
Abstract
COVID-19 has affected people all over the world. For those who were infected by the virus, the repercussions go beyond immediate medical conditions to include social stigma, fear, uncertainty, and lifestyle changes. This study presents data collected as part of a mental health intervention (COVID Response) with individuals who had been diagnosed with coronavirus and had completed the minimum 14 days isolation period, in the city of Delhi, India. Through a survey conducted telephonically, participants self reported on six major mental health indicators: levels of worry, mood, lifestyle changes made through the phase of diagnosis and recovery, perceived discrimination faced due to the diagnosis, and the willingness to donate blood plasma. Descriptive findings show lower levels of worry than at the time of testing and diagnosis, positive mood states, and availability of social support. One Way Anova results further indicate that worry differed significantly across groups with differences in lifestyle changes, reported mood, availability of medical care, and the willingness to donate plasma. These findings contribute toward an informed understanding about recovery from coronavirus and sustainable coping with the pandemic, which can aid related health initiatives and evolving policy.
Introduction
The COVID-19 pandemic has resulted in a global health crisis. The virus has affected 214 countries across the globe and caused over a million deaths worldwide. With a population of 1.35 billion people in a developing country like India, a surge in the number of COVID cases has put immense pressure on an already overburdened healthcare system (Dubey et al., 2020). The lack of appropriate healthcare infrastructure in such a densely populated country has caused worry and panic among the masses who feel helpless due to the inadequacy of protective measures (Roy et al., 2020). Yet, this is not a one-off case and several countries have struggled to cope with the sudden and unprecedented repercussions of the pandemic (Kmietowicz, 2020; The Lancet, 2020). Beyond the physical health of the masses, the pandemic has had detrimental effects on the psychological well-being of people all over the world (Kazlauskas & Quero, 2020; Kumar & Nayar, 2020; Roy et al., 2020; Torales et al., 2020). Cross cultural studies have highlighted the significant relationship between physical symptoms of COVID-19 and adverse psychological outcomes (Wang et al., 2021). In the United States a COVID-19 diagnosis was associated with an increased risk of a subsequent psychiatric diagnosis in nearly 20% of patients (Taquet et al., 2020). In China, COVID-19 patients reported significantly higher levels of distress than healthy controls and were comparable to patients with psychiatric history in mental health outcomes (Hao et al., 2020). This calls attention to the continuing psychological effects of coronavirus and a need for suitable post-treatment care. Balachandar et al. (2020) emphasize the need for follow-up care and research with recovering COVID-19 patients which can better inform current health practices as well as preparedness models for the future. Our paper investigates this further while presenting findings on multiple psychosocial health indicators that were self-reported by individuals who had been diagnosed with the virus and were in the process of recovery. The findings highlight lived experiences of the pandemic that can provide useful insights for health initiatives globally, as we continue to design effective rehabilitation for survivors of the virus.
Psychosocial and Mental Health Factors During Recovery
The necessary measure for prevention and treatment of COVID-19 entails a period of quarantine, which may include home-isolation, isolation in quarantine centers, or hospitalization in cases of escalated severity or comorbidities. Quarantine and isolation have been associated with negative psychological outcomes during COVID-19 as well as in previous outbreaks of communicable diseases like Severe Acute Respiratory Syndrome (SARS) and Ebola. Patients reported being irritable, fearful of transmission to other family members, lonely, frustrated, anxious, depressed, sleep-deprived, and showed signs of suicidal ideation and PTSD (Brooks et al., 2020; Jeong et al., 2016; Liu et al., 2012; Reynolds et al., 2007; Robertson et al., 2004). Recent studies investigating the current COVID-19 pandemic have found similar patterns of a widespread increase in mental health problems, as well as psychological fear-related responses (Amsalem et al., 2020). According to studies with the Chinese population in the initial months of the year 2020, the spread of this disease was associated with anxiety, depression, distress, sleep disturbances, and suicidality (Ornell et al., 2020; Qiu et al., 2020; Shigemura et al., 2020; Wang et al., 2020). Similar findings have been reported from other parts of the world corroborating the negative psychosocial health outcomes of the pandemic (Holman et al., 2020; O’Connor, Wetherall, et al., 2020). In an online survey of 1685 Indian respondents, Grover et al. (2020) found that the prevalence rates of depressive symptoms according to PHQ-9 (Patient Health Questionnaire) was 10.5% and anxiety according to the GAD-7 was 38.2%. The level of stress was found to be moderate for 74.1% of the respondents and 71.7% of respondents reported poor levels of well-being.
