
Abstract
The use of complementary and alternative medicine (CAM) in Europe has intensely increased in recent decades. To acquire information about the patterns and trends of CAM use in Slovakia, a nationwide representative survey was conducted on Slovakian adult population. A nationally representative cross-sectional survey was administered to the general population of Slovakian residents aged 18 years and over. The respondents were interviewed face-to-face by professional interviewers. Data were collected during September 2019 as a part of an omnibus survey on a variety of subjects. Altogether, 82.4% of the respondents reported either regular CAM method use or the lifetime prevalence of such use. The most frequently reported group of methods were biologically based treatments (78.9%), followed by manipulative and body-based methods (54.4%), mind-body interventions (31.9%), whole medical systems (18.2%), and energy therapies (4.2%). Vitamins (71.1%), herbal teas (68.1%), massages (53.6%), religious healing (20.3%), and special diets (18.8%) were the five most commonly preferred CAM modalities. Female gender, higher income and higher education are significant predictors of CAM use. The study highlights the association between satisfaction with healthcare systems, health situations, and the use of CAM.
Introduction
One of the most often-cited definitions of complementary and alternative medicine (CAM) was developed by the National Centre for Complementary and Integrative Health (NCCIH, formerly the National Centre for Complementary and Alternative Medicine NCCAM): “CAM is a group of diverse medical and health care systems, practices and products that are not presently considered to be part of conventional medicine” (Koithan, 2009). Several studies have confirmed that the use of CAM in Europe has intensely increased over recent decades (Eardley et al., 2012; Frass et al., 2012; Kemppainen et al., 2018). However, the existence of severe possible risks connected to the use of CAM raises important questions that need to be considered appropriately (Werneke et al., 2004). Moreover, the impact of CAM on the healthcare system and public health policy is essential to consider. To optimize the safety of patients and stimulate development of appropriate healthcare policies, it is crucial to obtain knowledge about current trends and patterns of CAM use by the general population.
Attitudes toward CAM in European countries have undergone various stages of development. Under socialism in Central and Eastern Europe, almost every kind of unconventional healthcare option was considered, to a great extent, as backward and superstitious practice (Křížová, 2015; Souček, 2020; Stepan, 1985; Stöckelová & Klepal, 2018). Since the change of political regime and the structural transformation of social, political, and religious sectors, various complementary and alternative therapies have become widespread. Data on CAM use in this part of Europe (Bosak & Słowik, 2019; Hegyi, 2018; Pokladnikova & Selke-Krulichova, 2016, 2018), have revealed that the prevalence of CAM use in these countries is significant and may considerably differ. For instance, in the Czech Republic, 76% of a survey’s respondents reported the use of one or more CAM modalities during the past 30 days (Pokladnikova & Selke-Krulichova, 2016), while in Poland, one in four respondents reported that they or a close family member had used CAM (Olchowska-Kotala & Barański, 2016). A survey conducted in Hungary showed that 15% to 20% of the population had experience with CAM (Buda et al., 2002). In Slovakia, only limited data are available regarding the prevalence of CAM usage, and only a few research studies have been conducted on the use of practices outside the dominant medical paradigm (Souček & Hofreiter, 2017). A survey on CAM was conducted within the health and healthcare topic module of the International Social Survey Programme (ISSP) in 2012, which consisted of a cross-national research programme conducting annual surveys on diverse topics relevant to social sciences. The subject of CAM was examined in two questions. The first question demonstrated that in Slovakia, 12.7% of respondents either fully or partially agreed that alternative medicine provides better solutions for health problems than does conventional medicine. The second question showed that 13% of respondents either visited or were visited by an alternative healthcare practitioner during the past 12 months (Souček & Hofreiter, 2017). As is the case in other European countries, the use of CAM in Slovakia is not covered by national insurance schemes. The existing inclination to cover the costs “out of one’s pocket” indicates that several CAM methods are gaining more significant attention among the general population. However, a survey on the general population in Slovakia has not yet been carried out. A comprehensive review of the use of CAM in the general adult population is needed in order to stimulate discussion about safety and public regulations. Moreover, an investigation into the subject is important because it is in line with the World Health Organization Traditional Medicine Strategy that encourages member states to promote the safe and effective use of provided-healthcare through research of CAM practices Accordingly, the aim of this study is to investigate the most frequently used CAM methods in Slovakia, the socio-demographic and socio-economic characteristics of CAM users, as well as the reasons that CAM is used. Moreover, with respect to public health issues, the study describes relations between satisfaction with healthcare systems, health situations, and the use of CAM.
