
Abstract
This article offers a qualitative analysis of how people discursively justify and make sense of their COVID-19 vaccination intentions. Drawing on in-depth interviews with 39 people in British Columbia, Canada, just prior to the availability of a COVID-19 vaccine (Oct–Dec 2020), the objective of this study is to explore why some citizens are in favor of a COVID-19 vaccination while others are against receiving a COVID-19 vaccine. Our qualitative data reveals three key factors that inform people’s discursive justifications of their COVID-19 vaccine intention: (i) self-rated health, (ii) (mis)trust, and (iii) intuition. First, we found that vaccination justification was coordinated through participants’ self-rated views of their own health and whether they adopted an individualist or a collectivist cultural perspective of risk. Second, participants’ justification was tied to (mis)trust in government and public health initiatives, affecting participants’ upcoming willingness to receive a COVID-19 vaccination. And third, drawing on the concept of epistemic repertoires, we observed that vaccination justification was expressed through various types of intuitions that were grounded in personal “gut feelings,” religious beliefs, and scientific reasoning. Overall, our research highlights the importance of qualitatively examining the cultural and social meanings that citizens attach to vaccines and the “cultural scripts” they draw on when responding to public health vaccination initiatives. Our findings reveal the need for local, contextualized, and community generated health strategies that go beyond simply providing public health information.
Keywords
Introduction
The global COVID-19 pandemic, caused by SARS-CoV-2 coronavirus, lead scientists and health authorities to develop and implement a variety of health and safety protocols to keep the public safe, reduce illness and death, and limit societal disruptions (Canadian Public Health Association, 2021). These efforts were vital given that COVID-19 has “caused illness and death in more people than any other pandemic in the last hundred years” (Muhajarine et al., 2021, p. 2). A main public health response to COVID-19 was mass vaccination, put in place with the aim of slowing the spread and severity of illness associated with COVID-19. Public responses to health initiatives like vaccinations ranged from support and compliance to rejection, with some Canadians feeling unsure “about the value and safety of the vaccination” (Muhajarine et al., 2021, p. 1). Notwithstanding state, scientific, and public efforts, governments are usually dissatisfied with the effectiveness of their campaigns during pandemics, particularly with vaccination uptake (Carlsen & Glenton, 2016).
There is a large amount of research exploring vaccination intent and identifying factors related to vaccination hesitancy. The reasons for vaccination intention and hesitancy are multifaceted and research in this area spans in focus from discussing the history of eugenics (Schwartzman, 2025), medical racism (Olatunde, 2025), anti-science rhetoric and the “autism scare” (Rodriguez, 2025), and the role of online influencers and social media (Eng & Kim, 2025). Other research identifies individual, psychological, familial, or community level attitudes, beliefs, and determinants, to more qualitative work that explores refusal and acceptance and the ethics or biopolitics of vaccination (Mamo et al., 2010). For example, scholars have emphasized that some people refuse vaccines or are vaccine hesitant because of cultural norms (Decoteau & Daniel, 2020), social beliefs (Polonijo et al., 2016), differing ideas of responsibility (Albert, 2019), and because of individualized and neoliberal health care practices (Reich, 2014, 2016). Vaccination hesitancy is also related to uncertainty, which is only heightened by the consumption and spread of misinformation and disinformation, as well as information overload (Albert & Gray, 2023; Nan et al., 2014; Parsons et al., 2018; Scannell et al., 2021, p. 443; World Health Organization, 2020). Indeed, vaccines themselves are biomedical innovations that are imbued with cultural meanings of safety, risk, and risk management. In a time of risk calculation, anxiety, and uncertainty, people often rely on both direct and implicit risk assessments to organize and manage everyday life (Kaufman, 2010).
We join this abundance of excellent insights into vaccination behaviors but focus on how people discursively justify their vaccination during a unique time frame, just prior to the availability of COVID-19 vaccines in Canada. This is a particularly important focus since insights come from a very “unsettled time” (Swidler, 1986) marked by uncertainty, misinformation, fear, and panic. Focusing on justifications reveals “cultural scripts” (Mills, 1940; Swidler, 1986, 2001) and ways that people “make sense” of and rationalize the situation they were in when faced with new, and soon to be available, COVID-19 vaccines. The goal of this article is to explore this. Employing a qualitative analysis based on 39 semi-structured interviews with a group of citizens in Southern British Columbia, Canada, we look at a group of people’s discursive justifications for their COVID-19 vaccination intention in October to December 2020, just before COVID-19 vaccines were available in Canada. Our qualitative data reveals three key factors that inform people’s justifications and how they rationalize vaccine intention: (i) self-rated health, (ii) (mis)trust, and (iii) intuition. First, we found that vaccination justification was coordinated through participants’ self-rated views of their own health and whether they adopted an individualist or a collectivist cultural perspective of risk. Second, participants’ discursive justification was tied to (mis)trust in government and public health initiatives, affecting participants’ upcoming willingness to receive a COVID-19 vaccination. And third, drawing on the concept of epistemic repertoires, we observed that vaccination justification was expressed through various types of intuitions that were grounded in personal “gut feelings,” religious beliefs, and scientific reasoning. To begin, we explore the complicated landscape of COVID-19 and vaccination politics in general, and offer a brief contextual overview of COVID-19 vaccinations and social scientific insights on vaccination hesitancy.
Context
COVID-19 Vaccination in Canada
Public responses to COVID-19 vaccines in Canada have ranged from support and compliance to rejection and dissonance. In October 2020, when we began our qualitative research, Statistics Canada reported that 75% of Canadians were likely or somewhat likely to receive a COVID-19 vaccination when one became available. The Angus Reid Institute (Korzinski, 2020) also reported at that time that 48% of Canadians would be vaccinated immediately if a vaccine became available with another 31% stating they would likely be vaccinated after waiting a period of time. They also reported that 14% would not get vaccinated and that 7% of Canadians were undecided.
