
Abstract
The prevalence of vaccine hesitancy underscores the fact that the general public does not uniformly embrace scientific recommendations. Vaccine hesitancy represents a spectrum, encompassing both those who accept all vaccines and those who outright reject them. This paper aims to explore the relationship between science literacy, contextual factors, and vaccine hesitancy while accounting for specific mediation mechanisms. The authors applied a theoretical framework derived from the deficit model and the contextual model of public understanding of science. Hypotheses regarding the relationship between scientific literacy, religiosity, political identification, and vaccine hesitancy were tested. The authors also tested several hypotheses based on the assumption that the perception of scientific credibility and institutional trust are significant mediators of the above-mentioned relationships. The data from an online survey with a nationally representative quota sample of the Croatian population (with an average age of 42.6 years.) were used (N = 1,500), while the data were analyzed using structural equation modeling. The results indicated that the perception of scientific credibility plays a significant role as a mechanism that translates the impacts of literacy, religiosity, and political identification. Institutional trust proved to be a significant mediator but in a way opposite to the hypotheses, which points to the need to contextualize the aforementioned relationships. The authors also determined that younger age, right-wing political orientation, higher religiosity, and lower scientific literacy were the determinants of hesitancy in both vaccine types (COVID-19 and vaccines in general), thus indicating that they might be connected to deeply rooted value dispositions.
Plain Language Summary
The paper deals with the issue of vaccine hesitancy and tries to determine the characteristics of people with a more skeptical attitude towards vaccination. The results of online research conducted among the general Croatian population showed that younger people, more religious people, and people with a right-wing political orientation have a more negative attitude towards vaccination and that this can mostly be explained by their lower trust in science and scientists.
Introduction
Although the “honeymoon” between science and the public has long passed (Miller & Pardo, 2000), with the onset of the COVID-19 health crisis, it has become even more obvious that the public does not accept scientific recommendations and advice with unconditional approval. This manifested itself in the widespread vaccine hesitancy and low vaccination rates, especially in some countries (Sallam et al., 2022). According to the SAGE Working Group on Vaccine Hesitancy (MacDonald, 2015), vaccine hesitancy represents a continuum that ranges from an acceptance of all vaccines to a complete refusal. In an attempt to explain vaccine hesitancy, it might be preferable to start from the already existing approaches developed in the field of public understanding of science. In the initial stages of the development of this field, the so-called deficit model was the dominant approach (Bauer, 2008), which assumed that the negative attitude toward science stems from insufficient knowledge and information, which makes people less likely to endorse scientific achievements that they do not fully grasp. Subsequent research studies confirmed a small positive correlation between knowledge and positive science attitudes (for a review, see Allum et al. 2008). In the matter of vaccine hesitancy, the studies generally confirmed the link between lower science and/or health literacy and higher hesitancy, both in the case of COVID-19 vaccines (Gusar et al., 2021; Motoki et al., 2021; Siani et al., 2022; Weerakoon et al., 2022; H. Zhang et al., 2022) and other specific vaccines or vaccines in general (Pavić and Šuljok, 2022; Smith et al., 2015; Wang et al., 2018), even though reports which failed to find such connection are not uncommon (Casigliani et al., 2020; Castro-Sánchez et al., 2018; Siewchaisakul et al., 2022).
With the further development of the field, it has become apparent that science attitudes depend not only on the amount of knowledge, that is, on scientific or other specific types of literacy, but also on other determinants unrelated to knowledge. This led to the development of the so-called contextual model (Brossard and Lewenstein, 2010), that is, to the realization that individual characteristics and the social context can influence the formation of attitudes about science, as well as that the aforementioned factors can distort the effect of scientific literacy. Therefore, a more complete understanding of vaccine hesitancy should account both for scientific literacy and other factors unrelated to scientific literacy which could influence vaccine hesitancy or even distort the effects of literacy. Among other things, the roles of politics, religion, institutional trust, and trust in science have been frequently researched (Yaqub et al., 2014), and the importance of mental models, that is, beliefs, values, and prior experiences has been also established in other areas, such as climate change perception (Bostrom et al., 2012; van den Broek et al., 2021).
When it comes to political identification, Wollebæk et al. (2022) found that right-wing ideological beliefs (mainly the opposition toward state power) were related to higher COVID-19 vaccine refusal. Institutional trust proved to be linked to lower refusal, whereas that was not the case for partisanship. Institutional trust also partially mediated the relationship between right-wing ideological beliefs and COVID-19 hesitancy. Baumgaertner et al. (2018) found that conservative political ideology was negatively correlated with pro-vaccination attitudes toward flu, pertussis, and measles vaccines, while this connection was partially mediated through the trust in government medical experts. Cowan et al. (2021) detected that politically conservative Americans were less likely to express willingness to receive the COVID-19 vaccine, where institutional trust mediated the relationship only in the first phase of the pandemic. Kossowska et al. (2021) obtained similar results by confirming that political orientation had an indirect impact on beliefs and attitudes toward vaccines through distrust and negative perceptions of scientists, both in the pre-COVID-19 era and during the COVID-19 health crisis.
