
Abstract
This study aimed to determine the factors influencing the community’s acceptance of booster vaccination, focusing on sociodemographic characteristics, knowledge, media exposure, and attitude. An analytical observational design was used with a quantitative method and cross-sectional study. The data were collected in September and October 2023 through a digital questionnaire using the Google Forms platform distributed by Line, WhatsApp, Instagram, Twitter, and TikTok, and 425 respondents from Indonesia were selected. Data analysis included univariate, bivariate (Chi-Square Test), and multivariate analyses (Multiple Logistic Regression Test) using IBM SPSS Statistics. The results showed that the majority of respondents possessed good knowledge (51.8%), were actively exposed to the media (99%), and showed a positive attitude toward booster vaccination (57.9%). Furthermore, this study showed that gender, education, knowledge, and attitude had a statistically significant relationship with the community acceptance of booster vaccination and education was found to be the most influential variable in the community acceptance of booster vaccination. The education levels and knowledge were found to have a significant relationship with the attitude and actions of the community. To face the threat of a future pandemic, the government can focus on equal distribution of education and dissemination of information related to disease (prevention, symptoms, treatment, and more) while also building public trust in the government and health workers. This study aims to see the overview of public knowledge, attitudes, and behavior towards booster vaccines in Indonesia. The factors that influence people to do or not do booster vaccines are very diverse. Therefore, the results of this research can be used for future learning when a pandemic is possible. This research was conducted using online questionnaires and shared through social media. The respondents in this study are Indonesian citizens who are adults or over 18 years old the results of this research indicate that education is the dominant factor influencing people to get a booster vaccine Therefore, education should be maximized to enhance booster vaccination in case of future pandemics
Introduction
The COVID-19 pandemic was declared over, but cases were still reported in healthcare services with new variants suspected to be more infectious. Vaccination is a crucial effort to reduce the spread of the virus, decrease case surges, and lead the community out of the pandemic (Kementerian Kesehatan Republik Indonesia, 2021). The Centers for Disease Control and Prevention (CDC) recommended a third vaccine dose for individuals with immune disorders (Center for Diseases Control and Prevention, 2021; Shekhar et al., 2021). Globally, 66.8% of the population has received at least one dose (World Health Organization, 2022). The decline in vaccine-induced immunity, coupled with the emergence of SARS-CoV-2 variants, has led to an increase in new infections, thereby prompting consideration for booster doses (Burckhardt et al., 2022). There is a growing concern that the two doses may not produce sufficient antibody responses to protect individuals from the virus (Jørgensen et al., 2022). The third dose, also known as “booster,” has been implemented for COVID-19 vaccination with some countries considering a fourth dose. It is important to acknowledge that booster injections are available for Pfizer-BioNTech recipients who received their previous vaccine at least 6 months ago and are aged 65 and above, as well as those aged 18 years and above in long-term care, have certain medical conditions, working in high-risk environments, and living in high-risk environments (Center for Diseases Control and Prevention, 2021).
Based on the Ministry of Health Circular Number HK.02.02/II/252/2022, booster vaccination is for individuals aged 18 and above, in good health, who received the second dose at least 3 months ago, possess a National Identity Card (KTP), have vaccination reappointment ticket in PeduliLindungi apps, and currently not declared positive for COVID-19 (Corona Jakarta, 2023). However, the third or subsequent doses have the potential to increase antibody titers against SARS-CoV-2 and its variants, specifically in individuals with compromised immune systems, have underlying comorbidities; or are at increased risk of exposure and transmission of COVID-19 (Shekhar et al., 2021). Booster vaccination is necessary to maintain immunity and extend the protection period from primary vaccination (Corona Jakarta, 2023). There are three reasons for administering additional doses (World Health Organization, 2021a): (1) Individuals may not adequately respond to the first two doses received. The World Health Organization (WHO) stated that individuals with immune disorders may need a third dose because the first two doses might be less effective compared to normal, healthy individuals (World Health Organization, 2021a); (2) Over time, the immunity acquired through vaccination may diminish, deteriorate, or decrease. Current evidence shows that vaccines remain highly effective in protecting individuals from severe disease, hospitalization, or even death. There is no strong evidence suggesting the need for a third dose for vaccinated individuals (World Health Organization, 2021a). Although the efficacy of vaccination in preventing infection may decline over time, current data shows that effectiveness against severe disease, hospitalization, and death remains high (Rzymski et al., 2021); (3) Vaccine performance may be insufficient against new variants of concern. The currently available vaccines are effective against SARS-CoV-2 variants and WHO monitors this situation closely (World Health Organization, 2021a).