Of the several psychosocial correlates, one of the most widely reported has been anxiety and worry (Taquet et al., 2020). The fear of being infected as well as the levels of worry after being diagnosed have consistently been high across reports (Schimmenti et al. 2020). The nature of the disease, the fatality and uncertainty, the likelihood of infecting others, continued effects of the virus, confusing and contradicting evidence about the remission and resurgence of symptoms, possible stigma, and job-related uncertainties are all reasons for increased levels of worry (Bagcchi, 2020; Bhattacharya et al., 2020; Godlee, 2020). Though closely related, worry and anxiety are distinct psychological constructs, with worry implying a more cognitive state of overthinking about possible future outcomes, usually without immediate somatic symptomatology (Zebb & Beck, 1998). We therefore chose to measure levels of worry among the callers who were recovering from coronavirus as a general, non-psychiatric indicator of coping with their present circumstances.
Mood and affect states have also been associated with perceived threat from the pandemic and as an outcome of isolation (Pérez-Fuentes et al., 2020). However most of this literature has focused on a general population that was affected by pandemic related lockdown and we do not have adequate information on how mood states and levels of worry might shift in the period of recovery and post-recovery from the virus. It is also important to point out that while the immediate medical effects of the virus are believed to cease after about 14 days, this has not been a uniform experience (Balachandar et al., 2020). For instance, Lan et al. (2020) found in their case studies with four patients who had been diagnosed with the disease and had been cleared for discharge post-hospitalization, that they tested positive for the virus upto 13 days after discharge. Moreover, those who might not actively show symptoms, still have to live through the ongoing pandemic (and related lockdown), return to social and professional life, all of which could be anxiety producing and make them vulnerable to being stigmatized (Gupta et al., 2020)
COVID-19, with its high rates of contagion, has automatically become associated with social stigmatization, disproportionately affecting marginalized communities, similar to previous outbreaks like SARS and tuberculosis (Bhattacharya et al., 2020; Singh & Subedi, 2020; Siu, 2008; Villa et al., 2020). Speculations about refugees and immigrants being the source of this infection have also surfaced (Slater, 2020), with rising xenophobic attitudes toward Asians (Rzymski & Nowicki, 2020). Xu et al. (2021) document the discrimination toward Chinese speaking individuals in different parts of the world that have resulted in violent hate crimes, and highlight how stigma was deeply intertwined with political ideology, media framing, and racism. In India, domestic workers and daily wage laborers had their jobs discontinued indefinitely due to the fear of infection, causing them to go without pay for months. Losing jobs can exacerbate strife, adding to frustration, depression, and anguish (Subbaraman et al., 2014). When selected communities are stigmatized, they tend not to reveal their experience of symptoms and hide important medical and travel history which delays the reception of medical attention and increases the peril of virus transmission. The fear of infection and stigmatization in India has resulted in “health crimes” (Dubey et al., 2020) with instances of attacks on people for reporting probable cases with travel history, and violence toward health workers (Health team attacked in Indore during screening: India News, 2020; Thakur, 2020). Societal rejection during the quarantine period in the form of suspicion, discrimination, avoidance, prejudiced attitudes in the workplace, and social withdrawal from events and gatherings can have an acute psychological impact on the recovered patients (Brooks et al., 2020). Some studies from Australia and UK have suggested that the perceptions of social and financial changes are more significantly related to detrimental mental health effects when compared to the fear of catching the virus (Dawel et al., 2020; Holmes et al., 2020) Therefore, perceived social discrimination and non-reporting of symptoms amongst infected individuals and its relationship with their reported states of worry are important psychosocial factors that can highlight the lasting consequence of COVID-19. The disease-associated stigmatization of the survivors of the SARS outbreak in 2003 lasted years after their recovery and remarkably hampered the reinstatement of normal social life (Dubey et al., 2020; Lee et al., 2005; Person et al., 2004; Siu, 2008).