Concerning religiosity and the related mediation mechanisms, the research studies generally confirmed the positive correlation between religiosity and vaccine hesitancy. Higher individual religiosity consistently predicted mistrust of the COVID-19 vaccine (Upenieks et al., 2022), general hesitance toward COVID-19 vaccines (Tolstrup Wester et al., 2022), and lower COVID-19 vaccination intentions (Olagoke et al., 2021). On the macro level, Martens and Rutjens (2022) demonstrated that spirituality and religiosity were negatively associated with COVID-19 vaccination rates, even after controlling for other factors (GDP, population age, general skepticism toward vaccinations, etc.). Trust in science was identified as having a mediation role between higher religiosity and COVID-19 vaccination intentions by Tippins et al. (2023). Higher religiosity is generally connected with higher vaccine hesitancy related to other vaccines as well, especially HPV (Best, 2019; Bodson, 2017).
Previous research studies also pointed to the importance of institutional trust and trust in science when explaining vaccine hesitancy. According to Yaqub et al. (2014), skepticism toward science, refusal to accept medical research findings and absence of evidence-based knowledge regarding vaccines significantly influence people’s immunization behavior. According to a study by Freeman et al. (2022b), people who held stronger beliefs in coronavirus conspiracy theories were less likely to follow government guidelines, undergo diagnostic or antibody testing, or get vaccinated. The researchers also found that these individuals tended to exhibit paranoia and hold a general belief in vaccine conspiracy theories, climate change conspiracy theories, and a general distrust of institutions and professions. Sturgis et al. (2021) found that both micro-level and macro-level of trust in science were connected with higher confidence in vaccines. The data were collected from a sample of 144 countries before the COVID-19 pandemic. In research conducted on a representative sample of the Serbian population, MiloševićĐorđević et al. (2021) found that belief in the vaccine conspiracy theories motivates vaccine hesitancy through its effect on reduced trust in medical science and low objective vaccine knowledge. On the same note, Soares et al. (2021) found that factors associated with both refusals and delay to take the COVID-19 vaccine comprised low confidence in the health service response during the pandemic, negative perception of the adequacy of measures implemented by the government, and perception that the information provided by health authorities during the pandemic was inconsistent and contradictory. The importance of trust in science when COVID-19 vaccination intentions are considered was also confirmed by Seddig et al. (2022).
It could be hypothesized that the above-mentioned contextual factors could play a more prominent role in vaccine hesitancy concerning COVID-19 vaccines in comparison to the vaccines in general or other particular types of vaccines. Namely, liberty infringements were not only related to the issue of the vaccines themselves but also to the lockdown and other measures. Therefore, the ideological differences in relation to the tolerance toward manufactured risks and their sources might have become more operative during the COVID-19 crisis (Wollebæk et al., 2022). Moreover, COVID-19 vaccines were also developed in a sudden and serious public health crisis, with their development thus being very fast. This induced additional skepticism about their effectiveness and safety. Research studies conducted in Croatia also confirmed that the development speed was a crucial factor for the skepticism, both among the general public (Pavić et al., 2022; Bagić et al., 2022) and among healthcare workers (Miskulin et al., 2022). However, several research studies (Dombrádi et al., 2021; Durmaz et al., 2022; Meier et al., 2021; Olagoke et al., 2022; Romer et al., 2022; Ruiz & Bell, 2021) determined that there was a strong correlation between the acceptance of COVID-19 vaccines and other vaccine types, as well as that socio-demographic correlates of both types of vaccine hesitancy were similar. However, none of the studies was designed to deeply explore other types of determinants or possible differences in their mediation mechanisms.
Having reviewed related work, we can conclude that up to this moment, only a few research studies have been concerned with the exploration of the relationship between literacy, contextual factors, and vaccine hesitancy by accounting for specific mediation mechanisms. In addition, few research compared vaccines in general and COVID-19 vaccine hesitancy. Therefore, the main goal of this paper is to fill the above-mentioned gaps by investigating mediation mechanisms and comparing their importance when explaining general vaccine hesitancy and COVID-19 vaccine hesitancy.
