
Abstract
Stigma and discrimination against people living with HIV (PLHIV) can seriously affect their mental well-being and overall health. However, limited research has focused on the most economically active age group. This study sought to measure the extent of HIV-related stigma and examine the factors associated with discriminatory attitudes. This study utilized data from a nationwide survey conducted in 2020. The survey employed a cross-sectional design with a complex sampling strategy to ensure national representativeness. Data on HIV stigma were collected through a self-administered questionnaire due to the sensitive nature of the items. A total of 2,818 individuals aged 15 to 49 years who responded to the HIV stigma module, which assessed six stigma domains, were included in the analysis. IBM SPSS Statistics version 29.0 was used to conduct descriptive analyses and multivariable logistic regression. The prevalence of the global indicator for discriminatory attitudes towards PLHIV was 78.7%. Additionally, the prevalence of each six HIV stigma domains was: experienced stigma (70.3%), fear of HIV infection (64.4%), discrimination (60.6%), anticipated stigma (57.6%), social judgment (44.9%), and perceived stigma (42.2%). Multivariable logistic regression analysis identified lower education levels (aOR: 2.42, 95% CI [1.85, 3.15]) and rural residence (aOR: 1.57, 95% CI [1.20, 2.04]) as significant factors associated with discriminatory attitudes towards PLHIV. HIV-related stigma and discrimination remain common among individuals aged 15 to 49 years in Malaysia. Effective and timely action is needed to address these issues and contribute to the global effort to end the AIDS epidemic by 2030.
Plain Language Summary
HIV related stigma and discrimination continue to be major public health challenges that affect people living with HIV (PLHIV). These negative attitudes can limit access to testing, treatment, and support, and worsen mental health and quality of life. Despite its importance, few studies in Malaysia have focused on HIV stigma among people in their most productive years, those aged 15 to 49. This study used data from a nationwide health survey carried out in 2020. A total of 2818 individuals aged 15 to 49 years responded to questions on HIV stigma, which included six types of stigmas, such as fear of infection, social judgment, experienced stigma, anticipated stigma, perceived stigma and discrimination. Because the topic is sensitive, the questions were answered through a self-administered survey. The data were analyzed using statistical software to explore patterns and factors linked to stigma. This study found that nearly eight in ten people in Malaysia aged 15 to 49 held negative or unfair attitudes toward PLHIV. Many also believed or felt stigmas such as fear of getting infected (64.4 percent), having personally experienced stigma (70.3 percent), or discrimination (60.6 percent). Other common views included expecting to be treated badly if diagnosed (57.6 percent), judging others with HIV (44.9 percent), and feeling ashamed or isolated (42.2 percent). People with lower levels of education and those living in rural areas were significantly more likely to hold discriminatory views. These results suggest that stigma and discrimination are still widespread among Malaysian adults in this age group. Addressing these issues is crucial for improving HIV prevention and treatment efforts. Public education, especially for rural communities and those with limited schooling, could help reduce stigma and support Malaysia’s goal of ending the AIDS epidemic by 2030.
Introduction
HIV stigma refers to negative beliefs, feelings, and attitudes directed toward people living with HIV (PLHIV), often resulting in prejudice, marginalization, and discrimination (Joint United Nations Program on HIV/AIDS [UNAIDS], 2024a). Theoretical frameworks such as Goffman’s stigma theory and Link and Phelan’s conceptualization emphasize that stigma arises when individuals are discredited based on socially constructed stereotypes, which limits their social functioning and reinforces inequality (Blom et al., 2023). These dynamics remain central in understanding how HIV stigma persists and affects health-seeking behavior. Stigma and discrimination have profound negative effects on PLHIV, impacting their overall well-being, social acceptance, access to Human Immunodeficiency Virus (HIV) testing, and treatment adherence (Musheke et al., 2013). Such stigma often stems from associations with socially taboo behaviors, such as injecting drug use or engaging in non-marital sexual activity, which remain sensitive topics in many settings, including Malaysia. According to the Centers for Disease Control and Prevention (CDC), stigma may arise when individuals perceive that PLHIV deserve their condition due to personal choices, often compounded by misinformation and outdated beliefs about transmission (Centers for Disease Control and Prevention, 2022).These factors contribute to isolation, mental health challenges, and poor clinical outcomes, including suicidal ideation and diminished quality of life (Pantelic et al., 2020; Rasoolinajad et al., 2018; Rueda et al., 2016; Shrestha et al., 2017).
