herd immunity, a “concept in immunology used to describe the resistance to the spread of a contagious disease within a population or a herd” (Xia et al., 2020). Lessons learned from eradicating smallpox underscored the value of international cooperation, surveillance, and vaccination, demonstrating that clear communication, rapid response, and community engagement are crucial for global health initiatives combating infectious diseases (Heymann & Wilder-Smith, 2020). Therefore, during the COVID-19 crisis, to increase immunity among the people in the USA and decelerate the virulence of the disease, everyone was strongly urged to vaccinate once the COVID-19 vaccines were widely available, supported by masking and social distancing regulations. To counter the impact of social restrictions during the pandemic, people relied on digital media to stay current and foster social connections (Dé et al., 2020). During the COVID-19 crisis, public frustration over shifting guidance from health agencies and government institutions about the enforced social restrictions, the uncertainty about the effectiveness and safety of the vaccines, and their prevalent perceptions and beliefs consequently contributed to the dissemination of misinformation and disinformation on social media platforms (Reno et al., 2021). Not everyone chose vaccination or supported masking and social distancing (Khubchandani et al., 2021). Coincidentally, COVID-19 infections caused by multiple virus variants continued to increase nationwide, with individuals who declined vaccination or participated in social restrictions being perceived as contributing to the upsurge in infections (Levin & Bradshaw, 2022; Shiehzadegan et al., 2021). Given the dramatic rise in social media engagement during the pandemic, it became crucial to ask: Were those who declined vaccination influenced primarily by their digital interactions, or were other behavioral and contextual factors at play? During the 2009 H1N1 pandemic, Mills et al. (2020) found that the following behavioral factors underpinned vaccination uptake: (1) perception of risk and severity of the disease; (2) trust and confidence about the efficacy and safety of the vaccines against the disease; (3) barriers and access to vaccines; (4) sources of information about the pandemic and the vaccines; and (5) past vaccination behavior. Conversely, did these factors also influence people to not opt for vaccines during the H1N1 pandemic? Not opting for vaccination during a health crisis is not a new phenomenon (Razai et al., 2021). People have previously avoided vaccines, such as the routine influenza vaccine and the measles, mumps, and rubella (MMR) vaccines (Dubé et al., 2013). Considering the potentially significant impact of this phenomenon on herd immunity (Neely et al., 2022), the WHO listed vaccine hesitancy among the world’s top 10 threats in 2019 (Wilson & Wiysonge, 2020). People who demonstrate this behavior “… may refuse some vaccines, but agree to others, delay vaccines, or accept vaccines but are unsure of doing so” (Larson et al., 2014) and are on a continuum, with those either strongly for or against vaccines at opposite extremes (MacDonald et al., 2015). Although the U.S. health and economy largely stabilized by 2024, the period preceding this, particularly 2023, represents a pivotal point for understanding vaccine hesitancy prior to the widespread decentralization of public health infrastructure and changes in federal health authority (Gostin et al., 2023; Hodge, 2023). Additionally, even post-COVID-19, participation on social media platforms continues to grow (8% increase in 2024; Chaffey, 2024), with social media activity remaining an integral lifestyle choice for many in the US.
This study, therefore, aimed to document the lived experiences of social media users in 2023—a year marked by rising skepticism, social fragmentation, and changing perceptions of institutional authority—focusing on the behavioral and informational factors that influence vaccine hesitancy. Considering the increased reliance on social media during the COVID-19 pandemic, this study expanded on the five behavioral dimensions identified in previous research by incorporating the role of social networks, reflecting their heightened relevance during the pandemic's digital surge to guide its methodology, address its problem and purpose, and answer the following research question (RQ):
Literature Review
COVID-19 Vaccine Hesitancy
Researchers investigating vaccine hesitancy during the COVID-19 pandemic faced challenges due to lockdowns, requiring a shift to virtual platforms like Zoom, which introduced technical barriers, sampling biases, and reduced engagement (Goje & Kapoor, 2024; Russ et al., 2024; Sharp et al., 2024). Researchers refined virtual interview techniques to maintain rigor and protect confidentiality despite these limitations (Russ et al., 2024). During the COVID-19 pandemic in the USA, people’s political affiliations, especially those who voted Republican, were negatively correlated with their intentions of supporting vaccinations and COVID-19 mandates (Fridman et al., 2021). During the COVID-19 pandemic, vaccine mandates affected large companies’ healthcare workers, government employees, and private-sector staff, reducing individual agency in vaccination decisions (Goje & Kapoor, 2024; Russ et al., 2024). CMS regulations required vaccination for 10.4 million healthcare employees, while the OSHA mandate impacted 84 million private-sector workers and 3.5 million federal employees, including military personnel. Many faced job loss or disciplinary action if they refused vaccination despite medical and religious exemptions, significantly influencing uptake in high-exposure professions (Sharp et al., 2024). Khubchandani et al. (2021) found that the perceived COVID-19 threat also strongly predicted COVID-19 vaccine hesitancy. Troiano and Nardi (2021) found that individuals expressing vaccine hesitancy were primarily concerned that the vaccines were too dangerous and produced in a rush. COVID-19 vaccination rates in the U.S. varied across demographics. Overall, 81% of adults received at least 1 dose, with 90% of individuals aged 65+ vaccinated compared to 67% of those aged 18 to 29 (Eitze et al., 2024). Urban areas had higher vaccination rates, exceeding 85% coverage, while rural regions lagged at 605 to 65% (Russ et al., 2024). Lower-income communities reported vaccination rates below 55%, reflecting access barriers and healthcare inequities (Aw et al., 2021; Fridman et al., 2021). Similarly, Neely et al. (2022) observed that the three most common reasons for holding off a COVID-19 vaccine were concerns about (1) the potential side effects, (2) the speed-to-market, and (3) the lack of confidence in the vaccine’s effectiveness. Hence, considering the heightened utilization of social media during the COVID-19 pandemic, this study sought to determine how vaccine hesitancy by social media users in the USA is influenced by behavioral factors listed in the research question (RQ).
