
Abstract
As a reaction to late-life events (e.g., bereavement, retirement) and feelings of meaninglessness and purposelessness, one-third of older problem drinkers only start to consume alcohol excessively later in life. Referred to as late-onset, limited research has been undertaken on this distinct cohort of older problem drinkers from the perspective of recovery generally, and more specifically, in the context of recovery capital (RC). Framed within Viktor Frankl’s theory of meaning (logotherapy), semi-structured interviews were undertaken on nine early- and nine late-onset problem drinkers (≥50-years old), now in recovery; early-onset refers to individuals who begin drinking problematically earlier in life. Semi-structured interviews were undertaken on both cohorts and their recovery narratives were analysed, interpreted and compared. Having a meaning and purpose in life (MPL) was prevalent among both groups, as were high levels of abstinence self-efficacy (AS-E). Peer-based recovery support (P-BRS) was equally important to both groups. Late-onset participants reported more salience for social networks and greater social recovery capital (SRC) than early-onset participants. The families of late-onset participants were supportive, whereas the families of early-onset participants were ambivalent about recovery. Both groups experienced considerable improvements to their psychological, emotional and mental health in recovery. The study’s findings suggest that P-BRS and MPL mediate AS-E. The important role that P-BRS, MPL and AS-E play in recovery, can inform addiction/recovery practitioners and other healthcare professionals about how recovery can be sustained and how further support for late-onset individuals can be provided through connection to meaningful activities and groups.
Plain language summary
A study which analysed and compared the interviews of two types of older individuals (50+) who drank problematically and who are now in recovery (abstinent from alcohol). Why was the study done? The study wanted to compare late-onset problem drinkers in recovery with early-onset problem drinkers in recovery. Late-onset individuals start drinking problematically later in life (usually after 50-years-old) as a reaction to events that happen in later years, whereas early-onset individuals begin drinking problematically earlier in life. Limited research has been undertaken on late-onset problem drinkers. This study wanted to better understand how they recover and how they maintain their recoveries. The study’s findings can inform healthcare professionals to better understand late-onset problem drinkers. What did the researchers do? Nine early-onset and nine late-onset problem drinkers were interviewed and the interview transcripts were analysed. In the first stage of analysis the participants’ individual personal themes were identified. In the second stage of analysis the individual themes were further analysed and sorted and reduced to group themes for each of the two groups. In the final report, extracts from the interviews were presented as examples of each theme. What did the researchers find? Having a meaning and purpose in life was prevalent among both groups. A high degree of self-belief in being able to stop drinking was common across both groups. Peer-based recovery support was equally important to both groups. Late-onset participants reported having greater social networks and social support than early-onset participants, including family support. Both groups experienced What do the findings mean? The study’s findings suggest that having a meaning and purpose in life, along with the support of other individuals in recovery, encourages the self-belief that one can maintain
Keywords
Introduction
The current paper discusses the recovery narratives of two types of problem drinkers, early- and late-onset. Late-onset are individuals whose drinking becomes problematic later in life, estimated to be ≥50-years old (McInerney et al., 2023, 2025); in contrast, early onset individuals experience problems with alcohol much earlier in life. Many of the individuals in the present study are in long-term/stable recovery. The National Institute on Alcohol Abuse and Alcoholism (NIAAA) have defined stable recovery from alcohol use disorder as, ‘cessation from heavy drinking’ for ‘greater than 5 years’ (Hagman et al., 2022, p. 810). Definitions of recovery from problem drinking have evolved considerably since Jellinek’s (1960) treatise on problem drinking, the Disease Concept of Alcoholism. Jellinek’s concept, however, is concerned with one polar extreme of a problem drinking continuum (Best & Hennessy, 2022). Contemporary definitions, on the other hand, aim to capture a broader range of problem drinker types. The U.S. government’s Substance Abuse and Mental Health Services Administration (SAMHSA, 2012) working definition of recovery, for example, defines recovery as: A process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential (p. 3). SAMHSA’s definition fits comfortably alongside other leading contemporary definitions of recovery (e.g., Laudet, 2007; UK Drug Policy Commission, 2012; White, 2007), representing a move away from earlier paradigms, that pathologised alcohol and other drug problems, towards a paradigm that focusses on ‘recovery-orientated systems of care’, as the solution to these problems (White, 2007, p. 229).
The conclusion to White’s (2007) own definition, ‘develop a healthy, productive and meaningful life’ (p. 236), for example, highlights an important and integral component of the recovery capital (Cloud & Granfield, 2001) model of recovery, that is, (re)discovering meaning and purpose in life. Because of the positive relationship between (re)discovering meaning and purpose in life and recovery, the current study is framed within Viktor Frankl’s theory of meaning (logotherapy). Frankl (1963, p. 83) cites the words of Friedrich Nietzsche to summarise logotherapy: ‘He who has a why to live for can bear with almost any how’. Frankl proposed that the primary force that motivates all human beings, is an innate need to find meaning and purpose in life, ‘the will to meaning’ (Frankl, 2014, p. 9). Frankl developed logotherapy to treat his existential vacuum concept: a feeling of psychological and spiritual emptiness, resulting from a lack of meaning and purpose in life. Describing the vacuum’s symptomatology, Frankl (2011) claimed that ‘alongside depression and aggression, addiction too is at least partially to be traced back to the feeling of meaningless’ (p. 26). Similarly, Forstmeyer (cited in Frankl, 2011, p. 28) found that many problem drinkers ‘view their existence as meaningless and without purpose’. Therefore, (re)discovering meaning and purpose in life is viewed as essential to finding and maintaining recovery and as such, is recognised as one of the eight domains of the recovery capital framework (United Nations Office on Drugs and Crime [UNODC], 2008).