A Preliminary study conducted in China showed a relatively large proportion of respondents receiving booster vaccination, but more efforts are needed to enhance perceived benefits and reduce barriers to boost acceptance (Lai et al., 2021). Among Danes, an estimated 87% (95% CI [86.3, 87.8]) of the adult population were willing to receive booster (Jørgensen et al., 2022). Furthermore, a study on healthcare workers given boosters showed that only 7.9% (n = 107) of respondents were hesitant to take the first or second dose (Burckhardt et al., 2022). Younger age (18–40 years) and lower education levels are associated with hesitancy toward higher doses, while self-identified Asian racial identity correlates with greater acceptance of vaccination (Pal et al., 2021). Among vaccine-hesitant groups, more respondents express distrust in regulatory authorities (45.3%), government (48.6%), and pharmaceutical companies (50%) than in doctors (25.4%). Almost two-thirds of respondents were concerned that vaccination may not be effective against new strains, and acceptance of a hypothetical booster among hesitant respondents was only 14.3% (Pal et al., 2021). In general, vaccine hesitancy was observed to have similar demographic predictors. In a previous study, the hesitancy of some U.S. healthcare workers to receive boosters reflected general reluctance toward receiving other forms of vaccination (Pal et al., 2021). Meanwhile, in Indonesia, there has not been much study on the acceptance of booster vaccines, even though this is a government program that needs to be successful. The knowledge, attitudes, and practices of the Indonesian people towards booster vaccines need to be assessed for the government to evaluate the program and prepare for future vaccination programs.
The government needs to develop guidelines for the use of boosters while considering the potential risks of waning immunity and new virus variants as well as prioritizing vulnerable populations globally, including those in low-income countries. Several factors influence the acceptance, hesitancy, and rejection of COVID-19 vaccines. Therefore, it is essential to investigate whether similar factors apply to booster, given the intended purpose of providing enhanced protection against COVID-19. Study on acceptance, hesitancy, and rejection of both third and fourth booster doses is crucial. However, it is necessary to apply appropriate criteria for the use of third or subsequent additional doses without jeopardizing global vaccination efforts (Shekhar et al., 2021). The effectiveness of the booster has been known to be able to enhance immunity against new variants (Koh et al., 2022) and reduce infection rates, severity of disease, and death from COVID-19 (Khalisha et al., 2024). Despite that, the coverage for all three injections (first, second, and booster) in Indonesia has not yet reached 80% (Kementerian Kesehatan Republik Indonesia, 2022). Several challenges include low community acceptance, government-prepared vaccine availability, and insufficient information about vaccination implementation (Arifin & Anas, 2021). The community acceptance of boosters also could be linked to individual knowledge and attitude, because a person takes an action based on the knowledge and attitude towards the topic (Rachmawati, 2019). To increase public acceptance towards booster, a study about factors that affect vaccine (booster) acceptance is needed.
Despite the need for community awareness about booster vaccination to ensure successful government programs, limited studies have been conducted on vaccination implementation in the community. Therefore, the results of this study could provide a basis for government policy and health workers in developing guidelines for the implementation of booster vaccinations in the future. Studies on COVID-19 booster vaccination are relatively limited and less explored especially those related to the acceptance of booster vaccines. Therefore, this study provides insights into public acceptance of COVID-19 booster vaccination in Indonesia focusing on barriers and factors causing hesitancy to participate in mitigating the impact of the pandemic including booster vaccination and taking lessons learned from the past COVID-19 pandemic. Identifying risk factors can assist the government and health officials in developing policy and preparation to face the challenges of the upcoming pandemic.