Perception of Health Risks Against a COVID-19 Infection
During the H1N1 pandemic, people with zero or low-risk perceptions about the disease did not have a reason to vaccinate, but those who were worried were more likely to vaccinate (Mills et al., 2020, p. 9). The same was observed in people supporting masking and social distancing measures during the COVID-19 pandemic (Fan et al., 2021). Eitze et al. (2024) also found that familiarity with Long-COVID experiences increased COVID-19 vaccination intentions (p. 5). However, just as in past health crises, exposure to anti-vaccination information had influenced risk perceptions (Betsch et al., 2018) during the COVID-19 pandemic in the USA as well; this was observed to be the case resulting from consuming misinformation on social media (Malecki et al., 2021). Hence, this study sought to determine how vaccine hesitancy by social media users in the USA during the COVID-19 pandemic is influenced by the perception of health risks against a COVID-19 infection.
Consumption of Sources of Information About the COVID-19 Pandemic and Vaccines
From H1N1 pandemic studies, Mills et al. (2020) found that consumers of information about the disease and the vaccine from healthcare providers, public health agencies, or the government perceived the vaccine as safe. Conversely, exposure to information about conspiracy theories can cause vaccine-hesitancy behaviors (Douglas et al. 2019, p. 11), with those inclined to consume anti-vaccine conspiracy theories showing a lower intention to vaccinate. Lockdowns significantly increased social media exposure, shaping public views on vaccines. Wu and Brennan-Ing (2023) noted that prolonged isolation led to higher reliance on digital platforms, reinforcing algorithmic biases and limiting access to diverse perspectives. Puri et al. (2020) argued that extensive anti-vaccine content on social media during the COVID-19 pandemic could have influenced vaccine hesitancy. Similarly, Reno et al. (2021) found that information sources consumed on social media could affect vaccine hesitancy attitudes toward COVID-19 vaccination, concluding that using social media could increase vaccine hesitancy. Younger individuals relied more on social media for COVID-19 information, while older adults preferred traditional news sources (Eitze et al., 2024). 91% of adults aged 18 to 29 used digital platforms, compared to 70% of those aged 65+, who favored TV, radio, and newspapers (Puri et al., 2020; Reno et al., 2021). Social media influenced vaccine hesitancy, with algorithmic filtering reinforcing biases and influencers amplifying selective viewpoints (Malecki et al., 2021; Wu & Brennan-Ing, 2023). Misinformation spread quickly, and fact-checking efforts remained inconsistent, raising concerns over social media accountability (Swire-Thompson & Lazer, 2020; Wilson & Wiysonge, 2020). Hence, this study sought to determine how vaccine hesitancy by social media users in the USA during the COVID-19 pandemic is influenced by their consumption of sources of information about the pandemic and vaccines.
Ineffectiveness and Unsafety of COVID-19 Vaccines
Aw et al. (2021) found that individuals expressing vaccine hesitancy strongly believed that COVID-19 vaccines were unsafe or ineffective. In 2020, people presumed that the vaccine development had a political impetus (“Operation Warp Speed”) while misinformation and disinformation were proliferating on social media (Mills et al., 2020, p. 10). In 2021, regulators linked AstraZeneca’s Vaxzevria to a rare blood clotting disorder, prompting 75 affected individuals to take legal action (Dyer, 2023). Barmada et al. (2023) linked SARS-CoV-2 mRNA vaccination manufactured by Pfizer to a cytokine-driven process that may cause heart tissue damage and fibrosis, offering insights into vaccine-related myocarditis and future vaccine development. Tunç and Çevirme (2024) found that healthcare professionals were also doubtful about the efficacy and safety of the COVID-19 vaccine and concerned about the side effects after vaccination. Wilson and Wiysonge (2020) showed a significant relationship between social media and public doubts about vaccine safety. According to Wu and Brennan-Ing (2023) the information overload on social media during the COVID-19 pandemic caused distrust in authority, leading to vaccine hesitancy. Hence, this study sought to determine how vaccine hesitancy by social media users in the USA during the COVID-19 pandemic is influenced by the perceptions about the ineffectiveness and unsafety of the COVID-19 vaccines.
Past Vaccination Behavior
Past vaccination behavior was one of the strongest predictors of vaccination during the H1N1 pandemic (Mills et al., 2020, p. 12). Similarly, past vaccine refusal, perceived risk of infection, and presence of comorbidities were confirmed as significant predictors of COVID-19 vaccine hesitancy (Reno et al., 2021). People who recognize vaccines’ role in eradicating smallpox and significantly reducing diseases like polio and measles tend to have greater trust in and acceptance of vaccinations (Kroese et al., 2024). Fan et al. (2021) concluded that past vaccination uptake behaviors had directly influenced COVID-19 vaccination uptake. Freeman et al. (2024) examined the effect of post-vaccination allergies on future vaccine hesitancy and found that most participants with negative perceptions declined future vaccination intentions. Hence, this study sought to determine how vaccine hesitancy by social media users in the USA during the COVID-19 pandemic is influenced by past vaccination behavior.
Influence of Social Networks
During the COVID-19 pandemic, perceptions of friends and relatives strongly predicted vaccination intentions (Husain et al., 2021; Yahaghi et al., 2021). Dubé et al. (2013) argued that the robust behavior of people who favored vaccine-uptake intentions on social media was a powerful driver of vaccine acceptance. Koban et al. (2023) observed a significant correlation between the intervention by healthcare experts in COVID-19 discussion groups on Facebook and the trust in public health institutions, improving vaccination intentions in individuals and others within their respective social networks. Sharp et al. (2024) found that the fear of adverse reactions from the vaccine, misinformation surrounding the pandemic and the vaccine, and external pressure to get vaccinated were significant factors that influenced COVID-19 vaccine hesitancy. Hence, this study sought to determine how social networks influence vaccine hesitancy by social media users in the USA during the COVID-19 pandemic.