According to Witkiewitz et al. (2020), recovery holds different meanings for ‘different stakeholders’ (p. 2). Arguably, the most important of these, are individuals with lived experience of problem drinking (e.g., Collins et al., 2016; Jacobs, 2018), their families and their friends (e.g., Haeny et al., 2018; McCrady & Flanagan, 2021). An essential consideration when defining recovery, therefore, is what recovery means to those who have been most affected by problem drinking. Individual conceptualisations of recovery are informed by several factors, including gender (Laudet, 2007), cultural and societal norms and attitudes (Best & Hennessy, 2022), spiritual or religious beliefs (Laudet et al., 2006) and the personal meaning that each factor holds for the individual in recovery (J. Nelson & Ogilvie, 2022). Moreover, individual concepts of recovery, particularly for people who engage with mutual-aid organisations are likely to have been influenced, in varying degrees, by the tenets of the mutual-aid organisation to which they are affiliated (Glassman et al., 2022; Williams, 2021).
Koch (2019), for example, who explored the narratives of nine U.S. veterans in recovery, reported a single, joint definition for the study’s nine participants, ‘as total abstinence and enhancement of quality of life’ (p. 112). Although Koch (2019, p. 116) reported a ‘diversity in participants’ and ‘different demographic variables’, the author did not account for the participants’ homogenous membership of Alcoholics Anonymous (AA) as a single source bias. In contrast, L. A. Nelson et al. (2023) explored the lived experience of alcohol use disorder and recovery pathways through the cultural lens of urban, American First Nation and Alaskan Native communities. L. A. Nelson et al. (2023) found their participants conceptualised recovery within a cultural framework, that included meaningful, cultural and spiritual activities, community and indigenous peer support. For the American First Nation population, a marginalised minority, recovery ‘must ensure basic needs are met and thus go beyond a focus on abstinence achievement and maintenance’ (L. A. Nelson et al., 2023, p. 153). Moreover, recovery is not a static construct, it changes over time (Laudet et al., 2002; Vaillant, 2009), as does the individual in recovery (Best & Aston, 2015; Martinelli et al., 2020) and their personal meaning of recovery (Laudet, 2007).
Research suggests that globally, millions of individuals are in long-term/stable recovery from alcohol and other drug disorders (Day et al., 2024). As alluded to above, many of the individuals in the present study fall into this category. However, limited research has been undertaken on the relationship between long-term recovery and meaning and purpose in life, and the dynamics of that relationship over time; the current paper addresses this paucity of empirical information. For instance, although recent surveys in the UK have highlighted long-term recovery, they have not considered the relationship between long-term recovery and meaning and purpose in life. 31% of the respondents to Alcoholics Anonymous Great Britain’s (2022) most recent survey, for example, reported having between 5 and 10 years of continuous sobriety, while 45% reported over 10 years continuous abstinence, many with multiple decades. Additionally, the UK Life in Recovery survey (Best et al., 2015), which gathered data from a broad spectrum of addictions, found the average age people in the UK begin their recovery journey is 38.2-years old. Similarly to Day et al. (2024), both surveys suggest there is likely to be a growing demographic of older individuals experiencing long-term recovery, as well as the challenges that accompany ageing (Gubi & Marsden-Hughes, 2013; Laudet et al., 2002; McInerney et al., 2022). Of the many dictionary definitions of the noun ‘recovery’, two have relevance in the context of problem drinking: (1) ‘the act or process of recovering, especially from sickness, a shock, or a setback and (2) the regaining of something lost’ (Dillons, 1990). The overarching aim of the current study then, is to investigate the recovery narratives of early- and late-onset problem drinkers, compare their characteristics in recovery and identify the factors that support and sustain recovery in both groups. To achieve these objectives, the study addresses the following question: What are the factors that help to sustain recovery in early- and late-onset problem drinkers and what are the differences between the two groups?
Method
Based on Frankl’s ontological positioning of logotherapy as an adaption of ‘the phenomenological methodology’ (Frankl, 2014, p. xvi), interpretative phenomenological analysis was considered to be the most appropriate method of investigation. The choice of interpretative phenomenological analysis as the study’s method of investigation is informed by the philosophical theory or approach of phenomenology, which is concerned with the lived experience of the individual. Semi-structured interviews took place during 2021, when the COVID19 Pandemic was still a major health risk. Therefore, the interviews were undertaken online using Microsoft Teams. On a positive note, this meant that there were no restrictions concerning the geographical locations of the interviewees. However, this method does have its limitations. For example, there can sometimes be connectivity glitches. Moreover, not all individuals are tech savvy, and some potential participants may not have access to the internet.
Sample Size and Eligibility Criteria
Qualification for participation were individuals of ≥50-years old, in recovery from alcohol use disorder/problem drinking, which in the context of the present study, refers to an abstinence model of recovery. Interpretative phenomenological analysis studies typically investigate small, homogenous groups consisting of five/six participants. That said, leading interpretative phenomenological analysis researchers have investigated larger samples of nine (Osborn & Smith, 1998). Therefore, and because the two cohorts are two separate, heterogeneous groups (i.e., early- and late-onset), nine participants for each cohort were recruited.
Recruitment
The current study is part of a larger project and the participants were recruited from a related quantitative paper that included a survey (McInerney et al., 2025). The survey provided a box in which people who were interested in being interviewed could leave their email address to be contacted. That study, which recruited 381 participants, quantified the ages for early- and late-onset, that are used in this study. McInerney et al. (2025), were able to recruit as diverse a sample as possible, by contacting prominent mutual-aid organisations (e.g., AA, SMART Recovery) and the R&D department of a National Health Service (NHS) Trust. Potential participants were contacted, interview dates and times were arranged and Teams invitations, along with informed consent forms were dispatched. Prior to each interview, a complete discussion of the study with potential participants took place, before they signed and returned the informed consent form.
Data Collection
Data was collected using Teams’ transcription function. However, the accuracy of the transcripts depends on the clarity and enunciation of the participants and the interviewer and has a tendency to misinterpret language, therefore, audio recordings of the interviews were also undertaken. Teams transcripts were downloaded as Word documents, crossed referenced against the audio recordings, cleaned and amended to produce accurate, verbatim transcripts. Participants were pseudonymized. The following phases of analysis were undertaken for each participant.
Analysis
Analysis was informed by Smith and Nizza’s (2022) recommended guidelines. Additionally, Smith et al.’s (2009) earlier interpretative phenomenological analysis guidelines informed the practical and theoretical considerations of analysis. Analytical terms have evolved since Smith et al.’s (2009) original recommendations, to more accurately reflect the theoretical focus of interpretative phenomenological analysis, that is, the lived experience of participants. As such, Emerging Themes have become Experiential Statements and Individual Superordinate Themes are now Personal Experiential Themes.
