
Abstract
To compare the relationships between symptoms of attention-deficit/hyperactivity disorder (ADHD), family functioning, and gaming problems reported by adolescents and parents. Adolescents with ADHD (N = 144) reported their gaming behaviors and perceived family functioning. Parents reported pre-treatment ADHD/oppositional defiant disorder (ODD) symptoms and gaming problems in their children. Multiple linear regression analyses were used to test the associations of ADHD/ODD symptoms, family functioning, and their interaction with gaming problems. The results based on parent and adolescent reports were compared. Subdomains of family functioning were also explored. Overall ADHD/ODD (B = 4.36 [95% CI 2.65, 6.06], p < .001) and all three domain symptoms (inattentive: B = 3.59 [95% CI 1.86, 5.32], p < .001; hyperactive: B = 2.73 [95% CI 0.94, 4.52], p = .003; ODD: B = 4.42 [95% CI 2.72, 6.12], p < .001) were positively associated with gaming problems reported by parents, but not adolescents. Family functioning was negatively associated with gaming problems regardless of informants (parent reports: B = −3.24 [95% CI −4.98, −1.50], p < .001; adolescent reports: B = −3.35 [95% CI −4.81, −1.89], p < .001) but modulated the relationship between overall ADHD/ODD and inattentive symptoms and gaming problems based on parent reports only (both p = .020) . Moderating roles of general functioning and affective involvement subdomains of family functioning were also highlighted. ADHD/ODD symptoms are positively associated with gaming problems reported by parents but not adolescents, probably reflecting reporting bias. Improving family functioning could be protective against problematic gaming in the ADHD population.
Plain Language Summary
This article compares parent and adolescent reports of gaming problems and explores a moderating role of family functioning on gaming problems in adolescents with ADHD. What’s Known on This Subject: ADHD increases the risk of problematic gaming and a good family environment could be protective. Most previous studies rarely focused on this at-risk population and relied on self-reports of gaming despite a risk of reporting bias. What This Study Adds: Symptom severity is positively associated with gaming problems reported by parents but not adolescents. Family functioning is negatively associated with gaming problems regardless of informants. The moderating effect of family functioning is detected only when gaming is reported by parents.
Introduction
Both online and offline game playing have been a rapidly growing global phenomenon. However, excessive time used on gaming might develop into behavioral disorders such as Internet gaming disorder (IGD), which is included as a condition for further study in the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2022). In addition, gaming disorder is officially classified as a mental health disorder according to the 11th revision of the International Classification of Diseases by the World Health Organization (World Health Organization, 2019). A recent meta-analysis revealed that the worldwide prevalence of gaming disorder was 3.05% with higher rates among adolescents and males (Stevens et al., 2021). A systematic review of evidence has shown that problematic gaming is associated with multiple adverse psychological and physical health outcomes, including depression, anxiety, attention deficit, sleep problem, and somatization (Mannikko et al., 2020), supporting its significance for clinical attention.
Attention-deficit/hyperactivity disorder (ADHD), characterized by inattention, hyperactivity, and impulsivity, is the most common neurodevelopmental disorder in children and adolescents and commonly co-occurs with problematic gaming. For example, a large cross-sectional study in Sweden found that the prevalence rate of ADHD among adolescents with problematic gaming is approximately 20% in the community setting and doubles in the clinical setting (Vadlin et al., 2016). A positive association between ADHD symptoms and problematic video game play was also consistently reported in both adolescent and adult populations (Dullur et al., 2021; Gonzalez-Bueso et al., 2018; Jeong et al., 2021; Panagiotidi, 2017; Tolchinsky & Jefferson, 2011), suggesting a link between ADHD symptoms and gaming behaviors. Moreover, a 3-year prospective study in patients with IGD showed that those with comorbid ADHD have a lower recovery rate, greater recurrence rate, and more severe IGD symptoms over time than those without the comorbidity (Lee et al., 2021). On the other hand, ADHD with comorbid IGD shows more severe ADHD symptomatology, more internalizing symptoms, and more impairment than those without IGD (Berloffa et al., 2022), emphasizing the seriousness of the co-occurrence of these two conditions.
