
Abstract
For this qualitative case study, 23 semistructured interviews were conducted with clients of a private coaching center in the Netherlands. We explored why adults with attention deficit/hyperactivity disorder (ADHD) prefer coaching, which is financed out-of-pocket, over public mental health care and what the perceived added value is for them. The participants highly valued the optimistic strength-based and solution-focused approach, which was contrasted with what they have experienced as a deficit and symptom-centered approach in public mental health care. Coaching was perceived as a joint venture, resulting in a more thorough understanding of how one approaches life and can be better equipped to deal with future problems. This study identified a group of adults with ADHD who feel that their needs are currently unsatisfactorily addressed in public mental health care. Future research should further explore whether this is a specific group of adults or whether these experiences are more common.
Introduction
Attention deficit/hyperactivity disorder (ADHD) is increasingly diagnosed and treated in adults (American Psychiatric Association [APA], 2000; Fredriksen, Halmøy, Faraone, & Haavik, 2013). In the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000), the symptoms are categorized as inattention, hyperactivity, and impulsivity (APA, 2013). 1 A growing body of literature addresses the impact of adult ADHD on daily life, including underemployment and academic underachievement (Adamou et al., 2013; Biederman et al., 2008), low self-esteem, problems with intimate relationships (Eakin et al., 2004), and, in general, a lowered quality of life (Able, Johnston, Adler, & Swindle, 2007; Kooij, Bejerot, Blackwell, Caci, & Casas, 2010; Young & Amarasinghe, 2010). This evidence suggests that adult ADHD is a serious disorder that requires diagnoses and treatments that address not only an individual’s symptoms but also how ADHD affects daily functioning.
Treatment for adult ADHD in the Netherlands generally involves two approaches: pharmacotherapy, mainly in the form of psychostimulants such as methylphenidate (Ritalin), and psychosocial interventions, such as psychoeducation, skill training, and cognitive behavioral therapy (CBT; Kooij et al., 2010). Pharmacological treatment of ADHD has proven effective in reducing symptom severity in several randomized controlled trials (RCTs; Mészáros et al., 2009; Surman, Hammerness, Pion, & Faraone, 2013). Pharmacological treatment alone, however, may not sufficiently improve negative impacts of ADHD beyond these symptoms, and, therefore, many scholars recommend a combination of pharmacological and psychosocial interventions as treatment (Emilsson et al., 2011; Kooij et al., 2010; Murphy, 2005; Weiss et al., 2012). Despite this, psychosocial interventions remain largely unstudied and lack scientific support (Moriyama, Polanczyk, Terzi, Faria, & Rohde, 2013).
The guidelines for mental health care in the Netherlands, including the guidelines for the diagnosis and treatment of adult ADHD, favor treatment options which have been proven effective using RCTs, which are often considered the “gold standard” in evidence-based medicine (Hutschemaekers & van Kalmthout, 2006). The focus on evidence-based interventions stimulates new forms of therapy, such as strength-based coaching, to develop outside of the public mental health system. Nevertheless, for people with mental health problems, there is an increase in the use of complementary and alternative treatments, as well as the scientific enquiries as to how and why these treatment options are utilized (Bahceci et al., 2013; Segar, 2012; Vlieger, 2007), particularly for children with ADHD (Majorek, Tüchelmann, & Heusser, 2004; Sinha & Efron, 2005).
In the Netherlands, a growing number of private “ADHD clinics” and “coaching” centers offer treatment for adults with ADHD, which differ from services provided in public, reimbursed mental health care. Many of these centers describe themselves as “strength-based coaching centers.” 2 Strength-based coaching aims to reinforce and utilize innate competences to achieve goals established by both the client and coach (Linley & Harrington, 2006b). Strengths can be defined as “a natural capacity for behaving, thinking, or feeling in a way that allows optimal functioning and performance in the pursuit of valued outcomes” (Linley & Harrington, 2006a, p. 88). Moreover, coaching offered in these centers does not adhere to a specific theoretical foundation but typically draw from a number of complementary and alternative methods such as mindfulness, neurolinguistic programming, solution-focused brief therapy, and transactional analysis. As of yet, strength-based coaching is not a part of official clinical guidelines in the Netherlands and, to the best of our knowledge, no articles have been published that describe the added value of this type of coaching in the treatment of ADHD.