First Stage of Analysis
Transcript text was arranged in a three-column landscape format in desktop publishing software (QuarkXpress); Microsoft Word can also be used for this purpose. Transcript texts were placed in the middle column. To become familiar with them, transcripts were read at least twice. During this initial stage of interpretation, when the researcher becomes immersed in the participant’s narrative, the fundamental interpretative phenomenological analysis technique of the ‘double hermeneutic’ occurs, whereby the researcher attempts to view the participants’ narrative from the perspective of the participant, who themself are attempting to make sense of their own discourse. This technique results in interesting, informative and meaningful statements being highlighted, using different colours.
Interpreting Experiential Statements
The statements highlighted in the text in the initial stage (above) were interpreted into experiential statements and reported in the left-hand column. Interpretation is a fluid and evolving process; the same experiential statements can, for instance, appear on multiple occasions throughout the transcript and the meaning and wording of experiential statements can be changed as each page of the transcript is explored. Additionally, at this stage of analysis, exploratory notes are recorded in the right-hand column; these notes are important as they inform interpretation.
Clustering Experiential Statements Into Personal Experiential Themes
Each participant’s experiential statements were printed and cut out individually. The statements were placed randomly on a table, to allow a ‘bird’s-eye view’ (Smith & Nizza, 2022, p. 43) and moved around, until conceptually similar clusters began to form (Shinebourne & Smith, 2009), with each being given an appropriate title (Appendix 1). Experiential statements that did not make sense conceptually or map onto any personal experiential themes were discarded. Tables of the participants’ individual personal experiential themes were then compiled.
Bringing it all together – moving from Personal Experiential Themes to Group Experiential Themes
Finally, comparisons and conceptual links between the individual personal experiential themes of each participant were identified; these mapped onto and formed the group experiential themes for each cohort. Each group experiential theme was given a title, which again, made sense conceptually.
Results
Demographics
Both groups had a similar mean age, the early-onset cohort ranged from 50- to 71-years old (m = 60-years old), while the late-onset group ranged from 53- to 67-years old (m = 61.7-years old). That said, years in continuous recovery differed considerably, ranging from 18-months to 35-years among the early-onset group (m = 12.27-years), approximately three times longer than the late-onset group, whose continuous time in recovery ranged from 1 month to 15-years (m = 4.6-years). Gender was distributed equally across onset-types, with five females and four males in either group. The participants’ characteristics are summarised in Table 1.
Participants’ Characteristics.
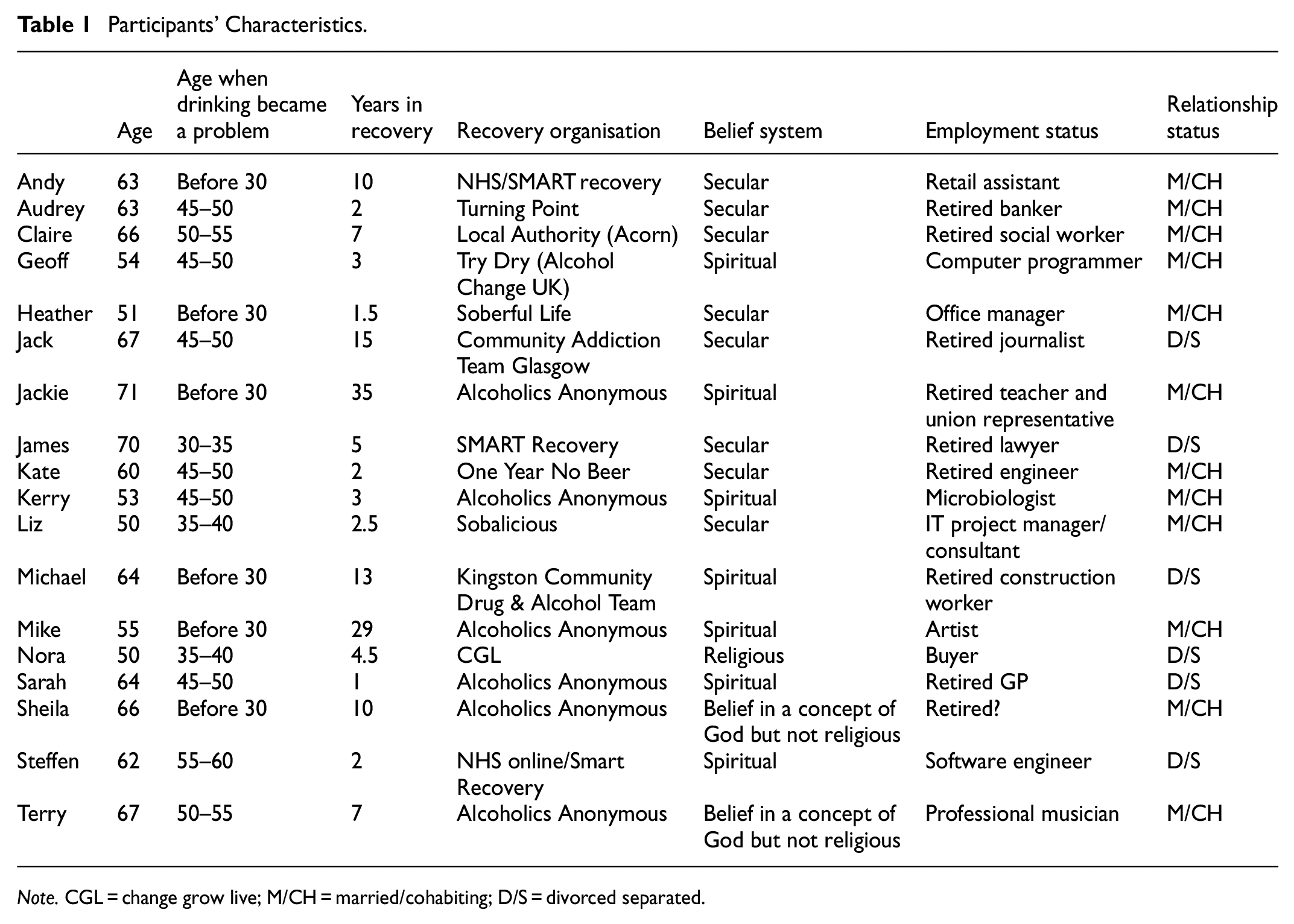
Note. CGL = change grow live; M/CH = married/cohabiting; D/S = divorced separated.