Research Objectives and Hypotheses
The main research objective was to test two mediation mechanisms (trust in science and institutional trust) that link scientific literacy, religiosity, and political orientation with general and COVID-19 vaccine hesitancy. To gain a deeper understanding of such mechanisms, three general hypotheses were put forward in this study. The first one presumes a mediation mechanism that connects science literacy, political identification, and religiosity with vaccine hesitancy through science credibility serving as a mediator. In the second hypothesis, institutional trust serves as a mediator of the above-mentioned relationship. The first two general hypotheses are each divided into three specific hypotheses. The third hypothesis has a very general scope since it aims to test whether the determinants of vaccine hesitancy will be similar when COVID-19 and vaccines in general are concerned. Hence, the hypotheses are listed as follows:
H1. Science credibility is a mediator of the association between vaccine hesitancy and its predictors.
H1.1. Perception of science credibility is a mediator of the negative association between scientific literacy and vaccine hesitancy. H1.2. Perception of science credibility is a mediator of the positive association between religiosity and vaccine hesitancy. H1.3. Perception of science credibility is a mediator of the positive association between right-wing political identification and vaccine hesitancy.
H2. Institutional trust is a mediator of the association between vaccine hesitancy and its predictors.
H2.1. Institutional trust is a mediator of the negative association between scientific literacy and vaccine hesitancy. H2.2. Institutional trust is a mediator of the positive association between religiosity and vaccine hesitancy. H2.3. Institutional trust is a mediator of the positive association between right-wing political identification and vaccine hesitancy.
H3. The determinants of COVID-19 and general vaccine hesitancy will be similar.
Methodology
Sample
In this study, the data from an online survey with a nationally representative quota sample of Croatian adult citizens were used (N = 1,500). The quota sample was determined according to gender, age, settlement size (rural or urban, as defined by Croatian laws), and region (Zagreb, Northern Croatia, Slavonia, Lika and Banovina, Croatian Littoral and Istria, and Dalmatia), thus reflecting the structure of the general adult (18+) Croatian population when these demographic characteristics are concerned. The data were collected by a public opinion company using an existing opt-in panel of respondents with self-administered data collection. All respondents declared their informed consent to participation. The ethical approval was obtained from the Ethical Committee of the Faculty of Humanities and Social Sciences, Josip Juraj Strossmayer University of Osijek (No. 602-04/19-04/7). The survey was conducted in July 2022, with the pandemic still ongoing but with a noticeable shift in everyday life regarding official anti-COVID measures.
The sample structure is presented in Table 1. As can be noted, no missing values were present.
Sample Structure.

Measures
As Miller and Pardo (2000) summarized, civic scientific literacy is usually conceptualized and measured in two ways: (1) as the understanding of basic scientific constructs and (2) as the understanding of the nature of scientific inquiry. The first approach is related to the substantive knowledge of the constructs pertaining to the various scientific fields (belonging to natural sciences), whereas the second approach puts emphasis on the basic understanding of the research process and/or on the institutional background in which science develops. In the current study, scientific literacy was measured by the 13-item scale regarding objective scientific facts, wherein it is assumed that an average person has encountered them during primary education (Durant et al., 1989; Miller, 1998). Some of the items were: “Radioactive milk is safe for drinking if boiled” and “The Sun moves around the Earth.” The scale included three answer options (Yes, No, Don’t Know). As in some previous studies, the “don’t know” option was subsequently coded as an incorrect answer since it is considered as an indicator of lower literacy (e.g., Evans, 2011; D. Johnson et al., 2015). Cronbach alpha in the current study amounted to .72.
The Credibility of Science Scale (CoSS) was used to determine participants’ perceptions of the credibility of science (Hartman et al., 2017). Specifically, the scale measures the degree of belief in the legitimation of scientific methods and results, as well as attitudes toward scientific activity and scientific credibility. It is a seven-point Likert scale that contains six items (e.g., “Many scientific theories are completely wrong”). In the current study, higher results on the scale indicate a positive perception of scientific credibility. Hartman et al. (2017) confirmed the validity and reliability of the scale and subsequently, it has been used in research examining attitudes toward science regarding various scientific topics (e.g., Saling et al., 2021; Thorpe et al., 2022). Cronbach alpha in the current study amounted to .90.
Institutional trust was measured using three items, where respondents rated their self-perceived level of trust in the parliament, the government, and the judiciary on a scale ranging from 1 (“I do not trust them at all”) to 5 (“I completely trust them”). Cronbach alpha in the current study amounted to .86.
As a measure of COVID-19 vaccine hesitancy, we used The Oxford Vaccine Hesitancy Scale (OVHS) proposed by Freeman et al. (2022a). The scale contains seven items on a Likert scale ranging from one to five (e.g., “I would describe my attitude toward COVID-19 vaccination as: (1) completely positive to 5) completely negative”), with higher scores representing higher levels of hesitancy. The scale has been found to be reliable and valid in measuring vaccine hesitancy as it is highly associated with the Vaccine Hesitancy Scale (VHS) proposed by Shapiro et al. (2018). Additionally, the scale has been validated in a few countries and among different populations (e.g., Fazel et al., 2021; Huang et al., 2022a; Joshi et al., 2021; Karabulut et al., 2022; Van Duong et al., 2021). Cronbach alpha in the current study amounted to .86.
