
Abstract
After the outbreak of the COVID-19 pandemic, the importance of the Effectiveness of Community Epidemic Prevention and Control (ECEPC) which is directly related to the safety of people’s health and the stability of the society, is highlighted under abnormal circumstances. However, researches on Community Emergency Preparedness (CEP) and ECEPC in low and middle-income countries are of different quality. This study adopted the random sampling method. 2,250 residents from 150 communities in 140 municipalities in 20 provinces in Chinese mainland participated in the cross-sectional survey on ECEPC, with 2,112 questionnaires validly returned. Data were analyzed through descriptive statistics with optimal scaling regression model to explore the influencing mechanism of CEP and Resident Emergency Response Capacity (RERC) on ECEPC. The results revealed that 74.47% of respondents thought ECEPC was relatively good, and over 40% of respondents thought emergency risk awareness, emergency mutual-aid capacity, and psychological resilience were fairly good. Both CEP and RERC had positive and significant effects on ECEPC. The impact ranking showed the importance of emergency response system drills was ranked first at 0.165. Emergency response system could be revised and improved in practical drills. The results of the study provided new recommendations for different measures to be taken in the preparation, adjustment, and improvement phases of Emergency Response System Drills, which were conducive to building a resilient community-based epidemic prevention and control system.
Plain language summary
CEP is an important tool for improving ECEPC. Existing studies have focused on the construction of emergency prevention and control systems in developed countries, calling on governments to play a more important role and assume more responsibilities in community epidemic prevention effectiveness and emergency prevention and control. This study used the random sampling method. 2,250 residents from 150 communities in 140 municipalities in 20 provinces in mainland China participated in the cross-sectional survey on ECEPC, with 2,112 questionnaires validly returned. This study believes that for developing countries and low-income countries, community epidemic prevention effectiveness requires the joint efforts of grassroots communities and residents, and communities should involve residents in emergency prevention and control drills.
Keywords
Introduction
In December 2019, a massive outbreak of COVID-19 pandemic occurred in Wuhan of China, which quickly spread around the world. On January 31, 2020 (Beijing time), the World Health Organization (WHO) declared that the outbreak constituted a Public Health Emergency of International Concern (PHEIC). Until 3 years later, on May 5, 2023 (Beijing time), WHO declared the outbreak no longer a PHEIC. According to WHO statistics, as of March 11, 2023, more than 759 million cases of COVID-19 had been diagnosed globally, and nearly 6.9 million COVID-19 deaths had been reported. Pandemics exerted significant pressure on the healthcare systems, resulting in the indirect deaths with excess mortality. A community referred to a social interaction group constituted by interrelated individuals or a number of people within a definite spatial scope (Tonnies, 2002). As the most basic unit of governance and administration in China (A. J. He et al., 2020), the community was the forefront of dealing with outbreaks and emergencies, whose emergency preparedness was directly related to ECEPC. According to the statistics of the Ministry of Civil Affairs of China in the third quarter of 2022, there were 489,000 village committees, 117,000 neighborhood committees, 29,077 community service centers, 502,464 community service stations, and 50,698 community special service agencies, which were grass-roots organizations to respond to disasters such as earthquakes, floods, mudslides, and epidemics, and were directly related to ECEPC, disaster management, and community safety.
During the Covid-19 pandemic, Chinese communities became the basic defense line against public emergencies, organizing a large number of activities such as material assistance, protection propaganda, and life services, and carrying out nucleic acid testing for all personnel, which played a fundamental and critical role in epidemic prevention and control. ECEPC referred to the community’s performance in handling epidemic crisis, preventing the spread of the epidemic, mobilizing residents’ participation, safeguarding residents’ health and safety, the effectiveness and relevance of the interventions, as well as the residents’ satisfaction with the community epidemic prevention and control (Halloran et al., 2002). A further question was what factors influenced ECEPC. Academic researchers had been conducted to explore ECEPC from three aspects:
First, the impact of modern technology on ECEPC. The studies focused on two factors: one was the impact of medical and health technologies, such as vaccine technology on ECEPC; the other one was the impact of modern information technology on ECEPC. Vaccination was a pro-social act that protects not only oneself but also family members, which was an effective way to interrupt the spread of the disease (Böhm & Betsch, 2022). Pan and King (2021) suggested that the elderly had lower immunity at higher risk of infecting with Covid-19 and that vaccination of the elderly could reduce mortality and severe cases. Based on this, Afolabi and Ilesanmi (2021) suggested that the active role of community resources, social organizations, and stakeholders should be fully utilized to improve vaccination rates through community culture and values to dispel doubts and misconceptions about vaccination. For those who were not vaccinated, or communities with low vaccination rates might be a barrier to epidemic preparedness (Dhama et al., 2021). From a moral and ethical point of view, the herd immunity created by vaccination was the public good that benefited all people in the community (Giubilini 2021). McAtee et al. (2022) explored the use of modern smartphone apps for emergency information collection, reporting, and emergency decision-making to improve the efficiency of dealing with outbreaks, but high-quality apps were often monopolized by large companies, making it difficult to be universally accessible. Li et al. (2021) argued that digital technology was widely used in outbreak areas for information collection, surveillance, and contact tracing, and that the use of information technology could significantly moderate the incidence curves.
Second, the impact of residents’ participation on ECEPC. In community epidemic prevention and control, residents were the main body of epidemic prevention and control, changing from “I am asked to prevent the epidemic” to “I want to prevent the epidemic,” instead of just passively preventing the epidemic, fully demonstrating the ownership spirit of community residents (Yang et al., 2021). Anna et al. proposed the concept of “The whole community,” which was an inclusive concept encompassing all community organizations and community members, and a dynamic concept that changed with social, economic, political, and environmental factors (Ramsbottom et al., 2018). The joint efforts of community organizations and community members were essential to improve ECEPC. Joseph et al. (2021) proposed the “academic-community-government” partnership to identify Covid-19-prone populations and distribute needed supplies in high-risk communities. Effective residents’ participation allowed community workers to act as intermediaries and links between government and individuals to access government medical supplies (Lead, 2014). A survey by Zhao et al. (2021) found that 60% of respondents were willing to participate or assist in community epidemic prevention and control, such as distributing medications, vaccinations, but more than 80% of respondents had not received basic healthcare training, so the healthcare training mechanism should be developed for volunteers in order to better respond to public health events. Residents’ participation were also reflected in active compliance with epidemic prevention and control regulations, such as adhering to frequent hand-washing, maintaining body distance, avoiding touching the face, and wearing masks in public places, which could significantly improve ECEPC (Bante et al., 2021).