Understanding these effects is especially important in Malaysia, where HIV remains a public health concern despite medical advances. The number of PLHIV increased from 51,000 in 2000 to 85,283 in 2023 (Joint United Nations Program on HIV/AIDS [UNAIDS], 2024b). Although previously concentrated among people who inject drugs (PWID), transmission now occurs primarily through sexual contact. Mother-to-child and occupational transmission are comparatively rare (Ministry of Health Malaysia, 2024). Malaysia’s 2021 HIV care cascade remains below the UNAIDS 95-95-95 global target at 83-66-82, indicating substantial gaps in testing, treatment, and viral suppression (Frescura et al., 2022; Ministry of Health Malaysia, 2022). Fear of stigma and late presentation for care contribute to these challenges (Ahmad et al., 2024).
Discriminatory attitudes persist globally: more than 25% of adults aged 15 to 49 in 52 of 58 countries expressed discriminatory views, and more than half did so in 36 countries (Joint United Nations Program on HIV/AIDS, 2022a). Although Malaysia lacked national data until recently, regional countries reported varying rates, Thailand (26.1%) and Pakistan (49%) suggesting cultural, religious, or policy-based influences (Joint United Nations Program on HIV/AIDS, 2024). Small-scale Malaysian studies have shown high stigma levels using tools like the DHS questionnaire but are not representative of the population (Lugova et al., 2015; Ministry of Health Malaysia, 2022). Other research among PLHIV receiving treatment also shows a high prevalence of perceived stigma (Ahmad et al., 2024).
Prior studies have linked stigma with sociodemographic characteristics such as education, income, marital status, and residence (Amo-Adjei & Darteh, 2013; Dahlui et al., 2015; Muluneh et al., 2022). In Malaysia, over three-quarters of new HIV cases in 2021 were among individuals aged 20 to 39 (Ministry of Health Malaysia, 2022), underscoring the need to focus on the economically productive age group. Therefore, this study aimed to assess the prevalence of HIV-related stigma and identify sociodemographic factors associated with discriminatory attitudes among Malaysians aged 15 to 49 years, using nationally representative data and a validated stigma questionnaire aligned with the UNAIDS global indicator.
Methodology
Study Design and Sampling
The Institute for Public Health, conducted a nationwide cross-sectional survey as part of an annual initiative to estimate the prevalence of common diseases in the Malaysian population. In 2020, the survey focused on communicable diseases, including HIV stigma. Respondents were selected through a multi-stage sampling approach, utilizing a geographical enumeration block sampling frame provided by the Department of Statistics Malaysia (DOSM). The sample size was determined using a single-proportion formula, with additional adjustments to account for survey design effects and complex sampling methods. Additionally, a two-proportion sample size was calculated based on previous study estimates, where the prevalence of HIV-related discrimination was 46.8% in urban areas and 38.3% in rural areas. Based on this difference, the required sample size was 528 participants per group, resulting in a total of 1,056 participants (Al Busthomy Rofi’i et al., 2023). While G*Power was not used initially, a post-hoc power analysis using G*Power indicated that the sample size of 2,818 respondents would be sufficient to detect a small-to-moderate effect size (OR = 1.4) with 80% power at a 5% significance level for logistic regression. For sampling purposes, Peninsular Malaysia was divided into four zones: Central, Southern, Northern and Eastern, while Sabah and the Federal Territory of Labuan were grouped into one zone and Sarawak was treated as another zone. The sampling process involved the random selection of 113 enumeration blocks as primary sampling units and 2,260 living quarters (LQs) as secondary units. Every household within these selected LQs was invited to participate in the study.