Two months later, on December 14, 2020, COVID-19 vaccines became available to the general Canadian public (Government of Canada, 2022). Three years later, compliance figures showed high initial compliance with COVID-19 vaccination but a declining uptake over time. Among Canadians older than 5-years-old, 95% had received at least one COVID-19 vaccine dose, 82.6% had received at least two doses, and 51.6% had received three COVID-19 vaccine doses (COVID-19 Tracker, 2024). These figures, while important for revealing statistical levels of compliance, do not disclose nor reveal the nuances and complexity of everyday vaccine decision-making among citizens. As a result, there is a need to examine “the other side of the compliance relationship” (Gray & Silbey, 2011) to reveal how COVID-19 vaccine initiatives have been interpreted and experienced by members of the general public.
Social Scientific Insights on Vaccination Hesitancy
Social scientific research on vaccination attitudes, hesitancy, refusal, and anti-vaccination has been growing over the past decades, focusing on vaccines from MMR, influenza, H1N1, to the HPV vaccine, and many others. Research has begun to untangle the complexity of vaccine decision-making, with specific focus on “vaccine hesitancy”– a complex idea that signals a refusal of a vaccine, a delay in acceptance (Keshet & Popper-Giveon, 2022), or a harboring of doubts about the benefits and safety of vaccines (Yaqub et al., 2014). Vaccination acceptance is usually not homogeneous with people being strictly for (pro) or against (anti) vaccination. For example, one could be hesitant toward some vaccines while accepting or refusing of others. Or, one may be accepting of a COVID-19 vaccination at one point in time, but hesitant in another point in time. As a type of health decision-making, vaccine hesitancy relates to one’s sense of risk and their trust in health authorities and scientific expertise (Larson et al., 2014).
Public trends in vaccination acceptance and hesitancy (and indeed other related practices such as inoculation, variolation, and immunization) vary across time and space and within individuals. Attitudes and behaviors can also vary over time (MacDonald, 2015, p. 4163). For example, inoculation has been strongly advocated for by religious and cultural institutions in Asia, such as in India and China since the 16th century, and in other places such as the Ottoman Empire, North Africa, and what would be known today as southern Libya (to name a few places) in the 17th and 18th centuries (Boylston, 2012, pp. 310–312). In the early to mid-18th century in India, inoculation with variolous (variolation) “was the most widespread” and well-established prevention against smallpox, which interfered with state (and European) efforts to promote the cowpox vaccine – discovered in 1796 by Edward Jenner (Brimnes, 2004, p. 199). The goal was to “replace variolation by vaccination” (Lahariya, 2014, p. 491), but was met with “reluctance, opposition and a slow acceptance of vaccination” (Lahariya, 2014, p. 491). Brimnes (2004, p. 199) points out that the “campaigns to prevent smallpox in the eighteenth and nineteenth centuries are commonly understood as the first attempt of large-scale state-sponsored medical intervention” in India and “represented an early encounter between an elitist state-sponsored medicine and various forms of popular resistance.” Indeed, what was framed as vaccination “resistance” in this colonial context is a form of othering by colonial Europeans, framing the Indian population as being irrational, superstitious, stubbornly resistant to western medical benevolence, despite “the fact that variolation had stronger roots in India than in Europe” (Brimnes, 2004, p. 200). Vaccination resistance was not limited to only colonial contexts. For example, skepticism and opposition was also seen in England. Inoculation was introduced in England for smallpox in the early 1700s and while widespread in many parts of England, likely through word of mouth, there were some, such as farmers and dairy maids, who resisted inoculation, which “was a mystery and a considerable problem for doctors” (Boylston, 2013, p. 352).
Vaccination hesitancy can take many forms and subsequently lead to a variety of different outcomes (Calnan & Douglass, 2020). For instance, a month prior to the availability of a COVID-19 vaccine in Canada, Benham et al. (2021) found that 63.9% of participants reported COVID-19 vaccine hesitancy and that this was linked to age, lower education, and non-Liberal political attitudes. Other researchers have reported similar findings. For instance, those with less than high school education had lower vaccination intention while older citizens and women were more likely to accept a COVID-19 vaccine (Gerretsen et al., 2021; Ogilvie et al., 2021). Racey et al. (2021) also found that 89.7% of teachers in the province of British Columbia, Canada, intended to receive a vaccine and that those with a background in engineering or science had higher vaccination intention. This research also noted that the reliability of the source of information on vaccines also impacted vaccination intention. Social norms, families, physicians, and public health officers all have been shown to play a role in vaccination intention (Ogilvie et al., 2021).
Vaccination hesitancy around COVID-19 vaccines is particularly interesting given that the virus itself is novel and was initially accompanied by confusion and surprise by the public, especially early in the pandemic. During the time-frame of our data collection (Oct–Dec 2020), the nature of the pandemic was changing and potential vaccinations were being announced using a seemingly “new” and novel technology (mRNA). Many citizens found the novel technology alarming despite it being a technology that has been around since the 1970s (Beyrer, 2021). By mid-December 2020, web searches for “mRNA vaccines” increased thirtyfold, leading to increased misinformation consumption (Hitti & Weissman, 2021; Leong et al., 2022). While scientists and public health officials praised the noteworthy speed at which vaccines against SARS-CoV-2 coronavirus were developed, the public was very concerned about its seemingly rapid development. As a result of this quicker than normal vaccine development process there was “increased public hesitancy towards novel mRNA vaccines compared to traditional vaccines” (Leong et al., 2022, p. 5). This led to varying levels of vaccination hesitancy, resistance, and confusion among the general public (Johnson, 2023).