Third, the impact of community resilience building on ECEPC. Rela et al. (2022) proposed a framework for community resilience based on a survey in Indonesia, including natural capital, human capital, social capital, stakeholder engagement, community action, technology and communication, economic and financial capital, and the ability to resist disruptions and collaborate effectively during the recovery stage in the face of change. The Centers for Disease Control and Prevention in the United States developed the Social Vulnerability Index, which recognized that poverty, lack of transportation, and overcrowded housing might affect the community’s ability to recover from crisis events (Sequist, 2020). Community infrastructure development could improve the community’s ability to handle crises, for example, the community could consult with experts through remote technology, which made the community measures more effective (Hedima & Okoro, 2020). Ghozali and Astuti (2023) examined whether the storage conditions of community epidemic prevention and control medicines as well as disposable medical supplies in a village of West Kalimantan, Indonesia, complied with the health department regulations, and found that the main purpose of the community medicine storage was to maximize profits rather than to improve ECEPC. Aruru et al. (2021) concluded that community pharmacists and pharmacy professionals were at the first line of defense against epidemics, but the limited supply of personal protective equipment and insufficient healthcare were not conducive to the full play of the role of medical personnel, so community pharmacists should be trained and educated professionally so that community pharmacists could become professional and comprehensive personnel to deal with epidemics.
Studies had been conducted to explore ECEPC in terms of epidemic prevention and control technology, residents’ participation and community resilience building, and researchers basically believed that residents were the main body of epidemic prevention and control, information technology was the key, and community resilience building was the foundation, which provided a basic theoretical foundation for subsequent studies. However, the above studies failed to point out which factors were essential to community resilience building. Meanwhile, the existing studies lacked the examination of RERC. Based on this, this study investigated the impact of CEP and RERC on ECEPC.
Theoretical Backgrounds and Hypothesis Development
Community Emergency Preparedness
In recent years, flash floods, mudslides, mass influenza, and terrorist attacks have become increasingly serious threats to the physical and mental health of the population, and both politicians and scientists have begun to focus on public health emergency preparedness. In 2001, the U.S. federal government invested $5 billion to improve CEP. Nelson et al. (2007) defined the concept of CEP as the ability of public health, health care systems as well as communities and individuals to prevent, rapidly respond to and recover from public health emergencies, especially which may overwhelm daily emergency preparedness because of that large scale, long period, or unpredictability. CEP included three dimensions, namely planning ahead, coordinated rapid response capacity, and the establishment of expert term, workforce, and accountability. Subsequently, WHO (2017) developed a strategic framework for emergency preparedness, which pointed out the importance of the elements of governance, capacity, and resources. The strategic elements included plan development, monitoring and early warning information systems, provision of physical and cultural emergency services, social risk communication mechanisms, and financial resources. Tri-Ethnic Center for Prevention Research at Colorado State University, USA, had proposed a community readiness theory on six dimensions: existing efforts, knowledge about the problem, knowledge about alternative methods or policies, leadership, resources, and community climate (Oetting et al., 2001).
Based on the above research, academics developed CEP theory which provided a basic understanding of the community intervention process, where community mobilization must be based on the involvement of multiple systems and the use of resources and strengths within the community (Thurman et al., 2003). The impact of CEP on ECEPC was mainly reflected in three aspects: Firstly, in terms of institutional and organizational development, the establishment of an emergency organization based on emergencies could guarantee community leadership in crisis management, with the community emergency leadership team unifying the command and coordination of all emergency work in the community, making rational, efficient and rapid emergency decisions, and organizing rescue to reduce the damage caused by the crisis. Secondly, in terms of emergency early warning capacity, emergency response plans should be formulated, monitoring and early warning systems established, and emergency warning systems set up. Through information technology, various indicators should be collected and tracked to monitor the probability of disasters occurring in the community, and the scale of disasters should be controlled through early intervention (Asadzadeh et al., 2020). Thirdly, concerning the development of community emergency plans and training of personnel, the formulation of emergency plans was directly related to the speed of disaster response. Incorporating medical staff, rescue personnel, etc. into emergency education and training could not only enhance the rescue capabilities and psychological resilience of emergency personnel, but also ensure the safety of front-line medical staff (Nahidi et al., 2022). Effective CEP offered the possibility of managing disasters and restoring normal life in the community. Based on this, the following hypothesis was proposed.
H1: There was the positive and significant relationship between CEP and ECEPC.
Resident Emergency Response Capacity
In times of disaster crisis, individuals usually experienced negative emotions such as anxiety, insomnia, depression, insecurity, anger, and other stress syndromes, resulting in physical vulnerability, cognitive vulnerability, and psychological vulnerability (Sheek-Hussein et al., 2021), reducing the individual’s ability to handle the crisis. Therefore, RERC became an essential element in coping with disasters and viruses. Crises and disasters affected individuals differently, depending on individuals’ preparedness for the emergency and their ability to cope with it. Factors such as age, gender, education, health disparities, and ethnicity had been proposed as key factors in handling the disasters (Amaratunga & O’Sullivan, 2006). At the same time, resident emergency risk awareness, emergency mutual-aid capacity and psychological resilience became important components of RERC. According to the “cognitive-behavioral” analysis framework, residents with a high level of risk awareness could reduce their fear, increase their sense of efficacy in emergency response and build their belief in overcoming disasters (Adu-Gyamfi & Shaw, 2022). Emergency mutual-aid capacity emphasized the importance of building a community of life among family members and residents to help each other cope with disasters, for example by participating in voluntary activities, donating goods, and helping vulnerable people to escape from disaster sites (Guo et al., 2021). Resilience was a particularly important issue in risk societies and was described as the ability to adapt to and maintain psychological equilibrium in times of high stress. Psychological resilience was described as a way to reduce or prevent disaster stress such as fear and anxiety from leading to more serious psychological consequences (Austin & Gregory, 2021), and good psychological resilience helped to improve ECEPC. Based on this, the following hypotheses were proposed.
H2a: There was the positive and significant relationship between emergency risk awareness and ECEPC;
H2b: There was the positive and significant relationship between emergency mutual-aid capacity and ECEPC;
H2c: There was the positive and significant relationship between psychological resilience and ECEPC.
Figure 1 shows the conceptual model of the entire research hypothesis.

conceptual model.