Family environment is another key factor influencing gaming behaviors. A recent systematic review found that positive parenting and positive family dynamics are associated with lower rates of both problematic gaming and problematic Internet use in adolescents, whereas negative parenting and negative family dynamics are associated with higher rates of both conditions (Nielsen et al., 2020). A large prospective study in school children also found that parent-child connectedness and a warm family atmosphere are protective against pathological gaming assessed 2 years later, and an increase in family warmth is associated with a decrease in pathological gaming (Liau et al., 2015). In addition, an intervention study in China demonstrated that a 6-week multi-family group intervention significantly reduced the time children spent over the internet and the proportion of those meeting the criteria of pathological gaming by 96%, which is partly explained by improved parent-adolescent communication and closeness as well as fulfillment of children’s psychological needs in real life (Liu et al., 2015). Altogether, such evidence highlights the critical role of a positive family environment in counteracting gaming problems.
Despite existing research on the interrelation among ADHD symptoms, family functioning, and IGD (Chu et al., 2012; Moen et al., 2016; Peñuelas-Calvo et al., 2021), evidence on the influences of family functioning on problematic gaming specifically in the ADHD population is much scarce. Besides, previous studies on problematic gaming mostly rely on self-reporting of gaming behaviors, which is potentially subjected to response bias due to a lack of insight or social desirability effect (Blake & Klimmt, 2012; Kahn et al., 2014). Indeed, a recent comparative study using a clinical diagnosis of IGD as a gold standard has detected a false negative rate of self-report IGD to be as high as 44% (Jeong et al., 2018). Therefore, in this study, we aimed to investigate the relationships between the severity of ADHD/oppositional defiant disorder (ODD) symptoms, family functioning, and problematic gaming using reports from both adolescents and their parents. We hypothesized that the ADHD/ODD symptom severity would be positively associated with problematic gaming, whereas family functioning would be negatively associated with problematic gaming. We also hypothesized that the relationships between ADHD/ODD symptoms and gaming problems would vary by the level of family functioning.
Methods
Participants
This cross-sectional study enrolled adolescents aged 12–18 and their parents from a psychiatric outpatient unit at a university hospital in Bangkok, Thailand, from January to July 2020. Those who were diagnosed with ADHD based on the Diagnostic and Statistical Manual of Mental Disorders (DSM), Fifth Edition (American Psychiatric Association, 2022) were included in this study with their caregivers. Exclusion criteria were (1) not playing games in the past 3 months; (2) having other serious neurodevelopmental comorbidities, including intellectual disability, schizophrenia, bipolar disorder, and autistic spectrum disorder; and (3) not willing to participate in this study. Written informed assent and consent were obtained from adolescent participants and their parents, respectively.
Measurements
ADHD Symptomatology and Treatments
Parents were asked to report pre-treatment symptoms of ADHD and ODD of their child, using the Swanson, Nolan, and Pelham IV Scale (SNAP-IV) 26 items for parent rating (Thai version) (Pityaratstian et al., 2014) It comprises 18 items from the DSM-IV criteria for ADHD (i.e., nine items for inattention and nine items for hyperactivity/impulsivity) and eight items from the DSM-IV criteria for ODD. Symptom severity was rated on a 4-point scale from 0 (not at all) to 3 (very much), with higher scores indicating more severe symptoms. Cronbach’s alpha of the SNAP-IV Thai version in our sample was .93. Additionally, medical records were reviewed to gather data regarding co-morbidities and medical treatments for ADHD.
Gaming Behaviors
Adolescents were asked to report their gaming behaviors in the past 3 months and respond to the Game Addiction Screening Test - child and adolescent version (C-GAST) to assess gaming problems (Pornnoppadol et al., 2014). The C-GAST contains 16 items assessing three domains of problematic gaming including preoccupation with games, loss of control, and functional impairment. Each item was rated on a 4-point scale (0–3), with greater scores indicating more severe problematic gaming. At a cut-off score of 24, the C-GAST could screen boys with self-identified game addiction at a sensitivity of 68% and a specificity of 89% (Pornnoppadol et al., 2014). For girls, a C-GAST cut-off score of 16 demonstrated a sensitivity of 88% and a specificity of 88% for game addiction (Pornnoppadol et al., 2014). Cronbach’s alpha of the C-GAST in our sample was .88.
Parents were also asked to respond to the Game Addiction Screening Test - parent version (P-GAST) (Pornnoppadol et al., 2014), a 16-item questionnaire assessing problematic gaming of children based on parents’ perspectives. Each item was rated on a 4-point scale (0–3), with greater scores indicating more severity of problematic gaming. At a cut-off score of 20, the P-GAST could screen children identified by their parents as having game addiction with a sensitivity of 92% and a specificity of 88% (Pornnoppadol et al., 2014). Cronbach’s alpha of the P-GAST in our sample was .93.