Vaccine hesitancy in both Canada and the USA has been associated with a low perception of the seriousness of COVID-19, mistrust in the benefits of vaccines, and right-wing political affiliation (Gerretsen et al., 2021). In a study of tweets on Twitter (now called X), vaccine hesitancy was also linked to “concerns over safety, suspicion about political or economic forces driving the COVID-19 pandemic or vaccine development, a lack of knowledge about the vaccine, antivaccine or confusing messages from authority figures, and a lack of legal liability from vaccine companies” (Griffith et al., 2021, p. 1; for international comparisons on COVID-19 vaccine hesitancy see Ejaz et al., 2021; Huizenga et al., 2023; Larson et al., 2022). The concept of trust is central to vaccine acceptance with lowered vaccination acceptance related to an eroding trust in health care professionals, scientific expertise, and government (Larson et al., 2018). In other words, trust has a personal element but is also an attribute of social systems (Brownlie & Howson, 2005).
Our research contributes to an ongoing understanding of COVID-19 efforts and public responses. These insights continue to be important as many citizens remain vaccine hesitant and/or refuse to be vaccinated, while those who have received a COVID-19 vaccine in the past must decide whether to maintain their vaccine uptake through additional COVID-19 booster shots. Moreover, focusing on how people discursively justify their vaccination decision themselves is important and insightful when working to increase vaccination acceptance for it can “meet people where are they are” or “speak their language” of vaccination politics.
Data and Methods
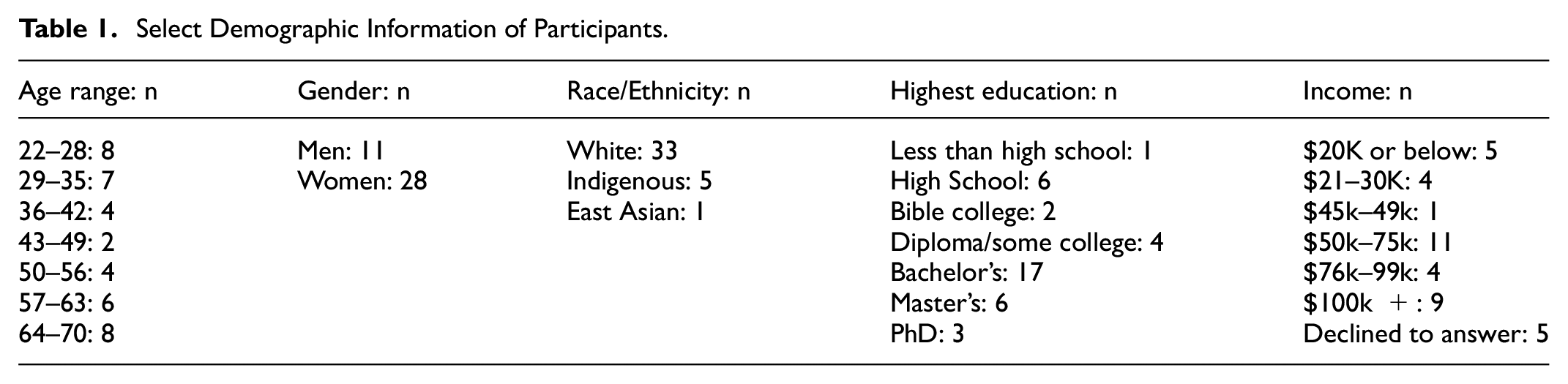
Data consisted of 39 in-depth semi-structured interviews conducted by the first author with members of the general public in Southern British Columbia, Canada (see Table 1) between October and December 2020. Notably, this was before COVID-19 vaccines were made available in Canada or announced in other countries. Each interview lasted approximately 60 to 75 minutes. Interviews were conducted over the video conferencing platform Zoom or by telephone and recorded externally to zoom using a digital audio recording device and transcribed verbatim by a research assistant. All identifying information was made anonymous and all participants were given a pseudonym. Interviews were semi-structured and no prior specific or technical knowledge on COVID-19 was required for participation.
Select Demographic Information of Participants.
The semi-structured interview guide was developed by both authors with questions designed to be neutral and to avoid asking leading questions or to ask questions that were framed towards a particular view or stance on vaccination or COVID-19. The semi-structured interview guide was reflexively developed to avoid inserting the authors’ biases into the research design or to influence the research process. All interviews followed the same semi-structured guide to ensure all participants were asked the same questions. Yet, given the semi-structured design of the interviews, participants were able to elaborate on the standard questions or move the conversation to topics or conversations they also thought were important which could shape the order of the conversation. Through this process, interviews were designed to elicit rich and detailed responses from participants rather than pre-determined answers. The interviewer also ensured that any personal opinions, thoughts, and feelings about vaccinations, COVID-19, and other topics did not guide the interview or conversation. The interviewer made sure to not insert personal beliefs or be “corrective” to participants. Doing so allowed participants to express their views, opinions, beliefs, and perspectives freely without worry of judgment and to avoid having participants’ express social desirability bias or acquiescence bias where participants shape their responses in order to be viewed in a socially desirable or favorable way (Garrett et al., 2003; Krug & Sell, 2013). To further ensure the reliability of the data, the interview guide was designed to move from more general questions to more specific questions about vaccinations and COVID-19. Carefully crafting question order can help mitigate acquiescence bias and can help establish rapport between the interviewer and the participants.