Data Collection
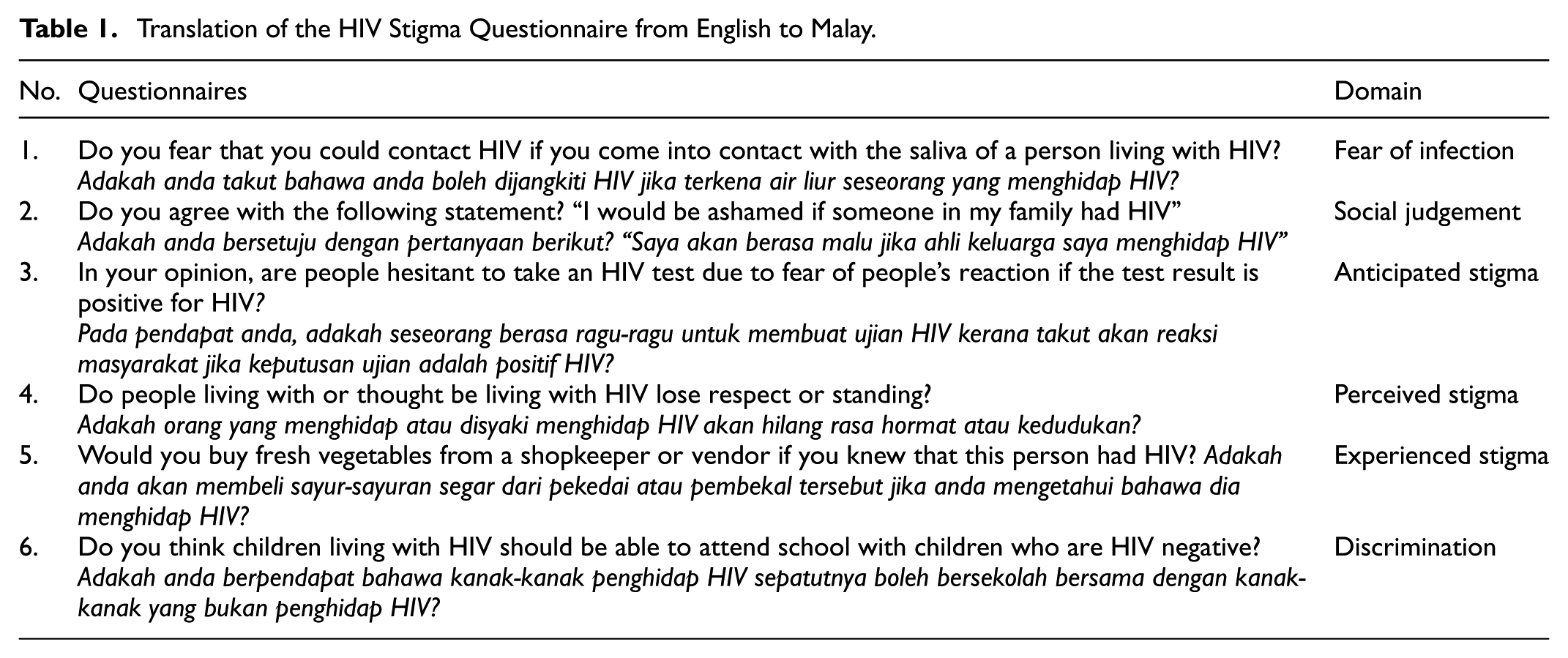
Data were collected nationwide between August and October 2020 across all 13 states and three Federal Territories in Malaysia. It was conducted through a combination of face-to-face interviews using a structured questionnaire and a self-administered questionnaire for sensitive topics, including HIV stigma. A validated Malay version of the HIV stigma questionnaire was used in this study, and the questionnaire demonstrated good internal consistency of Cronbach’s alpha .76 (Kassim et al., 2020). The original English version was developed by The Global Stigma and Discrimination Indicator Working Group (GSDIWG) and the STRIVE research consortium (Stangl et al., 2012). This questionnaire has been widely used to monitor HIV-related stigma at the global level. The questionnaire comprised six domains: fear of infection, social judgment, anticipated stigma, perceived stigma, experienced stigma, and discrimination, as outlined in Table 1. The final two domains were used to assess the Joint United Nations Program on HIV/AIDS (UNAIDS) global indicator for discriminatory attitudes. Responses to items 1 to 4 were considered indicative of stigma if answered “Yes,” while items 5 and 6 were considered stigmatizing if answered “No.” The analysis targeted individuals between 15 and 49 years old, a group recognized for being both sexually active and economically engaged. The validated Malay-language questionnaire, along with previously reported HIV stigma data for participants aged 13 and above, has been documented elsewhere (Institute for Public Health [IPH], 2021; Kassim et al., 2020).