Barriers and Difficulty of Access to COVID-19 Vaccines
A well-designed vaccination infrastructure and distribution chain of pharmacies offering convenient access to immunization during the H1N1 pandemic was crucial to promoting vaccination uptake (Mills et al., 2020). Conversely, COVID-19 vaccine hesitancy worldwide resulted from disparities in access, cost, and awareness of vaccines (Aw et al., 2021). Husain et al. (2021) also found availability, cost, location, and technological challenges measured up to be significant predictors for people to vaccinate (p. 8). Russ et al. (2024) explored vaccination influences impacted by healthcare inequities and logistical barriers in communities of racial diversity, poverty, political conservatism, and accessibility to healthcare and found that these resulted from perceptions of health risks, concerns about vaccine safety, mistrust of the medical system, and transportation challenges to vaccine appointments. Hence, this study sought to determine how barriers and difficulty of access to COVID-19 vaccines influence vaccine hesitancy by social media users in the USA during the COVID-19 pandemic.
This literature review showed that vaccination hesitancy by people in the USA during the COVID-19 pandemic was influenced by perceptions of health risks against a COVID-19 infection, consumption of sources of information about the COVID-19 pandemic and vaccines, ineffectiveness and unsafety of COVID-19 vaccines, past vaccination behavior, influence of social networks, and by experiences of barriers and difficulty in accessing COVID-19 vaccines. Determining how the above factors influence vaccine hesitancy would be pivotal for planning future health crisis remediation plans because vaccination is a pillar of recovery, and accomplishing herd immunity is mission-critical during any health crisis. Furthermore, with social media use integral to lifestyles in the current age, the impact of information disseminated and consumed on people’s intentions and behaviors would also be an essential consideration for the future.
Method
Methodological Approach
Philosophical worldviews are a set of beliefs which influence research practice and are hidden throughout a study (Creswell & Creswell, 2018, p. 5). To guide its qualitative design, this study adopted the pragmatist worldview, which, for Creswell and Creswell (2018), “arises out of actions, situations, and consequences rather than antecedent conditions,” collecting data through semi-structured interviews and analyzing it through coding and thematic analysis. These interviews elicited the essence (Creswell & Creswell, 2018, p. 13) of vaccine hesitancy in participants' lived experiences during the COVID-19 pandemic.
Participant Sampling and Recruitment
The sampling frame of this study was made up of U.S. residents 18 years or older who were actively using social media. Approval (Ref. No. 2023XXXXXXXX) was received from the Institutional Review Board (IRB) affiliated with the researchers’ institution to ensure no minors were recruited for the study. A survey crowdsourcing marketplace, CloudResearch® Connect™ (CRC), was leveraged to recruit participants using a non-probability sampling technique to frame a convenience sample. Based on a recommendation by Daniel (2012) for recruiting participants utilizing a non-probability sampling technique, 30 were interviewed. The sample size of 30 participants was selected based on data saturation, where additional responses yielded no new insights (Guest et al., 2006). Smaller samples allow for in-depth exploration of complex behaviors rather than broad generalization (Creswell & Creswell, 2018). Similar studies have used comparable sample sizes to maintain methodological rigor and feasibility (Morse, 2000; Patton, 2015). This selection ensured diverse perspectives while aligning with best practices for studying vaccine hesitancy. Interviews were conducted from late June 2023 through mid-July 2023 over “Google Meet” or “Microsoft Teams,” video-conferencing applications; a meeting link was shared with participants during the recruitment process. Although the video of the interviews was not recorded, the audio was recorded and transcribed by a third-party transcribing tool, “otter.ai.” The transcriptions and audio recordings were manually verified for accuracy. Informed consent was obtained from all participants before they were interviewed.