Hesitancy toward vaccines in general was measured using the VHS scale proposed by the SAGE Working Group on Vaccine Hesitancy (Shapiro et al., 2018). The scale contains 10 items (e.g., “Vaccines are important for children’s health”) on a Likert scale ranging from 1 (strongly agree) to 5 (strongly disagree). Similar to the OVHS, higher scores on the scale indicate higher levels of hesitancy. The scale has been used in several countries and studies indicate the reliability and validity of the scale in measuring general levels of vaccine hesitancy (e.g., Domek et al., 2018; Huang et al., 2022b; Temsah et al., 2021;). Cronbach alpha in the current study amounted to .95.
Political orientation (left-right), as well as self-perceived religiosity, were measured with a single item on a Likert scale ranging from 1 to 10, with lower results indicating left-wing orientation and lower religiosity.
In the following Table 2, the descriptive statistics of the employed measures are presented.
Descriptive statistics of the measures.

Analytical Approach
In order to test the research hypotheses, structural equation modeling (SEM) was conducted. SEM is a second generation of multivariate analysis used to simultaneously assess the relationship of multiple independent latent variables while considering measurement errors of each indicator in analysis (Awang, 2012; Hair et al., 2010). For SEM implementation, certain requirements need to be met, with the adequate ratio of sample and parameters used in the models and no missing data being the most important among them (Hair et al., 2010). The rule of thumb for the adequate ratio of sample and parameters suggests that the sample needs to be at least 10 times bigger than the number of parameters used in the models. In view of the fact that the sample size was 1.500 and that no missing cases were present in the dataset, it can be concluded that the SEM requirements were met.
In order to evaluate our hypotheses, the following four models were tested:
Model 1: Predictor model – vaccines in general
The first model incorporated only the predictor variables and attitudes towards vaccines in general as the dependent variable (VHS scale). As already noted, scientific literacy was applied as a latent variable, while religiosity and political orientation were used as manifest variables. As in all subsequent models, gender and age were used as control variables.
Model 2: Predictor model – COVID-19 vaccines
The second model that was tested included the same predictor structure as the first model, but a different outcome variable. Namely, attitudes toward COVID-19 vaccines (OVHS scale) served as the outcome variable. Model 3: Parallel mediation model – vaccines in general. The next two models can be conceived as the extended versions of the first two models. The extension included two new variables: institutional trust and perception of scientific credibility which served as the mediators. The difference between the third and the fourth model lies in the outcome variables. In this model, the outcome variable comprised attitudes towards vaccines in general (VHS scale). Model 4: Parallel mediation model – COVID-19 vaccines. In the final model, the predictors included scientific literacy, religiosity, and political identification, while institutional trust and perception of scientific credibility served as mediators. The attitudes towards COVID-19 vaccines were the outcome variable (OVHS scale).
Results
The results of the first and the second model indicated that scientific literacy, religiosity, political orientation, and age were significant predictors of attitudes toward both vaccines in general and COVID-19 vaccines. That is to say, the negative relationship between literacy and hesitancy suggests that individuals with higher levels of scientific literacy are less likely to be hesitant toward vaccines. Additionally, the positive association between religiosity, politics, and hesitancy suggests that more negative attitudes toward both types of vaccines are held by more religious individuals and those who identify as right-leaning on the political spectrum (Figure 1).

Model 1 results (standardized coefficients).
The negative relationship between age and hesitancy means that younger participants were more likely to express hesitancy toward both general and COVID-19 vaccines. As for gender, it was not a significant predictor of the attitudes toward both COVID-19 vaccines and vaccines in general (Figure 2 and Table 3).

Model 2 results (standardized coefficients).
Model 1 and Model 2 (Full Details).

The results of the third model confirmed the existence of a direct path between science literacy and attitudes toward vaccines in general. However, there was no mediation of institutional trust since no connection between science literacy and institutional trust was established. On the other hand, science credibility served as a partial mediator of the connection between science literacy and attitudes toward vaccines in general. Both institutional trust and science credibility were partial mediators of the connections between religiosity and political orientation and the attitude toward general vaccines. However, contrary to the stated hypotheses, higher religiosity and right-wing political orientation were connected to higher institutional trust and, consequently, lower vaccine hesitancy. Namely, the indirect path through scientific credibility increased hesitancy among right-wing and religious people, while the path through institutional trust had the opposite effect. Here we can note that control variables, even though they were a constitutive part of Model 3 and Model 4, are omitted from all subsequent figures in order to more clearly depict the hypothesized mediation relationships (Figure 3).