Methods
Study Design
This study used an epidemiological design with an observational analytical technique through quantitative cross-sectional methods order to be able to assess multiple variables simultaneously (Setia, 2016). The analysis examined the relationship between the community acceptance of booster vaccination as the dependent variable with sociodemographic characteristics, knowledge, attitude, and media exposure being the independent variables.
Study Location and Time
The study was conducted online through a digital questionnaire using the Google Forms platform distributed by Line, WhatsApp, Instagram, Twitter, and TikTok in 2023 among Indonesians. The questionnaire was distributed online from September to October 2023.
Population and Sample
The population for this study comprised eligible individuals in Indonesia who qualified to receive vaccine boosters. The minimum required sample size was 385, obtained from the Lemeshow formula. This study used a 95% confidence level with a 5% margin of error and a perfect proportion value of 50%. The population size uses data from the Indonesian Central Bureau of Statistics, which is Indonesians aged 17 years and over, amounting to 188 million people Indonesian Central Bureau of Statistics (2022). With an additional 10% to account for potential incomplete question responses, the number of samples used in this study was 425 samples. Inclusion criteria consisted of respondents aged 18 and above who were capable and willing to complete the questionnaire. Exclusion criteria consisted of respondents who provided duplicate responses or failed to complete the questionnaire in its entirety. Duplicate responses were identified by reviewing emails. The questionnaire on the Google form has also been set to accept only one response, so this effort is considered to reduce the risk of multiple responses from one person.
Study Instrument
The questionnaire was developed based on references from (Abullais et al. 2022; Chilongola et al. 2022; Wang et al. 2022) using variable components of knowledge, attitudes, and practices and adapted to specific needs. Subsequently, validity and reliability tests were carried out with the reliability results deeming the questionnaire reliable. Validity and reliability tests were using the Correlation Pearson Product Moment test. The validity test results for the attitude variable included twelve valid questions, while the knowledge variable comprised nine. Taber (2018) explained that cronbach’s alpha values are commonly interpreted using the following rule of thumb ≥.90 indicates excellent reliability, ≥.80 indicates good reliability, and ≥.70 is considered acceptable. The reliability test showed a Cronbach’s alpha value of .809 for the knowledge variable and .861 for the attitude variable. These results indicate that the instruments made to measure these variables are consistent and reliable for measuring each variable. That way the results produced describe these variables well. Knowledge was categorized as “good and poor,” while attitude was considered “positive and negative” by observing the cut-off point using the median. Furthermore, social media usage was categorized as “more than 3 hrs per day and 0–3 hrs per day.” The community acceptance of booster vaccination was grouped as “implementing and not implementing.” Sociodemographic characteristics queried were residential location, gender, age, ethnicity, occupation, education, and comorbidity status. Media variable was tested by assessing the time spent by individuals on social media per day. Finally, the community acceptance of booster vaccination was determined by the willingness of individuals to undergo either the third or fourth injection.
Data Collection and Analysis
This study used primary data collected directly through a questionnaire using the Google Forms platform. The questionnaire was distributed online through Line, WhatsApp, Instagram, Twitter, and TikTok to the community and 425 respondents from Indonesia were selected. Data analysis included univariate, bivariate, and multivariate analyses. Univariate analysis was conducted to observe the distribution of sociodemographic characteristics in terms of frequency and percentage. Moreover, the bivariate analysis used the Chi-Square test to examine the relationship between independent and dependent variables with a significance level of .05. Multivariate analysis used the multiple logistic regression test, where variables with a p-value <.25 were included in the modeling. Variables with a p-value >.05 were removed from the modeling and the test was repeated until the final modeling results were obtained. The final results showed variables with a p-value <.05 (95% Confidence Interval [CI]), signifying that these independent variables had a significant relationship with the dependent. The Exp(β) value signified the extent of the influence of independent variables on the dependent. All data analysis processes were performed using IBM SPSS Statistics open access version 23.