Instrumentation
The interview consisted of twelve open-ended questions (Table 1). A CloudResearch® Connect™ (CRC) project provided participants with the particulars of the interview and its purpose, assured confidentiality, and estimated 40 min for the interview. On a few occasions, the interviews ran longer.
Qualitative Interview Questions.
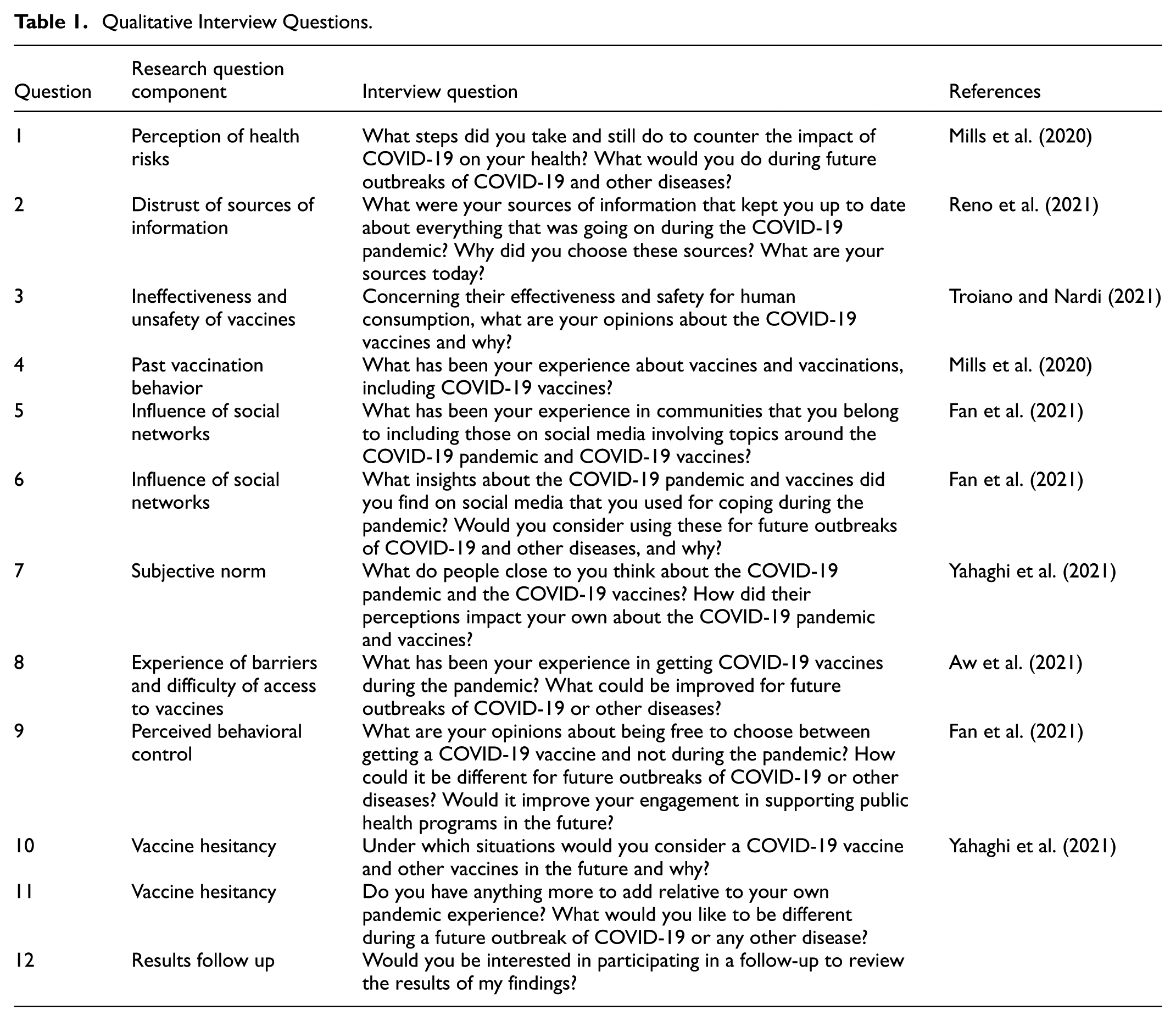
At the end of the interview, after participants had voluntarily consented to question 12 to review the summarized findings and confirm their alignment with their own experiences on vaccine hesitancy, they were paid $20 for their time on the interview.
Reliability, Validity, and Ethical considerations
Reliability and validity are key aspects of qualitative research, ensuring the study’s rigor and trustworthiness (Bell et al., 2022). To establish trustworthiness, this study applied several recognized strategies:
Credibility: Respondent validation was conducted to confirm that findings accurately represent participants’ experiences. A summary of the results was reviewed with seven participants at the end of the study.
Transferability: Thick descriptions of participants’ lived experiences were provided, following recommendations by Creswell and Creswell (2018, p. 200). Direct quotations from interviews have been included in the results section to enhance the richness and depth of qualitative insights.
Dependability: A research advisory committee oversaw data collection and analysis procedures to ensure methodological rigor. Complete records were maintained to support transparency and consistency (Bell et al., 2022, p. 365).
Confirmability: All documented steps and conclusions would be available for auditing if needed, aligning with best practices in qualitative research (Bell et al., 2022, p. 365).
This study supported ethical considerations by obtaining approval from the Institutional Review Board (IRB) affiliated with the researchers’ institution to ensure no minors were recruited. Although the participants were compensated for their time, participation was voluntary. The process was governed by strict confidentiality during and after the study, and no personal identification information was collected. Transcriptions were de-identified to protect participants’ identities and, along with the audio recordings, uploaded to a password-protected storage location on the cloud.
Data Analysis
The study used NVivo to organize and analyze the audio recordings and transcribe data collected using a transcription tool, “otter.ai.”Creswell and Poth (2018) recommend a lean coding technique that begins with a short list (five or six) of categories or codes (p. 190). Significant sentences and phrases from the transcribed interviews were categorized into five general themes identified through inductive thematic analysis, which helped form the basis of this study’s findings.
Results
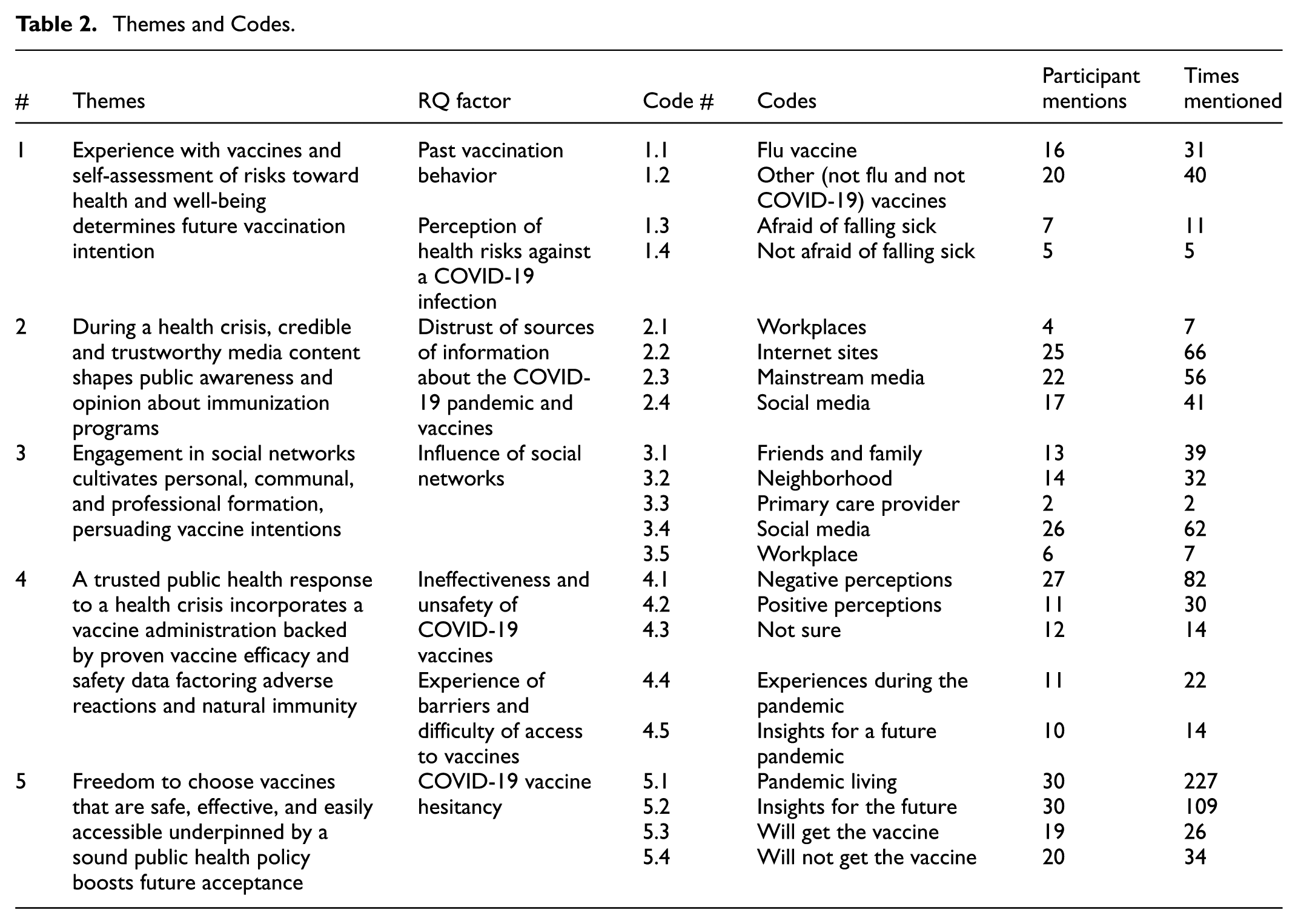