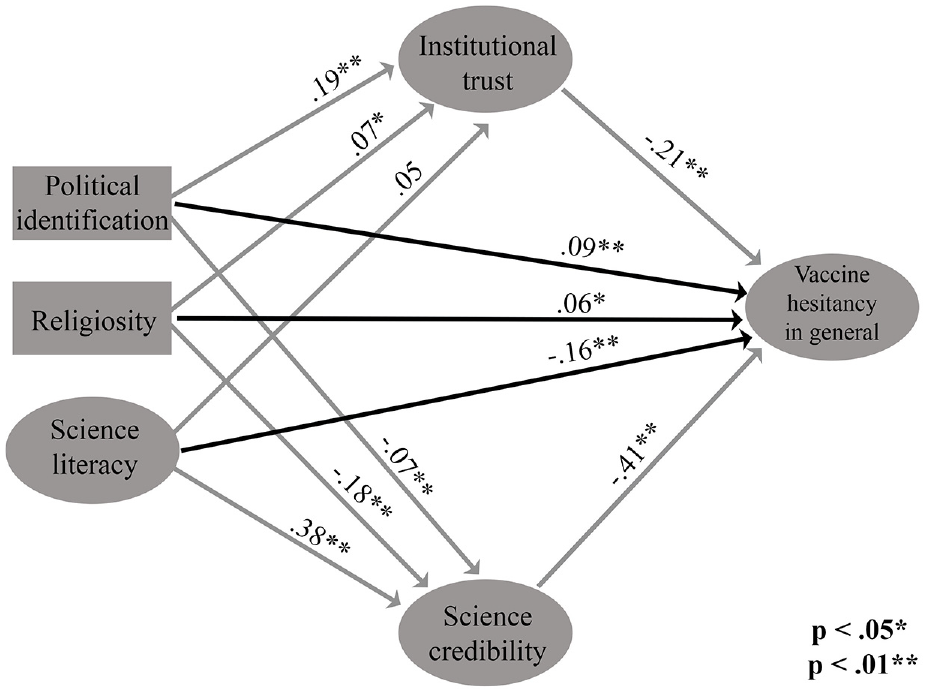
Model 3 results (standardized coefficients).
The full details of the mediation analysis pertaining to the Model 3 are presented in Table 4.
Model 3-Mediation Test Using Bootstrap Analysis (95% Confidence Interval).
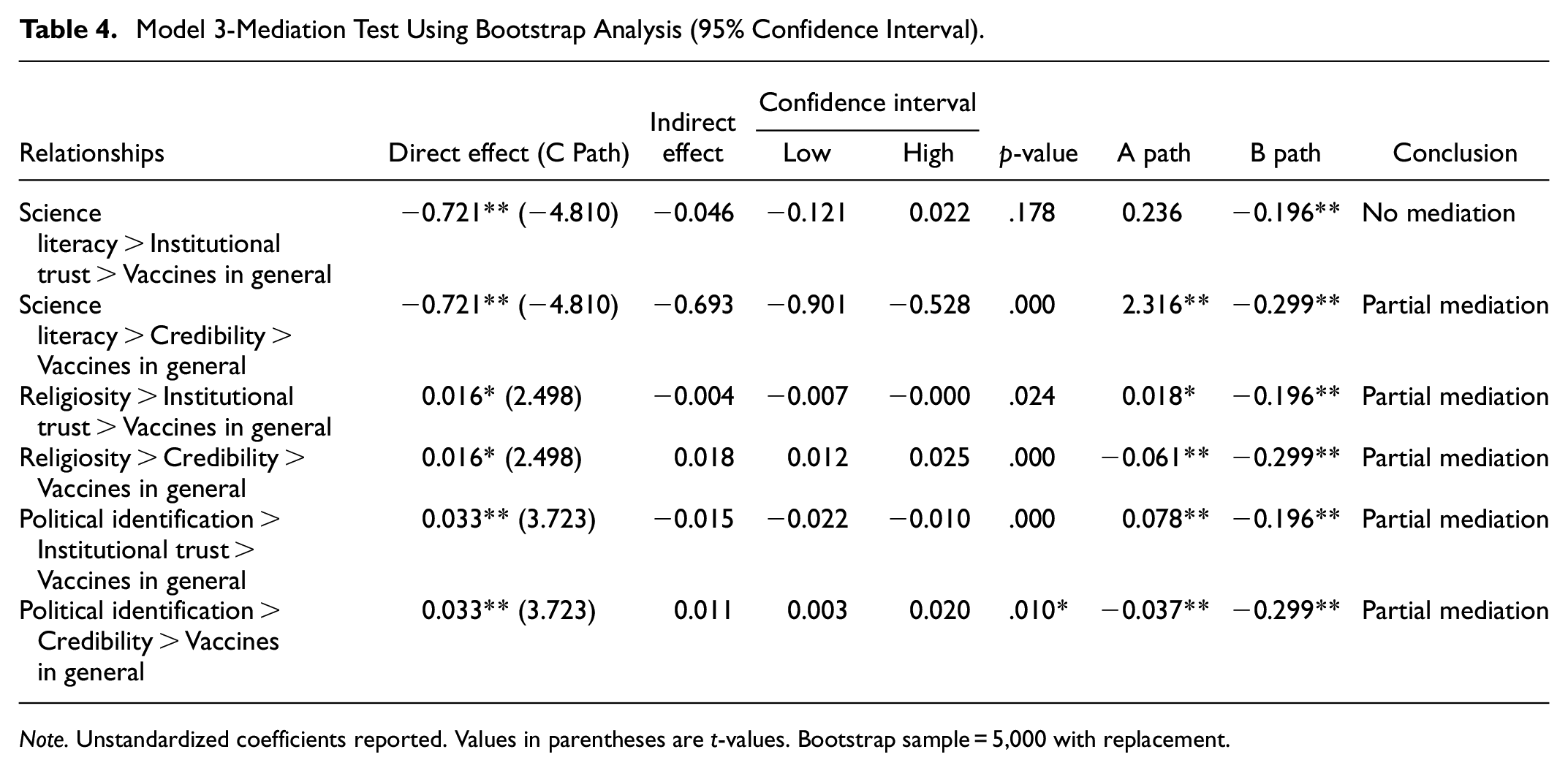
Note. Unstandardized coefficients reported. Values in parentheses are t-values. Bootstrap sample = 5,000 with replacement.
The results of the fourth model revealed that science credibility served as a full mediator of the connection between science literacy and attitudes toward COVID-19 vaccines. In contrast, there was no mediation of institutional trust since there was no connection between science literacy and institutional trust. Both institutional trust and science credibility were full mediators of the connection between religiosity and attitudes toward general vaccines. In the case of political identification, they represented partial mediators of the aforementioned connection. However, in concordance with Model 3, the two indirect paths had opposite outcomes in the cases of religiosity and political orientation (Figure 4).

Model 4 results (standardized coefficients).
The full details of the mediation analysis related to Model 4 are presented in the following Table 5.
Model 4-Mediation Test Using Bootstrap Analysis (95% Confidence Interval).

Note. Unstandardized coefficients reported. Values in parentheses are t-values. Bootstrapping sample = 5,000 with replacement.
p < 0.05. **p < 0.01.
The models were evaluated with an ML estimator. All four models indicated statistically significant chi-square values (p < .05), implying that the data do not perfectly fit the hypothesized models. However, as chi-square is sensitive to sample size, and as such, it is not the best index for model fit assessment (Peugh and Feldon, 2020). The Comparative Fit Index (CFI) values for all models are above 0.9, which represents an acceptable level of fit. The Tucker-Lewis Index (TLI) values are also above 0.9, also indicating adequate model fit. The Root Mean Square Error of Approximation (RMSEA) values range from 0.031 to 0.065, with all values below the recommended threshold of 0.08, suggesting that the models fit the data well. Additionally, the 90% Confidence Interval (CI) upper and lower bounds for all models do not include the threshold value of .08, indicating that the models have a good fit. The Standardized Root Mean Square Residual (SRMR) values range from 0.037 to 0.039, which is below the recommended threshold of 0.08, further supporting good model fit (Hu and Bentler, 1999). In summary, while the chi-square values suggest that the models do not perfectly fit the data, the other indices (CFI, TLI, RMSEA, and SRMR) indicate that the models represent a good fit to the data (Table 6).
Model Fits.

In Table 7, we summarized the results of the hypotheses testing. As can be noted, the role of science credibility (H1.1, H1.2., and H1.3.) in explaining the connection between scientific literacy, religiosity, and political orientation was confirmed. In contrast, institutional trust was not confirmed as the mediator of the connection between scientific literacy and vaccine hesitancy (H2.1.). The role of institutional trust when explaining the relationship between religiosity and hesitancy (H2.2.) and political orientation (H2.3.) was detected, but in the direction which was opposite to the one which was posited in the hypotheses. With respect to H3, the results, by and large, confirmed that the hesitancy determinants of COVID-19 vaccines and vaccines in general were similar.
Overview of the Hypotheses Testing.