Method
Study Design and Sample Selection
As an appropriate method for obtaining information on patterns and trends of CAM use in Slovakia, a survey was conducted on a sample of 1,027 citizens of the Slovak Republic. The sample size was representative of the Slovakian adult population aged 18 years and over (4.5 million citizens) with a 95% confidence level and a 3% confidence interval on the basis of quota sampling for the main socio-demographic characteristics: gender, age, nationality, education, place of residence, and region of residence (Table 1). Only respondents under 18 years of age were excluded from the study sample. Use of nationally representative sample is a standardized methodology and frequently used method to gather large amounts of data on prevalence and predictors of CAM use (Ernst & White, 2000; Harnett et al., 2019; Linde et al., 2014). The data collection was carried out during September 2019 as a part of an omnibus survey by FOCUS research agency. FOCUS is one of the leading research companies in Slovakia, specializing in the provision of complete analytical services and professional advisory consulting in the areas of marketing research and public opinion polls (FOCUS). The respondents were randomly selected and interviewed face-to-face by professional interviewers. In addition to the sociodemographic attributes relating to the quota sampling, the survey included additional information associated with marital status, household monthly income, religious identity, number of household members, work status, and political view. Table 1 summarizes the sociodemographic characteristics of all respondents.
Sociodemographic Characteristics of the Sample.
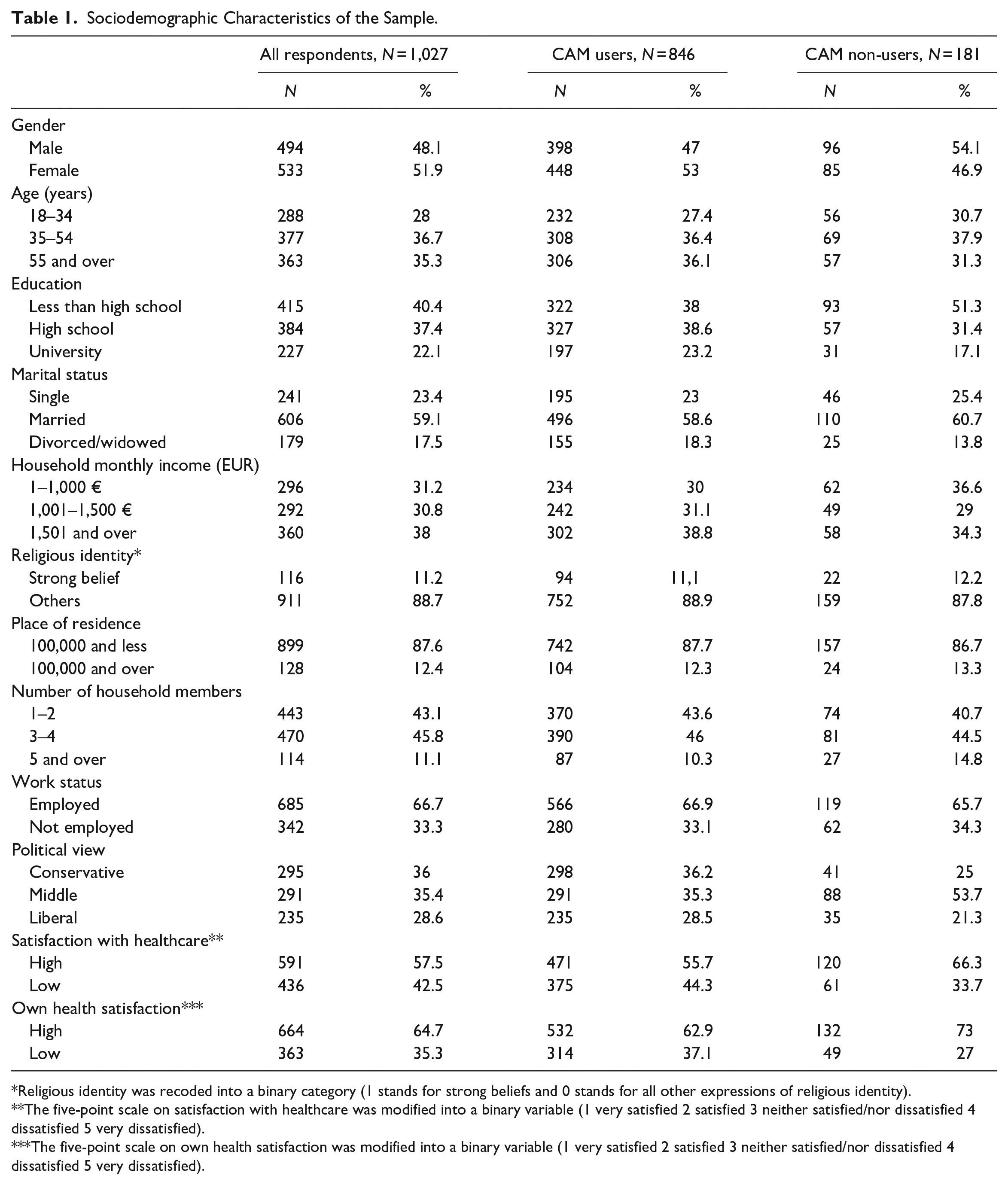
Religious identity was recoded into a binary category (1 stands for strong beliefs and 0 stands for all other expressions of religious identity).
The five-point scale on satisfaction with healthcare was modified into a binary variable (1 very satisfied 2 satisfied 3 neither satisfied/nor dissatisfied 4 dissatisfied 5 very dissatisfied).
The five-point scale on own health satisfaction was modified into a binary variable (1 very satisfied 2 satisfied 3 neither satisfied/nor dissatisfied 4 dissatisfied 5 very dissatisfied).