The pandemic in general and the quarantine period during recovery specifically, can bring about certain lifestyle changes. As positive compliance measures like handwashing and social distancing become mandatory for all, for those who are infected, they can hold particular significance. While many patients feel grateful for surviving the disease and may therefore adopt positive lifestyle changes, others feel extreme guilt for being carriers which could also lead to compliant behaviors (Dehkordi et al., 2020). People suffering from anxiety during their period of quarantine may adopt unwanted lifestyle changes like repeated sterilization, obsessive-compulsive handwashing, body temperature checks (Li et al., 2020), and severe dietary modifications that can hamper the recovery process (Banerjee, 2020). However, research with a Pakistani sample of recovering COVID-19 patients showed that lifestyle changes like adequate physical activity and sleep along with proper diet was positively associated with recovery rates (Rabail et al., 2021). Hence lifestyle changes can be a positive coping mechanism and have significant associations with worry and mood. Studies have also reported several protective factors that can alleviate COVID related worry and help in recovery. Social support from national agencies, the health care system, and its workers as well as from family and friends was found to positively affect mood among patients affected by the virus (Hao et al., 2020). Social support and resilience factors play an important role in the isolation and recovery periods and is negatively associated with anxiety (Labrague & De los Santos, 2020). Hence protective factors like perceived social support, availability of adequate mental and physical healthcare, and economic stability can be important determinants of stress in the recovery journey.
Overall, the COVID-19 outbreak poses many challenges for those infected and is capable of evoking an existential anxiety that threatens one’s accustomed identity and sense of place in the world (Peteet, 2020). While the scientific community has responded promptly to the crises with a rapidly growing body of research on COVID-19, there is still limited work documenting experiences of recovering patients and survivors of the virus (Olufadewa et al., 2020). Moreover much of the work with patients has focused on cases of acute illness or hospitalization, while not adequately covering the larger population who are infected but not hospitalized. In order to highlight the ongoing nature of the experience and the potential after effects of the disease, we specifically selected participants who were in the recovery phase (Dehkordi et al., 2020; Sun et al., 2021). The present study included participants who had completed the 14 days quarantine period at the time of the study, after being infected by the virus. The uncertainty of complete remission of the disease post-recovery and the unpredictability of a relapse can cause patients to experience indefinite stigmatization and discrimination. A study by Roy et al. (2020) found that when participants were questioned about the inclusion of recovered COVID-19 patients back in society, they reflected significant fear, apprehension, and possible stigma associated with their health condition. Therefore, going beyond the framework of assessing anxiety, depression, and related clinical outcomes of the COVID experience, we looked at psychosocial factors that are relevant to the lived experience of recovering individuals. Specifically, we examined levels of worry, current mood, perceived discrimination, reported social support, and lifestyle changes along with the willingness to donate plasma to help other patients. As Banerjee (2020) points out that the pandemic could have unique and complex implications in developing regions like South Asia with several constraints related to medical care, limited resources and high viral caseloads. This study would be particularly useful in adding to the much-needed understanding of psychosocial assistance and health policies in understudied contexts. It would also add to the wider literature on COVID-19 and previously identified research priority areas by focusing on individuals with lived experiences of the virus, understanding short and long terms mental health consequences and behavior change (O’Connor, Aggleton, et al., 2020).