Out of the 30 participants recruited, fourteen were women (46.67%) and sixteen were men (53.33%). Four participants were aged 18 to 29 (13.33%), 14 were 30 to 49 (46.67%), 10 were 50 to 69 (33.33%), and 2 were 70 or older (6.67%). Sixteen participants were single (53.33%), eight were married (26.67%), two were widowed (6.67%), one was in a domestic relationship (3.33%), and three were divorced (10%). Eleven participants had no bachelor’s degree (36.67%), but nineteen had a bachelor’s degree or higher (63.33%). Fifteen participants (50%) were employed in several roles in professional services; the rest (50%) ranged from working in health care to academia, construction, warehousing, and research. Thirteen participants (43.33%) received at least 1 dose of the COVID-19 vaccine, and 17 (56.67%) did not receive any dose. Participants actively used Facebook, X (formerly Twitter), Snapchat, Reddit, LinkedIn, Instagram, Pinterest, Tumblr, TikTok, and YouTube. Interview minutes ranged from 11 to 52 min, averaging 27 min per participant for the 30 participants interviewed. Thirty transcripts recorded by “otter.ai” yielded 958 significant sentences and phrases arranged into clusters of 22 categories or codes aligned with the 7 behavioral factors from the research question RQ. An inductive thematic analysis of these codes yielded five themes, summarized in Table 2: Themes and Codes.
Themes and Codes.
Thematic analysis
Note: Code# provided in parentheses with other participant demographic information.
Theme 1: Experience with Vaccines and Self-Assessment of Risks Toward Health and Well-Being Determines Future Vaccination Intention
Participants were vaccinated as children: “… the typical vaccine (and) measles” (1.2, 51-year-old man, unvaccinated). Although not 100% effective, participants trusted vaccines: “Usually … with the flu vaccine, … never any bad consequences … I have still gotten flu a few times,” (1.1, 56-year-old woman, vaccinated) and “… our family is fully vaccinated against everything that we had been asked to or scheduled for” (1.2, 51-year-old man, unvaccinated). For choosing vaccines, the severity of the disease and its effectiveness against it: “That depends on how severe and dangerous this virus (is). So, if it is very extreme, then definitely consider” (1.3, 20-year-old woman, vaccinated) and the fear of getting someone else with pre-existing health conditions sick were significant factors: “I was not concerned for myself … (but of) someone in my family that has pre-existing conditions” (1.3, 48-year-old man, unvaccinated). However, some were unafraid of falling sick from COVID-19: “I just was not worried … I do not get sick” (1.4, 30-year-old woman, unvaccinated) and “I never really worried that much about the flu … I have had it before; I have survived … I will get over it” (1.4, 69-year-old man, unvaccinated).
Theme 2: During a Health Crisis, Credible and Trustworthy Media Content Shapes Public Awareness and Opinion About Immunization Programs
Participants relied on information from the following sources during the pandemic: (a) workplaces, (b) internet sites, (c) mainstream media, and (d) social media. One participant was an emergency dispatcher: “We had access to the county health department. We had direct contact with the medical director and the CDC. So, we had information first” (2.1, 48-year-old man, vaccinated). Participants trusted internet sites: “I trusted the most was the CDC and my State’s public health website” (2.2, 71-year-old man, unvaccinated). Conversely, others found internet sites untrustworthy and inundated with misinformation: “There was a lot of misinformation … about … the vaccine … I was not a fan of it” (2.2, 34-year-old woman, unvaccinated). Participants found unbiased information on mainstream media: “I listen to Fox News more than anything … they were trying to give both sides of the story” (2.3, 69-year-old man, unvaccinated) but also biased and conflicting information: “… you had the same thing coming out of … the Wall Street Journal, … you could see the bias … (and) so much conflicting information” (2.3, 69-year-old man, unvaccinated). Participants found social media reliable: “From TikTok, I was getting headlines about breakthrough cases, daily trending news and updates,” (2.4, 28-year-old woman, unvaccinated) but also found inaccuracies: “… it was hard at the time to … filter out what is real and what is not” (2.4, 34-year-old woman, unvaccinated).