Materials and Methods
Data Sources
The data used came from a sample survey project conducted from January to June in 2022. We consulted authoritative experts in this field, referred to the research of Shen and Shen (2021) and considered the feasibility of data collection to determine the sample size. To test the validity of the questionnaire, the research team conducted a 2-week trial survey in the cities of Xuzhou, Wuhan, and Chengdu. The formal survey was conducted by random sampling method, and 20 provinces in Chinese mainland were selected from 34 provincial administrative units in China. First, 7 cities were selected from each province (20 provinces × 7 cities), and then 1 community was selected from each city (20 provinces × 7 cities × 1 community); second, 15 residents were randomly selected from each community to distribute questionnaires for the survey, with a sample size of 2,100 (20 provinces × 7 cities × 1 community × 15 residents). Before the questionnaire survey, the researchers informed the respondents of the purpose, content, and significance of this survey, and only started the survey after obtaining the consent of the respondents. Respondents can withdraw from the survey at any time, this survey caused no harm to the respondents. It took about 20 min to complete a questionnaire, and a small gift was given to the respondents as compensation after they finished it. Due to the large regional differences in China, on the basis of consultation with experts, another 10 typical communities were selected in the East, Middle, and West areas of Chinese mainland to conduct the online survey, with a sample size of 150. The online survey was conducted by the researchers through phone calls and emails, and respondents who completed the online survey received five RMB in compensation. As a result, a total of 2,250 questionnaires were distributed, and after checking the authenticity and reliability, 2,112 questionnaires were effectively recovered after excluding invalid questionnaires, and the effective recovery rate of the questionnaires was 93.86%, which met the requirement of questionnaire validity rate of 90%. The researchers participating in this survey were mainly postgraduate students and grass-roots cadres from the surveyed areas. The professional interview training was provided to all the researchers involved to enhance their professional research capabilities.
Nine variables of CEP were included in the analysis, and the results showed that the KMO value was 0.918, the p-value of Bartlett’s Test of Sphericity was less than 0.000, and one factor was extracted, with a Total Variance Explained of 59.526%. Three variables of RERC were included in the analysis, and the results revealed that the KMO value was 0.719, the p-value of Bartlett’s Test of Sphericity was less than 0.000, and one factor was extracted, with a Total Variance Explained of 73.974%. This indicated that the questionnaire had good validity. The Cronbach’s Alpha of the independent variable was detected. The Cronbach’s Alpha of the nine variables of CEP was 0.914, and the Cronbach’s Alpha of the three variables of RERC was 0.824, both of which were greater than 0.8, indicating that the questionnaire had a certain degree of reliability.
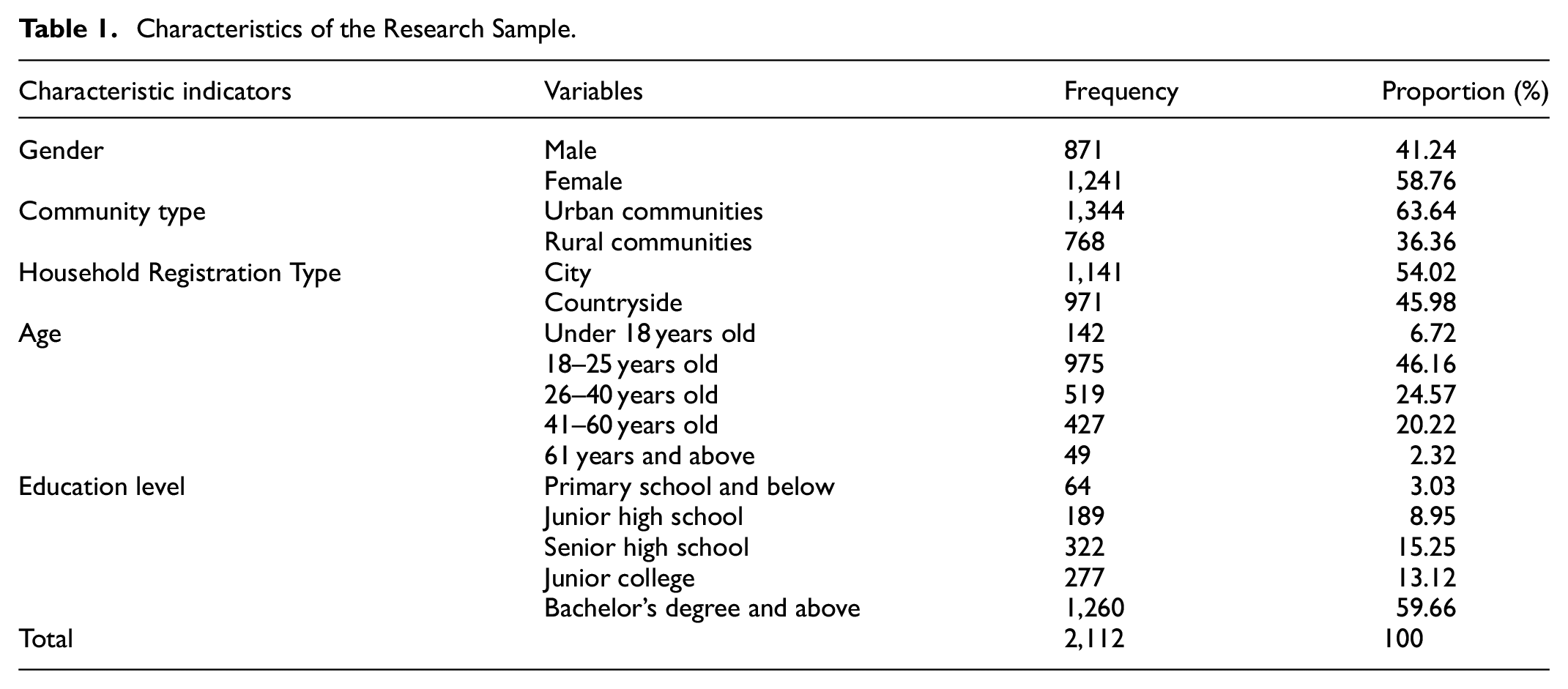
The characteristics of the sample of 2,112 were as follows, as shown in Table 1: in terms of gender, there were 871 male respondents (41.24%) and 1,241 female respondents (58.76%); in terms of community type, there were 1,344 respondents in urban communities (63.64%) and 768 respondents in rural communities (36.36%); in terms of household registration, there were 1,141 respondents in cities (54.02%) and 971 respondents in countrysides (45.98%); in terms of age, 975 respondents (46.16%) were aged 18 to 25, followed by 519 respondents (24.57%) aged 26 to 40 and 427 (20.22%) aged 41 to 60; in terms of education level, the percentages of respondents with education level of primary school and below, junior high school, senior high school, junior college, bachelor’s degree and above were respectively 3.03%, 8.95%, 15.25%, 13.12%, and 59.66%. Overall, it seemed that the sample of respondents was in line with objective reality and could be statistically analyzed.