Method
Study Overview
Due to the unprecedented nature of the pandemic several governmental and non-governmental organizations developed rapid action programs to address the growing anxiety and uncertainty across all sections of the Indian society. COVID Response team (consisting of three non-profit organizations working in the area of mental health) along with Governmental medical agencies came together to provide mental health assistance to residents of Delhi and the surrounding region (also called the National Capital Region or NCR). Residents called in via an open and free helpline to speak with trained counselors and discuss their fears and anxieties brought about by the pandemic, through the first few months of the lockdown. A second phase was initiated in July and August 2020, wherein counselors reached out to residents who had been diagnosed with COVID-19 with the help of a government database. These were recovered or recovering patients of COVID-19 who had been registered onto the database at the time of their testing and diagnosis. The main aim of this initiative was twofold- firstly this was a follow-up effort to provide mental health support to those who had been diagnosed with coronavirus and were presently recovering from the infection. Secondly, this was also a means of reaching out to seek assistance for the blood plasma donation drive that was being tried out as a potential safeguard against the virus at that time (COVID-19 Convalescent Plasma Donation, 2020). The data presented in this paper pertains to respondents who were contacted during the second phase of this initiative in the month of August 2020. The participants in this study did not partake in any of the previous phases
Participants
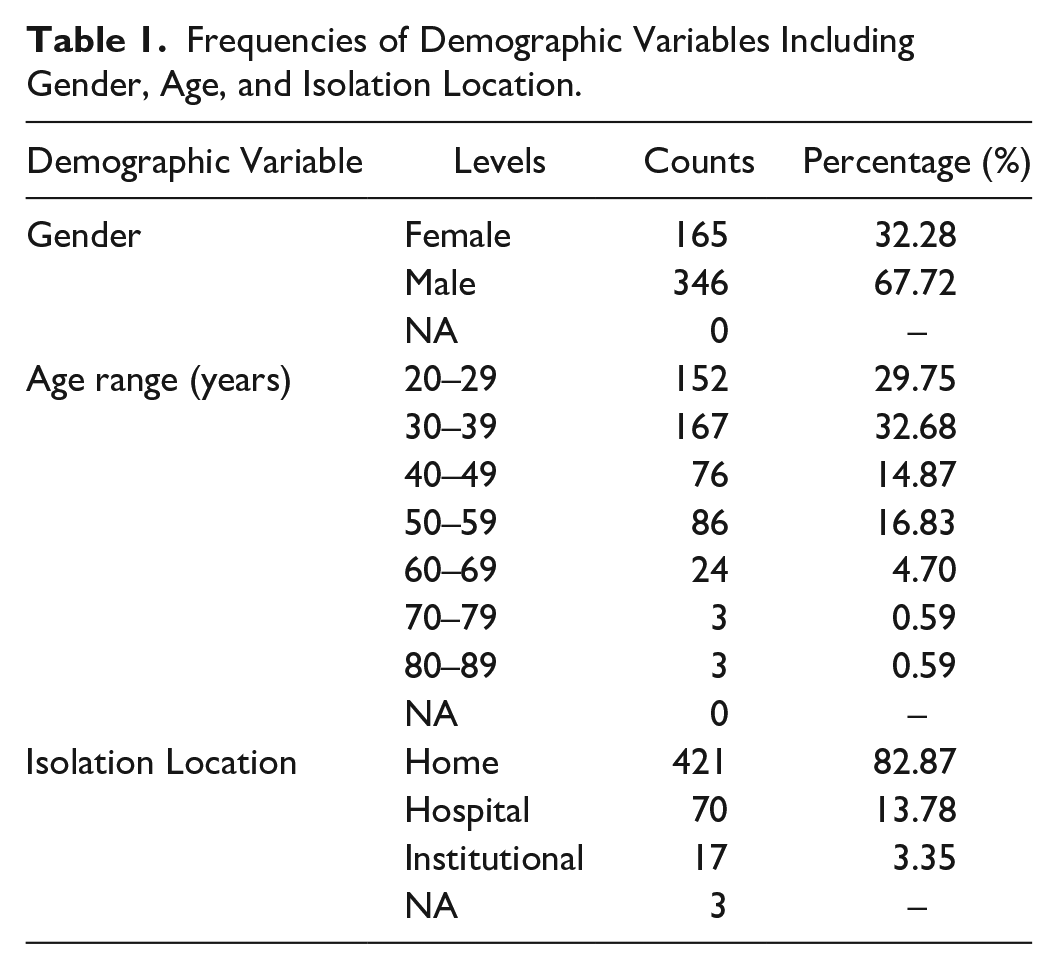
Participants were recruited through the telephonic helpline that was part of the COVID Response initiative. Through the months of July and August 2020, counselors reached out to residents who had tested positive for coronavirus and had been in either of the three types of quarantines (home, hospital, and non-medical institutions or special COVID care setups) as mandated by the Delhi Government. Data was collected from 707 patients who responded to the telephonic calls upto August 2020. After cleaning the dataset, a total of 511 participants’ data was included in this study. About 165 participants identified as female, while 346 were males. The age of participants ranged from 20 to 89 years, with a majority of participants being in the 20 to 39 age range. About 62% of the participants were in the age group ranging from 20 to 39 years. Of these 32% were in the age group of 40 to 59 years. Only 6% of the patients were above the age of 60 years. A majority of the participants (83%) had been in home isolation during the 14 days recovery period (Table 1).