Family Functioning
Adolescents were asked to respond to the Chulalongkorn Family Inventory (CFI) (Trangkasombat, 2006), a questionnaire specifically developed for Thai families to evaluate personal perceptions of one’s family based on the McMaster Model of Family Functioning (Epstein et al., 1978). It comprises 36 items, some of which were modified from the Family Assessment Device (Epstein et al., 1983). The items are categorized into seven dimensions: problem-solving (i.e., the ability of the family to resolve problems and overcome difficulties), communication (i.e., the degree to which family members effectively communicate with one another in a direct and clear manner), roles (i.e., the recurrent patterns of behavior by which family members fulfill family functions and needs), affective responsiveness (i.e., the ability of family members to respond with appropriate emotions to situations in the family), affective involvement (i.e., the degree to which the family shows interest in and values the activities and interests of other family members), behavior control (i.e., the expected standard and rules of conduct to limit inappropriate behaviors of family members), and general function. The option was a 4-point scale (1 to 4), making up a total score ranging from 36 to 144; the higher the score, the better the family functioning. All the items of each dimension were also averaged to indicate domain functioning index ranging from 1 to 4. In the original study, the scale could differentiate psychiatric patients from a general population sample (Trangkasombat, 2006). Cronbach’s alpha of the scale in our sample was .90.
Statistic Methods
Sample size calculation was performed a priori using G*power software version 3.1.9.6 (Faul et al., 2009). According to a recent systematic review (Dullur et al., 2021), the association between ADHD and gaming disorder appears to be small to medium effect size. Therefore, if the expected effect size f2 is 0.06, we need a sample size of 133 for a multiple linear regression model with seven predictors to have a power of 80% and alpha of 0.05.
Statistical analysis was performed using STATA version 13.0 (StataCorp, 2013). The numbers of missing data are reported in Table S1. Using the Stata “mcartest” command, missingness was found to be completely at random and, therefore, was handled using pairwise deletion.
For univariate analyses, participants were dichotomized into non-problematic and problematic game users based on P-GAST or C-GAST scores to identify factors associated with clinically meaningful gaming outcomes to be further adjusted for in multivariate analyses. Demographic characteristics, illness-related factors, and gaming characteristics of the two groups were compared using a chi-square test for categorical variables, a t-test for normally-distributed continuous variables, and a Wilcoxon rank-sum test for non-normally-distributed continuous variables.
For multivariate analyses, continuous P-GAST and C-GAST scores were used as the outcomes to maximize the explained variance. To facilitate the interpretation of the findings, SNAP-IV scores and CFI scores were standardized to a mean of zero and a standard deviation of one. Then, multiple linear regression analysis was performed to test the main effect of ADHD/ODD symptoms and family functioning on gaming problems (i.e., P-GAST or C-GAST scores) in separate models. Participants’ characteristics showing an association with problematic gaming in the univariate analyses at p < .10 were added into the models as covariates. To investigate whether the relationships between ADHD/ODD symptoms and gaming problems vary by the level of family functioning, the interactions between SNAP-IV and CFI scores were tested using multiple linear regression analysis with similar sets of covariates. Subsequently, the Stata “marginsplot” command was used to plot conditional marginal effects of SNAP-IV and CFI scores at the mean, and one standard deviation (SD) above and below the mean on the prediction of P-GAST and C-GAST scores while keeping the covariates constant at the mean values. Statistical significance was set at p < .05. To explore the interplay between subdomains of ADHD/ODD symptoms and family functioning on problematic gaming, similar interaction analyses were performed, using each subdomain of SNAP-IV and CFI instead of the overall scores as exploratory analyses.