Characteristics of the Research Sample.
Measurements
Effectiveness of Community Epidemic Prevention and Control
The dependent variable in this paper was ECEPC, as shown in Table 2, which was measured from the subjective perspective of the residents, with the question “How effective do you think ECEPC is?” These answers were set on a 5-point Likert scale of “very poor, fairly poor, fair, fairly good, very good” with assigned values from 1 to 5.
Variable Definitions and Assignments.

Community Emergency Preparedness
CEP was the relocation of crisis management, and the evaluation system of CEP was proposed. In 2011, the Centers for Disease Control and Prevention (CDC, 2011) developed the Public Health Emergency Preparedness Capability: National Standards for State and Local Readiness, which contained 15 capability criteria such as community recovery, emergency operations coordination, emergency public information and alerting, information sharing, and medical response deployment and management. This survey learned from CDC’s capability standards and WHO’s strategic framework for emergency preparedness to measure nine aspects, namely emergency response system development, emergency response system drills, emergency response team building, emergency response team training, allocation of emergency responsibilities, emergency information collection, emergency information monitoring, emergency information early-warning, and emergency resource reserve, with the answers set on a 5-point Likert scale of “very poor, fairly poor, fair, fairly good, very good,” and assigned values from 1 to 5.
Resident Emergency Response Capacity
RERC directly determined residents’ ability to handle crises, and this survey examined three aspects: emergency risk awareness, emergency mutual-aid capacity, and psychological resilience. Emergency risk awareness examined the residents’ ability to perceive crises. Beck (2004) proposed the risk society theory, which considered risk awareness as the anticipation and avoidance of crises. Emergency mutual-aid capacity examined the ability of residents to help each other, and was important for the living community and life community. Psychological resilience examined residents’ ability to recover from setbacks, which helped to build psychological capital. Answers were set on a 5-point Likert scale of very poor, fairly poor, fair, fairly good and very good, and assigned values from 1 to 5.
Control Variables
Drawing on the results of previous studies, some of the control variables included were gender, age, education level, community type, and household registration type (Wang et al., 2020), as set out in Table 2.
Analytical Methods
In this study, the explanatory variable was ECEPC, which was a five-category ordered variable. The ordered logistic regression model was more suitable to analyze it. However, CEP and RERC were both five-category variables, and the ordered logistic regression model required to take a certain value of the independent variable as the reference value. The output results were rather cumbersome, inconvenient to present and interpret. Compared with the ordered logistic regression model, the advantage of the optimal scaling regression model was that it could demonstrate the influencing degree of the independent variables on the dependent variable through diagrams, and directly reveal the most critical influencing factors. Therefore, this study chose to use the optimal scaling regression model in SPSS24.0 (IBM, Almond, NY, USA) software. The basic idea of this model was to analyze the changes in the strength of the influence of each category of the variables on the dependent variable. Under the premise of ensuring that the relationship between each independent variable was linear, it found the best quantified score for the original categorical variable through repeated iterations, which was used to replace the original variable for subsequent analysis, and then fit the best regression equation (Zhang & Zhong, 2013).
The optimal scaling regression model was a statistical regression model for regression analysis of ordered multi-categorical variables and unordered multi-categorical variables, and the basic model was as follows.
The regression of CEP and ECEPC was used as an example to illustrate this. “γ” was the standardized ECEPC, with “
Results
Describe Statistical Analysis
When examining the overall ECEPC, the percentages of respondents who answered very poor, fairly poor, fair, fairly good, and very good were 1.42%, 2.79%, 21.31%, 50.09%, and 24.38% respectively. It showed that over 50% of the respondents thought that ECEPC was fairly good, adding up the percentage of respondents who answered very good to 74.47%. Thus, overall, the majority of respondents considered ECEPC to be effective.
CEP was a prerequisite for effective crisis response, and the development of an emergency system was the basis for CEP. A complete, systematic, clear, and formal emergency management system should be formed through emergency response system development, which provided detailed provisions on the functions, guidelines, objectives, scope, structure, and processes of community emergency management. The descriptive statistics found that 45.69% of respondents thought that the emergency response system development was fairly good and 26.09% thought very good. The community emergency response system also required drills in order to adjust, modify, and improve the emergency response system. 44.70% of the respondents thought that the emergency response system drills were fairly good, while 28.65% thought it was very good. In terms of emergency response team building, 45.08% of the communities were fairly good, while 28.69% were very good. Meanwhile, in terms of emergency response team training, 43.32% of communities were fairly good and 34.85% were very good. Clear responsibility allocation between the community emergency department and its members was essential for orderly and effective response to emergencies. 45.03% of communities had a fairly good allocation of responsibilities and another 26.28% had a very good allocation of responsibilities. When responding to public crises, the collection, monitoring and early warning of emergency information could achieve early detection, reporting and disposal of epidemic prevention and control, and achieve technological empowerment. Statistics found that the percentage of fairly good in terms of emergency information collection, monitoring, and early-warning was 43.80%, 44.51%, and 43.89% respectively, while the percentage of very good was 34.19%, 26.28%, and 22.73% in that order. Finally, in terms of emergency resource reserve, 43.42% of the respondents answered fairly good and 23.30% answered very good. Overall, it appeared that CEP were relatively impressive.
Table 3 reflected the basic situation of RERC. In terms of emergency risk awareness, 47.02% of the respondents had a fairly good risk awareness and another 27.27% had a very good emergency risk awareness. In terms of emergency mutual-aid capacity, 46.54% of the respondents answered fairly good and 27.04% answered very good. In terms of psychological resilience, 45.12% of the respondents answered fairly good and 25.52% answered very good. The high RERC as responded by the sample was related to two factors: firstly, the respondents in this survey had a relatively high education level, which gave them an advantage in terms of human capital. They had a good knowledge of emergency response, and the higher educational level also shaped individuals’ reversible psychological resilience; secondly, the government’s role of propaganda and science popularization. Since the outbreak of the COVID-19 pandemic, the Chinese government had used the internet, television, and other new medias to promote emergency management knowledge and raised the public’s awareness of emergency risks and crises.
Descriptive Analysis of RERC (Unit: Piece, %).