Discussion
Overall, the results confirmed the mediating role of science credibility, while the mediating role of institutional trust was also detected, but not in a direction predicted by the stated hypotheses. The results also confirmed that by and large, the hesitancy determinants of COVID-19 and vaccines in general are similar. In other words, all specific hypotheses related to the first general hypothesis were confirmed, while all three specific hypotheses related to the second general hypothesis were rejected. As for the differences between hesitancy related to COVID-19 and vaccines in general, the only differences detected in the study were connected to the mediation differences in the case of science literacy and religion. Namely, in the case of COVID-19 vaccines, the connection between the two predictors was fully mediated, while in the case of vaccines in general the connection was only partially mediated.
As for H1.1, in the case of vaccines in general, science credibility served as a partial mediator of the connection between science literacy and vaccine hesitancy, while in the case of COVID-19 vaccines, science credibility fully mediated the connection. Therefore, H1.1 was confirmed since the mediating mechanism was detected in both cases. The confirmation of H1.1. leads to the conclusion that people with higher levels of literacy will have higher levels of trust in science, which ultimately leads to positive attitudes toward vaccines. While there are no studies analyzing the mediating role of trust in science in the context of general vaccines, we can note that Capasso et al. (2022) have established the mediating role of trust in science in COVID-19 attitudes in a specific population of unvaccinated men and women. The fact that science literacy was a full mediator in the case of vaccines in general, and only a partial mediator in the case of COVID-19 vaccines, can be explained by the special context in which COVID-19 attitudes have been formed. It can be hypothesized that in the COVID-19 vaccination context, institutional trust and trust in science were of more critical importance given the unknown nature of the new disease source, and, therefore, not completely related to knowledge/literacy. A study of COVID-19 vaccine hesitancy determinants in Croatia also found that the impact of distrust in science and scientists was particularly pronounced (Bagić et al., 2022). Institutional trust was not confirmed as a mediator of the negative association between scientific literacy and vaccine hesitancy, thus H2.1. was rejected. In contrast, Chen et al. (2022) found that institutional trust moderated the relationship between information overload/misinformation related to COVID-19 and COVID-19 vaccine hesitancy by reducing the connection. However, this study cannot be directly compared to the current study since COVID-19 overload and misinformation are more specific measures than science literacy.
Science credibility mediated the relationship between religiosity and vaccine hesitancy related to both vaccine types, confirming H1.2. Bearing in mind the contents of the scale with which we measured science credibility, the aforementioned mediating influence on the relationship between religiosity and vaccine hesitancy can be explained in two ways. First, it is possible that relying on religion in everyday life leads people to rely less on science, so that, among other things, they externalize responsibility for their health. This mechanism was confirmed in one study which determined that higher beliefs in an engaged God were associated with a lower probability of vaccination against COVID-19 (Upenieks et al., 2022). This was also confirmed by K. A. Johnson et al. (2021) since they determined that science and faith mindsets (beliefs concerning who is the source of truth and knowledge and who possesses problem-solving capacity when humanity is concerned) were strongly negatively correlated. Second, science and religion may be perceived as competing social identities, wherein scientists may be looked upon as members of a hostile outgroup who cannot be trusted. For instance, Chu et al. (2021) showed that religious persons will express higher levels of trust in medical professionals if similarities between their religious beliefs and those of medical professionals are accentuated. Moreover, in that study, religiosity moderated the effect, with more religious persons exhibiting higher susceptibility to common identity cues.
The established mediation role of science credibility on the relationship between right-wing political orientation and vaccine hesitancy confirmed H1.3. The results are in agreement with Kossowska et al. (2021) since they also established that political identification worked through distrust and negative perceptions of scientists. Even though in Croatia, before the COVID-19 pandemic, science topics have not been significantly present among political discussion topics, it seems that distrust in science and scientists is more present among people with right-wing political identification. Wollebæk et al. (2022) suggested that the opposition toward state power might be the reason why right-wing ideology is less positively disposed toward science and scientists, but we could not verify this in the current study bearing in mind that we did not measure ideological beliefs.