Translation of the HIV Stigma Questionnaire from English to Malay.
Data Analysis
IBM SPSS Statistics version 29.0 was used to analyze the data. A total of 2,818 respondents aged 15 to 49 years were extracted for further analysis. Sociodemographic variables included age group, gender, marital status, residential strata (urban/rural), geographical zone, education level, and occupation. In Peninsular Malaysia, the residential zones were categorized as follows: the Central Zone (Kuala Lumpur, Putrajaya, and Selangor), the South Zone (Johor, Negeri Sembilan, and Melaka), the North Zone (Penang, Perak, Kedah, and Perlis), and the East Zone (Kelantan, Pahang, and Terengganu). A descriptive analysis was performed to summarize sociodemographic characteristics. The prevalence of HIV stigma domains was estimated while accounting for survey design effects. The prevalence of discriminatory attitudes toward PLHIV was compared across sociodemographic groups. Multivariable logistic regression analysis was conducted, with discriminatory attitudes toward PLHIV as the dependent variable, and sociodemographic characteristics as the independent variables. Findings were presented as adjusted odds ratios (aOR) with corresponding 95% confidence intervals (CI), and statistical significance was determined at a p-value of less than .05.
Ethical Approval and Consent to Participate
This study was registered under the National Medical Research Registration (NMRR-19-867-47973). Ethical approval was obtained from the Medical Research and Ethics Committee, Ministry of Health, Malaysia. All participants provided informed consent before taking part in the study. For those younger than 18, consent was additionally obtained from a parent or legal guardian. To minimize potential harm, particularly due to the sensitive nature of HIV-related questions, the study adopted a self-administered questionnaire approach for the HIV stigma module, which ensured participant anonymity and reduced social desirability bias. The survey design also excluded direct identifiers, and participation was entirely voluntary. The potential benefits of this research include generating nationally representative data on HIV stigma, which is essential for informing targeted public health interventions. These benefits outweigh the minimal risks involved, as the data collection method was non-invasive and privacy was rigorously protected.
Results
The 2020 national survey achieved an overall response rate of 77.9%, accounting for response rates at the household level (89.2%) and individual level (87.4%). Of the 5,957 total respondents, 2,818 individuals aged 15 to 49 years were included in the final analysis. Their sociodemographic characteristics are summarized in Table 2. The majority were aged 25 to 49 years (68.4%), with a near-equal distribution of males (47.4%) and females (52.6%). More than half of the respondents resided in urban areas (55.9%). Ethnic distribution showed that Malays constituted the largest group (60.4%), followed by Bumiputera Sabah and Sarawak (18.3%), Chinese (7.3%), and Indians (4.7%). There were fewer participants from East Peninsular Malaysia, Sarawak and Sabah and Labuan zone than the South, Central, and North Peninsular Malaysia. Over half had secondary-level education (51.5%), while 31.2% had tertiary education. The largest employment category was the private sector (34.3%), followed by those unemployed (23.7%) and self-employed individuals (14.9%).
Sociodemographic Characteristics of the Respondents, N = 2,818.

Table 3 presents the prevalence of HIV stigma across different domains. The highest prevalence was observed for experienced stigma (70.3%; 95% CI [66.8, 73.5]), followed by fear of HIV infection (64.4%; 95% CI [60.0, 68.6]), and discrimination (60.6%; 95% CI [57.6, 63.6]). The UNAIDS global indicator for discriminatory attitudes was 78.7% (95% CI [75.6, 81.5]), indicating a high level of discriminatory attitudes towards PLHIV.