Regression Analysis of ECEPC
Table 4 presented the regression models for the influence of CEP and RERC on ECEPC. A stepwise regression was used in the study to include control variables in the model to obtain Model 1, three variables of RERC in the regression model to obtain Model 2, and nine variables of CEP to obtain Model 3. The tolerance values of all independent variables in the three models before and after the transformation were greater than 0.1, indicating that there was no multicollinearity in the independent variables. The F-values of the three regression models were 6.555, 34.053, and 22.510 respectively, and the ANOVA results of all three models were less than 0.000, which met the significance requirement of 0.05, indicating that the model fitting results were valid. The R-square of the model increased from 0.033 to 0.393, and the adjusted R-square increased from 0.028 to 0.375, indicating that the fitting effect of the model was gradually improving along with the inclusion of RERC and CEP. Overall, it showed that the model fitting results could be analyzed.
Regression Results for ECEPC.

Note. Pre- and post-transformation tolerances of the independent variables for the three models were not presented due to space limitations of the table.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
In model 1, gender, age, education level, and household registration type had a significant effect on ECEPC, while community type did not have a significant effect. In Model 2, gender, age, education level, and RERC all had significant effects on ECEPC, while community type and household registration type did not have significant effects, indicating that the effect of household registration type was unstable as independent variables were incorporated into the model. In Model 3, community type and household registration type still did not make significant influences. A possible explanation was that the new type of urbanization promoted by China accelerated the flow of elements between urban and rural areas, and the medical services reaching rural areas improved the backward medical conditions in rural areas. The establishment of a unified resident identity system mitigated the gap of the household registration system, and the concept of life first under epidemic prevention and control suppressed the dividing effects of household registration. Gender, age, education level, RERC, and CEP made significant influences. Model 3 was the final result of the regression of all variables, and the specific analysis was as follows.
Among the control variables, gender made a significant impact on ECEPC. The evaluation of ECEPC by females was 0.042 higher than that by males. Based on women’s gender characteristics such as gentleness, sensitivity, and patience, women became an important force in community self-management, self-service, and self-education. As a result, the majority of grass-roots community members were female (Song, 2018), and even 80% of community cadres in some areas were women, who were directly responsible for community epidemic prevention and control, and had some decision-making power regarding grass-roots crisis events. The sensitivity of female community cadres to crises, their personal crisis management skills, and their ability to work in a comprehensive manner directly affected ECEPC. At the same time, health workers in community health service stations were also predominantly female. According to statistics, 90% of health care workers in Hubei province were women (Wenham et al., 2020), which meant that women were at the front line of epidemic prevention and control, directly contacting with infected people or the virus, and tended to be a vulnerable population. However, grass-roots community health workers were less educated with a lack of professional knowledge and skills, thus failing to effectively meet the needs of community epidemic prevention and control.
Oktari et al.’s (2021) study showed that women’s vulnerability to epidemics or disaster events was influenced by unequal gender relations in traditional patriarchal systems, yet women were actually the main force in community epidemic prevention and control, shaping the issue of gender mainstreaming. So, gender issues cannot be ignored before, during, and after community epidemic prevention and control.
Age had a significant effect on ECEPC. For each unit increase in age, the evaluation of ECEPC increased by 0.041. From a biological point of view, the elder an individual was, especially the elderly, the lower the body’s immunity. The elderly often suffered from underlying and chronic diseases, making them a vulnerable group in epidemic prevention and control, and the elderly with COVID-19 often developed into heavy infections, increasing the risk of death (Grolli et al., 2021). Therefore, certain epidemic prevention measures, such as social isolation, trip tracking, health statistics, and information referral, were beneficial for the elderly, whose evaluation of ECEPC was enhanced. Conversely, there was a discrepancy between the evaluation of epidemic prevention and control measures by some young people and the elderly. Young people were the main source of economic income for their families and were responsible for their family’s living expenses, so when measures such as social isolation were taken, it meant that the family’s income was cut off and they were unable to maintain a normal life, thus leading to emotional resistance. As a result, young people did not have a very high opinion of ECEPC.
Education level made a significant effect on ECEPC, with an effect of 0.056. For each unit increase in education level, the evaluation of ECEPC increased by 0.056. The higher the level of education of the population, the higher the level of awareness of COVID-19, and its transmissibility, hazards, lethality, which created a certain degree of crisis awareness and led the population to cooperate with the community’s epidemic prevention and control policies. At the same time, a higher level of education indicated a higher level of human capital, which meant they might have a stable job and source of economic income without worrying about the livelihood of the family. However, for people with a lower level of education, on the one hand, they did not have sufficient knowledge of COVID-19 and were unable to take right preventive measures because of the lower understanding degree of community epidemic prevention and control policies, thus leading to the lower participation degree; on the other hand, people with a low level of education were often at the bottom of the society ladder and did not have a stable source of income. Especially community epidemic prevention and control measures sometimes caused a family economic crisis and survival crisis. Therefore, the lower the level of education, the lower the evaluation of ECEPC.
In both Model 2 and Model 3, all three variables of RERC had a positive and significant effect on ECEPC. In Model 3, there was a positive and significant effect between emergency risk awareness and ECEPC. For each unit increase in resident emergency risk awareness, the evaluation of ECEPC increased by 0.061, proving hypothesis H2a. Residents with higher risk awareness could increase the awareness level of COVID-19, understand the severity and danger of the epidemic, improve risk warning awareness, increase protection awareness, and consciously take epidemic prevention measures, such as washing hands, ventilation, wearing masks, and keeping social distance (Lu et al., 2021). At the same time, resident emergency risk awareness influenced individuals’ attitudes toward epidemic prevention and control and reduced unnecessary panic. Resident emergency risk awareness was a flexible supplement to the rigid epidemic prevention policies of the grass-roots government, and residents would also be more cooperative with community epidemic prevention and control policies, such as timely reporting of individuals’ travel history and health conditions. In other words, if community epidemic prevention and control policies could gain residents’ acceptance, the residents would naturally rate ECEPC higher.
There was a positive and significant effect between emergency mutual-aid capacity and ECEPC. For each unit increase in the emergency mutual-aid capacity of the residents, the evaluation of ECEPC increased by 0.048, proving the hypothesis H2b. Traditional rural communities were communities based on blood and local ties, and as Tonnies (2002) says, members of the community helped each other, relied on each other, and were a community of interest and fate. The good emergency mutual-aid atmosphere in a community could increase the overall emergency knowledge of the population and reduced the adverse effects of disasters in general. When a community was at risk of an epidemic, the people’s ability to cope with the epidemic was enhanced through knowledge dissemination, information sharing, and resource exchange, which could also shorten the disaster recovery period. At the same time, people with a higher capacity for emergency mutual-aid could reduce the pressure and burden of community emergency response, providing a buffer period for communities to formulate emergency plans, form emergency organizations, and allocate emergency resources. Thus, the higher emergency mutual-aid capacity could improve ECEPC.