Results
Participant Characteristics
One hundred and forty-four pairs of adolescents with ADHD and their parents were enrolled in this study. The characteristics of the patients are shown in Table 1. Around 80% of the participants were males and had a well-educated parent (i.e., having a Bachelor’s degree or above). The parent reports were mostly provided by the mothers (72%). Forty-three (30%) and 92 (64%) were classified as problematic game users based on adolescent and parent reports, respectively. As indicated by parent reports, problematic users spent more time playing games than non-problematic users both during the semester (Z = −2.28, p = .02) and semester break (Z = −2.73, p = .006). However, no differences in time spent on gaming were detected when problematic gaming was classified based on adolescent reports (Supplemental Table S1). Online gaming was positively associated with parent-reported problematic gaming (χ2(1) = 4.14, p = .04). Spending money on games was positively associated with adolescent-reported problematic gaming (χ2(1) = 6.06, p = .01) but only showed a trend of association with parent-reported problematic gaming (χ2(1) = 2.96, p = .09). No significant associations were found between other game use characteristics and problematic gaming based on both informants (Supplemental Table S1).
Characteristics of the Participants.

Note. Mdn = median; IQR = interquartile range; SD = standard deviation; ADHD = Attention-deficit/hyperactivity disorder; ODD = oppositional defiant disorder.
N = 141 due to data missingness.
Earning disorders, n = 44 (31%); oppositional defiant disorder, n = 12 (8%); depression, n = 10 (7%); tics disorders, n = 8 (6%); and anxiety disorders, n = 6 (4%);
N = 121 due to data missingness.
N = 118 due to data missingness.
N = 138 due to data missingness.
Associations of ADHD/ODD Symptoms and Family Functioning with Gaming Problems
Adjusted for age, sex, and gaming characteristics, overall ADHD/ODD (B = 4.36 [95% CI 2.65, 6.06], p < .001) and all three domain symptoms (inattentive: B = 3.59 [95% CI 1.86, 5.32], hyperactive: B = 2.73 [95% CI 0.94, 4.52], ODD: B = 4.42 [95% CI 2.72, 6.12], all p < .005) were positively associated with parent-reported gaming problems (Table 2). However, no significant associations were found based on adolescent reports of gaming problems (Table 2). In contrast, overall family functioning was negatively associated with gaming problems reported by both parents (B = −3.24 [95% CI −4.98, −1.50], p < .001) and adolescents (B = −3.35 [95% CI −4.81, −1.89], p < .001; Table 2).
Main Effects of ADHD/ODD Symptoms and Family Functioning on Parent-Reported (P-GAST) and Adolescent-Reported (C-GAST) Gaming Problems.
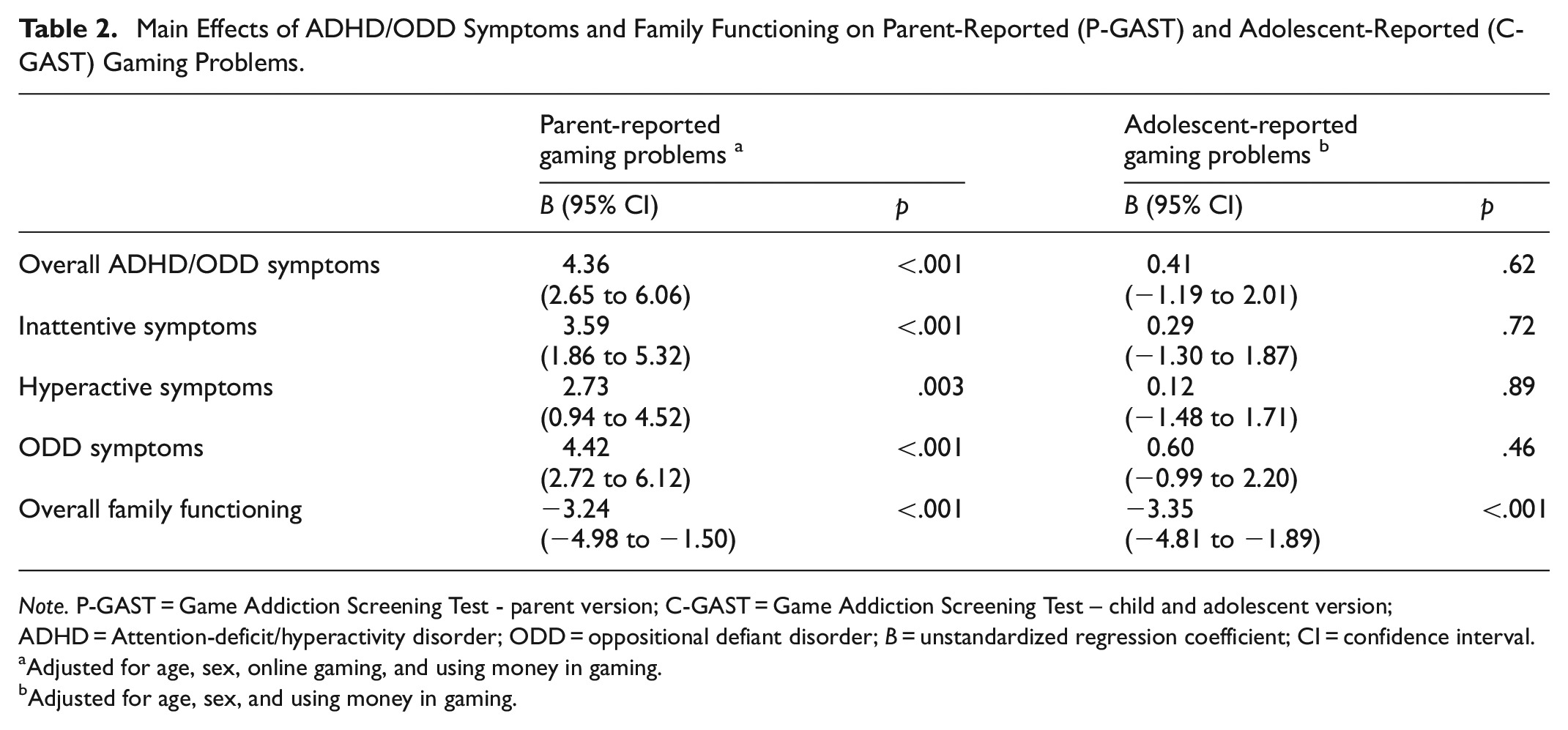
Note. P-GAST = Game Addiction Screening Test - parent version; C-GAST = Game Addiction Screening Test – child and adolescent version; ADHD = Attention-deficit/hyperactivity disorder; ODD = oppositional defiant disorder; B = unstandardized regression coefficient; CI = confidence interval.