The consequences for clients of these centers are that these services are not reimbursed by health insurance and are principally financed by out-of-pocket payments from users. That clients do pay for these coaching services implies that adults with ADHD have needs that are not fully addressed by public mental health and that these coaching services represent a niche that may address these needs. As little is known about these coaching practices for adults with ADHD, a good starting point is to explore the reasons why adults with ADHD seek, and pay for, treatment at these centers and what, from their perspective, the added value is in relation to treatment received in reimbursed mental health care. In addressing this knowledge gap, we aim to explicate what the unmet needs are of adults with ADHD that drive them to seek treatment at these centers, what the actual experiences are with treatment in these centers and the perceived added value of these treatments, and, finally, what lessons can be learned for the treatment of adult ADHD in general.
Methodology
An exploratory qualitative case-study design was chosen for this study. A strength-based coaching center in the Netherlands was selected and semistructured interviews were conducted with its clients.
Case Selection and Description
The selection criteria for a center were twofold: first, the provider must provide treatment for adult ADHD outside the public mental health system; second, it must have scaled up its services, implying it addresses a gap in current services for adults with ADHD. We selected a coaching service based in Delft, a medium-sized city in the metropolitan area of The Hague. When founded in 2007, the center had one facility. By 2015, it had grown to 13 facilities throughout the country. Moreover, its client base has steadily increased over the same period of time, with 186 invoiced ADHD coaching sessions in 2007 and 1,907 in 2013.
At the basis of the center’s approach is the vision that the problems of adults with ADHD, in addition to their symptoms, stem from the “collateral damage” of having ADHD, namely, the negative coping strategies that one may have developed over the years living with ADHD. It argues that addressing this collateral damage can quickly lead to improvements in wellbeing and daily functioning. Taking this perspective, coaching aims to utilize and reinforce individual strengths and competences to address collateral damage and bring about positive changes in the lives of individual clients. Coaching in the center draws from a number of methods developed outside of the evidence-based therapies, including mindfulness, neurolinguistic programming, solution-focused brief therapy, and transactional analysis. In practice, coaches discuss with clients their personal goals and talents, and together they decide on the content of an individual coaching plan matching the talents, needs, and wants of the individual client. This treatment trajectory, then, includes both the level of skills and abilities as well as a deeper level of emotions and self-confidence. Coaches are internally trained and receive internal examinations as well as continued education as employees of the center in the form of regular intervision meetings.
Recruitment
As this study is a qualitative explorative case study, the focus of participant inclusion aimed to obtain the full variety of perspectives held by the clients of this coaching (Green & Thorogood, 2005; Patton, 1990). The method for including participants was twofold (Figure 1). First, for convenience sampling, an e-mail was sent to the entire client base of the center, inviting clients to contact the researcher if they were interested in participating. Second, for purposeful sampling, coaches were requested to enquire whether clients would be interested in participating, and, if so, provide a short description of the study and the contact information of the researchers for official participation. By purposefully inviting clients who held critical opinions, either or both positive, negative, or both, toward the center, a diversity of attitudes and views was ensured.