Interviews were purposefully conversational to help establish rapport and ensure the participants felt comfortable in the interview. This is important given that members of the public have varying degrees of familiarity with these types of interviews (see Codó (2008) and Edley and Litosseliti (2010) for more on interview familiarity in research design). All interviews began by asking participants demographic questions, including questions on self-identification of their gender identity and race and ethnicity. Participants were then asked about their early memories of COVID-19, general thoughts on the COVID-19 pandemic, what they knew about COVID-19 and where they got their information from, and questions on their health and safety behaviors. From there, participants were asked questions about potential COVID-19 vaccinations, their opinions on vaccinations in general, and specific questions about their attitudes and beliefs about COVID-19 vaccinations. Participants were also asked to speak about their anticipated vaccination intention as well as their justifications and reasoning for their anticipated intention. Interviews covered other topics as well such as perceptions of state efforts during COVID-19, such as “bubbling” and other public health measures. Through this process, the authors established and maintained methodological rigor to ensure the data and findings are reliable and valid.
Recruitment occurred through virtual posters distributed on social media platforms (e.g., Facebook and Twitter), and through minimal snowball sampling methods. Recruitment materials emphasized that this “research explores public attitudes towards a potential COVID-19 vaccine in British Columbia” and that participants “will be asked questions about what information [they] have about COVID-19, [their] views on the risks associated with the virus, and [their] thoughts on a potential vaccine.” As specified on the recruitment materials, participants were eligible to participate if they were between the ages of 19 and 70 and if they currently lived in British Columbia. Participation included a $20.00 online gift card. Recruitment materials also specified the research funding associated with this research as well as the authors’ university affiliation. Participants were directed to email the first author directly if they were interested in participating or had any questions – rather than signing up on public social media posts – to help ensure confidentiality and anonymity. The authors halted recruitment and interviews when they achieved saturation (see Hennink et al., 2017 for more on saturation).
Participation required written (electronically singed) informed consent and participants were assured that they could express their opinions and thoughts freely without judgment as the interviews were anonymous and confidential. The first author obtained informed consent prior to the start of the interviews, and reviewed all informed consent materials and procedures before the interviews began. Participants were sent their online gift card before the start of the interviews, and were reminded they could end the interview at any time without penalty and that they could decline to answer any questions they did not want to answer. This research received Human Research Ethics approval from the University of Victoria.
Data analysis was inductive, and interviews were coded and analyzed using the qualitative and mixed methods data analysis software, Dedoose. Coding initially began with open coding to “pull out from the data what is happening and not impose an interpretation based on pre-existing theory” (Gibbs, 2018, p. 11). Open coding provided a starting point and was subsequently followed up with categorization to organize the data and retrieve data on shared topics and themes across the interviews. From there, we moved to analytic and thematic codes in order to reveal patterns and themes in the data (Braun & Clarke, 2006).
Findings
Analysis of the data revealed variation in vaccination intention with the majority of participants expressing some vaccination intention, ranging from an intention to get a COVID-19 vaccine when one becomes available but with hesitancy, to firm support and intention to vaccinate. Two participants were truly unsure of their vaccination intention and the rest expressed low to firmly no intention to be vaccinated (see Figure 1).

Continuum* of vaccination intention, by participant count.
Qualitative thematic analysis revealed three themes that capture participants’ COVID-19 vaccine justifications. In what follows, we first describe how vaccination intention was influenced by participants self-rated views of their own health and whether they adopted an individualist or a collectivist perspective on risk. Second, we discuss how trust in government and public health initiatives impacted participants’ willingness to receive a COVID-19 vaccination. And, third, we draw on the concept of epistemic repertoires to illustrate the role of intuition on vaccination intention. Here, we highlight how vaccination intention was organized by intuitions that were grounded in personal “gut feelings,” religious beliefs, and scientific reasoning.
Self-rated Health
Self-rated health is an indicator of quality of life that has been shown to both positively and negatively influence health behaviors (Dominick et al., 2002; Shockey et al., 2017). For instance, individuals who consider themselves to be healthy tend to opt out of preventative health activities (Guthrie et al., 2017). In contrast, low perceptions of self-rated health have been observed to positively influence initiatives such as annual flu vaccination (Watson & Oancea, 2020) while negatively influencing other initiatives, such as shingles vaccination (Vogelsang & Polonijo, 2022). In regards to COVID-19 vaccination, our qualitative data reveals that low self-rated health was a justification used in relation to positive vaccination intention while high self-rated health was a justification used in relation to both positive and negative vaccination intention depending on whether one adopts an individualist or a collectivist perspective of risk when justifying their vaccination intention (see Douglas & Wildavsky, 1982; Tansey & O’riordan, 1999).
High Self-rated Health (Individualist)
Being “healthy” was defined by some participants as having a strong immune system in the context of COVID-19. For example, Herman, a 22-year-old white male with no plans to be vaccinated, expressed the following: I’ve had people at work get a cold before. I’ve been at school and everyone gets the flu. You know, things get passed around. Even if I did get it [COVID-19], I feel like I have a strong immune system, and I have a pretty high pain tolerance. I don’t know. You just deal with it. I don’t think I’m going to die or anything.
The notion that individuals need to take care of risks themselves was also discussed by Josiah, another 22-year-old white male who is against COVID-19 vaccination. According to Josiah, people should “build up their immune systems [and] fight it on their own.” Josiah explained that if people did this, they wouldn’t need a COVID-19 vaccine.
Similar to Herman and Josiah, Mathaius, (a 59-year-old white male with no plans to be vaccinated, also placed his trust in his immune system but went further by describing a social Darwinist survival of the fittest type perspective: I have an immune system and as long as it functions and functions well, I will be alive, and when it doesn’t, it will be time to go. I am not afraid of death … I’m very much inclined to say nature designed us in a good way, and a lot of the enhancements that we are trying to make are not necessarily good for us at all … I feel I could handle it [COVID-19] … you know, the mortality rate.
On three separate occasions during his interview, Mathaius justified his intention not to be vaccinated against COVID-19 by discussing his natural good health and his ability to recover even when he gets sick. However, Mathaius did reveal that he supplements his natural health through non-biomedical means such as elderberries, mushrooms, and other natural immune boosters. In addition to Herman, Josiah, and Mathaius, another participant named Mic (who also has no intention to be vaccinated) stated that he is not at all worried about COVID-19 because he considers himself healthy. Mic cited his vegetarianism as evidence of his health as well as his ability to take evasive action when he senses the onset of a cold.