Pretest
The overall design of the questionnaire was partly inspired by the International Questionnaire to Measure use of Complementary and Alternative Medicine (I-CAM-Q) (Quandt et al., 2009; Re et al., 2012; Wemrell et al., 2017), and similar research has been conducted on the prevalence of CAM use in the Czech Republic (Pokladnikova & Selke-Krulichova, 2016, 2018). The I-CAM-Q was developed by an expert group as a suitable method to investigate CAM prevalence and to provide knowledge appropriate for health planning and suitable to meet patients’ needs. Originally, it consisted of four main questions about visiting healthcare providers, complementary treatments received from physicians, use of herbal medicine and dietary supplements, self-help practices (Quandt et al., 2009). The original version of the I-CAM-Q was modified and various variables were comprehensively combined. Accordingly, respondents were asked whether they had received any CAM healthcare options, without categorizing the options into analytical subgroups of self-help practices and practitioner-based treatments. To increase face validity, content validity, and compliance with instructions, the questionnaire was pretested on 102 subjects through an online survey. Considering that the survey asked about health-related issues, an online method, which provides a higher sense of privacy and confidentiality, was used. The purpose of the pretest was to gather information mainly from CAM users. The sample in the pretest included both genders of different ages. For this purpose, the SurveyMonkey platform was used, and the survey was carried out during June and July 2019. In the pretest, the survey respondents suggested that some categories were not clearly specified and that they did not understand the meaning of some of the terminology used. Relatedly, suitable names of healthcare practices, according to country specifics, were developed. The aim of the pretest was to identify the most commonly referred to treatment practices that are not presently considered to be part of conventional medicine. Following this identification, the results of the pretest analysis were used to develop the cross-sectional nationwide survey on CAM use among adults in Slovakia.