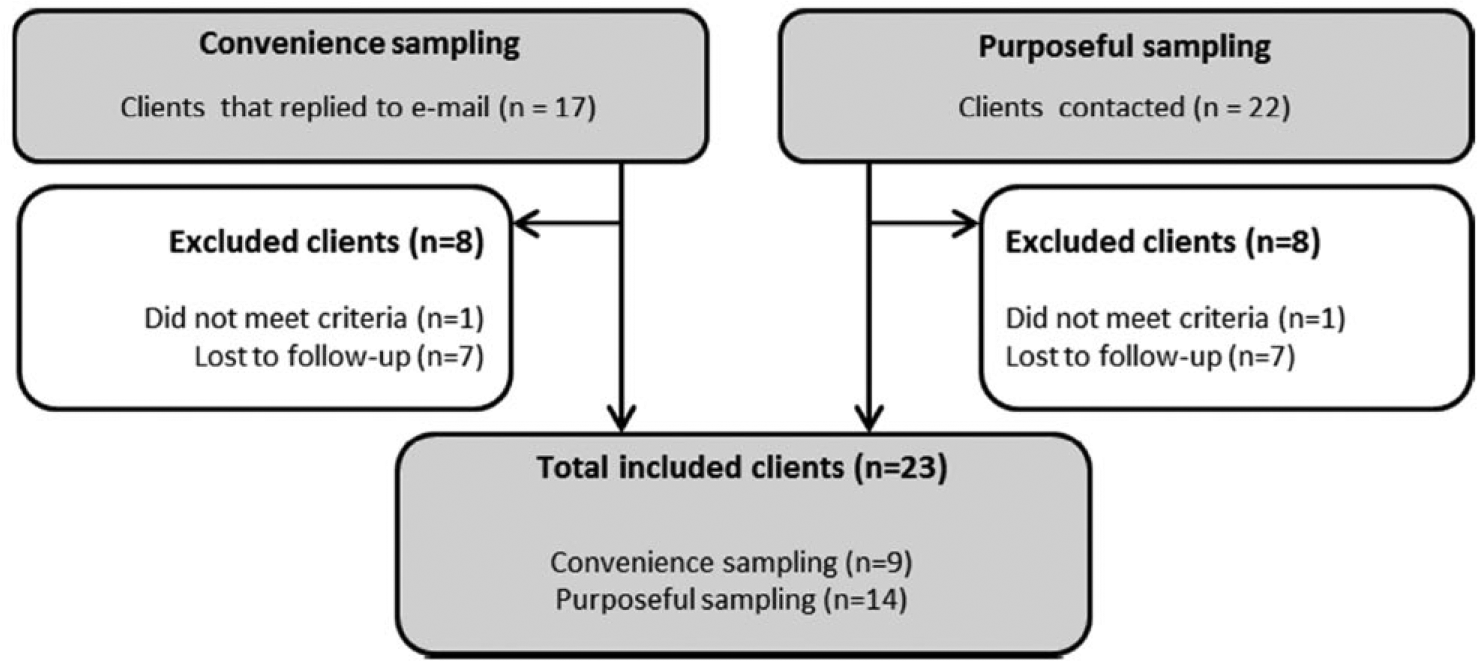
Number of clients contacted and included per recruitment strategy.
Interviewees were included if they had a primary ADHD diagnosis or a diagnosis in-progress. Clients with comorbid diagnoses were also included because 60% to 89% of adults with ADHD are estimated to have at least one comorbid psychiatric disorder (Sobanski, 2006). As adult ADHD can cause serious problems with both education and employment (Adamou et al., 2013; Biederman et al., 2008), only participants above the age of 25 years were eligible to take part, to highlight experiences with education and employment, and treatment.
Data Collection
Semistructured interviews were chosen for this study because this method allows study participants to further elucidate on topics that are of great importance to them while maintaining focus on topics of interest for the researchers (Britten, 1995). Main themes were experiences with the current treatment, experiences with previous treatments, favorable and unfavorable characteristics of therapists and therapies, and the extent to which these characteristics were encountered during coaching and during previous treatments.
The location of the interview was decided on by the interviewee and was required to be an environment where an open conversation was possible. The main reason for this was to ensure the interviewed clients would feel comfortable in addressing specific thoughts or feelings with regard to their therapist. Interviews were conducted by one interviewer (first author) who explicitly mentioned affiliation with the university, of the whole research team, with no interest in positive evaluation of the received therapy. Thirteen of the interviewees preferred to speak in a private room at the coaching center; four interviews were conducted at home and one at the office of the respondent. Interviews lasted 40 to 90 min.