Results
The variables of this study consisted of location, gender, education, occupation, comorbidity status, age, ethnicity, knowledge, and attitude. The frequency distribution of the variable is presented in Table 1. It shows the overview of respondents in this study, with the majority living in urban areas (65.9%), females (78.6%), had a diploma education or higher (52%), unemployed (66.1%), had no comorbidities (96.7%), between the age of 18 to 24 (74.1%), and mostly Javanese (56.2%). Furthermore, the knowledge variable was measured using questions related to information about COVID-19 and vaccination. Respondents in this study were dominated by those with good knowledge about vaccination (51.8%) and predominantly characterized by a positive attitude toward booster vaccination (57.9%). Moreover, the media exposure variable was measured using questions related to booster vaccination information. The frequency distribution of questions related to media exposure is shown in Table 2.
Demographic Characteristics, Knowledge, and Attitude of Respondents Towards Booster Vaccines (n = 425).

Media Exposure to Respondents Related to Booster Vaccine of COVID-19 (n = 425).
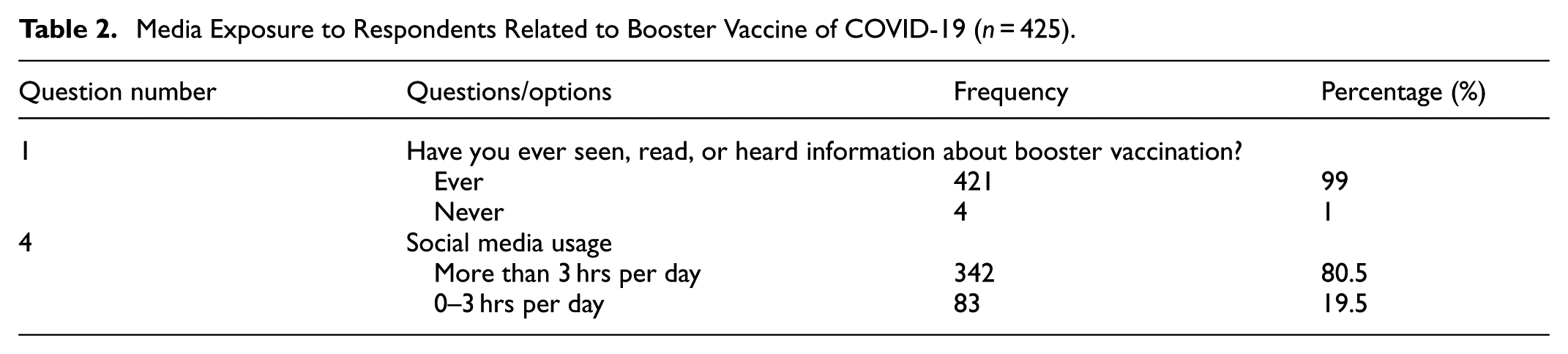
Table 2 shows the overview of respondents in this study, primarily consisting of those who have ever seen, read, or heard information about booster vaccination (99%) from websites/online news (19.6%) and using social media more than 3 hrs per day (80.5%). The frequency distribution of questions related to media sources is presented in Table 3. It shows an overview of media sources where respondents acquire information about booster vaccination, dominated by websites/online news (64.9%) and Instagram (63.5%). Subsequently, the attitude variable was measured using questions related to COVID-19 and booster vaccination. Furthermore, bivariate analysis was conducted using the Chi-Square test to determine the relationship between the two variables. The results for each variable are presented in Table 4. Table 4 showed that after conducting the Chi-Square test, four variables were found to be significant toward the community acceptance of booster vaccination, namely gender, education, knowledge, and attitude, with a p-value <.05.
Type of Media that Provides Exposure to Respondents about Booster Vaccines.

Note. Have you received information about booster vaccines from the following media? (n = 425).
Bivariate Analysis of Demographic Characteristics, Knowledge, Attitude, and Media Exposure Toward Acceptance of Booster Vaccination.

Variable with p < .05 and entering the multivariate analysis.