Questionnaire Development
The list associated with CAM, which reflected country-specific CAM usage, included 18 different modalities from which the respondents were able to choose the preferred option. The survey included an extensive list of the following therapies: acupuncture, homeopathy, Chinese medicine, Ayurveda, chiropraxis, massage, reflexology, meditation, yoga, visual imagery, psychotherapy, herbal teas, vitamins, minerals, and dietary supplements, special diets and detoxification, Bach flower remedies, energy healing, religious healing, and spiritual ceremonies. In addition, open-ended questions were introduced at the end of the section to enable CAM methods that did not appear in the list to be inserted. No qualitative data were obtained through open-ended question. The study relied on the widely accepted CAM classification by the NCCIH, which groups CAM into the following five categories: mind-body interventions, biologically based treatments, manipulative and body-based methods, energy therapies, and whole medical systems (Tataryn, 2002). The pretest revealed that rather than asking respondents about a particular recall period, a more appropriate method for investigating respondents’ experience with particular CAM methods would be to investigate the frequency of their CAM use. Considering that health issues may occur irregularly during a lifetime, for each reported method, the respondents were asked to indicate how often they used the selected method on the following scale: regularly, at least once a year, several times in life, at least once in a lifetime and never. Such an approach allows the identification of not just regular but also casual CAM users.
The question of why people are using different CAM modalities in countries of Central and Eastern Europe remains inadequately answered. The respondents were thus asked to identify the level of importance for reasons for CAM use based on the occasion of their most-recent use of the selected options. On a 4-point scale (strongly important—strongly unimportant), the importance of the following reasons was reported: fewer side effects, financial availability, complementary use with conventional medicine, connection to one’s own worldview and belief, unknown medical condition, greater efficiency in comparison to conventional medicine, absence of trust in conventional medicine and prior positive experience. Particular variables in this question were derived from pretest investigations and from similar research activities conducted on the reason for seeking CAM (Hyland et al., 2003; Köse et al., 2018; McFadden et al., 2010; Vincent & Furnham, 1996). Perception of health quality and provided healthcare are important indicators that can measure the predictors of CAM use (Astin, 1998). Therefore, the respondents’ satisfaction with the healthcare system and their personal health were investigated on a five-point Likert scale with two following questions: (1) How satisfied you are with the healthcare system in Slovakia? (very satisfied—very dissatisfied), and (2) How satisfied you are with your health? (very satisfied—very dissatisfied). Moreover, the survey asked the respondents to clarify their source of information about CAM.
Statistical Methods
The dependent variables in the analysis were the overall prevalence of CAM use, as well as the prevalence of selected CAM methods in four categories: mind-body interventions, whole medical systems, biologically based treatments, and manipulative and body-based methods (Table 3). Due to the low reported sample, energy therapies were not included in the statistical analysis. As mentioned above, we decided to the gather data on frequency of CAM use. Respondents’ answers to this question were dichotomized, enabling us to divide the respondents into two categories. Respondents who reported the use of CAM therapies either regularly, at least once a year, or several times in their life were grouped into the category of CAM users and coded as 1. For the purpose of the study respondents showing tendency for regular or semiregular intervals in use of CAM are defined as CAM users. It is expected that these respondents have the nature of habit by use of CAM. On the other hand, casual users who reported their use of CAM to be at least once in a lifetime or never were associated with non-users and assigned as 0. These respondents obviously do not follow the usual pattern in CAM use. Due to dichotomization of main dependent variables and to test hypotheses a logistic regression analysis was conducted. The significance level was 95% (p value <.05). For data analysis, SPSS for Windows version 25 was used. The independent variables were selected according to the socio-behavioral model (SBM). This model predicts