Prevalence of Each Domain of the HIV Stigma Among Respondents Aged 15 to 49 Years in Malaysia.

Table 4 illustrates the prevalence of discriminatory attitudes by sociodemographic variables. A significantly higher proportion of discriminatory attitudes was observed among respondents from rural areas (86.2%; 95% CI [83.8, 88.2]) compared to urban residents (76.6%; 95% CI [72.7, 80.1], p < .001). Similarly, respondents with primary or lower education had the highest prevalence (88.3%; 95% CI [81.4, 92.9]) compared to those with secondary (84.6%; 95% CI [81.6, 87.3]) and tertiary education (67.7%; 95% CI [62.4, 72.6], p < .001).
Prevalence of UNAIDS Global Indicator for Discriminatory Attitudes Towards PLHIV Among Respondents Aged 15 to 49 Years Across the Sociodemographic Characteristic Variables.
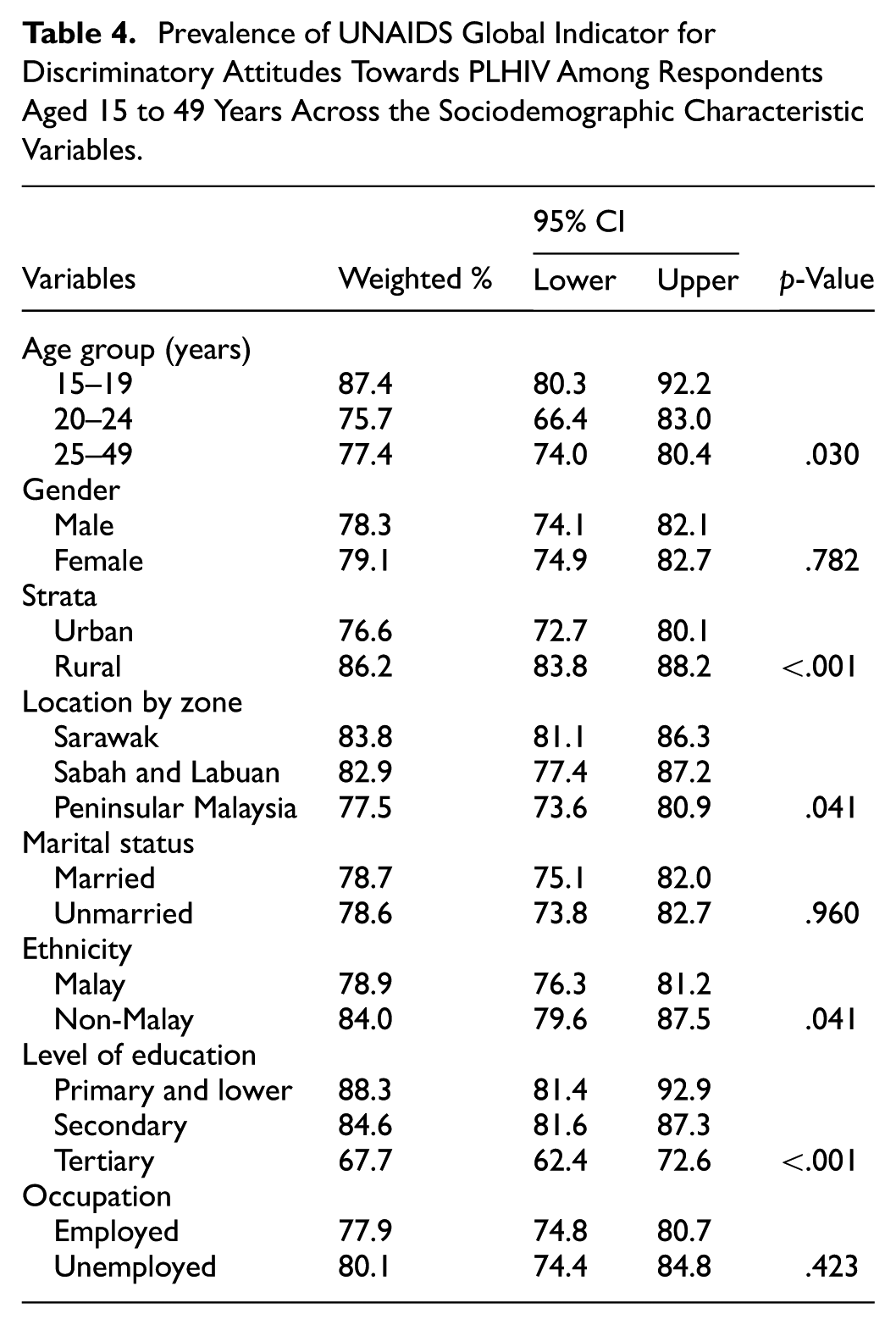
Table 5 presents the adjusted odds ratios (AOR) for factors associated with discriminatory attitudes towards PLHIV. Education level was the strongest predictor of discriminatory attitudes. Respondents with secondary or lower education had 2.42 times higher odds of exhibiting discriminatory attitudes compared to those with tertiary education (AOR = 2.42; 95% CI [1.85, 3.15]). Strata also played a significant role, with respondents from rural areas having 1.57 times higher odds of expressing discriminatory attitudes compared to their urban counterparts (AOR = 1.57; 95% CI [1.20, 2.04]; p = .001). Other variables, including age, gender, marital status, employment status, and geographic location, were not significantly associated with discriminatory attitudes. Although respondents aged 15 to 19 years had higher odds compared to those aged 20 to 24 (AOR = 1.58; 95% CI [.72, 3.49]), the association was not statistically significant (p = .252). Similarly, individuals residing in Sarawak (AOR = 1.24; 95% CI [.97, 1.60]; p = .084) and Sabah and Labuan (AOR = 1.10; 95% CI [.76, 1.58]; p = .620) did not have significantly different discriminatory attitudes compared to those in Peninsular Malaysia.
Multivariable Logistic Regression for the Factors Associated with UNAIDS Global Indicator for Discriminatory Attitudes Towards PLHIV Among Respondents Aged 15 to 49 Years in Malaysia.

Note. Complex sample classification table percentage: 78.7%. Bold values denote significant associations.