Some interviewees in this study also framed their risk perception of COVID-19 in relation to the flu vaccine and influenza. For these individuals, the flu vaccine, in combination with their high self-rated perception of their individual health, was used to justify their intention not to be vaccinated against COVID-19.
High Self-rated Health (Collectivist)
In contrast to participants who described themselves as “naturally healthy” with an individualist perspective on risk, other participants in our data who similarly felt “naturally healthy” stated that they wanted to decrease risk exposure to keep others safe. Several of these participants described a more collectivist attitude towards risk and were more open to the idea of being vaccinated against COVID-19. For example, when Elizabeth, a 67-year-old white woman, was asked about her COVID-19 vaccine intention and what might guide her decision she stated: Vaccines and other things have slowed the spread, so I think that’s a good thing … and maybe protect in some ways, like not get rid of it but protect seniors, people who are immunocompromised, if it slows it down, yeah that’s, to me a good thing … because germs like these can redevelop or mutate.
Similar to Elizabeth, participants Claire, a 23-year-old white woman, and Alison, a 45-year-old white woman, also expressed concern about collective health and safety even though Claire was still undecided about receiving a COVID-19 vaccine.
[I’m] motivated to protect other people in the community too. I think I’m a little more worried about other people getting it than myself because I know if I get it, that there is a higher chance that I can just get it and be done with it, whereas for other people it can be quite, [well] it can kill them.
I think I am in some ways more afraid of (pauses) not in some ways, I am more afraid of passing on this disease than getting it … if there was a way to know that I could be safe around other people, I would want that.
Despite a high self-rated view of their own health, and believing that they would be fine if they were to contract COVID-19, some participants, such as Claire and Alison, were more worried about the impacts that contracting COVID-19 would have on others.
Low Self-rated Health
Participants in our research with a low self-rated health perspective held positive intentions toward COVID-19 vaccination. For instance, a 64-year-old white woman named Norma stated that her positive vaccination intention was linked to a chronic illness. She noted: “I have COPD (chronic obstructive pulmonary disease), so anything that will reduce the chance of me getting COVID-19, I’m all for it.” Several participants pointed out that they were immunocompromised. For example, Suzanne, a 36-year-old white woman who is pro COVID-19 vaccination, noted that she is compromised because of being on immunocompromising medication. She stated: “I’m considered a high-risk population … I’m not leaving [the house].” Another participant named Christopher, a 30-year-old white man, disclosed that his partner is immunocompromised making him even more cautious since it would take her a long time to recover if she were to get COVID-19. However, for Christopher, being blind created additional health risks beyond his partner being immunocompromised. He expressed: I would try my best to (pauses and sighs) keep 6 feet away from people, but that is extremely difficult when you’re blind … it would be easier for me to catch it because of the fact that I have to use my hands to find things or feel for things, and instead of being able to see an object, I have to use my fingers. For instance, because the further an object is away from my face, the harder and less detail I get from it.
As a result of his increased chances of catching COVID-19, blindness shaped Christopher’s understanding of his own health and risk during the pandemic. He noted that despite all the health precautions taking place (i.e., masks, strict handwashing, flu vaccines, and hand sanitizer) that one can still get sick. Indeed, he believed people have a false sense of safety from COVID-19. According to Christopher, “the people who are holding these no-vaccine rallies, they are just putting more people at risk and spreading fake info and fake science.”
In addition to participants with pre-existing conditions, some individuals, such as Raphael, a 69-year-old Indigenous man, posited that simply getting older and the aging process itself represented an increased risk. As a result, Raphael justified his pro COVID-19 vaccination intention in the following way: I get my flu shot every year. I mean, what the heck, why not? Even if it’s only 50 or 70 percent effective, that is better than zero, and I’m not getting any younger, so my body’s ability to fight off things, in many cases, you know, it’s just common sense, and you know, I’ve always been a supporter of science and you know, medical developments and stuff like that.
In contrast to Norma, Suzanne, Christopher, and Raphael, a 32-year-old white woman named Roxy stated that while she is generally healthy (high self-rated health perspective), she also believed that her health was compromised and at risk in a structural way due to her employment as a teacher surrounded by children. She noted that protecting her health was the main motivating factor behind her pro-vaccination intent. For Roxy, vaccines are one way to ensure she will stay healthy and feel more comfortable in her vulnerable role as a teacher.
(Mis)trust
No Trust at All
Individuals who stated that they were not going to be vaccinated against COVID-19 also noted that they did not trust the government, politicians, and public health officials. Some of these participants also expressed the view that they lacked trust in COVID-19 vaccines because both the government and “big pharma” were corrupt. This perceived corruption around COVID-19, these participants argued, was leading to a loss of personal rights and freedom.
For some participants who stated that they were not going to be vaccinated, the topic of COVID-19 appeared to be a tipping point in their mistrust of government and public health. For example, a 62-year-old white woman named Evelyn stated: I feel our government is really letting us down and you know, like, COVID-19 is just exposing that … things have been ignored … who is our government working for? If a COVID-19 vaccine became available … I would not trust her (Dr. Henry, Provincial Health Officer), because it’s not possible to have tested the virus properly by December! It’s just not possible … how are we fast tracking the testing of this vaccine? Who is telling us that it is 90% effective? 90% effective for what? Like, how long afterwards are we looking at these people who have taken the vaccine and saying they’re 90%, this is a 90% effective vaccine? A month? Two weeks? Bullshit (laughs)
Evelyn’s mistrust in the state and government was also tied to a larger mistrust in scientific research on COVID-19 vaccine development and approval. She mistrusted the science behind the vaccine and consequently, mistrusted any expert who would approve the vaccine. Mistrust was a common theme among participants who were skeptical of the vaccine and did not plan to be vaccinated. For example, Thea, a 24-year-old Indigenous woman, stated that she was hesitant to receive the COVID-19 vaccination because she believed it was too political and thus was unable to trust Dr. Henry, the Provincial Health Officer. She noted: I’m going to say no, [I don’t trust Dr. Henry] … [because] a lot of political officials are going to back it ([vaccines) no matter what when it does come out, right? Because I just feel like that is the agenda being pushed right now.