Narrative Extracts
The focus of the results section is to present extracts from the participants’ personal accounts (personal experiential themes) of their recoveries, which in turn, embody the group experiential themes of each of their groups. There were five early-onset group experiential themes and four for the late-onset group (Figure 1). Refer to Appendices 2 and and 3 for tables of the participants’ individual personal experiential themes, which also demonstrate, conceptually, how they map onto and form each group experiential theme.

Group experiential themes.
Early-Onset Group Experiential Themes
Early-Onset Theme 1 – Mutual-Aid and Peer-Support Nurturing Recovery
The first early-onset group experiential theme, indicates that peer-based recovery support (P-BRS), usually (but not always) found at mutual-aid organisations, had been fundamental to recovery for six of the group’s participants. P-BRS is, arguably, the most important component of mutual-aid organisations (e.g., AA, SMART Recovery). However, a single mutual-aid organisation model doesn’t work for everyone, people seeking recovery can choose the organisation where they feel most comfortable, as evident in Andy’s discourse. Nonetheless, the participants’ extracts suggest the most prominent feature of P-BRS, common across all mutual-aid organisations, is the emotional mutuality inherent in identification. Identification has a powerful, liberating quality, demonstrating to the individual in recovery that they are no longer alone and that others too, shared a similar relationship with alcohol.
Powerful, welcoming, ehm … and a bit, bit frightening before you actually start, before I actually started, but, because I’m going to the SMART community, I knew I was among friends or people who at least knew what I was going through. (Andy) … you’re confused, and it’s a new world, and that’s why AA’s great for you. You’ve got other people to share that journey with. [… .] you suddenly realise, oh yeah, I know I’m going through that now, I’m doing that, I’m behaving like that, and I’ve seen that in someone else. (Mike)
Summary of Early-Onset Theme 1
Although not all the participants’ personal experiential themes mapped onto this group experiential theme, the narratives of those who did, highlights the role that ‘identification’ plays in the mutual-aid organisation recovery pathway. ‘Hope’, a feature of the CHIME recovery framework (the other four components being: connectedness, identity, meaning in life and empowerment; Leamy et al., 2011), characterises the collective narrative of the six participants that constitute this theme. Hope that the examples of recovery that the participants had witnessed in fellow sufferers was possible for them too. Hope, the consequence of P-BRS, was generated by two closely linked forces: (1) identification and (2) the power of example, which, according to Moos (2007, p. 117), can be explained by theoretical ‘evidence-based social processes’, such as social learning theory and social control theory.
Early-Onset Theme 2 – Abstinence Self-Efficacy: A Primary Mechanism of Behaviour Change
Central to this theme is the participants’ realisation that they have the ability to access abstinence self-efficacy (AS-E), something explicitly referenced by four of the theme’s constituent personal experiential themes and implied by the remaining personal experiential themes. Self-efficacy is the individual’s perceived ability (self-belief) to undertake certain actions that will help them to achieve their goals, which in the context of the participants’ behaviour in this study, is cessation of drinking. Mike’s AS-E, for example, is manifested in his pragmatic life philosophy, while Sheila’s willingness to behave differently, has resulted in being able to view life from a positive perspective.
I don’t want to drink no more. I just don’t want to drink no more, you know. […] Life doesn’t ask for terms, it’s whether I choose to put terms on it, and that’s when I get upset. […] We exist, you know, we exist, and we make the best of it. But a little bit of planning is not a problem. (Mike) I used to wake up and if it was sunny, it’s a reason for a drink. Now, I wake up and it’s reason not to drink. Ehm, you know, but it’s not just AA, it’s actually my perception of life. […] And I don’t want to feel sorry for myself because every day you feel sorry for yourself, it’s a wasted day… (Sheila)
Summary of Early-Onset Theme 2
The participants’ narratives in this theme place their drinking at the extreme and harmful end of a problematic drinking continuum. The theme suggests that high-levels of AS-E may have been the primary mechanism of behaviour change, in the participants’ transition from problem drinking to a different way of living and being in the world, that is, recovery. The notion of AS-E as a mechanism of behaviour change for problem drinking, is supported by prior research in this area (e.g., Kelly, 2017; Kelly et al., 2009; Kelly & Hoeppner, 2013).
Early-Onset Theme 3 – Finding Psychological and Emotional Equilibrium
The participants’ discourses in this theme suggests the clarity of sobriety creates a positive space in which they can acknowledge and better understand their emotional and mental health. That said, Jackie’s narrative shows that emotions can be difficult and challenging in recovery too. For Jackie, sobriety affords her the psychological and emotional space to cultivate and nurture methods that enable her to navigate challenging emotions and negative thought processes, without having to self-medicate them with alcohol. For Nora, who has bipolar disorder, recovery means that she can look after herself better and manage her medication, something she was unable to do when she was drinking.
You know, I’m getting old. I’m finding it more and more difficult to sort of cope and I’m not, you know, not particularly happy. I can’t seem to get rid of it. But you know, the difference is, I’m not rushing out and picking up a drink or drugs. (Jackie) … my life has changed significantly for the better. Ehm, with not drinking alcohol, you know, mental health is a lot better. Ehm, you know, I’m on the right medication. I look after myself more because I’m a diabetic and insulin dependent. You know, those are things that I couldn’t do when I was drinking. (Nora)
Summary of Early-Onset Theme 3
The participants all follow an abstinence-based model of recovery. However, the narratives in this theme highlight that cessation of drinking is only the beginning of a journey to find and restore mental, psychological and emotional equilibrium. The participants understand, that similarly to their behaviour, their psychological, mental and emotional problems are deeply embedded in their being, their discourses demonstrate that the clarity of thought that follows recovery, allows them to understand and address these problems.