Psychological resilience had a significant positive effect on ECEPC. For each unit increase in psychological resilience, the evaluation of ECEPC increased by 0.072, proving the hypothesis H2c. Psychological resilience included individual material stocks, disaster information, sense of community belonging, social capital, social support (Sherrieb et al., 2010), and individual capacity (Garmezy, 1991). People with strong resilience were able to neutralize or mitigate the negative effects of a crisis, avoiding panic and even triggering a herd effect. Individual resilience included individual absorptive capacity, adaptive capacity, and resilience (Béné et al., 2012). Absorptive capacity referred to an individual’s ability to absorb the impact of the external crisis environment; adaptive capacity referred to an individual’s ability to adapt to the new environment that emerged after a crisis and to maintain good individual psychological capacity so that the individual’s physiology and psychology were better suited to the changes caused by the environment; resilience referred to an individual’s ability to bounce back from the crisis, to overcome individual vulnerability and return to a normal level. Thus, a high level of psychological resilience could lead to self-adjustment to a new environment and was compatible with community epidemic prevention and control policies, which combined to create a synergistic effect in response to crises and thus improve ECEPC.
In Model 3, there were nine variables for CEP, all of which had a significant effect on ECEPC, proving hypothesis H1. First, for each unit increase in emergency response system development, the evaluation of ECEPC increased by 0.099. For each unit increase in emergency response system drills, the evaluation of ECEPC increased by 0.135. Emergency response system development was equivalent to an emergency plan for crisis management, which provided detailed provisions for the definition of crisis, organizational leadership, allocation of human resources, division of labor among departments, etc. A qualified emergency system included people, money, material, and organization, and the textual content was operational and feasible, which could overcome the fragmentation and suddenness of the crisis. However, emergency response system development was only a text-based system information, its practicality and effectiveness required to be tested through emergency response system drills. Emergency response system drills could test the distance between the system and practice, identify the system’s problems, and make changes and adjustments to the system based on the results of the drills. At the same time, training community members through emergency response system drills would help community members to clarify the content, division of responsibilities and operational procedures of emergency response, and improve their motivation and flexibility in emergency management (Richmond et al., 2021), which could make good effects on the epidemic prevention and control.
Second, emergency response team building had a significant impact on ECEPC. For each unit increase in emergency response team building, the evaluation of ECEPC increased by 0.069. From the perspective of organization management, the establishment of a temporary emergency response team in the face of a crisis was equivalent to the leading team of a crisis, which could integrate resources, coordinate the human and material resources of various departments, and realize the unified action of community members (Leach et al., 2022). At the same time, the emergency response team played the role of “information bridge,” and traditional information transfer required layers of transmission, through multiple levels and departments. The emergency response team could directly achieve information aggregation, reduce the cost of information transfer, improve the efficiency of information transfer, and facilitate community leaders to quickly formulate action plans and take action. In addition, the emergency response team was equivalent to a front-line command for crisis management, which enhanced the speed of community response and enabled a rapid response, thus improving the efficiency of crisis management and minimizing disasters. In epidemic prevention and control, communities often set up epidemic prevention and control command teams to handle epidemic crises, which helped to improve ECEPC.
Third, emergency response team training made a significant effect on ECEPC. For each unit increase in emergency response team training, the evaluation of ECEPC increased by 0.068. According to the competency model, emergency response team training was competency- and professional-oriented training that enhanced members’ professional knowledge and skills, familiarity with emergency response steps, and adaptability (Gallardo et al., 2015). Emergency response team training was often delivered through lectures and scene simulations teaching, which promoted familiarity, communication and collaboration between team members and shaped an effective emergency response team. The training covered contents such as rescue deployment, risk prevention and control, rescue response and procedures, mobilization of rescue resources, and field-based life saving operations to improve the operational capability of the emergency response team. A trained emergency response team would be able to perform in a more standardized and institutionalized way in handling crises, improving the order and stability of crisis management, which in turn would enhance ECEPC.
Fourth, allocation of emergency response responsibility made a significant positive effect on ECEPC. For each unit increase in allocation of emergency response responsibilities, the evaluation of ECEPC increased by 0.116. In communities with unorganized responsibility distribution, there was a clear tendency for emergency response responsibility to be fragmented, with unclear distribution of responsibility between departments and members, leading to the phenomenon of shirking and bickering over the responsibility for epidemic prevention and control, and the spread of hazards caused by crisis events. An orderly and clear responsibility allocation plan could guide the behavior of departments and members, providing a basis for emergency actions and forming a responsibility matrix. According to the role-playing theory, each member was aware of their role and position in emergency handling and assumed corresponding responsibilities based on their role, such as commanding, coordinating, supervising, and executing. Meanwhile, the allocation of responsibilities could promote the standardization and normalization of crisis management, enhancing the degree of close cooperation among members. Additionally, the allocation of emergency responsibilities was conducive to supervision. When problems arose in crisis management, responsibilities could be quickly traced and claimed based on the allocation list.
Fifth, emergency information collection, emergency information monitoring and emergency information early-warning all made significant positive effects on ECEPC. For each unit increase in emergency information collection, emergency information monitoring, and emergency information early-warning, the evaluation of ECEPC increased by 0.112, 0.060, and 0.077 respectively. There was a procedural and developmental relationship among emergency information collection, emergency information monitoring, and emergency information early-warning: emergency information collection referred to gathering information about the situation, environment, and emergency knowledge around a specific information carrier, and forming comprehensive, identifiable, professional, and precise information after processing the validity of the information; emergency information monitoring was based on information collection, and involved marking and tracking the collected information for supervision, achieving dynamic supervision of information, and enabling early detection, reporting, and handling crises; emergency information early-warning was a mechanism and platform established on the basis of information collection and monitoring, which could transform the statistic analysis of data information into visual information resources, and establish the early-warning information indicators and evaluation system. The construction of an information early-warning platform could provide support for epidemic prevention and control.
Sixth, emergency resource reserve made a positive and significant effect on ECEPC. For each unit increase in emergency resource reserve, the evaluation of ECEPC increased by 0.084. Emergency resources were the material basis for community response to emergencies. Communities were unable to respond effectively to disasters with a lack of resources. Emergency resources included rescue equipment, supplies, vehicles, medical and health care, funds, etc. Due to the uncertainty of crisis events, it was also necessary to regularly update the physical emergency resources, and regularly take inventory to eliminate obsolete resources and replenish new ones. For the community, emergency resource reserve should focus on the adequacy, diversity and abundance of resources, and the fairness, openness and effectiveness of resources distribution. In a crisis situation, communities need to provide people with the basic necessities of life to meet their basic needs, which could enhance the legitimacy of the community. At the same time, crisis events usually caused fear, panic, anxiety, and nervousness. Community emergency psychologists should be taken into account to provide people with mental health counseling services, which could effectively improve people’s psychological resilience and thus enhance ECEPC.