As for H2.2 and H2.3., they were not rejected based on the non-existence of the mediation mechanisms, as in the case of H2.1., but based on their direction, which was opposite to those predicted in the hypotheses. Namely, higher religiosity and right-wing political orientation were connected with higher institutional trust, which itself was connected with lower vaccine hesitancy. Therefore, this indirect path reduced vaccine hesitancy of right-wing and religious people. In comparison, as visible from H1.2. and H1.3., the path through science credibility was in the opposite direction. Our results are different from those established by Wollebæk et al. (2022) and Baumgaertner et al. (2018), bearing in mind that they also confirmed the mediating role of the institutional trust within the connection between political identification and vaccine hesitancy, but in the opposite direction than ours. Such findings indicate the importance of contextualizing religiosity and political orientation as determinants of vaccine hesitancy, that is, the importance of ad-hoc factors and specific socio-historical and socio-political circumstances. Namely, in Croatia, the connection between right-wing political orientation and religiosity and higher institutional trust can be interpreted by evoking deeper historical circumstances related to the nation-building and independence of the Croatian nation, as well as specific circumstances related to the COVID-19 pandemic. The independent Croatian state was created in the 1990s by the separation from socialist Yugoslavia. By definition, left-wing political orientation in Croatia is associated with less emphasis on nationalism, that is, national sovereignty. Accordingly, it is not surprising that among right-wing and religious people there is more pronounced attention to the independent state as a constitutive political principle, and thus a connection with stronger trust in the institutions of the Croatian state (Franc et al., 2020). This connection is even stronger because the institutions listed in the survey questionnaire included legislative, executive, and judicial institutions. In a broader context, some empirical data on changes in value orientations (Sekulić, 2012) showed that after the collapse of socialism in Croatia re-tradionalization took place in dimensions of nationalism and religiosity. Furthermore, the fact that for the entire duration of the COVID-19 pandemic, as well as today, the center-right party is in power in Croatia is also very important. Therefore, stronger trust in institutions probably reflected stronger trust in the current power holders. Another finding in a previous Croatian study (Bagić et al., 2022) indicated that vaccine-hesitant respondents were more distrustful toward scientists but they were more likely to trust the government.
As for the differences between COVID-19 vaccine hesitancy and vaccine hesitancy in general, most determinants were generally the same. Namely, younger age, right-wing political orientation, higher religiosity, and lower scientific literacy were connected with higher hesitancy in both cases. All other mediation mechanisms were confirmed in both cases, with the exception that scientific literacy was not directly connected with COVID-19 vaccine hesitancy, while this was the case for general vaccine hesitancy. In this regard, the results of the current study confirmed previous findings which determined that vaccine hesitancy determinants both before and during the COVID-19 pandemic were similar (e.g., Dombrádi et al., 2021; Meier et al., 2021). Therefore, even though COVID-19 vaccines had been developed and applied in very special circumstances, the overall determinants of vaccine hesitancy might be deeply rooted in psychological dispositions and the more lasting socio-structural conditions.
Conclusion
In this study, we aimed to extend previous research on vaccine hesitancy by exploring mediation mechanisms that connect scientific literacy and values (religiosity and political orientation) with vaccine hesitancy. In addition, we aimed to test whether the determinants of vaccine hesitancy and the mediating mechanisms are similar in vaccine hesitancy in general and COVID-19 vaccine hesitancy. Our results confirmed that science credibility plays a significant role as a mechanism that translates the impacts of literacy, religiosity, and political identification. On the other hand, the results related to institutional trust as a mediating mechanism point to a conclusion that its role should be contextualized, having in mind that the connection between religion, politics, and institutional trust might be dependent upon specific socio-historical circumstances, and/or ad-hoc factors related to the current relationship between power holders and other institutional actors. In addition, the results of our study confirmed that the determinants of vaccine hesitancy probably have not significantly changed with the outbreak of the COVID-19 health crisis, thus indicating that they might be connected to the deeply rooted value dispositions.
Overall, our results point to the importance of building trust in science as a factor in reducing vaccine hesitancy, especially when it comes to groups with stronger resistance to vaccination. The fact that trust in science is a full mediator of the relationship between scientific literacy and vaccine hesitancy points to the need for stronger and more comprehensive science education, with a goal of building positive attitudes and trust. Contemporary topics related to science are extremely complex, and it does not seem that misunderstandings with groups that reject the scientific consensus can be resolved simply by providing additional information, but by developing general positive attitudes toward science, whereby science education is an important part of building trust. This opens up new venues for future research of a more general nature, which might explore whether the effect of knowledge on positive attitudes toward science is really the result of a better understanding of the debated scientific topics, which leads to less frequent rejections of scientific consensus, or whether it is a matter of knowledge creating greater respect for scientific findings and the scientists’ work, even when it does not allow a deeper understanding of the disputed issues.
The main limitation of the study stems from the specific approaches that we took when deciding which measurements to include in the study. For instance, science literacy was measured as content literacy, this being only one of the possible approaches when approaching the topic. Therefore, future studies should test the results by using different measures of the constructs employed in this research study. In addition, taking into consideration the context-dependence of vaccine hesitancy, validation of our findings among other populations is warranted. Another notable limitation of this study is the use of opt-in self-administered data collection, which offers limited control and may introduce selection biases and a potential lack of representativeness (Einarsson et al., 2022; C. Zhang et al., 2020).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was fully supported by the Croatian Science Foundation under Grant IP-2019-04-7902.
Ethical Approval
Ethics Committee of the Faculty of Humanities and Social Sciences Josip Juraj Strossmayer University of Osijek approved the study (Ethical approval code: 2158-83-02-19-2).