Adjusted for age, sex, online gaming, and using money in gaming.
Adjusted for age, sex, and using money in gaming.
Interaction Effects Between ADHD/ODD Symptoms and Family Functioning on Gaming Problems
To investigate whether family functioning modifies the relationship between ADHD/ODD symptoms and gaming problems, an interaction analysis was performed. Controlling for demographic and gaming characteristics, family functioning showed significant negative interactions with overall ADHD/ODD (B = −1.99 [95% CI −3.65, −0.32], p = .02; Figure 1a) and inattentive symptoms (B = −1.97 [95% CI −3.63, −0.31], p = .02; Figure 1b) in predicting parent-reported gaming problems (Supplemental Table S2). However, no significant interactions with family functioning were observed for hyperactive (B = −1.13 [95% CI −2.88, 0.63], p = .21) or ODD symptoms (B = −1.13 [95% CI −2.72, 0.46], p = .16; Supplemental Table S2). When adolescent-reported gaming problems were used as the outcome, family functioning did not significantly interact with overall ADHD/ODD and domain symptoms in predicting gaming problems despite its significant main effects consistently observed across all models (Supplemental Table S2).

Margins plots showing linear prediction of parent-reported gaming problems at the specified values of overall family functioning and overall ADHD/ODD symptoms (a) or inattentive symptoms (b) while keeping covariates (i.e., age, sex, online gaming, and using money in gaming) constant at the mean values.
Exploratory analyses on subdomains of family functioning revealed that the general functioning subdomain negatively interacted with overall ADHD/ODD symptoms (B = −2.28 [95% CI −3.86, −0.70], p = .005), inattentive symptoms (B = −1.91 [95% CI −3.49, −0.32], p = .02), and hyperactive symptoms (B = −1.99 [95% CI −3.76, −0.22], p = .03) in predicting gaming problems based on parent reports (Supplemental Table S3). This pattern was not found for adolescent-reported gaming problems (Supplemental Table S4). The affective involvement subdomain significantly interacted with overall ADHD/ODD (B = −1.93 [95% CI −3.59, −0.27], p = .02) and hyperactive symptoms (B = −2.00 [95% CI −3.67, −0.34], p = .02) in predicting gaming problems reported by parents (Figure 2a and Supplemental Table S3), but not adolescents (Figure 2b and Supplemental Table S4). In contrast, the communication subdomain interacted with inattentive symptoms in predicting gaming problems reported by adolescents (B = 1.80 [95% CI 0.16, 3.45], p = .03; Figure 2d and Supplemental Table S4), but not parents (Figure 2c and Supplemental Table S3). However, the behavioral control domain consistently modulated the influences of ODD symptoms on gaming problems reported by both parents (B = −1.58 [95% CI −3.12, −0.04], p = .04; Figure 2e and Supplemental Table S3) and adolescents (B = −2.11 [95% CI −3.53, −0.69], p = .004; Figure 2f and Supplemental Table S4). No other significant interactions between family functioning subdomains and ADHD/ODD symptom domains were observed (Supplemental Tables S3 and S4).