Data Analysis
Interviews were recorded and transcribed verbatim and summaries were sent to the respondents as a member check. Transcripts were read carefully and analyzed using open coding in line with the content analysis of Hsieh et al. (Hsieh & Shannon, 2005). With this approach, a preliminary coding scheme was developed. After that, a selective coding scheme was discussed and agreed upon by the research team; this scheme was then used in Atlas.ti qualitative data analysis software for selective coding. Intermediate results were reviewed by the research team on a frequent basis, and doubts and disagreements were discussed until consensus was reached.
Ethical Considerations
According to Dutch law, no approval from an ethical commission was needed as the study explores perspectives on health care and not medical histories and medical dossiers and is therefore not considered invasive and psychologically and emotionally disturbing. Before recording, verbal informed consent was obtained for recording and publication of data under the promise of anonymity. Participants were informed of opportunity to retract from the study at any time without providing a reason and without consequence.
Results
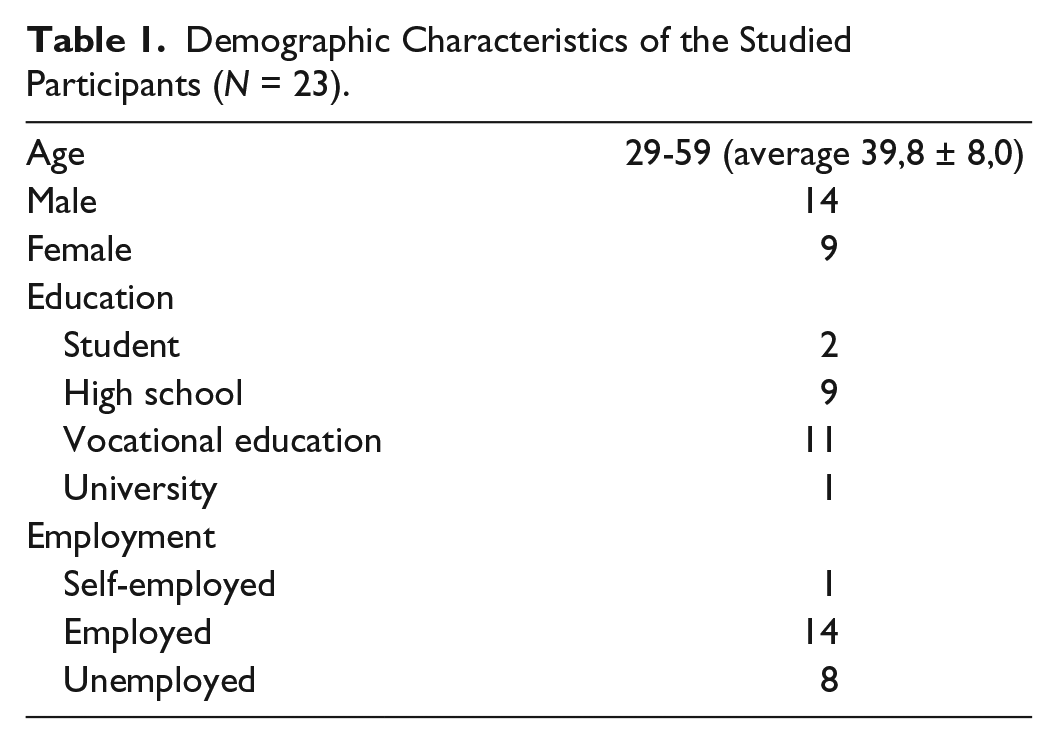
In total, 22 clients were interviewed face-to-face and one on the phone because no suitable time and location could be found; 14 were male and the average age was 40 years. All participants but one had an official attention deficit disorder (ADD) or ADHD diagnosis, and, all but one participant had experiences with mental health care before starting coaching at the center. Five interviewees were known to be taking stimulant medications at the time of the interview. Further demographic information is presented in Table 1.
Demographic Characteristics of the Studied Participants (N = 23).