Theme 3: Engagement in Social Networks Cultivates Personal, Communal, and Professional Formation, Persuading Vaccine Intentions
Families, neighborhoods, workplaces, and social media influenced participants’ COVID-19 vaccination stances. There were alternative thoughts in families: “Some other people thought the vaccine was going to change our DNA … listening to them, my mother was worried that something would happen to me because I took the vaccine” (3.1, 30-year-old woman, unvaccinated). People in neighborhoods were judgmental and shaming others: “They were criticized on Instagram for having different views” (3.2, 28-year-old woman, unvaccinated) and “Those wearing masks were mad at the ones who did not” (3.2, 63-year-old man, vaccinated). Participants disagreed with masking policies at work: “When they told us to mask, it did not make sense to me because it was an airborne virus and based on my training and ten years in nursing, masks do not do anything for it. N95s do, but you must wear these the entire time” (3.3, 42-year-old woman, vaccinated). Participants shared anti-vaccine sentiments: “I do belong to a community on social media, and they are very against the vaccine,” (3.4, 71-year-old man, unvaccinated) but preferred respect for diverse thoughts, opinions, and beliefs: “They must always appreciate someone’s judgment on whether they feel it will benefit them or if they have a religious reason for not wanting to take the vaccine” (3.5, 61-year-old man, vaccinated).
Theme 4: A Trusted Public Health Response to a Health Crisis Incorporates a Vaccine Administration Backed by Proven Vaccine Efficacy and Safety Data Factoring Adverse Reactions and Natural Immunity
Participants expressed concern that the public health response during the COVID-19 pandemic was untrustworthy, vaccination was incentivized: “People have never needed to be incentivized to get a vaccination before,” (4.1, 39-year-old woman, unvaccinated) vaccine distribution was rushed: “I was hesitant about it then because I thought they were rushing things without clinical trials” (4.1, 61-year-old man, vaccinated) and vaccines were ineffective and unsafe: “I did not feel like it was very effective because people were still getting COVID just as the people that were not vaccinated” (4.1, 48-year-old man, unvaccinated). For some, natural immunity was sufficient in combating a disease: “My body was made to take care of itself … I don’t see how some synthetic immune response is more beneficial than my body creating it on its own” (4.1, 43-year-old man, unvaccinated). Conversely, participants also favored vaccines: “I felt like it was in my best interest to get it … the vaccines were needed to protect people because many people perished” (4.2, 38-year-old woman, vaccinated). But those worried about adverse reactions sought more vaccine efficacy data: “… there was not enough data because we did not know how other people with certain health conditions would react to it” (4.5, 48-year-old man, vaccinated). According to most accessing vaccine administration sites was easy and smooth, except for a few. For one, the vaccination site was too far away: “I had to rent a car and drive to Springfield, 300 miles away, to get the shots. We live in a city and do not own a car” (4.4, 56-year-old woman, vaccinated).
Theme 5: Freedom to Choose Vaccines that are Safe, Effective, and Easily Accessible, Underpinned by Sound Public Health Policy, Boosts Future Acceptance
Participants expressed frustration with the government and the public health agencies’ crisis management during the pandemic: “Everyone was confused by the changing stuff every 2 s,” (5.1, 63-year-old man, vaccinated) believing that the government incited polarization: “… get your vaccine, get your booster, by the left, and the narrative is that the right did not take it seriously enough,” (5.1, 39-year-old woman, unvaccinated) racial bias: “Our mayor decided to prioritize the black community for the vaccines. So, because I live on the north side and not the south … I was not eligible for the vaccine,” (5.1, 56-year-old woman, vaccinated) and the inflation of COVID-19 numbers: “The numbers for flu have practically disappeared … everything is COVID now. People who end up in the hospital end up dying in the hospital from COVID-19” (5.1, 61-year-old man, unvaccinated). In the future, participants want to make their own decisions in considering the vaccine or the booster if mandated (5.2), if the disease was far more severe, and if the efficacy and safety of the vaccines were well supported by credible information (5.3). However, others would not consider COVID-19 vaccines or booster shots in the future since there are no vaccination mandates, the risk of infection is negligible, questions about the effectiveness and safety of vaccines remain unanswered, and concerns about the long-term effects of the vaccines on their health and that of others remain relevant (5.4).
Discussion
Influence of Perceived Health Risks on Vaccine Hesitancy
Pre-existing beliefs motivated by circumstances and experiences from the COVID-19 pandemic influenced this study’s participants’ varying intentions toward vaccination. Those afraid to fall sick from COVID-19 or concerned about infecting others were inclined to receive the vaccines. However, those unafraid to fall sick from the disease did not want the vaccine. Brewer et al. (2017) found that perceptions about risk beliefs impacted motivation, which correlated reliably with getting vaccinated or not. Truong et al. (2022) found that people who had reported having better health felt safer and, therefore, were less inclined to vaccinate. These perspectives were formed during a period of declining disease transmission but before many structural changes in public health governance, underscoring how perceptions were still deeply shaped by the immediate aftermath of the pandemic. Recent CDC data from 2025 (CDC, 2025) show that only 20.4% of U.S. adults received the updated COVID-19 vaccine, with low perceived risk and concerns about safety driving hesitancy, confirming that risk perception still shapes vaccine choices.
Past Vaccination Behavior and Its Role in Decision-Making
Participants of this study also revealed that their past vaccination behavior and experiences influenced their decisions to receive the COVID-19 vaccine. Participants who received the flu vaccines annually were open to COVID-19 vaccines in a time when COVID-19 remained a public health concern but no longer an emergency. Those not open to receiving the flu vaccine were not open to receiving the COVID-19 vaccine. Fan et al. (2021) had previously found that individuals who had not received a past vaccine were twice as uncertain about the COVID-19 vaccine and more than three times as likely to refuse it. These findings serve as a reminder that vaccine behavior during 2023 reflected not only pandemic-specific concerns, but also longer-term attitudes toward public health engagement. A 2025 study by Dhawan et al. (2025) confirmed that individuals with a history of vaccine acceptance, like regular flu shots were significantly more likely to follow through on COVID-19 vaccination, reinforcing that past behavior shapes current decisions.