Another participant, Tamar, a 26-year-old Indigenous woman with no plans to be vaccinated, also discussed politics and stated that she does not trust the science and the institution of medicine. As a result, she illustrates how trust for her is tied to her own personal sense of truth. She stated: I don’t trust it (COVID-19 vaccine) … I feel like everyone is kind of on level playing ground. Like I don’t put medical students or medical professionals on a pedestal, and I really don’t think they’re more enlightened than the average person. They do have the education and the tools, and they have the power to use that to help people, which is wonderful, but … people should be free … but we’re not … Big Pharma and corporations can pay independent researchers and companies to skew data and to skew numbers. It is really hard to find what is the truth and what is like real …
The perception that the pharmaceutical industry is corrupt was a concern for several participants. We also observed that trust concerns were interrelated and one concern was often connected to another concern. In other words, issues related to trust appeared to “snowball” into various issues in a layered manner. Thus, it is important to understand the nuances and issues of trust put forth by participants. This is especially the case given that because of the above concerns a few participants questioned “the realness” of COVID-19 during the interviews which was often framed within a narrative of losing personal freedom and personal rights as a consequence of corruption.
Cautious Trust
Participants with higher vaccination intention tended to express more trust in public health. For these participants, trust in science was important when justifying their vaccination intention. However, it was not an unconditional level of trust as these participants did have some concerns. For instance, they did express some skepticism on the speed of vaccine development. For example, a 30-year-old white woman named Doloris stated that despite having a general trust in scientific testing she is unsure as to whether she would receive a COVID-19 vaccine. She stated: I’m kind of on the fence [about getting a COVID-19 vaccine]. It depends on the vaccine and how well it works and what the research shows about it. It’s kind of hard to say because there is too much going on. I mean personally I would prefer to get vaccines that have been thoroughly tested.
Trust in science was an important theme for many participants when justifying their vaccination intention. While some participants who had low vaccination intention had a clear mistrust in science, others believed in and trusted science, but had concerns. For these latter participants, they were not turning away from or rejecting science, but rather, wanted to make sure the science of the vaccine was being conducting in an ethical manner. For example, Elizabeth, a 67-year-old white woman who was undecided if she would be vaccinated, raised the following questions: Well, what are the side effects? I mean, you know, if there are any. Where is it going to be given, you know? What should you watch for? Is it from a reliable source? … Not that I’m prejudice, but I want our vaccine to be produced in Canada … and that’s because I guess I just think we have such great standards here … that would be another factor in it.
While Elizabeth put forth a national twist on the concept of trust (i.e., placing greater trust in vaccines produced in Canada), some participants worried about a rise in anti-vaccination sentiment. For instance, both Helena, a 52-year-old white woman, and Joan, a 56-year-old white woman, noted that even if the efficacy levels of the vaccine were high, they did not trust that enough people would choose to be vaccinated. While both participants planned to be vaccinated, they expressed the following.
Three years ago, even a year ago, I would have said yes, [a vaccine for something like COVID-19 would be effective]. But … it’s absolutely astounding the stupidity of people who, they will deny to their dying breath that they have COVID-19 or that it could possibly be COVID-19, and just the thought that there are hundreds of thousands, if not millions, of people out there … I think it’s probably going to take more like two years because of the number of people who are reluctant to believe the science.
I think um that is a big worry for me. That the pandemic will not fade away because not enough people take the vaccine. That is a real fear I think I have.
Epistemic Repertoires and the Role of Intuition
Epistemic repertoires are “essentially ways and practices of learning, thinking, and resolving problems” (Chai et al., 2016, p. 110). They shape what people know, what they consider true, right, or wrong, and provide a conceptual lens for understanding how people justify a position, such as vaccination intention. When people make decisions about something like COVID-19 vaccines, part of what they are doing is thinking about what they consider to be true. How people derive their truth about something is also tied to their perceptions of risk in everyday life. The epistemic repertoires that people have about the world and about themselves shape their intuition. Some of this stems from collective and social resources, where ideas are framed in particular ways, which could be either mainstream or alternative points of view. These truths, based in these epistemic repertoires, are not just about the information that people have, but about how they frame or think about issues (Ten Kate et al., 2021). In our data, we observed that when participants arrived at or expressed their truth on COVID-19 vaccines, their intuitions were either driven by by personal “gut feelings,” religious beliefs, or discourses of science.
Individual “Gut Feelings”
Participants who relied on their own intuition and gut feelings to guide their vaccination decision-making tended to have no intention of receiving a COVID-19 vaccine or were hesitant about it. While they did not specifically use the words, “gut feelings,” they did express feeling that it just wasn’t right for them. For example, one participant named Rusty, 65-year-old white male against receiving a COVID-19 vaccine, stated the following: “Personally, I would be hesitant to take it. I’ve never had the flu shot or anything … I know that vaccines have worked in the past so I don’t deny that they work or anything, but I just don’t know if it would be right for me.”