From Public to Private Mental Health Care
Most participants had longstanding treatment histories with formal mental health care up to 14 years. Moreover, a majority of clients was treated for other problems other than ADHD, most of which were depression and burnout complaints. Therefore, they had experiences with medications other than those used for the treatment of ADHD, such as antidepressants or antianxiety medications. The experiences with formal mental health care were often portrayed as negative, especially when compared with coaching received at the center. For most participants, it took a long time before ADHD was recognized as the core problem; the diagnosis and treatment of ADHD started many years after first contact with mental health care, which was often portrayed with a negative tone: I wasn’t initially treated for ADHD. Before that [the diagnosis of ADHD], I think I had every psychiatric diagnosis possible: depression, dysthymia, that is why it took me so long, up to 12 or maybe 13 years. Until, finally, someone had the clarity of mind to say, “well, maybe this [ADHD] is your problem.” (P6, male)
During the interview, the interviewer asked the participants to elaborate on reasons for searching for alternative service providers for ADHD therapy and why they chose this particular center. Most participants indicated that they found it “by chance” on the internet or via friends or family and became interested by the vision and method of the center after an introductory session or after further research: Their approach appealed to me. You know, the combination of methods they use. The way they work fits me better than that pragmatic work [previous therapy] where they just ask you: well, what do you need? (P11, female) The atmosphere felt right also in terms of their approach, which is really positive ( . . . ) looking at the possibilities instead of the deficits, and that is exactly what I am too. With me the glass always is half-full. (P14, male)
Appraisal of Optimistic Approach
A majority of clients perceived the center as being solution focused in that coaches try to draw the attention away from life problems and toward the things that go well and toward solutions to the problems. In contrast, previous mental health providers often framed their problems as chronic; for example, one interviewee explained that her psychiatrist told that mental illness is “just the same as diabetes, you’ll never get rid of it” and that she would never overcome it. Contrastingly, most interviewees explained that it is a better strategy to shift the focus away from problems people can experience: At the moment you dig yourself into your garbage bag [mental health problems], you get down, and you see the dark side of everything, and you’re unable to see the positive side of things. The advantage [of this center] is that they stop you from digging yourself into that garbage bag, and that garbage bag is good for no one. (P5, male)
Coaches point their clients to competences and talents which can be exploited. Interviewees felt that this approach fosters a more positive outlook on daily life, an important step in moving away from a focus on the deficits imposed by ADHD, toward the hope of a better life.
And they [coaches] really looked at the possibilities. People can achieve so much, but sometimes one doesn’t know how to anymore. So all of a sudden, the negativity and causes of my problems were not in the picture anymore so to say. And then I thought, well if other people can overcome their problems, I too can get better. (P4, female)
According to a minority of the participants, however, there are limits to the abovementioned approach. For example, one participant explained that she had the feeling the coaches somehow neglected the existence of ADHD, while, for her, the ADHD diagnosis had been reassuring; she wanted to reframe her life in accordance with ADHD as it explained a long history of problems in her life. Another participant doubted the sincerity of the positive approach and felt that it represented an avoidance of taking responsibility to support the client in certain situations. In this example, the client had to see a doctor hired by the state to evaluate the repercussions of his diagnosis and treatment as they related to his employment and wanted his coach, for credibility and support, to come to this appointment: She [the coach] would never honestly say she herself can’t come to the company doctor; instead, she would make it a pep-talk pushing me to do it myself which will only make me stronger. That’s all fine but, in this way, she makes everything the responsibility of the client. (P15, male)
It was stressed that, the positive approach should not overlook or dismiss the self-perceived needs of clients, and coaches should be sensitive as to when a more supportive role is necessary. When this was not done, the clients felt that their needs were not met or started to doubt the sincerity of the approach.