Consumption of Information About COVID-19 and Vaccines
People in the USA could consume information from abundant sources and form independent perceptions and opinions about the COVID-19 pandemic and vaccines (Puri et al., 2020). Throughout the COVID-19 pandemic, public health agencies and healthcare authorities disseminated their plans to restore order and control through the media (Quon et al., 2023). Participants trusted information about the pandemic and vaccines hosted by public health agencies and other healthcare experts on mainstream media and the internet. However, not everyone found information on mainstream media and the internet trustworthy due to the prevalence of misinformation and disinformation (Reno et al., 2021). Similarly, participants also experienced misinformation and disinformation on social media (Swire-Thompson & Lazer, 2020). For participants, political bias was evident in the information from significant sources, including social media, which fueled their uncertainty and caused their lack of trust in authorities and the vaccination programs they were implementing. Zelaya et al. (2023) found that information that fulfills the needs of people in the middle of a vaccine hesitancy continuum during a health crisis will earn their trust and influence a possible vaccination uptake in the future. Similarly, for Singer (2023), truth-based information must be fact-checked to earn consumers’ trust before it is hosted or posted. Therefore, public health agencies should ensure their messaging is vetted on all communication channels, including social media. These insights are especially pertinent given the post-2023 fragmentation in federal communication strategies and the erosion of trust in scientific institutions (Kennedy & Tyson, 2023).
Social Networks as a Source of Reinforcement
Although life in the USA returned to normalcy in 2023, people relied heavily on social networks (Wong & Bottorff, 2023). Social networks helped bring people closer during the pandemic by informing them about the happenings in their neighborhoods, towns, cities, and nations. Participants learned what others believed about the pandemic and the vaccines, providing participants with much-needed comfort, knowing that they were not alone and that others were also experiencing what they were going through. In social communities, they experienced the ill effects of political affiliations, encouragement or discouragement, and unsavory experiences regarding stances about masking and vaccination. Han (2023) confirmed the role of social networks in forming social support systems, which, for participants of this study, formed perceptions that reinforced whatever they already believed and led them to develop new beliefs, forming a connection with others with similar interests, opinions, and beliefs. Additionally, a collective inclination like in families influenced participants to adopt the same familial mindset, supporting the findings of Deng et al. (2023), who found that when a family decision-maker believed that the vaccine was unsafe, other family members chose not to vaccinate their children against COVID-19. These findings illustrate that even in 2023, before the complete retreat of national vaccine messaging, many people had already migrated their trust to more intimate or ideological circles.
Perception of Ineffectiveness and Safety Concerns
Many in the USA thought that COVID-19 vaccines were rushed without the backing of adequate clinical tests (Troiano & Nardi, 2021) but instead by political motivations (Mills et al., 2020, p. 10). For Enwezor et al. (2021) and Galanis et al. (2023), the most common reasons for people not wanting the COVID-19 vaccines were concerns about their safety and efficacy. The recurrent need for boosters made participants believe the vaccine was more like the flu shot and ineffective against the virus. Furthermore, participants were fearful about the long-term effects on those who had received the vaccine. Participants who trusted COVID-19 vaccines were concerned about potential adverse effects and wished that more data regarding the efficacy and safety of the vaccines would be available to the public. For Teófilo et al. (2023), systematic monitoring of adverse drug reactions to vaccines is essential to establish the efficacy and safety of the COVID-19 vaccines. Importantly, participants expressed this distrust prior to the dismantling of centralized vaccine initiatives by policy changes (Godoy, 2025), underscoring that hesitancy was already entrenched prior to the structural transformation of U.S. public health (Gostin et al., 2023).
Barriers and Access to Vaccines Challenges
Most participants of this study found their experiences at vaccine administration sites during the pandemic easy and smooth; however, they recommended improvements in accessibility, education, and privacy protection. Until May 2023, COVID-19 vaccines were offered to the people in the USA at no cost (Hodge, 2023). Kholina et al. (2022) found that while the rollout of the COVID-19 vaccine was a success, vaccine delivery systems needed substantial improvements to ensure optimal uptake and equitable vaccine access for all (pp. 12–14). Expecting vaccine hesitancy during any health crisis, public health programs should make the best healthcare resources, including vaccines, available and accessible to all those in need. Consistent data about the vaccine’s efficacy and safety should be publicly emphasized.
Future Vaccination Decisions Based on Perceived Threats
Participants in this study would decide against the vaccine if symptoms from COVID-19 continue to be mild and less severe. At present they feel safer and more confident in letting their natural immunity protect them from reinfection in the same manner as they have been protected from other viral infections. If the death rate from the disease is higher than before and proven data supports the efficacy and safety of vaccines, then participants will more readily receive the vaccine or the booster in the future. But, under current circumstances, participants wanted to wait and not consider the COVID-19 vaccines or the booster in the future because there were no vaccination mandates in effect, the rate of infections and deaths have been lower, questions about the efficacy and safety of vaccines have not been fully answered, and the long-term effects from the vaccine on health and well-being was a big unknown and a significant concern. Participants subjected to employment-related mandates could request an exemption or seek employment elsewhere. From their experiences during the pandemic, participants concluded that they were free to receive or not receive the COVID-19 vaccine in the US. Participant’s emphasis on autonomy and transparency mirrors today’s public health climate, where decentralized decision-making and legal limits on agency enforcement have further elevated personal discretion over collective mandates (Gostin et al., 2023).