Early-Onset Theme 4 – Managing and Accepting Family Dynamics in Recovery
This theme emphasises the variable family reactions to the participants’ recoveries. Heather, for example, had to negotiate a hostile reaction from a family steeped in a drinking culture, who are resentful that Heather has chosen recovery, particularly an abstinence-based model. They lack understanding, tolerance and empathy for Heather’s sobriety.
My dad’s, my da, I mean, he’s in his eighties, he’s already told me I’m on the wrong path, being sober. I mean, that’s not very, very helpful, is it? […] mum’s feeling that somebody that doesn’t drink isn’t normal, right? My sister, it’s, it’s always been again […] We had the same upbringing, her drinking has always been actually worse than mine and her behaviour has always been worse than mine […] And the sad thing is now, is she kind of like doesn’t want anything to do with me either because I’ve stopped drinking. (Heather)
Mike recalls childhood experiences of family holidays and his narrative reflects on a ‘place of safety’ he discovered, where he could escape the chaos of his family’s drinking behaviour. Today, he uses the thought of that place as a reflective technique, that acts as a coping mechanism.
I was only, like, under five anyway. Long story short, I was up in the roof and the pigeons used to sit on the roof and coo in the morning […] And I was very content there, you know, I felt very safe there and so that became my thing, that was my place. Take myself out of this and put myself in that loft room knowing the whole family is all downstairs. […] So, when I say oh, pigeons are my Higher Power, they go “what?” I use them as a safe place, it’s a link to something bigger and better and wider. (Mike)
Summary of Early-Onset Theme 4
The role of the family in recovery is a major area of investigation, and a considerable body of work is available on the topic (e.g., McCrady & Flanagan, 2021; Moos & Moos, 2007). The narratives of the participants in this theme highlight how variable family reactions to recovery are. The selected extracts from this theme indicate that both family drinking cultures and alcohol-related behaviour and events are deeply embedded.
Early-Onset Theme 5 – Empathy: Reaching Out to Others Gives Life Purpose and Meaning
The relationship between empathy and meaning and purpose in life was present in the personal experiential themes of eight of the early-onset participants. Empathy for individuals who are suffering fulfils two psychological functions in recovery; it reinforces sobriety, which in turn, promotes having meaning and purpose in life. Apart from its primary existential purpose, recovery for the early-onset participants, among other things, is about finding meaning and purpose in life. In this theme, the participants’ narratives are bound together by the common strands of empathy and meaning and purpose in life.
… I’ve got enough emotional fuel to be able to help other people. But there’s a sober person, there’s a part of me that tries to help. I know for an absolute fact I’m not qualified to help, the only thing that I can do is talk about my experience. (Liz) … there’s a role that I want to develop in, in long-term recovery, which is the role of a recovery coach. Somebody who would work one to one with four or five people, who are on their feet and sorted, but need some additional support in pulling their plan together. (James)
Summary of Early-Onset Theme 5
The last early-onset theme highlights the simple relationship between empathy and having a purpose in life. The participants’ narratives suggest that helping other individuals who are ‘in the same boat’, appears to take on greater relevance and meaning to those participants in relatively early to stable recovery (James, Liz, Nora). For the participants in long-term recovery (Andy, Mike), empathy appeared to take on a broader meaning, beyond being an individual life purpose of supporting others in recovery.
Late-Onset Group Experiential Themes
Late-Onset Theme 1 – Abstinence Self-Efficacy: A Primary Mechanism of Behaviour Change
The first late-onset and the second early-onset themes share the same label. Personal experiential themes from eight of the nine late-onset participants mapped onto this theme, compared to six participants in the early-onset version, suggesting the presence of high levels of AS-E across both groups. Abstinence is, undoubtedly, the ‘foundation’ on which all the participants base their recoveries.
And I feel as though even from twelve months ago, I am in a much better place, for lots of reasons, but it’s ‘gonna be, the bottom line has got to be through being sober. But that’s the foundation. (Kate)
Claire’s continuous abstinence, now totalling 7 years, began with a drinking reduction programme, aimed at helping people to gradually reduce their alcohol intake.
… and I’d got to the point where I literally was pouring most of it down the sink, and having a glass, a big glass, you know, one like that (indicates with her hands the size of a big glass), not a few ones, but it was one glass. It suddenly struck me that it was just the height of stupidity. And that’s when I stopped. But I’d been getting help for about two or three weeks before that. […] I went to a programme that was called RAMP (Reduction and Motivation Programme) and that was about education. (Claire)
Summary of Late-Onset Theme 1
The participants’ narratives in this first late-onset theme suggest that, along with mutual-aid organisations or community drug and alcohol services (in early recovery), their recoveries are supported by AS-E. Their narratives suggest that AS-E is a personal, cognitive attribute, that can be accessed to facilitate behaviour change. It is important to emphasise that AS-E is not and should not be conflated with willpower, AS-E is having enough self-belief to be able to access and utilise a positive and liberating cognitive resource.
Late-Onset Theme 2 – Connecting and Being in the World With Others
Developing social networks and connecting with other people is typically considered to be high value social recovery capital (SRC; Mawson et al., 2015) and is an essential component for many people in recovery and is particularly important for the participants in the current study. SRC counteracts isolation and loneliness, prevalent characteristics among older problem drinkers (Canham et al., 2016; Ingram et al., 2020). Kate, for instance, has recognised the importance and benefits of being and connecting in the community. When Kate lost her job as an engineer, she lost her identity too. Her professional identity gave her life a purpose and meaning and she experienced an existential vacuum and her newly constructed community connections, can be viewed as the SRC that contributes to filling that void.
I now realise that my priorities are my family, my friends and connections, you know, community connections. You know, if I can help with anything I do, you know, I help old ladies go to hospital and appointments and stuff like that now. (Kate)
This fundamental social function of ‘being with others’, is often interpreted purely in terms of helping a fellow sufferer and thereby reinforcing one’s own sobriety and recovery, while the pragmatism of building social networks is often overlooked. Working with the Alcohol Care Team, in a voluntary capacity at King’s College Hospital (London), Terry visits patients who have alcohol and other drug problems.