that women, younger persons, people with higher education, as well as people with higher incomes, are more likely to be CAM users (Bishop et al., 2007). To test whether these findings are valid for CAM users in Slovakia, the aforementioned socio-demographic characteristics of respondents were incorporated into the logistic regression models. Age category (18–34 coded as 0, 35–54 coded as 1, 55 and over coded as 2), gender (male 0, female 1), education (lower than high school coded as 0, high school coded as 1, university education coded as 2), household monthly income (the reference category is monthly household income lower that 1,000 euros, income 1,001 -1,500 euros coded as 1, income higher than 1,500 coded as 2). Moreover, it was also expected that dissatisfaction with the healthcare system would be another factor in favor of CAM use. Generally, the principal complaints due to which individuals seek CAM treatments are impersonal and uncompassionate treatment within the conventional healthcare system (Astin, 1998; Bishop et al., 2007). The legacy of the authoritarian position of doctors inherited from the time of communist government rule combined with weak patients’ rights movements has preserved the unfriendliness of the Slovakian healthcare system. According to a previous investigation, only 50% of Slovakian respondents are satisfied with the overall quality of the healthcare system (compared to the EU-28 satisfaction average of 71%) (Smatana et al., 2016). Therefore, we formulated the hypothesis that low satisfaction with the national healthcare system is a significant predictor of an individual’s CAM use. In addition to dissatisfaction with the healthcare system, studies have suggested that CAM use emerges when individuals have experienced a chronic illness or when they have perceived low satisfaction with the health situation (Eardley et al., 2012). Based on these findings, we formulated the expectation that low satisfaction with one’s personal health situation explains CAM use. In both cases—satisfaction with healthcare and satisfaction with one’s own health—a five-point Likert scale was modified into a binary variable and respondents’ answers dissatisfied or very dissatisfied were coded as 1. The remaining answers (very satisfied, satisfied, neither satisfied nor dissatisfied) were defined as the reference category and coded as 0. Finally, previous studies have also linked increased religiosity and spirituality with higher CAM use in the general population (Hsiao et al., 2008). It was therefore presupposed that high religiosity could be an important predictor of CAM use in Slovakia. There are several ways of how to measure degree of religiousness using quantitative and qualitative methods (Billiet, 2002). This study relies on general question on the basis of self-identification of intensity of religious identity. A five-point Likert scale investigating religious identity (strength of beliefs) was recoded into a binary variable where 1 coded for strong beliefs, and all other expressions of religious identity were assigned 0.
Results
Descriptive Data
Altogether, 846 (82.4%) out of the 1,027 survey participants reported the use of some method of CAM on a regular basis, that is, at least once a year or several times during their life. The sociodemographic characteristics of CAM users are summarized in Table 1. The most frequently reported group of methods were biologically based treatments (78.9%), followed by manipulative and body-based methods (54.4%), mind-body interventions (31.9%), whole medical systems (18.2%), and energy therapies (4.2%). The analysis showed that most of the CAM users took vitamins, minerals, and food supplements (71.1%). Next, the methods highlighted by CAM users were herbal teas (68.1%), massages (53.6%), religious healing (20.3%), special diets (18.8%), homeopathy (14.4%), yoga (10.6%), reflexology (6.2%), and meditation (6.1%). Other methods (acupuncture, aromatherapy, chiropraxis and osteopathy, Chinese medicine, psychotherapy, spiritual ceremonies, visualization, and Ayurveda) were used by approximately 6% or less of the respondents (Table 2).
CAM Users by Groups and Types of Therapy.

The respondents identified the level of importance for reasons for CAM use. Lessened side effects were the primary reason for the respondents’ last use of a CAM treatment method (85%), followed by complementary use with conventional medicine (84.4%) and prior positive experience (82.3%). The other reasons for CAM use were the connection to one’s own worldview and belief (63%), greater efficiency in comparison to conventional medicine (57.5%), and financial availability (55%). And 29.3% of the respondents employed CAM because they do not have trust in conventional medicine.