The importance index was calculated based on the standardized coefficient and correlation coefficient to determine the percentage of the significance of each explanatory variable in the model. The larger the value, the more crucial the variable was in predicting the explained variable. Figure 2 presented the ranking of the significance of each variable in Model 3 for CEP and RERC. Among the 12 variables, 8 of CEP variables were ranked at the top, with emergency response system drills topping the list and emergency information monitoring coming last. The three variables of RERC were ranked from 9th to 11th. On the whole, the significance of CEP was higher than that of RERC.

Importance analysis of factors influencing ECEPC.
Discussion
In order to investigate the influence of CEP and RERC on ECEPC, the relationship among them was explored with the optimal scaling regression model as an analytical tool. The results of the stepwise regression model showed that CEP and RERC had a positive and significant effect on ECEPC, which proved the hypotheses H1, H2a, H2b, and H2c.The findings revealed as follows:
First, while previous studies suggested that residents with insufficient emergency response capacity were unable to respond effectively to crisis events, this study found that, overall, residents appeared to have high emergency response capacity. Xing and Zhang (2021) study of the Covid-19 in Wuhan found that residents had insufficient emergency response knowledge and low awareness of the crisis. Liu et al. (2021) concluded that people lacked awareness of the ways in which the virus was transmitted in the early stages of the outbreak and were unable to access effective information and acquire emergency response skills, leading to inadequate personal preparedness. China and Japan belonged to the same East Asian culture, but the Japanese culture emphasized keeping a social distance, which did not include shaking hands, hugging, or kissing; this culture of social etiquette helped to prevent the spread of the virus, but did not equate to a higher level of emergency awareness among the population (Iwasaki & Grubaugh, 2020). Qian and Hanser (2021) found that residents had low awareness of emergency response, insufficient self-rescue and mutual rescue capabilities, and low participation in community emergency development. Residents’ inadequate emergency response capacity led to the amplification of the impact of a crisis or disaster and increased losses. However, this study found that, unlike previous studies, RERC was not as low as had been suggested. Firstly, the Chinese government attached great importance to emergency education and conducted emergency campaigns in the community to enhance residents’ emergency awareness. The role of communities, neighborhood committees, and the general public had been brought into play, and various community resources and forces had been pooled to promote emergency knowledge, emergency rescue, and emergency drills in the community, so that every community member had a greater awareness of emergency response and had some basic emergency knowledge and ability (Ma et al., 2021). Secondly, grass-roots communities had the ability to learn from disasters, draw from crisis management experience, invite experts in emergency management to disseminate knowledge about emergencies, print emergency publicity manuals and make them available to residents so that they were familiar with the use of emergency equipment in the community, and constantly improved their awareness and ability to help themselves and each other. Finally, the education level of the residents affected their emergency response capabilities, with higher education levels increasing their emergency response awareness (S. He et al., 2021). This was consistent with the higher education levels of the sample surveyed in this study. The community emergency culture also influenced RERC which was reflected in their awareness of crisis mitigation, knowledge of emergency avoidance, and psychological tolerance of disasters.
Secondly, this study found that CEP was more important than RERC in terms of its impact on ECEPC. A further question was why CEP was more important than RERC. On the one hand, there were differences in the emergency response capacity and levels between communities and residents (Feng & Cui, 2021), and data from a national survey by Qiu et al. (2020) showed that after the outbreak of Covid-19 in Wuhan, individual residents experienced a variety of psychological problems such as panic attacks, anxiety, and depression, which severely affected individuals’ resilience. Communities as organizations were more resilient than individuals, and they were able to handle crises that individuals could not cope with and overcome their vulnerability. On the other hand, communities as government organizations had an advantage over individuals in terms of handling disasters. Mao (2021) argued that communities were at the end of the hierarchy of state institutions, and that the state capacity shaped by the state system transmitted some of its capacity to communities, forming community crisis management capacity, including information capacity, decision-making and implementation capacity, coercive capacity, and mobilization and cooperation capacity.
Third, among CEP, emergency response system drills ranked first in importance and had the greatest impact on ECEPC. Halloran et al. (2002) argued that vaccination was an effective measure to improve community preparedness, and that vaccines could increase the potential of communities to prevent the epidemic, called epidemic prevention potential. Kuo et al. (2021) discussed ECEPC from the perspective of planned behavior theory, and argued that the establishment of community management structures and the adoption of necessary vaccination measures were key to improving ECEPC. Chen et al. (2021) discussed this from a medical perspective, arguing that stockpiling sufficient and effective antibiotics was essential to respond to the outbreak of epidemics. From an emergency management perspective, this study found that emergency response system drills played an important role in ECEPC.
Firstly, emergency response system drills could enhance the community’s emergency response capabilities. By simulating real or hypothetical emergency scenarios, participants could familiarize themselves with emergency procedures and master emergency skills without actual losses. They could also identify and solve problems in practice. Emergency response system drills tested the completeness, applicability, and flexibility of emergency systems or plans. During the drills, the responsibilities of each member was clarified, and the behaviors of various entities were coordinated, thereby improving the professionalism, accuracy, and completeness of the community’s emergency response teams. This practical drill approach not only helped to enhance individual emergency response capabilities, but also promoted teamwork, enhanced the coordination and efficiency of the overall emergency response, and improved the community’s response speed to crises, minimizing the adverse effects of crises to the greatest extent.
Secondly, emergency response system drills could optimize the allocation of community’s emergency resources. Emergency response system drills facilitated the optimization of emergency resource allocation. During the drills, it could be distinctly discerned which resources were requisite, which were superfluous, and which needed urgent replenishment. This assisted decision-makers in allocating emergency resources rationally based on actual demands and enhancing the efficiency of resource utilization. Meantime, through drills, the reliability and effectiveness of emergency resources could be verified to ensure that the necessary resources were promptly and accurately mobilized at a critical time, providing robust support for emergency responses.