Just that the idea that each of us is on their own journey. And you know, when we do the hospital service, for example, we go in and we speak to people and we’ve got maybe twenty minutes with them, maybe half an hour, if you’re lucky, and then you never see them again. In that, in that brief time you connect, you listen to them, you impart some of your own experience and then that’s it you go your separate ways. (Terry)
Summary of Late-Onset Theme 2
The theme highlighted the importance and value of SRC. Additionally, the theme emphasises that P-BRS and mutual-aid organisations are not solely about support through the reciprocation of shared lived experiences, they support individuals in recovery to access social networks.
Late-Onset Theme 3 – Recovery as a Family Journey
In common with the early-onset cohort, this late-onset group experiential theme is framed within the context of the family in recovery, however, that is where the similarity ends. In contrast to the negative and often hostile dynamics of the early-onset group, the family dynamics apparent in the narratives of the late-onset cohort were mostly positive and supportive. For example, Steffen’s ex-wife and her partner, became the scaffolding that supported his early recovery.
And so, she and her partner, you know her boyfriend, were living together and they, you know, they opened-up their house to me after I left the detox and I was waiting to go to a particular, you know, inpatient programme. […] So, it was really helpful that I was able to stay with her during that time, to stay with them and, and …. because otherwise, I think I would have relapsed, you know, and started drinking again. (Steffen)
Sarah had a history of relapsing and there were times, when her children were teenagers, that the parent/child roles were reversed. Her children have been deeply affected by her drinking. Sarah’s narrative about her relationship with her daughter being a contributory factor in her drinking, shows that she still has some way to go in her recovery. Nonetheless, Sarah’s children have been extremely supportive in her recovery.
I was encouraged and supported through my last couple of relapses. They took me to rehabs. They were the adults, and I was the child, and we had several meetings around that. […] I would say that they’re supportive in terms of things, like they say “We’re really proud of you, you’re changing, you seem different, you don’t seem so anxious. We’re not so worried about you”. (Sarah)
Gary’s daughter had a life-limiting illness and died when she was just 8-years old. Gary’s other children (he has twins) were affected by his drinking, ‘Oh he’s drunk, he’s sleeping in bed’. He is aware of the psychological damage his problem drinking caused, so not surprisingly, family is his primary purpose in life.
… I’ve got a family, a wife, two kids who are doing pretty well at school, nice house, so my sort of, my purpose is to kind of try and lock that in a bit a bit more reliably, so that I can, I can then inch forwards with getting a job and, and ehm, being out of the house or doing a lot more work where I won’t upset the apple cart of where we are now. (Gary)
Summary of Late-Onset Theme 3
The third late-onset theme suggests that for most of the late-onset participants in the current study, recovery is framed within the context of a positive and supportive family; as such recovery, is not so much an individual experience, rather it is a family journey. In contrast, the narratives of the early-onset cohort described family support, at best, as indifferent and at times, even hostile to recovery. Typically, the late-onset participants had greater baseline SRC than the early-onset group. Interestingly, the narratives of the late-onset group refer to family relationships, as the theme title suggest, a journey that is happening in the present moment. Whereas for the early-onset cohort, family is typically constructed as their family of origin and often contained recollections from the past.
Late-Onset Theme 4 – Having a Purpose Gives Life Meaning
The final late-onset theme reflects the last early-onset theme, highlighting that both cohorts viewed meaning and purpose in life as an essential component of recovery. However, the routes the participants in each group have taken in their search for purpose in life and consequential meaning, although similar in their purpose, differ in their application. Whereas the early-onset cohort have found purpose in life, mostly in supporting others in recovery, the source of purpose in life for the late-onset group, although still found in reaching out to others in recovery, was more likely to manifest in a broader and more inclusive community and societal context.
So, I did the training and I began doing facilitating and, and I found it rewarding, right? And it gave me purpose, you know. I could take from, you know, my experience or my perspective and, you know, sometimes maybe help someone else, you know. So, I, I looked at it more, like, community and society, you know, is something that I care for in a sense, as opposed to just my kids or family, in a way. (Steffen) I recognise now the importance of community and connection. And it is that meaning and purpose that I’m seeking in my older age to, ehm, to push me forward really, because, you know, before COVID, I had two little jobs, you know, nothing special but I enjoyed them. […] I spend as much time as I can either with friends or at the charity shop, volunteering at the charity shop. (Kate) To not necessarily have a single purpose because I’m not trying to stay sober or anything like that, but to take each day as it comes as a fresh set of challenges, but to look ahead and to keep doing things like the editing stuff I do. Like the, what else am I doing this week (?), oh yeah, I’m going to the voluntary fair on Wednesday to try and find new volunteer things, and babysitting, childminding for friends and family and stuff like that. (Jack)
Summary of Late-Onset Theme 4
The participants of both groups have found that having a purpose in life, is an essential component in their recoveries, suggesting that the meaning that emerges from having a purpose in life fills the ‘existential vacuum’, once occupied by alcohol.
Discussion
From a theoretical perspective, in accord with Frankl’s (2011)existential vacuum concept (i.e., the feeling that life is without meaning and purpose), the study’s findings suggest that ‘the will to meaning’ (Frankl, 2014, p. 9), is a central and necessary feature of recovery. Of course, it can reasonably be argued that a small sample of 18 older individuals in recovery does not generalise to the wider population of recovering older problem drinkers; interpretative phenomenological analysis, however, is not about populations, it is about ‘individual lived experience’. Frankl’s theory of meaning (logotherapy) was born from, and developed out of his own traumatic lived experience and suffering in the Nazi concentration camps in World War II (Frankl, 1963). After arriving at Auschwitz, Frankl was stripped of his clothes, which included, secreted in one of the pockets, the manuscript of his unfinished first book. He likened the experience of having his cherished manuscript taken from him, as having to come to terms with the loss of his ‘mental child’ (p. 118). After his experiences of internment, Frankl devoted his life to helping others. It is, therefore, worth noting that the development of meaning and purpose in life, highly prevalent among the present study’s population, was promoted by similar altruistic thoughts and actions in the form of P-BRS.