Frequencies of Demographic Variables Including Gender, Age, and Isolation Location.
Materials
A comprehensive online survey was constructed using Google Forms to measure the relevant conditions. The measures were built on information collected previously through the same helpline, wherein callers responded to questions on mood, sleep patterns, and availability of support factors like medical care and family. The earlier survey was conducted with individuals from the general population and were not patients of COVID-19 specifically. We retained some of these measures and added new measures of worry and perceived discrimination for the second round of data collection (as reported here) with recovering participants. After collecting demographic information, we asked about the current mood of the caller. Mood was measured by presenting 10 options of mood states (McGuirk, 2012; Shacham, 1983) ranging from negative (helpless, stressed, and irritable) to positive (hopeful, relieved, and supported). We used one item to measure levels of worry, which was adopted from the state anxiety scale (Gosselin, 2013; Marteau & Bekker, 1992). This was modified to ask how worried the respondent felt at the time of the call when compared to the time of diagnosis. This was measured on a scale from 1 to 5, with 1 being no feelings of worry and 5 indicating high levels of worry. Sleep pattern post-recovery was measured by one item that asked respondents to report how comfortable their sleep was on a scale of 1 to 5, with 1 being not at all and 5 being very much. This was followed by another question on sleep that asked participants to indicate reasons for discomfort (nightmares, insomnia, physical changes through recovery, effects of medicines, etc). We asked about the respondent’s willingness to donate plasma (yes, no, and maybe), if yes then we recorded the reasons as well as any perceived risk factors in donation (pregnancy, substance use, diabetes, etc.). The next item enquired whether the participant had made any lifestyle changes (yes/no/prefer not to say), if yes then what kind of changes specifically (physical activity, meditation, eating healthier food, sleeping well, quitting smoking, and reduced consumption of alcohol). These options were derived from literature and phase I (as mentioned previously) and included as forced choice options for our survey. We asked about perceived discrimination with three questions (i) Did you face any discriminatory behavior post your diagnosis from your community or peers? (ii) Did you hide your diagnosis in order to avoid discomfort or discrimination from your community or peers? (iii) Did you observe any changes in people’s attitudes toward you post-recovery? We asked participants to report available protective factors with four options: (i) support of family and friends, (ii) availability of adequate medical care, (iii) mental health and emotional support, and (iv) financial stability. Lastly, the counselors did a quick mood check with the same list of mood states followed by conclusive remarks and follow up instructions before ending the call.
Procedure and Ethical Considerations
As this was a multi sectoral project including government and non-governmental agencies and designed as a time sensitive crises intervention initiative, an independent ethics committee was appointed to rapidly assess the program, in line with the WHO ethical standards for research in public emergencies (World Health Organization, 2020). The Ethics Review Committee, Mindpiper, consisting of senior psychiatrists and data experts approved the study (#CRMP0720SM). Based on data available from a centralized medial system, recovering COVID patients were identified. A general text message informing them of a mental health support initiative was circulated, and those who replied to the same were then contacted via telephone calls. Thus, participants consented to take part in the study by opting in. As the counselors spoke to participants, all ethical measures were followed and caution was taken to give full disclosure about the purpose of the call and the intent of the helpline. The form was in English and the counselors used both English and Hindi in their verbal communication with the callers. Verbal informed consent was taken after providing all relevant information regarding the purpose of the call and survey components. Following initial rapport building, counselors inquired about the topics covered in the online survey with particular focus on our five main psychosocial factors. The survey was distributed among counselors through Google Forms and took about ten to fifteen minutes to complete. However due to the nature of the assistance program and data collection by counselors while on the helpline call, it was kept completely voluntary and as less intrusive as possible. Data collection was designed keeping in mind the health status and possible related distress of the respondent, and the sensitive nature of some of the questions. Participants could choose to not respond to any question that caused discomfort.