Multivariate analysis was subsequently performed using multiple logistic regression to identify the most dominant variables influencing acceptance of booster vaccination. The final results of the multiple logistic regression modeling are shown in Table 5. The final results of the logistic regression modeling after eliminating variables with a p-value >.05 are presented in Table 5. It shows two final variables, namely education (p = .0001) (OR = 2.881, 95% CI [1.648, 5.036]) and attitude (p = .006) (OR = 2.103, 95% CI [1.235, 3.583]). Based on Exp(β), education was found as the most influential variable on the community acceptance of booster vaccination with an Exp(β) of 2.881, which was higher than attitude at 2.103.
Multivariate Analysis Using Multiple Logistic Regression.

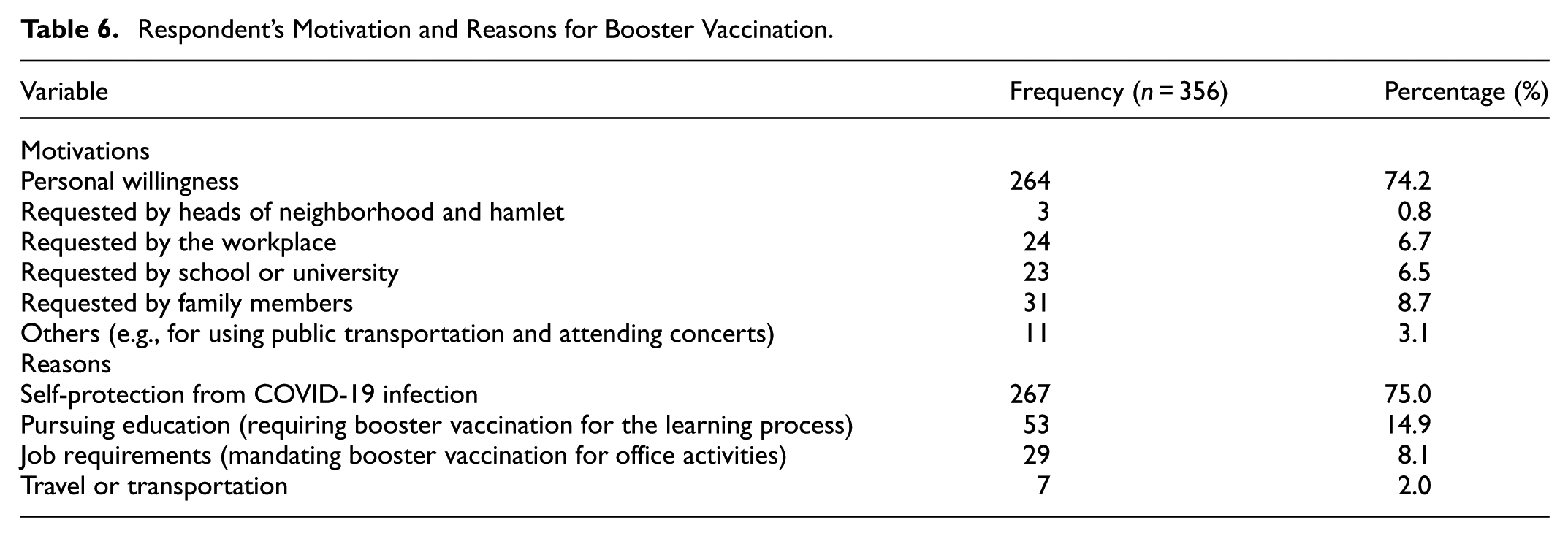
Among the 356 respondents who received booster, the overview of motivations and reasons leading to the implementation of booster vaccination is as follows in Table 6. It shows that the majority of the community implemented booster vaccination based on personal willingness, showing a widespread awareness of its importance. This was also supported by the results that most individuals had implemented booster vaccination to protect themselves from COVID-19 infection.
Respondent’s Motivation and Reasons for Booster Vaccination.