The respondents were asked to indicate their main source of information about CAM. The results identified that the most prominent source of information about CAM was one’s family, relatives and friends (77.7%), followed by a general practitioner or pharmacist (25.8%), social networks and websites (21.5%), relevant literature (19.8%), and advertisements or articles in the press, radio, or television (14.9%). Only 7% of the respondents chose practitioners of alternative medicine as their main source of information about CAM.
Main Results
In terms of socio-demographic explanatory factors on an individual level, the results of logistic regression presented in Table 3 indicated that women are more likely than men to have used mind-body interventions (OR 2.759, 95% CI [2.030–3.749]), whole medical systems (OR 1.595, 95% CI [1.123–2.266]), biologically-based treatments (OR 1.415, 95% CI [1.022–1.958]), and manipulative and body-based methods (OR 1.479, 95% CI [1.127–1.940]). In the case of age, no significant differences were noticed. In almost all CAM groups, higher education and higher household monthly income contribute to more frequent use of CAM among the respondents (Table 3; Education, Household monthly income). Strong religious identity (strength of belief) plays a role in the use of mind-body interventions (OR 3.213, 95% CI [2.008–5.142]). Table 3 also shows that respondents who report dissatisfaction with the healthcare system are more likely to use CAM in general (OR 1.581, 95% CI [1.097–2.278]) especially whole medical systems (OR 1.623, 95% CI [1.136–2.320]) and biologically based treatments (OR 1.417, 95% CI [1.012–1.984]). On the other hand, respondents who are dissatisfied with their own health prefer to use mind-body intervention (OR 1.464, 95% CI [1.036–2.069]) as well as manipulative and body-based methods (OR 1.734, 95% CI [1.259–2.387]) to solve their health problem.
Selected Predictors of CAM Users by Group of Methods.

Note. Values OR (Odd Ratio) and 95% CI were calculated by using multivariate logistic regression; p-values were calculated from Wald’s test. Significance level was 95% (p value <.05). Due to the low reported sample, energy therapies are not included in the logistic regression. Ref. = reference group; NS = not significant.
Discussion
Interpretation of Key Results
Using a representative research sample for the adult population, this study represents the first examination of the prevalence of CAM use in Slovakia. The results note that 846 (82.4%) out of the 1,027 respondents reported the use of one of the selected methods of CAM either at least once a year or several times in their life. The collected data show that the prevalence of CAM use in Slovakia is considerably high. Results from a recent study examining CAM use across 21 European countries based on data from the seventh round of the European Social Survey, indicates that overall CAM use is 17.9% (Fjær et al., 2020). The study focused on the prevalence of traditional complementary and alternative provider use in a nationally representative population from 32 countries. It showed a relatively low prevalence of CAM in a number of Eastern European countries, including Slovakia (Peltzer & Pengpid, 2018). This can be partly explained by different definitions of CAM usage, since this study focuses exclusively on visits to CAM healthcare practitioners and not on self-administrated CAM use and easily obtained products. In general, the use of CAM in European countries varies by a large extent (0.3%–86%) (Eardley et al., 2012; Frass et al., 2012; Kemppainen et al., 2018). This can be partly clarified by different regulations and health insurance policies. Another reason for this difference in use could be related to the variances in the selected methodologies of the surveys and the reported quality of the surveys conducted thus far. Even the absence of a consistent definition of CAM has a considerable impact on acquired results. Therefore, it is difficult to conclude whether the popularity of CAM in Slovakia is higher or lower in comparison to that in other countries. Due to the low reported data on CAM use in Central and Eastern European countries, comparisons are difficult to execute. However, altogether, the results of CAM users in Slovakia are very similar to the overall reported use of CAM in the Czech Republic (76%). Even the three most commonly preferred CAM modalities, namely, vitamins, herbal teas, and massages, are the same.