Being Accepted as a Unique Person
In line with this positive and strength-based approach, clients felt accepted as a unique person with unique strengths, competences, needs, and desires. This was frequently opposed with other experiences where clients felt equated with their disorders or where they were treated as “a number.” Formal mental health care was often described as impersonal: It was shocking to see how easily diagnoses were distributed in that institute [outpatient clinic], ( . . . ) like a factory where everyone enters, gets diagnosed, gets medicated. ( . . . ) It is so massive and not attuned to the individual. (P7, male)
In contrast, interviewees communicated the coaching process as a joint venture of both the coach and the client in which personal goals and coaching strategies were mutually agreed upon and aligned with the preferences of the client: I really feel that she [the coach] takes me seriously and that she looks at what I need. You know, sometimes I give my ideas and she gives hers, and then we discuss. And for me, that is being taken seriously. (P3, male)
Personal Relationship With the Coach
An important aspect of the coach–client relationship is, according to a majority of the participants, a “personal connection” or a “click” with their coaches which makes clients feel a mutual respect from both parties. This connection, already touched upon in the previous paragraph, was considered to be the result of the open, accepting attitude of the coaches.
It feels safe. I never have the feeling that she [coach] judges me. Everything is just fine and everything is good ( . . . ) and in that way she makes better connection with the client. (P22, male)
On the other hand, with respect to experiences with formal mental health care, some participants felt that their therapists were unapproachable and not open to discussing treatments and goals prescribed by the therapist: when I told them the medications did not work well they told me I shouldn’t be so stubborn and do what they told me to do, you know, ( . . . ) the standard approach works best so don’t be difficult. (P4, female)
Additionally, some participants valued their coaches as being “capable by experience” which, in turn, reinforced the “click” they experienced. Many coaches have endured struggles with adult ADHD and/or other mental disorders. This additional experiential knowledge gave some of the clients the feeling that their coach could better connect with them. Self-disclosure, according to some participants, was reassuring in times when clients felt they could never overcome their problems. Nevertheless, according to one client, the use of personal stories should be limited: Sometimes personal stories [of the coach] can really work to clarify things or show how certain things work. But, you know, only in some situations, you should not continuously tell your personal stories to the client. (P23, female)
Experienced Outcomes of Coaching
While discussing the outcomes of coaching, participants were often not able to clearly describe what changed and how these changes were brought about. Clients generally explained that it “worked better than previous therapies.” When the interviewer asked why this was the case, participants replied that it was “more substantial” and “more thorough,” or that it “simply just worked better.” In taking this conversation further, two outcomes stood out, namely, insight into how and why a person approaches daily life and feeling being better equipped when future problems arise.
By far the most frequently expressed outcome of coaching was insight. Participants mentioned that therapy enabled them to understand themselves, what they are doing, and how and why they are doing it. Clients contended that coaching at the center lets you discover who you are, and what you are allowed to be . . . how your internal communication works, how you treat other people. They [coaches] teach you how to enjoy life, something very simple actually. (P6, male)
Some clients explained that receiving coaching made it easier for them to proactively search for solutions and options when confronted with problems rather that becoming caught in the problem again. In this way, problems become less pervasive, but more importantly, some of the participants felt they had gained more control over problems by knowing what works for them. For one person this was relaxing exercises, whereas for another person it was taking a step back: Well, when I encounter problems in my life again I know I have to take a step back and think of what it is I need. And if I listen to what I need, I feel a lot better a lot faster than I used to. (P3, female)
Discussion
This study aimed to explore why adults with ADHD utilize out-of-pocket private coaching services over reimbursed public mental health care and what for them is the perceived added value of these services. All but one of the participants started to look for complementary services after longstanding experiences with public mental health care. Experiences with the coaching center were often described in contrast to this history often described as a series of negative experiences. The difficulties of adults to obtain a formal ADHD diagnosis, such as frequent misdiagnoses and longstanding contacts in mental health care before an ADHD diagnosis, are known in literature (Kooij et al., 2010; Matheson et al., 2013). Matheson et al. (2013) also described the negative feelings of their participants who perceived obtaining a diagnosis and treatment as an “uphill struggle.” Our participants were more negative about public mental health care, which, of course, does not imply that treatment received in public mental health care is bad per se, but that for this group of people it did not function ideally.