Discussions
The majority of respondents in this study were found to possess good vaccination knowledge at 51.8%, only slightly different from those with poor knowledge. Knowledge is crucial in shaping actions, as it is the basis of decision-making and action (Zheng et al., 2022). Without having any knowledge about COVID-19 and the booster vaccine, people can not make decisions and take any action. A study about health knowledge, behavior, and attitudes during the pandemic found that people who possess good health knowledge have a higher probability of adopting health behavior and practices, helping them to understand and take action more quickly (Uribe et al., 2021). The media exposure variable provided a more specific depiction of how respondents acquire knowledge about COVID-19 and booster vaccination. Social media is a platform where individuals can share and access various information, often without strict regulatory measures regarding accuracy. Given the wide and easy access, many individuals and health organizations use social media for health intervention, promotion, and education. However, the community needs to fact-check health information because misinformation can have fatal consequences (Samy et al., 2020). A study in China found that lower vaccine hesitancy was associated with higher vaccine literacy, with the conclusion that making it easier to access information and increasing people’s ability to evaluate this information (through education/schools) could reduce acts of rejection of vaccines (Lu et al., 2023). This study found that education had a significant relationship with the community acceptance of booster vaccination with an Odds Ratio of 2.930. This result suggests that individuals with a diploma or higher education have a tendency three times greater to implement vaccination compared to those with a Senior High School or lower education. In line with education, knowledge also showed a significant relationship with the community acceptance of booster vaccination with an Odds Ratio of 1.842. This means that individuals with good knowledge have a tendency two times greater to implement vaccination compared to those with poor knowledge. Similar results were found in a study conducted in West Java where knowledge correlated with the willingness to implement booster vaccination (Aprilia et al., 2022). Another study in Central Java reported a significant relationship between knowledge and booster vaccination behavior in the community (Purwesti et al., 2024). A study in South Korea also found that booster hesitancy was more common among people with lower education levels (Limbu & Huhmann, 2023). . education was one of the most significant determinants of CBVH, but had inconsistent results. Most of the studies found that people with lower education levels were more likely to have booster hesitancy, but some other studies had the opposite results (Noh et al., 2022). The results of the education and knowledge variables are consistent with the concept that knowledge shapes actions (Wendlandt Amézaga et al., 2022). High education forms better thinking patterns and broader knowledge, resulting in a greater tendency to implement booster vaccination.
The attitude was predominantly positive toward booster vaccination (57.9% n = 425), with only a slight difference from the negative attitude (42.1% n = 425). The attitude reflects the acceptance and rejection of respondents toward booster vaccination. Rejection may be influenced by the perception/information that primary vaccination is sufficient to combat COVID-19 (World Health Organization, 2021b). This perception triggers rejection or delay, even though booster vaccination can help enhance community immunity in the transition of COVID-19 from a pandemic to an endemic state (Limbu & Huhmann, 2023). The attitude of the community also showed a significant relationship with acceptance of booster vaccination with an Odds Ratio of 2.153. This means that individuals with a positive attitude have a tendency twice as great to implement vaccination compared to those with a negative attitude. In contrast, the previous study carried out on street vendors in Cimanuk, West Java did not find a significant relationship between attitude and the community acceptance of booster vaccination (Agustiani et al., 2023). Many respondents had a positive attitude toward booster vaccination, but many failed in the implementation stage (Agustiani et al., 2023). According to Agustiani et al., this may be attributed to the presence of comorbidities/diseases in individuals. Another study found a significant relationship between attitude and interest in receiving booster vaccination (Isnaini et al., 2021). Attitude plays a crucial role in the community’s acceptance of vaccination and disease prevention strategies. Health workers should play their role in shaping the attitude of the community toward healthy behavior, specifically in acceptance of vaccination (Abdelmoneim et al., 2022). The results also showed that gender had a significant relationship with the community acceptance of booster vaccination, suggesting males were three times more likely to implement vaccination than females. In contrast, a previous study conducted at one health center in Minahasa Regency, North Sulawesi did not find a significant relationship between gender and acceptance of COVID-19 vaccination (Pantow et al., 2022). Another study in the United States found that men are more likely to have lower hesitancy towards the COVID-19 vaccine than women even though they have higher agreement with other public health preventive measures; caused by low level of trust in the government and misinformation about the side effects of the vaccine specific to women’s health (Jayawardana et al., 2024). These disparities may be attributed to variations in the study locations, about sociodemographic characteristics. This suggests that socialization and intervention in the community should not be solely based on gender. Many other factors can be considered to aid the community in implementing booster vaccination or other health behaviors. In general, it has been found that women develop higher antibody responses and experience more side effects compared to men towards many vaccines (Jensen et al., 2022).