This study offers a historically situated perspective on the behavioral, informational, and institutional factors that shaped vaccine hesitancy in the United States during 2023, a pivotal year between the end of federal pandemic mandates and the onset of widespread decentralization in public health governance (Gostin et al., 2023). By capturing the lived experiences of individuals navigating uncertainty, mistrust, and evolving norms, the study contributes to a deeper understanding of how public sentiment, policy design, and communication strategies intersect during health crises.
Transparent, accessible communication remains foundational. Participants’ mistrust was often rooted in inconsistent messaging and perceived politicization of health guidance. Past research have underscored that precise, culturally sensitive, and evidence-based communication delivered through trusted messengers is essential to counter misinformation and build vaccine confidence (Goje & Kapoor, 2024; Singer, 2023). As centralized messaging has weakened post-2023, the role of local health professionals and community leaders has become even more critical.
Policy frameworks must acknowledge hybrid immunity and evolving risk perception. Participants expressed skepticism about repeated boosters and emphasized the importance of natural immunity. Incorporating both vaccine-induced and infection-acquired immunity into public health guidance can enhance credibility and foster more adaptive, personalized strategies (Dhawan et al., 2025; Truong et al., 2022).
Equitable access is a persistent challenge. While many participants reported smooth vaccine access in 2023, structural barriers such as transportation, scheduling, and digital literacy remain significant, especially in underserved communities. As federal funding recedes, state and local systems must innovate to maintain equitable delivery (Hodge, 2023; Kholina et al., 2022).
Autonomy and trust must be balanced in future interventions. Participants’ emphasis on personal choice reflects a broader shift in public health ethics, where coercive mandates may erode trust. Policies that prioritize education, transparency, and voluntary uptake are more likely to succeed in today’s decentralized and politically polarized environment (Gostin et al., 2023).
By placing these findings in the sociopolitical context of 2023, this study not only captures a moment of transition but also provides lasting insights for future readiness. Building resilient public health systems will require more than biomedical solutions; it will need trust, flexibility, and a deep understanding of the social fabric that influences health behavior.
Limitations and Future Considerations
This study used a crowdsourcing platform, CloudResearch® Connect™ (CRC), for recruiting participants whom CRC employed as professional survey takers motivated to earn supplemental income. Hence, the sample of participants for this study was a convenience sample (a non-probability sample) rather than a representative (probability) sample. As data were collected in 2023 after the formal end of the U.S. public health emergency (Hodge, 2023) participants’ perceptions may reflect a post-crisis normalization of pandemic experiences rather than immediate or acute risk reactions (Gostin et al., 2023). This study interviewed social media users. Expanding participation to include non–social media users or digitally marginalized populations would help capture perspectives from groups often underrepresented in online-recruited samples (Wong & Bottorff, 2023). Finally, an additional coder in the research team would enhance the reliability of thematic analysis.
Though the study targeted a broad demographic, recruitment and participation trends may have affected age representation. Future research can further examine older populations to refine public health strategies. This is especially important as vaccine hesitancy among older adults can intersect with chronic illness risk and healthcare access disparities, which may require different strategies than those effective with digitally native populations (Haeuser et al., 2025). Vaccine poses a threat to pandemic preparedness, fueled by distrust and misinformation. Future research must foster trust, ensuring that health measures are adopted rather than imposed upon individuals. This recommendation has become increasingly salient as public trust in federal health institutions has continued to decline in the post-emergency phase, with growing resistance to perceived top-down messaging (Kennedy & Tyson, 2023). Transparency, accessibility, and informed choice can strengthen preparedness and improve outcomes.
Future studies should also incorporate health-based theories such as the Theory of Planned Behavior (TPB; Ajzen, 1991) to explore the psychological and social factors influencing vaccine hesitancy. TPB emphasizes how attitudes, subjective norms, and perceived behavioral control shape vaccination intentions and behaviors. Applying this framework can help develop strategies that reinforce positive health norms, empower informed choices, and strengthen public trust in immunization programs, ultimately improving vaccine uptake and pandemic preparedness. Such theoretically grounded strategies are particularly valuable in today’s decentralized health policy environment, where public health decisions are shaped not only by evidence but also by legal, political, and cultural forces (Hodge, 2023).
Conclusion
Grounded in data collected in 2023, this study offers a retrospective perspective on the COVID-19 pandemic, which presented an unprecedented global challenge, providing valuable lessons for future health crisis management. This study highlights key factors—such as vaccine hesitancy, public trust, media influence, and access barriers—that shaped individuals’ responses to vaccination and public health measures during a period when U.S. public health institutions were transitioning from emergency operations to a more decentralized, state-led model. While vaccination and social restrictions were central strategies, they alone were not sufficient to ensure widespread public compliance. Understanding the societal dynamics that drive trust and hesitancy is crucial for policymakers and public health agencies seeking to foster more effective engagement.
Rather than viewing the public as passive recipients of health directives, this research highlights the importance of engaging individuals as active partners in crisis recovery. This is consistent with broader calls for participatory public health that emphasize education, transparency, and trust over mandates. Public trust is not merely a byproduct of policy implementation; it is a necessary foundation for achieving long-term stability. The study demonstrates that vaccine hesitancy, often exacerbated by misinformation and distrust, is not solely a resistance to science but a reaction to top-down enforcement without adequate transparency. By prioritizing credible and accessible communication, allowing people the freedom to make informed choices, and strengthening societal resilience, public health agencies and governments can improve vaccination uptake in future crises. Supporting this, a UK-based study found that while public sector managers valued rapid decision-making and teamwork during the pandemic, many organizations demonstrated limited engagement in substantive reflection after the crisis, leaving them underprepared for future disruptions (Meierdirk & Fleischer, 2025). As future health emergencies emerge in increasingly complex social and political environments, strengthening these foundations will be essential not only for vaccine uptake but for the legitimacy of public health itself.
Footnotes
Ethical Considerations
This study was approved and conducted according to the guidelines of the Robert Morris University Institutional Review Board.
Consent to Participate
Informed consent was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data collected will be used for other ongoing publications and will be available upon request.