A systematic literature reviews (Eardley et al., 2012; Frass et al., 2012) suggest that the most frequently used CAM therapies in Europe are herbal teas, acupuncture, homeopathy, chiropraxis, and reflexology. Although some of the acquired results are consistent with these findings, this research highlights that unlike other European countries, acupuncture and chiropraxis are less frequently reported in Slovakia. Eastern Europe is more ethnically homogenous than many other Western regions, and several studies have shown that some CAM treatments are embedded in health patterns of various ethnic minorities (Zeid et al., 2019). These are defined as group of people who have different set of traditions, language, culture, or religion from that of the majority of individuals living in particular society. This might explain why interest in acupuncture in the general population in Slovakia is relatively low compared to other countries where it is extensively practised (Hopton et al., 2012). Despite chiropraxis is visible represented in all European countries, less frequently reported use of this treatment in Slovakia could be explained by absence of possibilities to solve different musculoskeletal problems by experts trained in chiropraxis. The increasing demand for herbal teas and related products has been confirmed in Western Europe (Hritcu & Cioanca, 2016; Wemrell et al., 2017) and other parts of the world (Merritt-Charles, 2011). However, unlike Western Europe, where we can see the re-emergence of alternative healthcare together with a strong medical counterculture since at least the mid-1960s, the situation in the Eastern European region has been quite different. The collapse of communist governments in this part of Europe has also affected the medical environment (Souček, 2020). Furthermore, this situation has led to the growing popularity and acceptance of herbal products that have had a long tradition in most Eastern European countries (Kozlowska et al., 2018; Penkala-Gawęcka, 1995; Pokladnikova & Selke-Krulichova, 2016). An explanation for the prevalence of herbal teas could be found, moreover, in the fact that herbal teas are largely affordable and accessible.
The strength of this study lies in a wide-ranging set of sociodemographic factors and associations with healthcare and one’s own health satisfaction. Studies on sociodemographic determinants of CAM that have been conducted in various European countries suggest that women and highly educated people are inclined to use CAM (Eardley et al., 2012; Frass et al., 2012; Kemppainen et al., 2018). A recent study confirmed that women and respondents with higher education were the main users of all categories of CAM in Europe (Fjær et al., 2020). According to the ISSP survey data, the prevalence of CAM practitioner usage in the past 12 months was 22.8% among men and 28.8% among women (Misawa et al., 2019). The present research on CAM usage in Slovakia proved that gender, income, and education are significant predictors of usage. As in many other European countries, the methods and medicaments of unconventional medicine in Slovakia are not directly covered by health insurance companies. Hence unconventional treatments might end up being much more expensive than a visit to a regular medical professional. This might explain the economic interpretation of a higher use of CAM and indicates that the less education, leading to low income, was identified as a high predictor. A high prevalence of strong religious beliefs was noticed in mind-body interventions. This is because the presented survey allowed the respondents to report healing prayers as one of the CAM treatment methods. Although it is noteworthy that religious prayers are listed among the three most frequently used therapies in Slovakia (20.3%), the prevalence of use is not extremely high. The use of healing prayers is most frequently observed in studies conducted in the United States of America (USA) and Asia (Harris et al., 2012), where the overall rank of religiosity is high. To avoid distortion in the analysis of the religious predictor in Slovakia, where religious self-identification is also high (75.97% of people reported themselves as believers in the 2011 census) (European Commission, 2019), the analysis of odds ratios was undertaken only with respondents who reported strong religious beliefs.
Recent analysis shows that dissatisfaction with health services and the presence of a longstanding health problem were positively related to all categories of CAM use (Fjær et al., 2020). The study proved the relationship between satisfaction with the healthcare system, one’s own health situation and the use of CAM in Slovakia. On the one hand, the analysis for the predictive factors of CAM use indicates that CAM users, except respondents reporting mind-body interventions and manipulative and body-based methods, have a negative perception of the quality of provided healthcare; on the other hand, low levels of satisfaction with their own health leads to higher use of mind-body interventions and manipulative and body-based methods. Some other studies have focused on mind-body and manipulative and body-based therapies in connection to the disorders for which they are used. These studies show links between chronically painful conditions (Wolsko et al., 2004), back pains (Chou et al., 2007), mental disorders (Burnett-Zeigler et al., 2016) and mind-body, manipulative and body-based treatment methods. These links might indicate that conventional medicine is less effective for solving chronic and psychological conditions and that people suffering from such afflictions are consequently less satisfied with their own health and are thus more likely to use CAM than are those in other situations.