Furthermore, employment status did not show a significant association, with unemployed individuals having slightly lower odds than employed individuals (AOR = .86; 95% CI [.61, 1.21]; p = .386). Gender and marital status also did not influence discriminatory attitudes, as males (AOR = .91; 95% CI [.65, 1.27]; p = .569) and married individuals (AOR = 1.15; 95% CI [.79, 1.67]; p = .455) showed no significant difference compared to their respective reference groups. Overall, the findings highlight the significant role of education and rural residency in influencing discriminatory attitudes towards PLHIV in Malaysia. Addressing stigma-related attitudes through educational interventions and targeted rural outreach programs may be critical in reducing discrimination against PLHIV.
Discussion
This research explored HIV-related stigma within Malaysia’s most economically active demographic, including women of reproductive age and working-age individuals of both genders. This age group is also monitored by UNAIDS as part of its global indicator for discriminatory attitudes towards PLHIV. Notably, this is the first nationwide survey in Malaysia to estimate the prevalence of HIV stigma and discriminatory attitudes among the general population using the standard UNAIDS questionnaire. The prevalence of discriminatory attitudes among Malaysians aged 15 to 49 years was among the highest in the Asia-Pacific region, with comparative figures reported in Indonesia (68.7% in 2017), the Philippines (71.0% among women in 2017), and Samoa (90.5% in 2020; Joint United Nations Program on HIV/AIDS, 2022b). By contrast, Thailand had the lowest prevalence of discriminatory attitudes in the region, reported at 26.1% in 2015 (Joint United Nations Program on HIV/AIDS, 2024). These stark differences may reflect variations in cultural norms, religious conservatism, and national policies related to HIV, transgender rights, and sex work. Theoretical models such as Link and Phelan’s stigma framework suggest that structural conditions including legal systems and institutional practices reinforce stigma when they legitimize exclusionary attitudes. Thailand’s comprehensive public health education and community-based campaigns likely help dismantle these structural components, while Malaysia’s more limited initiatives may inadvertently maintain them (Barmania & Aljunid, 2016; Chautrakarn et al., 2023; Stangl et al., 2019).