Margins plots showing linear prediction of parent-reported (left) and adolescent-reported (right) gaming problems at the specified values of family functioning subdomains and ADHD/ODD symptoms while keeping covariates constant at the mean values. (a) and (b): affective involvement × hyperactivity; (c) and (d): communication × inattention; (e) and (f): ODD × behavioral control.
Discussion
In this study, we aimed to compare the associations between ADHD/ODD symptoms and gaming problems reported by parents and adolescents and to test whether family functioning could modify the relationship between ADHD/ODD symptoms and gaming problems. The results showed that the overall severity of ADHD/ODD symptoms, as well as all three symptom domains (i.e., inattentive, hyperactive, and ODD), was positively associated with gaming problems reported by parents, but not adolescents. Interestingly, family functioning was negatively associated with gaming problems regardless of informants and also interacted with overall ADHD/ODD and inattentive symptoms in reducing gaming problems based on parent reports, suggesting a protective role of good family functioning on problematic gaming.
Even though evidence supporting the link between ADHD symptoms and problematic gaming has been accumulated, most previous studies rely on self-report of gaming behaviors, posing a risk of response bias due to lack of insight or social desirability effect (Blake & Klimmt, 2012; Kahn et al., 2014). In this study, we found that time spent on gaming reported by adolescents appeared greater among those with problematic gaming identified by parent rating but not adolescent rating of gaming problems, implying poor reliability of self-assessment. Significant associations between gaming problems and overall ADHD/ODD and subdomain symptoms were also found solely when assessed by parents. This was in line with a recent systematic review reporting positive associations between gaming disorder and ADHD symptoms across all the studies included (Dullur et al., 2021). Consistently, large prospective studies in young children suggested a bidirectional relationship between gaming and attention problems (Gentile et al., 2012; Swing et al., 2010). In other words, exposure to video game playing is subsequently associated with lower attention (Swing et al., 2010); higher impulsivity and attention problems are associated with more time spent on gaming, which subsequently increases attention problems and impulsivity (Gentile et al., 2012). However, fewer studies exist to support the association of problematic gaming with hyperactivity/impulsivity specifically (Dullur et al., 2021; Yen et al., 2017). Interestingly, two intervention studies in patients with comorbid ADHD and problematic gaming showed that treating ADHD symptoms with methylphenidate or atomoxetine results in a reduction in gaming, which correlates with a decrease in total ADHD symptoms, inattention scores, and impulsivity (Han et al., 2009; Park et al., 2016), suggesting a shared pathway between both symptom domains and problematic gaming.
Apart from ADHD symptoms, an abundance of evidence indicates that family environment is another key factor influencing problematic gaming. We found that family functioning, reported by adolescents, was negatively associated with gaming problems regardless of informants. Providing the aforementioned risk of bias of adolescent reports on their gaming behaviors, this finding underlines a strong negative relationship between family functioning and problematic gaming. Furthermore, we found that family functioning, particularly affective involvement and general functioning subdomains, negatively interacted with ADHD/ODD symptoms in determining problematic game use, concordant with a prior study of problematic internet use in high-school students (Cacioppo et al., 2019). Evidence from intervention and prospective studies also supports the critical role of family warmth and closeness in counteracting problematic gaming and internet use (Liau et al., 2015; Liu et al., 2015). Altogether, these findings suggested that enhancing closeness and improving general functioning of the family could be a promising target of intervention for problematic gaming for the ADHD population.