Another participant, Elizabeth, a 67-year-old white woman who was hesitant about being vaccinated, stated that she too relied on her own intuitive feelings but based her vaccination intention on her past experiences with allergies and bad reactions to vaccinations. She expressed: I’m trying to get an answer to [whether I can get a COVID-19 vaccination] because 30 years ago, I was working in Vancouver and I had to have a vaccine for the hospital for the flu and I had one and I ended up being sick for three months and it took me another two months before I went back to work … They told me then never to have anything. So, I’ve never taken anything, I’ve never had another vaccine or like a flu shot or anything like that.
In addition to Elizabeth, Tamar, who previously noted her objection to being vaccinated against COVID-19 because of her mistrust of science and medical professionals, also revealed that she has allergies and stated that she feels personally prepared to take care of herself if she were to get sick. In addition to her lack of trust, she also noted that she would say no to a COVID-19 vaccine because of her allergy to peanuts, leading her to have a feeling that a COVID-19 vaccine was not right for her. Despite allergies and contracting COVID-19 being different health emergencies, her personal logic and how she makes sense of allergies informed how she would take care of herself if she were exposed to COVID-19. She stated that she would use the medical system (like she does in the case of her peanut allergy) and also rely on her religious faith (mentioned elsewhere) to keep her safe.
Religious Beliefs
Intuition, based on religion, was a second epistemic repertoire observed in the data justifying some participants’ low COVID-19 vaccination intention. For example, Herman, who previously was described as having high self-rated health coupled with an individualist perspective toward risk, noted that his intuition is rooted in his religious beliefs and his trust in God.
Like, I believe God, okay I don’t know if you know it, but there’s a book in the bible – Psalm 91. It talks about basically when you dwell with God or you spend time with God in the secret place, and you take personal time, like pray and reading … that’s what it kind of talks about, and I’ve read it a quite a few times. And it says that God, like as a Christian I believe the bible is true. And in that passage, it says, actually I am going to find it really quick. It says, (looking for passage …). Ya, it says, “a thousand may fall at your side, ten thousand at your right hand, but it will not come near you.” So, like I believe a lot of people, even someone (pauses) like a thousand people could get it at your side, or ten thousand people beside you but it will not come near you. And it also says, um “no harm will overtake you and no disaster will come near your dwelling place”… So, I feel totally safe.
For Herman, as with some other interviewees, his religious intuition guided him and helped him obtain what he considered to be truth. However, his religious based intuition also created a barrier for him to be vaccinated as his feeling of safety was rooted in God and preparation for an afterlife in heaven.
Scientific Reasoning
While epistemic repertoires consisting of intuitive gut feelings and religious beliefs were observed in the data to be associated with lower COVID-19 vaccination intention, a different pattern emerged among our participants who were guided by scientific truths. Participants who used scientific, logic-based reasoning when justifying their vaccination intent tended to base their decision-making in beliefs aboutscience. However, many still expressed vaccination hesitancy, though they generally had a desire to learn more information based on scientific research. As Henrietta explained: I think they [vaccines] are the single best advance that we’ve made in health care in the last century, the most cost-effective way to reduce the burden of disease on society, and that they have made a huge, huge difference in terms of, knowing that our kids are going to grow up.
For those whose epistemic repertoire was based on a belief in science, hesitancy was primarily rooted in how quickly COVID-19 vaccines were being developed and tested. They overcame this hesitancy through an intuition rooted in a belief in science. For example, Helena, described the rapid speed in the development of a vaccine as “taking a chance” given that the process usually takes much longer. But this is a chance Helena is prepared to take if it means collectively protecting people. This was similar for Lacey, who intended to get a COVID-19 vaccine, but had some hesitancy. Despite her worries, she appeared willing to take a scientific “leap of faith” and follow her intuition, rooted in an underlying trust and belief in vaccine science. She stated: But most vaccines that we have are really well researched, and like, have existed for some length of time. So, I have no problem with them. But, with one that is brand new with not a lot of trials on it in large populations, it’s a little bit, you just got to be like, (pauses) I probably would be okay [receiving a COVID-19 vaccine] because I don’t have a lot of [pre-existing health] issues. Like, the odds are probably that it would be okay, but you never know with some people, they might end up with some sort of acute reaction.
For Henrietta and Helena, their intuition stemmed from a belief in science. However, it was not a blind faith in science as they did illustrate hesitancy but were also quick to critically engage in and attempt to learn more about vaccine development.
Discussion and Conclusion
In this research, we demonstrate the importance of cultural and social context in understanding how people discursively justify their COVID-19 vaccination intentions. Our qualitative research reveals three main themes that capture participants’ justifications when describing their upcoming decision whether or not to be vaccinated against COVID-19. First, our findings provide partial support for research that suggests that those who consider themselves healthy and have a higher self-rated view of their health tend to opt out of preventative health activities (see Guthrie et al., 2017). In our data, we did observe several participants with high self-rated views of their health who stated that they were not going to be vaccinated against COVID-19. However, these individuals tended to express an individualist rather than a collectivist view of risk when justifying their decision (Douglas & Wildavsky, 1982; Kahan, 2008; Tansey & O’riordan, 1999). The pursuit of individual freedom and having a strong immune system was, for these participants, prioritized over collective public health and safety. A social Darwinist view of the consequences of COVID-19 also emerged as a rationale for justifying the acceptance of suffering that might occur among those with weak immune systems (see Kanık et al., 2022; Nachtwey & Walther, 2023).
In contrast, participants with high self-rated views of their health, and who were more willing to be vaccinated against COVID-19, expressed a collectivist rather than an individualist view of risk. These individuals, despite being healthy and feeling confident against COVID-19, were more open to being vaccinated because of a desire to keep other people safe. This is the opposite of the social Darwinist view held by those in our sample who advocated a more individualist perspective of risk. Our findings here, on the role of self-rated health and COVID-19 vaccination intention, point to the value of examining cultural theories of risk and how cultural worldviews and cognition toward risk contributes to our understandings of vaccine hesitancy (see Anderson, 2022; Brown, 2020; Brown & Zinn, 2021).