Analysis
The data was sorted in Microsoft Excel and analyzed with the use of R programing language and statistical software. Worry and sleep pattern post-recovery were measured on a 5-point scale. Most of the measures were dummy coded as categorical variables corresponding to the options- Perceived discrimination was coded as 0, 1, and 2 for yes, no, and prefer not to say, respectively. Lifestyle change was coded with responses ranging between yes, no, and prefer not to say. Willingness to donate plasma was similarly coded across yes, no, and maybe/undecided. Lastly, there were four protective factors, namely support from family and friends, adequate medical care, emotional support or mental health assistance, and financial stability. Along with descriptives, we conducted one way ANOVA with an independent between subjects design, to identify the significant differences in levels of worry and sleep comfort, across participants who differed on their responses to lifestyle changes, protective factors, and willingness to donate plasma. As the data was collected through a survey and given the nature of questions, absolute assumptions of normality were violated. However, ANOVA is robust against violations of normality, and a suitable parametric test for interval data (Norman, 2010). Hence, it is appropriate to describe the categorical differences in means for our study. Post-hoc pairwise comparisons were performed when ANOVAs had significant differences with three or more levels of a factor. The Benjamini-Hochberg method was used for the adjusted p-values. We present and discuss the results in the following section.
Results
Descriptives
Table 2 includes the frequencies for all the psychosocial factors. Most participants (72%) reported positive mood outcomes in terms of current feelings. Common descriptors included relieved, satisfied. and supported. However, 16% of participants had negative feelings of anxiety, stress, and tension. About 12% reported mixed feelings, with many participants feeling relieved but also feeling tired or bored. Self-reported worry at the time of the call when compared to at the time of diagnosis was measured on a scale from 1 to 5, with 1 being no feelings of worry and 5 indicating high levels of worry. Most participants had lower feelings of worry post-recovery as compared to when they were diagnosed with coronavirus. About 36% of the patients reported no feelings of worry and 26% reported extremely low feelings of worry. Participants were asked to rate how comfortable their sleep was at present on a scale from 1 to 5, with 5 being extremely comfortable, to which 70% reported having comfortable sleep while 15% indicated discomfort in sleep. Common reasons for sleep disturbances included feeling nervous or worried, insomnia, and physical changes post coronavirus diagnosis.