The multivariate analysis results showed that education and attitude had a significant relationship with the community acceptance of booster vaccination. Education had an Exp(β) of 2.881, while that of attitude was 2.103. This disparity implied that education was the most dominant variable influencing the implementation of booster vaccination among individuals. The government should make more significant efforts to improve the quality and accessibility of education in Indonesia, specifically the formal type. Additionally, given that attitude is a significant influencing factor, attention should be directed toward aspects affecting how individuals perceive booster vaccination, including health conditions, and diseases as well as exposure to misinformation (Agustiani et al., 2023). Education is also in line with knowledge as a factor shaping the behavior of an individual (Wulandari et al., 2021). Furthermore, knowledge can be influenced by occupation and educational background (Moudy & Syakurah, 2020). In this context, television, mobile phones, counseling, or even relatives may be sources of information. Mass media provide new information for the community that forms cognitive foundations shaping knowledge (Wulandari et al., 2021). However, the information available in the media is not necessarily correct. A study found that anti-vaccine information is one of the factors causing vaccine hesitancy (Ullah et al., 2021). Myths and conspiracies related to COVID-19, for example, the controversy over the safety of the COVID-19 vaccine have seriously damaged public trust in the vaccine (Ullah et al., 2021).
The motivation to implement booster vaccination should start with individuals themselves, as evidenced by the majority of the community. At the beginning of the COVID-19 vaccination rollout, the Indonesian government implemented legal measures mandating all citizens to comply except for certain groups. In some cases, such as when traveling long distances by plane or train and entering public places including malls, individuals are required to show a vaccination certificate. These regulations, although perceived as coercive by some people, were necessary measures taken by the government to safeguard public health and halt the pandemic (Bustomi, 2022). The implementation of booster vaccination follows a similar process but with more relaxed conditions, leading to voluntary participation by many individuals. Social media is an essential tool for health promotion, with both positive and negative impacts on knowledge and attitude of the community. Social media can be a source of misinformation and fear, but it also has the potential to counter misinformation through appropriate education, specifically preventive efforts. Media literacy is needed to strengthen the confidence of the community in their knowledge, fostering critical thinking skills to discern information circulating on social media and effectively intervening in health promotion (Melki et al., 2022). Social media is an excellent tool for increasing public access to health information with the hope of promoting positive changes in health behavior (Leonita & Jalinus, 2018). Therefore, social media should be maximally used to promote health. Studies in China showed that the most popular social media platforms in the country including WeChat, Weibo, and TikTok play a vital role in influencing the behavior of users (Li & Liu, 2020).
Despite the evident benefits, many individuals still harbor hesitancy toward receiving booster vaccinations. For example, a study in the East Mediterranean Region found that the reasons for refusing booster vaccination were believing that the vaccine was ineffective/useful/no benefit and fear of vaccine side effects (Ghazy et al., 2022). A study among the university academic community in Bangladesh found factors that reduce the desire for booster vaccination are side effects of booster vaccines and booster skepticism (Roy et al., 2023). Therefore, it is recommended to carry out health interventions that focus on knowledge of the effects of booster vaccines. Based on a systematic review, booster confidence (in the vaccine, healthcare services, healthcare workers, and others), complacency (self-satisfaction), and convenience (ease of getting the vaccine) are three factors consistently influencing hesitancy about booster vaccination (Limbu & Huhmann, 2023). These three factors are influenced by various aspects, such as vaccine access, perceptions of severity and vulnerability, skepticism, normative influence, bad experiences, and others. Therefore, interventions targeted at improving these factors are needed. In the future, when a pandemic reoccurs and vaccination is required, socialization and education in the community are crucial to shaping good knowledge and attitude. Good knowledge and attitude would lead people to take positive action, because knowledge, and attitude, along with culture, perception, and sociodemographic characteristics are predisposition factors for determining action (Rachmawati, 2019). The motivations and reasons for respondents to take booster vaccines as a result of this study can be used as a base or reference for creating a program or health promotion for the government and health workers if a pandemic occurs in the future. Health programs or health promotions carried out by the government based on the motivations of these respondents will result in higher awareness for the community to voluntarily support ongoing health programs. In the end, the highest public health is the ultimate goal of all existing health programs.