This study also assessed the prevalence of each domain in the HIV Stigma Questionnaire among people aged 15 to 49 years, revealing a range from 44.2% to 70.3%, with experienced stigma being the most prevalent. These findings were consistent with the survey results for the general population aged 13 years and above (Institute for Public Health [IPH], 2021) suggesting that focusing on individuals aged 15 to 49 years adequately represents the broader Malaysian population. Similarly, a survey in Thailand reported a stigma prevalence range of 23.7% to 76.9%, with the highest levels observed in the anticipated stigma domain (Srithanaviboonchai et al., 2017). Malaysia’s relatively high levels of stigma may stem not only from cultural conservatism but also from the limited reach of formal HIV education efforts. Although HIV education is incorporated into Malaysian school curricula and targeted outreach programs exist, these are often inconsistently implemented or confined to key populations. In contrast, Thailand has institutionalized HIV education through mass media, peer-led community interventions, and inclusive school programs. Malaysia could strengthen its response by adopting broader, culturally responsive, and community-embedded strategies that promote accurate HIV knowledge and reduce fear-based stigma (Disease Control Division, 2015; Siraprapasiri et al., 2020).
Consistent with previous studies, this research found that lower educational attainment and rural residence were significantly associated with discriminatory attitudes. Prior work in Malaysia and other settings including Ethiopia, Tajikistan, and Indonesia, has shown that stigma often concentrates in communities with limited access to health literacy and public health resources (Al Busthomy Rofi’i et al., 2023; Muluneh et al., 2022; Zainiddinov, 2019). Thailand’s differing predictors, such as gender and religion (Chautrakarn et al., 2023), point to how local sociopolitical and religious dynamics also shape stigma. These cross-country differences highlight the need for interventions that are contextually grounded.
The high prevalence of stigmatizing and discriminatory attitudes among Malaysians is supported by the low level of HIV knowledge in the general population, with only 22.6% demonstrating adequate knowledge (Institute for Public Health [IPH], 2021). Several local studies have reported similar findings, highlighting limited HIV awareness among youth, adolescents, and university students (Azri Adam Adnan et al., 2024; Choy et al., 2013; Rajikan et al., 2017; Saad et al., 2015). These findings underscore the urgent need for comprehensive HIV and sexual reproductive health education, particularly targeting younger generations. Education can be disseminated through both formal channels, such as school curricula, and informal platforms, including social media, to reach school-aged children and the economically active population aged 15 to 49 years.
Importantly, HIV stigma is not just a public perception issue, it affects health outcomes. PLHIV who experience stigma are more likely to delay testing and treatment and may engage in continued high-risk behavior. Some acquire HIV through non-preventable means, such as perinatal transmission or occupational exposure (Akpuh et al., 2020; Ewing et al., 2019), further highlighting the injustice of stigmatization. Fear of HIV status disclosure remains a significant driver of stigma (Chan et al., 2020). Furthermore, healthcare workers (HCWs) should receive proper training to minimize HIV-related stigma within healthcare settings. Studies suggest that personal interactions with PLHIV can lead to reduced stigma and lower social distancing attitudes towards PLHIV (Chan & Tsai, 2017).
Recommendations
Based on the findings’, targeted interventions are urgently needed to address HIV-related stigma and discriminatory attitudes, particularly among individuals with lower educational attainment and those residing in rural areas. Integrating HIV stigma reduction strategies within existing healthcare and community outreach programs could enhance testing uptake, early diagnosis, and sustained treatment adherence are the key pillars of effective HIV/AIDS management. Community-based education campaigns tailored to rural populations and culturally sensitive modules delivered through schools and public platforms may improve HIV knowledge and shift social norms over time. These interventions should be embedded within broader public health efforts and healthcare systems to promote continuity of care, reduce barriers to access, and support the overall goal of eliminating AIDS-related health disparities. Given the consistency of stigma-related predictors across diverse contexts, the approach demonstrated in this study may offer relevant insights for similar low- and middle-income countries pursuing the 95-95-95 targets globally.