In the introduction it was noted that recovery is a fluid concept, holding different meanings, depending on the perspective of the stakeholder (Witkiewitz et al., 2020). Analysis of the participants’ narratives reflects that position from an individual perspective. The introduction highlighted that an individual’s concept of recovery tends to be influenced by the mutual-aid organisation to which the individual is affiliated; this was particularly evident in the discourses of the AA participants, who framed their recoveries within the tenets of that organisation. The study identified several common group themes across the study’s two cohorts. The nine themes (five early- and four late-onset) have been further reduced and are explained within the confines of four domains: AS-E, family, SRC and meaning and purpose in life.
The participants across both cohorts shared a common theme: Abstinence self-efficacy: a primary mechanism of behaviour change. Their narratives highlight the dynamic relationship between P-BRS and AS-E. It is more than appropriate to frame both of these psychological constructs within Frankl’s logotherapy: P-BRS, for example talks to Frankl’s humanistic psychological principle of helping others, while AE-E reflects Frankl’s (2011) plea to the individual to be responsible for their own lives, something that he refers to as ‘responsibleness’ (p. 92). The first early-onset theme, Mutual-aid and peer support nurturing recovery, suggested that the mediating effect that P-BRS has on AS-E was greater among the early-onset participants. P-BRS formed the basis of a social network for the early-onset participants, and although P-BRS was important for the late-onset group too, they tended to have greater baseline SRC to fall back on (e.g., supportive families). Overall, these findings support both Bandura’s (1977) self-efficacy theory and social learning theory (Bandura & Walters, 1977). According to Bandura (1977), expectations of self-efficacy are informed and emerge from four primary sources: performance accomplishments, vicarious experience, verbal persuasion and physiological states” (p. 194), all of which are present in the narratives of both cohorts. The positive association between P-BRS and AS-E is supported by a broad body of work (Tracy & Wallace, 2016; van Melick et al., 2013).
Family is an important component of the SRC model of recovery (e.g., Best et al., 2021; Cano et al., 2017). The behaviour of individuals who drink problematically and their families are ‘inextricably bound’ (McCrady & Flanagan, 2021, p. 2), both during active drinking and also in sobriety/recovery. The participants’ narratives, however, highlighted notable differences in family dynamics between the two cohorts, evident in the titles of their respective themes (and constituent personal experiential themes): Managing and accepting family dynamics in recovery (early-onset), Recovery as a family journey (late-onset). The two contrasting themes showed that the late-onset group had more supportive families, contributing to greater SRC. Similar findings on differences in family dynamics between early- and late-onset individuals have reported that late-onset problem drinkers are likely to have lived in a functioning family environment, in contrast to their early-onset counterparts, who were more likely to have been associated with, and affected by a family drinking culture (e.g., Liberto & Oslin, 1995; Wetterling et al., 2003). These findings support the widely held premise that emotional development often stalls at the age an individual becomes addicted to substances, which in part, can be related to family attitudes and a history of addiction in the family (e.g., Bratek et al., 2013; Sullivan et al., 2016; Wilson et al., 2013). That each cohort had contrasting family themes, adds further support to the premise.
Broadly speaking, SRC includes the intellectual, material, psychological and emotional resources (this is not an exhaustive list), within family and social contexts, that are available and accessible to individuals, that can be utilised to support them in their recovery journeys. Having already considered the family component, the discussion focusses on the social aspect of the SRC model, of which P-BRS is a central component (e.g., Andreas et al., 2010; Best et al., 2012). The current discussion has already had much to say about the social model role that mutual-aid-orientated P-BRS plays in promoting and supporting AS-E (e.g., Majer et al., 2015, 2016; Marlow et al., 2015). P-BRS also played an important role in re-building positive social networks. P-BRS was a thread that ran throughout the narratives of both groups, a common link, supporting the participants to re-connect with society.
Although P-BRS was prevalent among both onset-types in describing early recovery, the early-onset participants were more likely to develop long-standing, P-BRS-linked social networks. In terms of social capital theory (Putnam, 2000), this type of capital is referred to as ‘bonding social capital’ and is within group, exclusive and inward-looking. Whereas the late-onset participants’ social networks were more likely to be categorised as ‘bridging social capital’ and were not restricted to mutual-aid circles. Bridging and linking social capital is between groups, inclusive and outward-looking and may include, for example, ‘workplace networks, and social clubs/activities’ (Boeri et al., 2016, p. 1). Regarding gender differences within a SRC context, there is some evidence to suggest that building and nurturing social networks is more likely to be associated with men as a mechanism of behaviour change, and that behaviour change in women is primarily associated with improvements in AS-E (Kelly & Hoeppner, 2013). That women may be less likely to foster positive social networks in recovery, may be associated, in part, with the greater perceived social stigmatisation they may have experienced when they were drinking problematically (Brennan et al., 1993; Fortney et al., 2004). There were, however, no noticeable gender differences regarding social context in the present study.
Already noted, many of the participants in the current study are in stable or long-term recovery. Length of time in recovery is associated with greater meaning and purpose in life (Junior, 2006) and is viewed as central to achieving and maintaining recovery (e.g., Laudet, 2007; White et al., 2006; World Health Organization [WHO], 2020). Such a transformational change in attitude, however, does not emerge in a vacuum. This life-changing way of thinking is the consequence of the complex interactions of the closely entwined themes and domains identified in the present study, evident in the personal themes that constitute the fifth early-onset theme, ‘Empathy: reaching out to others gives life meaning’, and the fourth late-onset theme, ‘Having a purpose gives life meaning’. The participants’ narratives, as expressed in the title of the two themes, construct the experience of helping others as a meaning-making process, demonstrating the considerable role that having meaning in one’s life plays in recovery.