The strengths of this study lie in the timing, namely at the end of the pandemic to assess acceptance of booster vaccination in Indonesia when COVID-19 cases were on the decline. This could serve as a reference for further study when a pandemic occurs in the future. The results also have the potential to guide the formulation of strategies for implementing booster vaccination in the future. The information on the knowledge, attitudes, and behaviors of the Indonesian people towards booster vaccines from this study can be used as a reference to evaluate government policies in health promotion. However, this study has some limitations, firstly, due to the use of a cross-sectional design, the results cannot explain a cause-and-effect relationship. All variables were collected at the same time and could not describe other influences outside of these variables such as the experiences of the respondents. However, this study has described the condition of the community’s knowledge, attitudes, and behavior toward booster vaccines and their statistical correlation. Secondly, data collection was carried out using an online questionnaire, thereby introducing the possibility of bias. Bias may occur when respondents have different perceptions of the questions being asked. However, efforts were made to minimize bias, such as creating a questionnaire based on previous studies in other countries with adjustments and simplifying the language for online use. Lastly, reasons for the community to forgo booster vaccination were not addressed, suggesting a potential variable for further study. This study only resulted in respondents’ motivations and reasons for getting the booster vaccine and did not provide questions for those who did not take it. In future studies in different cases, the researchers may consider providing these questions to both sides of the respondents.
Conclusions
In conclusion, four variables (gender, education, knowledge, and attitude) were found to be significant towards COVID-19 vaccine booster acceptance with education and attitude as the most dominant variables influencing acceptance of COVID-19 vaccine booster. According to the results, the government should focus on education by ensuring education equality and regulating the information about diseases (prevention, symptoms, treatment, and more) while also building public trust in the government and healthcare workers. Knowledge could be acquired through formal education and information circulated in the mass media, including social media. The community acceptance of booster vaccination in Indonesia was generally positive and was influenced by education level and attitude. Therefore, healthcare workers were tasked with shaping a positive attitude in the community to promote health improvement. The government can enhance the overall education quality in Indonesia, fostering a more educated and critical community. Moreover, the government, healthcare institutions, and health influencers should create engaging educational content on various social media platforms, specifically on websites and Instagram. This ensures that the community is exposed to credible information while combating misinformation. In the era of social media, people in Indonesia must be able to filter information received from social media. Literacy intelligence is needed to distinguish false information that may be circulating. The best way is to trace the information obtained and double-check it from several sources. So that negative information about booster vaccines or others can be combated.
Footnotes
Acknowledgements
The authors are grateful to the University of Indonesia for funding this study through the Directorate of Research and Development with the International Indexed Research Grant (PUTI) Q1 Fiscal Year 2023-2024, contract number: NKB-434/UN2.RST/HKP.05.00/2023. The authors are also grateful to all respondents.
Ethical Considerations
The research has been ethically tested and has passed ethics with the issuance of an Ethics Approval Letter with No. Ket-635/UN2.F10.D11/PPM.00.02/2023. Data from this study were obtained from respondents who had been given an explanation of everything about this study and they had agreed to become respondents in this study.
Consent to Participate
Informed consent was obtained from all participants involved in the study.
Funding
This study was funded by the Directorate of Research and Development with the International Indexed Research Grant (PUTI) Q1 Fiscal Year 2023-2024 with contract Number: NKB-434/UN2.RST/HKP.05.00/2023
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.