Strengths and Limitations
This study is the first nationwide survey in Malaysia to estimate the prevalence of HIV stigma and discriminatory attitudes towards PLHIV using a standardized UNAIDS questionnaire. The survey design and nationally representative sampling ensured that the findings provide robust and generalizable estimates for the Malaysian population. Additionally, the large sample size allowed for detailed subgroup analyses across sociodemographic factors, enhancing the reliability of the findings. However, this study has several limitations. As a cross-sectional survey, it cannot establish causal relationships between discriminatory attitudes and their predictors. Since responses were self-reported, there is a possibility of social desirability bias, whereby participants may downplay stigmatizing views to align with societal expectations. Furthermore, while the survey captured multiple domains of HIV stigma, it did not assess other potential contributing factors, such as personal experiences with PLHIV, cultural influences, or exposure to HIV education programs. Nevertheless, this study offers important perspectives on the nature of HIV stigma in Malaysia, highlighting key areas for intervention and the urgent need for public education campaigns to reduce discriminatory attitudes toward PLHIV.
Conclusion
Stigma and discrimination towards PLHIV remain highly prevalent among individuals aged 15 to 49 years in Malaysia. Given that lower education levels and rural residence were identified as significant predictors of discriminatory attitudes, targeted interventions should focus on enhancing HIV-related knowledge and awareness, particularly in underserved communities. Comprehensive public health initiatives, including HIV education programs, community engagement, and anti-stigma campaigns, must be implemented to challenge misconceptions and foster a more supportive environment for PLHIV. Additionally, healthcare workers should receive training to minimize stigma in medical settings, ensuring equitable and nonjudgmental healthcare access for PLHIV. Addressing stigma and discrimination requires a coordinated, multi-sectoral strategy that engages government bodies, NGOs, healthcare professionals, educators, and community stakeholders. While Malaysia has integrated HIV education into school curricula and outreach to key populations, broader efforts such as mass media campaigns and stigma-reduction initiatives are still limited. Strengthening community-level engagement, inclusive sexual health education, and culturally sensitive communication strategies will be essential to reduce stigma and improve support for PLHIV. Prompt implementation of such efforts is crucial to fulfill global pledges and advance progress toward the UNAIDS 95-95-95 targets, with the ultimate aim of ending the AIDS epidemic by 2030.
Footnotes
Acknowledgements
The authors wish to express their sincere gratitude to the dedicated data collectors and research team members involved in NHMS 2020. Appreciation is also extended to the Director General of Health Malaysia for granting permission to publish this article. The research team sincerely thanks the National Institutes of Health, Malaysia, for their valuable support in the successful implementation of the survey.
Ethical Considerations
This study was registered under the National Medical Research Registration (NMRR-19-867-47973), and ethical approval was obtained from the Medical Research and Ethics Committee, Ministry of Health, Malaysia.
Consent to Participate
Informed consent was obtained from all respondents before participation, and for participants under 18 years of age, parental or guardian consent was also secured. To minimize potential harm, particularly due to the sensitive nature of HIV-related questions, the study adopted a self-administered questionnaire approach for the HIV stigma module, which ensured participant anonymity and reduced social desirability bias. The survey design also excluded direct identifiers, and participation was entirely voluntary. The potential benefits of this research include generating nationally representative data on HIV stigma, which is essential for informing targeted public health interventions. These benefits outweigh the minimal risks involved, as the data collection method was non-invasive and privacy was rigorously protected.
Author Contributions
WSAWJ, SMA, NH, and MSAK contributed to conceptualization, methodology, data analysis and original drafting. MHAM and NS involved in project administration and data collection supervision. All authors reviewed and approved the final version of the manuscript for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is sponsored by the Ministry of Health, Malaysia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset for this study is available upon request to the corresponding author. The principal author kept the dataset according to the National Institutes of Health Malaysia research data repository guidelines.