The second conceptual finding in this research involves the role that trust played in public health COVID-19 initiatives. Trust in science and the practice of research were important factors for several participants when justifying their vaccination intention. Our findings reveal that although most participants were skeptical to some degree, they could be divided into two distinct groups. I) Those who had low vaccination intention had a clear mistrust in not only science but also in government and the profit motive of pharmaceutical companies. While there is some validity to this position given research highlights problems with industry sponsorship of pharmaceuticals (see Gray, 2013; Morrow et al., 2022, 2023a, 2023b), the concerns of this group were more deeply embedded in politics and a general distrust of government. Our findings, here, on this first group, lend support to previous governmentality research by Keshet and Popper-Giveon (2022) who find that people who had no plans to be vaccinated also had a general resistance to their government’s biopower. II) In contrast, participants in our research who did plan to be vaccinated held a more cautious level of trust. This second group trusted the institution of science but had concerns about the speed of vaccine. In turn, they placed more trust in public health officials and had higher vaccination intention. These findings point to the need for continued research on how vaccine hesitancy is affected by different conceptual understandings of trust in science, politics, and government (see Larson et al., 2018). As our findings illustrate, a complete lack of trust will lead to resistance whereas cautious trust may eventually lead to positive vaccination intention.
The role of epistemic repertoires and intuition on vaccination intention is our third major finding our research. Epistemic repertoires provide a conceptual lens for a more nuanced understanding of how people justify their decision on whether to receive a COVID-19 vaccine, as well as their broader perceptions of biomedical research (see Cottingham & Fisher, 2017; Rose, 2020). Given that epistemic repertoires have the power to shape decision-making on vaccines and public health initiatives, it is important to engage rather than dismiss the epistemic repertoires of different groups. In our research, COVID-19 vaccination intentions were guided by personal “gut feelings,” religious beliefs, and scientific reasoning.
In policy terms and regarding health messaging, our findings suggest that it is counter-productive to categorize those who do not wish to be vaccinated as absurd individuals or “anti-vaxxers” who lack reason and education. Thus, we posit a need to go beyond what Toth (2020) refers to as epistemic superiority, whereby individuals on both sides of the COVID-19 vaccine debate (pro-vaccine vs. anti-vaccine) continue to ridicule and insult each other for failing to adopt their preferred position. Epistemic superiority will only make it difficult, if not impossible, for healthy dialogue to take place between those with differing vaccination intentions. It would also be prudent to work with community leaders and culturally relevant leaders to deliver tailored messaging that addresses specific concerns, rebuilds trust, and works with local truths and beliefs. This may require a “hands off” approach, or what Epperson et al. (2022) call “public health partnerships” (p. 4). It could include efforts where local leaders, artists, and community members shape efforts and health messaging in a way that makes sense from within the community, rather than through an imposition of public health messaging or reasoning that is decontextualized, simplified, and culturally abstract. For example, during COVID-19, an Indigenous community in Minnesota, in partnership with the local department of health, worked with a variety of artists to design a COVID-19 vaccination campaign that joined vaccination with “an array of traditions and values” (Beard et al., 2025). This approach supported community and emphasized community thriving in the context of settler colonialism (Beard et al., 2025). Elsewhere, like in India, there are calls to integrate traditional knowledges and practices into public health efforts. For example, shepherds in rural India, drawing on Indigenous herbal knowledge systems, have long practiced, and continue to practice, potthi kattu, or herd immunity, “to address the epidemics and pandemics that affect their people, livestocks, and herds or flocks” (Bheenaveni, 2020, p. 183).
While our study is limited in that we are not able to generalize to the entire population in terms of “statistical-probabilistic generalizability,” we do provide insights on how people justify their COVID-19 intentions that can be generalized in a “analytic” way (see Smith (2018) for a fruitful explanation of types of generalizability) that contributes to a broader understanding of vaccination acceptance and hesitancy. While our findings are specific to a small regional area with a limited sample, our insights about mistrust, epistemic repertoires and truth, anti-science, intuition, and religion are relevant across spaces and locations, but might manifest or sound differently. Regardless, our findings, in conjunction with other historical and contemporary insights into vaccination resistance, hesitancy, and refusal reveal the need for tailored campaigns and messaging, as discussed above. Moreover, given that vaccination hesitancy is not necessarily static, it would have been interesting to interview people over time throughout the COVID-19 pandemic to understand how people’s beliefs, opinions, attitudes, and health decisions may have changed over time, and why they changed. Future research would benefit from more longitudinal engagement with participants. Our study offers what we consider to be useful conceptual and analytic understanding that may be relevant to other contexts and public health initiatives. These conceptual and analytic themes, that we inductively arrived at through qualitative analysis, could also be tested in future quantitative research.
Footnotes
Acknowledgements
We would like to thank all the people who spoke with us for this research and opened up to us about their lives during the COVID-19 pandemic.
Ethical Considerations
The study received Human Research Ethics approval from the University of Victoria (protocol #: 20-0424).
Consent to Participate
All research participants provided informed and signed (electronic) consent.
Author Contributions
Study conception and funding acquisition were completed by the first author. Material preparation, data collection, and analysis were performed by the first and second author. Both authors developed and commented on all versions of the manuscript, and have read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is financially supported by the Rapid SARS-CoV-2 Vaccine Research Initiative in BC award from Genome BC, Michael Smith Health Research BC, and the BC Center for Disease Control (BCCDC), under grant # COV2-2021-2340. It is also financially supported by University of Victoria's Faculty of Social Sciences COVID-19 Research Fund.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
In light of the nature of this research and as part of the informed consent, participants were assured that their data was private and not to be shared publicly, so supporting data are not available.