Frequencies of Psychosocial Factors.
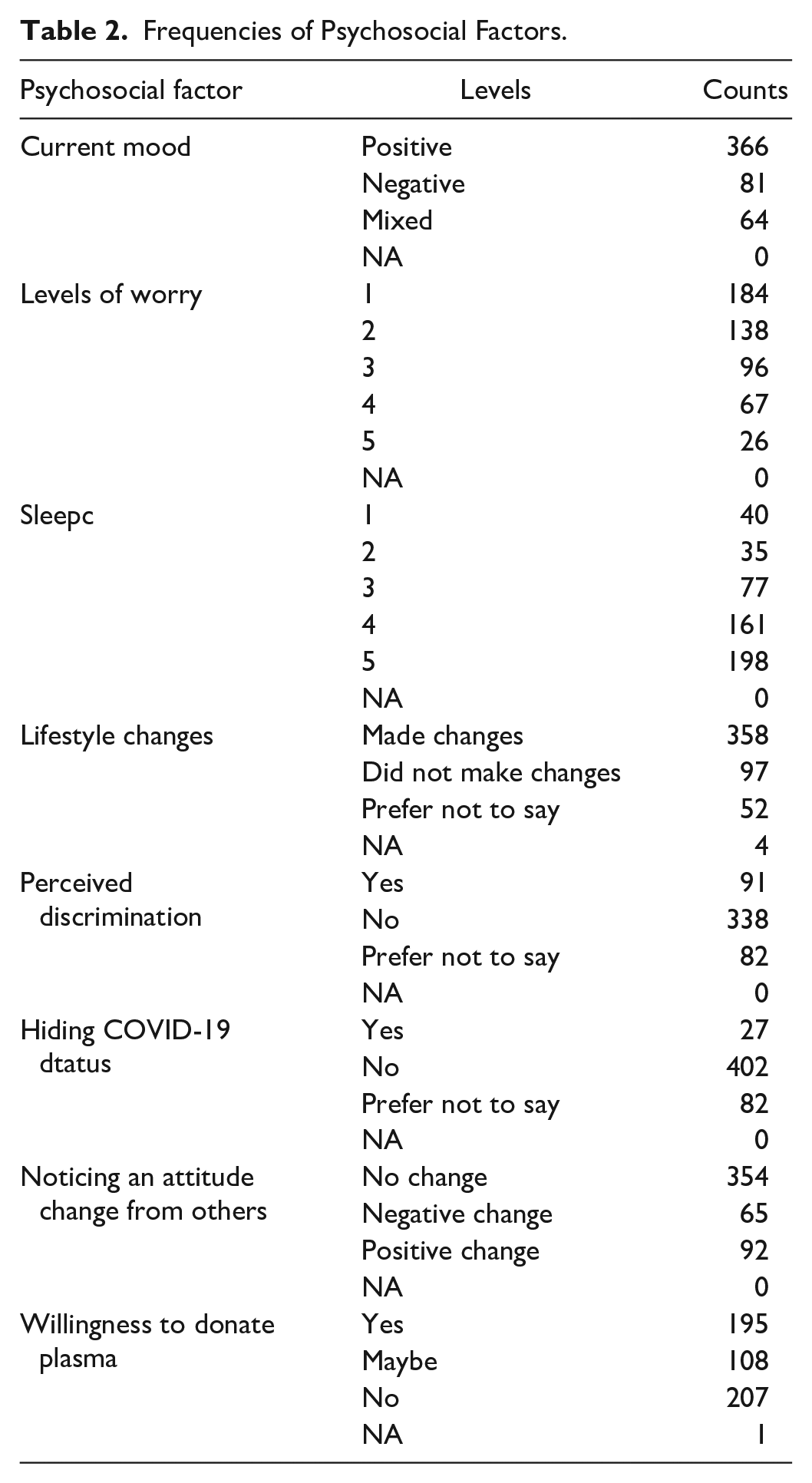
Eating healthier food and applying social distancing were among the highly reported lifestyle changes. Other major changes to everyday lifestyle adopted by participants post-recovery were avoiding public places, engaging in some form of physical activity, repeated hand washing, wearing protective masks, and staying at home. 19% of participants reported not having any major changes to their lifestyle, while 10% preferred not to answer the question. It is possible that some of them were already taking appropriate precautions and thus did not report any changes post-recovery. In order to understand the stigma associated with being infected with COVID-19, callers were asked about discriminatory behavior and people’s attitudes toward them. We observed that 66% of patients reported not facing any discriminatory behavior from their community and peers and only 18% reported facing some form of discriminatory behavior, while others preferred not to answer the question. In terms of people’s attitude toward them, no change was observed by 69% of the respondents. On the other hand, 18% reported a positive change and 13% reported a negative change in others’ attitudes post-recovery. Additionally, we observed that 79% of the respondents did not feel the need to hide their diagnosis from their community or peers in order to avoid any discomfort.
Reporting of protective factors can be viewed in Figure 1. A significant proportion of respondents (90%) reported having support from friends and family. Furthermore, 54% said that they had adequate medical care, 39% indicated emotional support and/or mental health care, and 32% reported having financial stability. While it is positive to know that many received the support of their family and friends, it is also important to note that only 54% had adequate medical care. This could not be investigated further due to the nature of the data collection but it would be interesting to investigate whether other forms of support were considered more important than adequate medical care when it came to coping with the virus.