Psychosocial interventions for ADHD in formal mental health care focus on psychoeducation about ADHD and the impact it has on one’s life, coping strategies to deal with living a life affected by ADHD, and the acquisition of skills necessary to function in daily life (Knouse & Safren, 2013; Murphy, 2005; Ramsay, 2009). These interventions, with the exception of CBT, try to compensate for the deficits that adults with ADHD generally have, such as problems with bookkeeping and planning. Coaching at the studied center, according to the study participants, deviates from this approach in three ways: first, it concentrates on problems and goals the clients want to address rather than focusing on predefined topics that are categorically assumed to be problematic for adults with ADHD in traditional conceptualizations of adult ADHD. Second, it aims to reinforce personal strengths and competences that can be used to address problems and reach the clients’ goals. Third, self-disclosure of the life experiences of coaches is deliberately used. These were the differences that were valued by the interviewees of this study. Moreover, clients felt that coaching had a positive and substantial impact on their lives and wellbeing.
Participants especially valued the optimistic and strength-based approach, which they felt fostered hope for a better life. Clients felt they were trained to use personal strengths and competences to overcome the deficits posed by ADHD. Furthermore, coaching was perceived as person-centered as clients felt accepted as a unique person and the coaching process was described as a joint venture. Fostering hope and healing in individuals by reinforcing personal strengths and competences (Jacobson & Greenley, 2001; Slade, 2010), person-centeredness, and the belief that everyone is capable of overcome mental illness to live a meaningful life (Farkas, 2006; Farkas, Gagne, Anthony, & Chamberlin, 2005; Slade et al., 2014) has been described as essential in building a meaningful life with schizophrenia. The importance of therapists’ empathy toward patients has been discussed in relation to treatment for depression (Davidsen & Fosgerau, 2014). As the participants frequently appraised these themes, often in contrast with reimbursed ADHD care, it can be concluded that the unmet needs of adults with ADHD relate to these characteristics of treatment. There is a vast literature that addresses these themes for severe mental illness; however, to the best of our knowledge, this is the first article to show the added value of these optimistic, strength-based, and person-centered practices in the treatment of adults with ADHD and, therefore, further exploration of use of these practices in ADHD care is merited.
This study has limitations. First, it is possible that the interviewed clients do not resemble the total client base of the center due to selection bias. We did, however, try to minimize bias by using two recruitment strategies (convenience and purposeful sampling). Second, it is not possible to generalize our findings to the greater population of adults with ADHD, due to the small exploratory design. Moreover, the participants in this study belong to a specific group: people with longstanding, often negative, contacts with formal mental health care where they have frequently been treated for other disorders than adult ADHD. Although we cannot elaborate on the characteristics or magnitude of this group in the general population, we did show the existence of a group of service users who feel that their needs are inadequately addressed by contemporary public mental health care in the Netherlands. These people seem to benefit from complementary strength-based coaching services.
In light of our results and given the limitations of this study, two directions for future research can be identified. On the one hand, more research is needed to pinpoint the size and characteristics of the group of adults with ADHD who can benefit from strength-based coaching services and who feel that their needs and preferences are overlooked and insufficiently addressed by contemporary ADHD treatments. On the other hand, more robust evidence is needed to support the use of strength-based coaching techniques in the treatment of adult ADHD.
Conclusion
Adult ADHD and its treatment are being increasingly studied and reported in contemporary literature. These investigations mainly limit themselves to evidence-based therapies, whereas other forms of therapy are on the rise yet remain unreported. Our findings suggest that strength-based coaching might prove beneficial for the treatment of adult ADHD, possibly in combination with treatments that are provided in the public sector.
The results of this exploratory study highlight two important findings. First, there is a group of adults with ADHD who feel inadequately addressed by public mental health care, and second, these adults seem to benefit from strength-based coaching. Future research should focus on quantifying the prevalence of adults with ADHD who have unmet needs in the public health care system.
Footnotes
Acknowledgements
The authors wish to thank Cathelijne Wildervanck for her contributions and support to this study and also wish to thank the interviewed clients for their participation. The authors would like to thank Sarah Cummings for editing the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.