As noted above, meaning in life is a characteristic of the CHIME model of recovery (Leamy et al., 2011). That meaning and purpose in life was equally prevalent in the narratives of both groups, confirms the importance of these two constructs (i.e., meaning and purpose) in supporting and maintaining recovery. Crucially, having a meaning and purpose in life is also associated with improvements in psychological and emotional health; meaning-making for example, mediates anxiety and depression (Marco et al., 2021; Radicic & Rivardo, 2019). The participants’ narratives suggest that the altruistic behaviour of helping one’s peers, provides one with enough purpose in life in early recovery to counteract the purposelessness of the existential vacuum. That said, the mean age of the study’s 18 participants is 61 years-old, many of whom are in long-term recovery. For the participants in the present study then, and driven by the social, cognitive, physiological and psychological decline inherent in the ageing process, purpose in life takes on a different, broader meaning. Not only does having a purpose in life prevent the re-emergence of an existential vacuum, having a life purpose can contribute ‘to health and well-being in older adulthood’ (Windsor et al., 2015, p. 984), something that is vitally important to the participants in this study.
Limitations
Although problem drinking permeates all socioeconomic groups, the participants in the current study were, predominantly, of a professional status, something that can be explained by self-selection bias. That is, individuals who volunteer to participate in research tend to share several characteristics: they are usually better educated, have a higher socioeconomic status (SES), and are interested in the topic of the research they are volunteering for (Nikolopoulou, 2022). Therefore, it could be argued that the results, to some degree, were affected by self-selection bias. Additionally, there was an oversight regarding the ethnic diversity of the participants. However, it is difficult to recruit black and ethnic minorities, who typically, are under-represented in drug and alcohol services throughout the UK (Bayley & Hurcombe, 2011). To address this commonly recurring issue, researchers should ensure their recruitment methods are designed to include ethnically balanced samples, representative of the population seeking recovery. That said, of far greater urgency, is the need for more research to better understand the stigmatisation and cultural barriers that prevent black and ethnic minority populations and other minority groups seeking help from alcohol services and mutual-aid organisations for their problematic alcohol use.
Concluding Remarks and Implications
There was a high degree of convergence among the recovery discourses of both cohorts, evident in the four recovery domains discussed above; this was particularly evident in high levels of perceived AS-E. Self-efficacy theory hypothesises that the individual’s expectation of a given action or behaviour will lead to a particular outcome, that is, ‘the conviction that one can successfully execute the behaviour required to produce the outcomes’ (Bandura, 1977, p. 193). In the context of the population being investigated, the participants’ narratives suggest that Family, SRC and having a purpose in life and finding meaning, constitute the scaffolding that supports AS-E. In summary, the current study found a high degree of convergence in the psychosocial characteristics and recovery pathways between early- and late-onset problem drinkers. It is evident that meaning and purpose in life plays a considerable role in recovery. However, meaning and purpose in life cannot be given, rather, it’s value lies in the seeker finding their own purpose and subsequent meaning. Although it has been used only rarely, logotherapy has been applied successfully on individuals recovering from alcohol and other substance use disorders (Ortíz & Flórez, 2016; Siadat & Gholami, 2018). The current study’s findings suggest that perhaps it is now time to consider logotherapy as a therapeutic tool to support older problem drinkers in recovery.
This study contributes much needed knowledge to the limited research undertaken on late-onset problem drinking, crucially from the perspective of recovery. So little is known about this population, whose problematic use of alcohol so often goes unrecognised, that the Royal College of Psychiatrists (2018) refers to them as ‘invisible’. Effective dissemination of the study’s findings can inform healthcare professionals and help to create an awareness of this distinct group of older problem drinkers, giving them a more palpable presence in health and social care settings. Moreover, by directing and helping people to find meaningful and creative activities and groups, recovery workers and healthcare professionals are supporting late-onset problem drinkers to find meaning and purpose in their lives, which importantly, supports and maintains recovery.
A Reflective Note by the Lead Author
It is pertinent that the lead author discloses his lived experience of problem drinking and recovery; he has been in recovery and continuously abstinent from alcohol for 35-years. Being a researcher with an insider perspective can be challenging. On one hand, being an ‘expert by experience’ and having first-hand knowledge of the object of investigation, means that one has the potential to access ‘the private perceptual world’ of the participants (Rogers, 1975, p. 3). On the other hand, over-familiarity with the object of investigation challenges one’s objectivity. The author managed this dichotomy and mitigated against his own biases by acknowledging them, by being constantly aware of his insider status and by applying Husserl’s (1999) bracketing technique (epoché), the phenomenological notion of discarding one’s preconceptions about the object of investigation. Finally, the lead author followed Smith et al.’s (2009) suggestion, that placing positive engagement with the study’s participants ahead of one’s bracketing concerns, insures that ‘skillful attention to the former inevitably facilitates the latter’ (p. 35).
Footnotes
Appendix
Personal Experiential Themes Mapped onto Group Experiential Themes for Late-onset Participants.


|
Note. Some of the participants’‘personal experiential themes’– dependent on the ‘experiential statements’ contained with the theme – map onto more than one ‘group experiential theme’. For example, Finding a purpose in life (Gary) maps onto Recovery Voice Group Experiential Themes 3 and 4; Recovery as a family journey and Having a purpose gives life meaning, respectively.
Author Notes
David Best is Professor of Criminology and Director of the Centre for Addiction Recovery Research (CARR) at Leeds Trinity University. He has a PhD in Addictions Studies and is currently involved in recovery from addiction research projects in the UK, Belgium, the Netherlands, Canada, the USA, Australia and New Zealand. Philip Hodgson is Professor of Criminology and Dean of the Faculty of Social Sciences and Education (FSSE) at Leeds Trinity University. Kevin McInerney has a PhD in Addictions Studies and is a post-doctoral researcher at Leeds Trinity University.
Ethical Considerations
Ethical approval was granted by: The College of Business, Law and Social Sciences Research Ethics Committee, at the University of Derby; application ID: ETH2122-2604. Additionally, because data was collected from the NHS, additional ethical approval was granted by: The NHS Health Research Committee (HRA) Research Ethics Committee (REC). REC reference 22/EM/0162s. Integrated Research Application System (IRAS) project ID: 314610.
Consent to Participate
An explanation of the research and an informed consent section was included at the beginning of the online questionnaire
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
Originality Statement
We, David Best, Philip Hodgson and Kevin McInerney, declare this report to be our own work. Wherever we have referred to the work of others, we have accurately credited their work using the American Psychological Association (APA) referencing system. The submitted work follows Leeds Trinity University advice on good academic conduct and practice.