Thirdly, emergency response system drills could fortify the public safety consciousness within the community. By engaging in the drills, the public could have a more intuitive understanding of the hazards of emergencies and coping approaches, thereby enhancing their awareness of self-protection and their abilities to save themselves and others. The publicity and education segments during the drill process could also impart safety knowledge to the public, exerting an educational effect on both individual residents and community workers, and escalating their emergency crisis consciousness. Moreover, the emergency response capabilities of individuals or the community could be assessed during the drills, thereby providing a reference basis for subsequent emergency preparedness endeavors (Biddinger et al., 2010). Emergency system drills could enhance the psychological resilience of individuals and the community, contributing to alleviating the fear, anxiety, and unease that individuals might encounter in times of crisis (Gündoğan & Serin, 2022). Such an escalation of safety consciousness was conducive to reducing the occurrence probability of emergencies, minimizing disaster losses, and offering a potent guarantee for the harmony and stability of society.
Conclusions
Based on 2,112 survey data, this study used an optimal scaling regression model to explore the impact of CEP and RERC on ECEPC. The results of the study showed that: firstly, 74.47% of the respondents thought ECEPC relatively good, and that emergency risk awareness, emergency mutual-aid capacity, and psychological resilience were effective, which was closely related to the government’s crisis publicity and education efforts; secondly, both CEP and RERC had the significant impact on ECEPC, and CEP was more important than RERC. Communities as emergency response organizations were more capable of withstanding risks and crises than the individual, overcoming the vulnerability of the individual in the face of crises, and enhancing the individual’s emergency response capacity; thirdly, emergency response system drills played a unique role in ECEPC. From the perspective of crisis management, emergency system drills could test the completeness of the emergency system, identify problems in a targeted manner for modification and adjustment, and also enhance the emergency awareness of the community and residents during the drills. Based on these findings, the following recommendations were made:
Policy Implications
First, the careful planning and preparation phase of emergency response system drills. In order to ensure the relevance, practicality and safety of the drills, community managers needed to conduct a risk assessment of the various types of emergencies that the community might face, identify high-risk areas, and potential danger, which was the basis for designing drill scenarios. The scenarios should be designed to be close to reality, covering various types of disasters such as fires, earthquakes, floods, epidemics, etc. The time, location, participants, and role assignments of the drills should be clearly defined to ensure that each participant was clear about his or her responsibilities and tasks. Sufficient emergency supplies and equipment, such as fire-fighting equipment, first-aid kits, and communication devices, should be prepared, inspected and maintained to ensure their normal use during the drills. Necessary training should be provided to the participants to familiarize themselves with the emergency procedures, master the emergency skills, and improve the efficiency and accuracy of the emergency response.
Second, the orderly implementation and flexible adjustment phase of emergency response system drills. The participants should strictly adhere to the drill regulations and operate in accordance with the preset emergency handling procedures, maintaining composure, and responding calmly, thereby demonstrating excellent emergency skills and teamwork spirit. In the face of unexpected circumstances or incidents during the drills, such as equipment malfunction, personnel injury, epidemic spread, virus infection, etc., adjustments needed to be made flexibly based on the actual situations, or the alternate plans should be initiated immediately to promptly adjust the drill plan and ensure that the drills were not affected. It was necessary to pay close attention to the security situation during the drills and take necessary measures to protect the safety of the participants and avoid accidents. In terms of the frequency of drills, the community could appropriately increase the number of drills, which not only cultivated the crisis awareness of residents, but also enhanced the crisis management ability of community workers and increased their professionalism.
Third, the comprehensive assessment and continuous improvement phase of the emergency response system drills. A comprehensive assessment of the drlls should be carried out, including the performance of the participants, the implementation of the emergency response process, and the preparation of materials and equipment. Through the assessment, problems and deficiencies in the drills could be found, such as the emergency response speed was not fast enough and the emergency disposal process was not smooth enough. Improvement plans should be formulated based on the assessment results, emergency plans should be revised, and improvement measures and those responsible should be clarified to ensure that problems could be solved in a timely manner. Through continuous improvement and constant optimization, the level of community epidemic prevention and control would be continuously enhanced, providing a more solid guarantee for the safety of residents’ lives and properties.
Limitations and Future Research Directions
This study had three limitations. Firstly, this study lacked sufficient theoretical support and had deficiencies in the theoretical depth. For instance, it inadequately explored the theoretical sources of ECEPC, failed to provide a thorough analysis of its constituent elements, and offered insufficient discussion on the theoretical origins of CEP and RERC. Secondly, the research data used in this study was from a one-off survey, lacking continuous survey data as support. Although the samples with missing data were excluded, it might still cause other bias. Thirdly, ECEPC was a comprehensive outcome of various influences. This study only explored two variables: CEP and RERC. There was also a lack of an examination of the relationship between them. More factors should be incorporated to future researches.
Footnotes
Acknowledgements
The authors are highly grateful to all the associated personnel that helps in the completion of this study.
Ethical Considerations
The study was conducted in strict compliance with Sage’s Guidelines for studies involving humans to ensure that the research process was legal, transparent, and the rights and interests of participants were protected. All the respondents of this questionnaire survey were adults. We provided the participants with an informed consent form, which was concise and clear in content, allowing the respondents to fully understand the research content and voluntarily participate in the research. Participants can refuse and withdraw from the interview at any time, fully respecting the interviewee’s wishes. The data of the respondents is anonymous. All identifiable information is deleted from the dataset, accessible only to team members, and encrypted to minimize the risks. The researchers provided the respondents with contact information in case they had any further questions or concerns. This study explores the influencing factors of the Effectiveness of Community Epidemic Prevention and Control in developing countries under the abnormal circumstances, providing empirical evidence for taking appropriate measures to improve the effectiveness of community epidemic prevention. It is conducive to ensuring the life, health, and safety of the people and further providing a safe and comfortable social environment. Participants can receive small gifts as compensation. Their interview information is completely anonymous and strictly confidential. The potential benefits are significantly greater than the potential harm risks to the participants. This study received ethical approval from the Ethics Committee of Xuzhou Medical University on January 11, 2022 (Approval Number: XZHMU-2022007).
Consent to Participate
We provided the participants with an informed consent form, which was concise and clear in content, allowing the respondents to fully understand the research content and voluntarily participate in the research.
Authors Contributions
All authors were involved in research design, implementation of the study, data gathering, data analysis, and writing of the manuscript. All authors approve submission of the manuscript for publication consideration. All authors read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research grants from the General Project of Philosophy and Social Science Research in Higher Education Institutions of Jiangsu Province (2022) (Grant numbers 2022SJYB1176), and the research project of Humanities and Social Sciences of Guizhou University in 2025: “Research on the Coupling Mechanism between Household Demand and National Food Security” (Grant numbers 600547253301).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon request.