Limitations
The limitations of this study are identified in the broader definition of CAM that includes vitamins, food supplements, or massages. For such methods, there is no consensus about whether to assign these methods to the category of conventional medicine. However, to cover the heterogeneous spectrum of CAM practices, several studies have included them in the research design. The next limitation of the study lies in the fact that religious prayer was included in the scope of the CAM investigation. Excluding prayer would definitely have had a significant impact on the analysis of the prevalence findings. When prayers were excluded, the prevalence rate in mind-body interventions decreased from 31.9% to 18.8%. Some studies even recommend the removal of prayer from the list of CAM practices. Notwithstanding this suggestion, the role of spirituality and religion in healing issues needs to be further discussed (Tippens et al., 2009). Also of relevance is the methodological decision to group together the respondents who reported both the regular and casual prevalence of use under the category of CAM users’ needs to be taken into consideration while interpreting the findings of this study. This means that the exclusion of the respondents who reported the use of CAM several times during their life would reduce not only the total number of CAM users but could also impact the logistic regression results for particular CAM modalities. One of the common problem in almost all survey studies is the bias caused by the type of people who are willing to participate. This should be taken into account while interpretation of acquired results. Finally, the fact that the survey was part of an omnibus survey could have affected the acquired results.
Conclusion
As there have been no statistics regarding the prevalence of CAM use in Slovakia thus far, all of the represented findings are valuable. Studies have proven that the use of CAM treatments in Slovakia is widespread and challenges conventional medicine. To bridge the gap between different sectors of healthcare, it is important to obtain knowledge on the prevalence and the types of CAM use and the reasons for using non-conventional methods. The acquired results partly fill the knowledge gap regarding the socio-demographic and socio-economic characteristics of CAM usage in this part of Europe. This knowledge gap has been the main reason why the subject has remained highly underestimated. Most importantly, the current study confirmed the prevalence of CAM use in Slovakia; likewise, in Western European countries, is considerably high. However, the current investigation has shown some specificities in Slovakia, especially taking into account the most preferred CAM modalities reported by the respondents. It was confirmed that female gender, higher income, and higher education are significant predictors of CAM use. Moreover, the relationship between satisfaction with the healthcare system, one’s own health situation and the use of CAM was proven. This knowledge could be a useful source of information to enable us to better meet patients’ needs and expectations. To improve the quality of healthcare provision, relevant official representatives should be thus informed about the findings of this study. To obtain further information, if the trends in the prevalence of CAM use in Slovakia are still present, follow-up research in this area is recommended, especially with focus on spirituality and religion on healing issues. Moreover, to gain a more comprehensive understanding of CAM in the context of the Slovakian healthcare system, it is important to conduct qualitative analysis and in-depth interviews with users of various CAM methods.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440211068480 – Supplemental material for Complementary and Alternative Medicine Use in Slovakia: Results of a National Population Survey
Supplemental material, sj-docx-1-sgo-10.1177_21582440211068480 for Complementary and Alternative Medicine Use in Slovakia: Results of a National Population Survey by Ivan Souček and Roman Hofreiter in SAGE Open
Footnotes
Acknowledgements
The authors are very grateful to all the respondents who completed the survey.
Author Contributions
The first author substantially contributed to the concept of the research and the interpretation of the obtained data. The second author participated in the submitted study by analyzing the obtained data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was prepared as part of the research project VEGA 1/0333/19: Analysis of Selected Social Contexts of Using Alternative Forms of Health Care in Slovakia and research project VEGA 1/0381/22: Cultural and value context of contemporary use of complementary and alternative medicine (CAM) in Slovakia.
Statement of Ethics
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee (Research Ethics Committee of Matej Bel University, reference 206) and with the 1964 WMA Declaration of Helsinki and its later amendments or comparable ethical standards.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.