Additionally, parallel analyses of information derived from both parents and adolescents also uncovered the interplay between certain domains of family functioning and ADHD/ODD symptoms that might explain discordant reports between both parties on gaming problems. For example, a positive relationship between inattentive symptoms and parent-reported gaming problems was consistently observed regardless of the level of family communication (Figure 2c); however, predicted adolescent-reported gaming problems decreased as inattentive symptoms increased if they perceived poor communication in their family (squares in Figure 2d). As adolescent-reported time spent on gaming also converged with parent-reported, but not adolescent-reported, problematic gaming, this observation implies that highly-inattentive adolescents who perceived family communication as unclear and indirect may be more likely to underreport their gaming problems. On the contrary, the interaction between behavioral control and ODD symptoms on gaming problems were consistently negative regardless of informants (Figure 2e and 2f), inferring that a strict family rule perceived by adolescents might help limit problematic gaming among those with more ODD symptoms. Altogether, we suggested future research in children and adolescents should employ a system approach to delve deeper into the interconnection between multidimension of family functioning, ADHD/ODD symptoms, and gaming problems while acknowledging a potential reporting bias influenced by different family dynamics.
Strengths and Limitations
To our knowledge, we are the first to explore the interacting effects between family functioning and clinical symptoms on problematic gaming in adolescents with ADHD. The parallel investigation of gaming behaviors based on perception of both adolescents and parents to unmask the potential reporting bias linked to informant-based assessment is another major strength of our study. Moreover, we also looked into the relationships between different domains of ADHD/ODD symptoms and family functioning in determining problematic gaming, which provided deeper insights into the interplay between these substructures in influencing gaming behaviors.
However, the interpretation of our findings should also be considered in light of potential limitations. First, the sample size of our study was relatively small, which might render the detection of interaction effects underpowered (<80%) for an effect size f2 of <.055 and limit the analysis to account for other psychiatric co-morbidities. Second, the majority of our participants were boys with well-educated parents, which could limit the generalizability of current findings to girls and those with lower parental education. Moreover, more than half of our sample is not a single child and has a close person (i.e., friends and family members) playing games, which is a common scenario for Asian countries. Therefore, cross-cultural comparison is deserved to gain more insight into the interplay between subdomains of family functioning and ADHD symptoms across a variety of family structures and sociocultural contexts. Third, as exploratory analyses, we did not correct for multiple testing in analyzing subdomains of family functioning and ADHD/ODD symptoms, which might lead to type I errors. Further studies should be conducted using a larger sample size to follow up on our findings. Finally, causality could not be drawn due to the correlational nature of our study. Experimental studies intervening in specific domains of family functioning might be warranted to prove their causal influences on problematic gaming in ADHD children.
Conclusion
ADHD/ODD symptoms are positively associated with gaming problems reported by parents but not adolescents, probably due to reporting bias. Family functioning is negatively associated with gaming problems regardless of informants and also modulates the relationships between ADHD/ODD symptoms and problematic gaming based on parent reports. Improving family functioning, especially in the domains of affective involvement and overall function, could be a key strategy for intervening in problematic gaming in the ADHD population. Future research should use an unbiased assessment of gaming behaviors and employ a system approach to delve deeper into the interconnection between family dynamics, ADHD/ODD symptoms, and problematic game use.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251367096 – Supplemental material for Discrepant Parent-Adolescent Reports of Gaming: A moderating role of family functioning in ADHD
Supplemental material, sj-docx-1-sgo-10.1177_21582440251367096 for Discrepant Parent-Adolescent Reports of Gaming: A moderating role of family functioning in ADHD by Thanavadee Prachason, Kittikoon Thiamkaew and Nida Limsuwan in SAGE Open
Footnotes
Abbreviations
ADHD: attention-deficit/hyperactivity disorder
ODD: oppositional defiant disorder
CI: confidence interval
DSM: Diagnostic and Statistical Manual of Mental Disorders
SNAP-IV: Swanson, Nolan, and Pelham IV Scale
C-GAST: Game Addiction Screening Test - child and adolescent version
P-GAST: Game Addiction Screening Test - parent version
CFI: Chulalongkorn Family Inventory
SD: standard deviation
Mdn: median
IQR: interquartile range
Ethical Considerations
The Ethics Committee of the Faculty of Medicine Ramathibodi Hospital approved this study (reference number: COA. MURA2020/34).
Author Contributions
Thanavadee Prachason supervised data analyses, and critically reviewed and revised the manuscript for important intellectual content. Kittikoon Thiamkaew designed the data collection instruments, collected data, carried out the initial analyses, and drafted the initial manuscript. Nida Limsuwan conceptualized and designed the study, supervised data collection, and drafted the initial manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from the Faculty of Medicine Ramathibodi Hospital, Mahidol University for publishing this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.