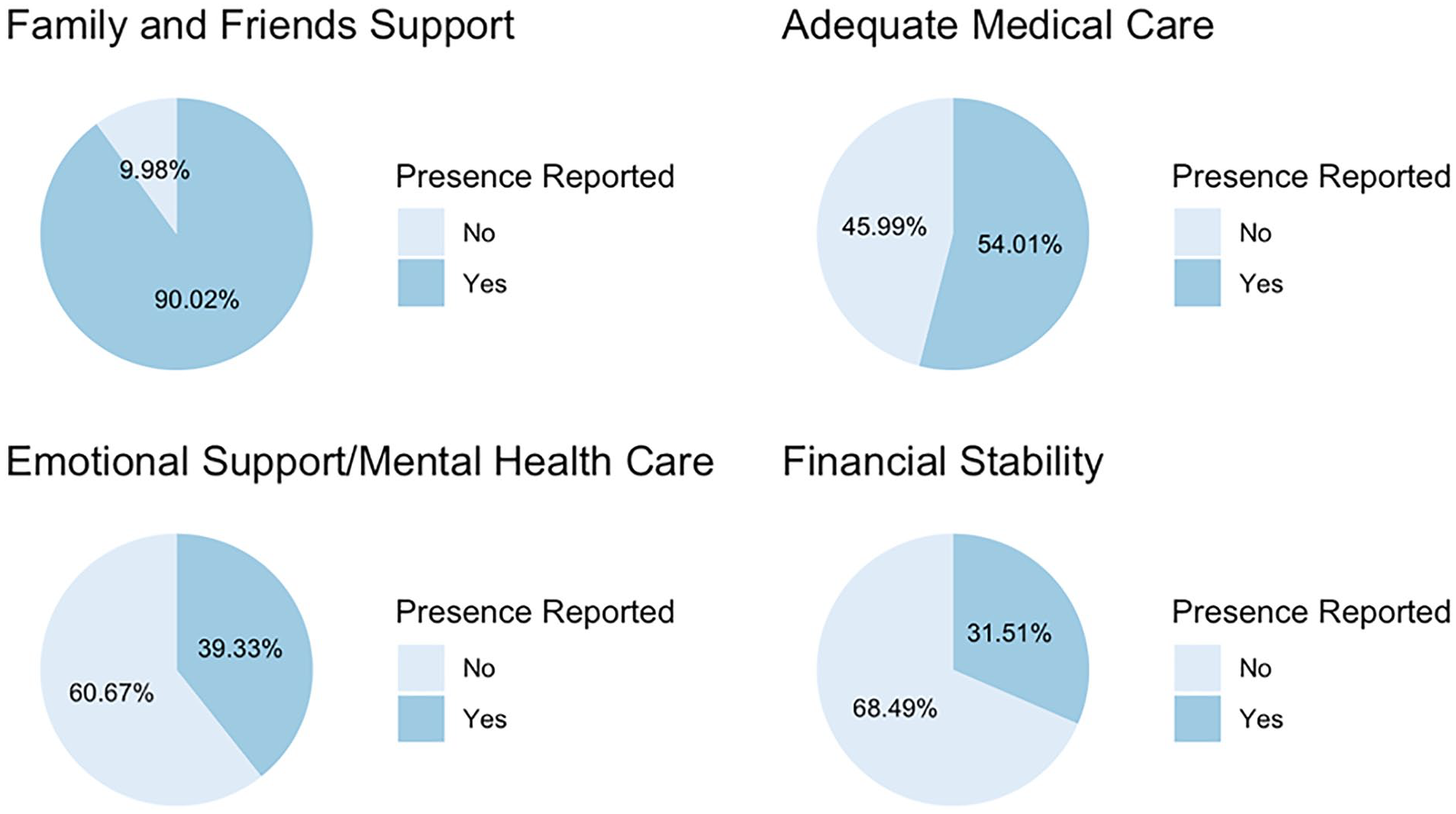
Protective factors reported by participants.
One of the factors explored in the survey was the willingness to donate plasma. Research suggests that those who have fully recovered from COVID-19 can donate their plasma to help currently ill patients as the convalescent plasma may contain antibodies for COVID-19 (Liu et al., 2020; Ye et al., 2020). Only participants who are eligible for general blood donation can donate convalescent plasma. This factor was included in the study due to Delhi Government’s emphasis on donation, particularly during the summer of 2020. However, looking into willingness to donate also provides insight into acts of prosocial behavior, particularly in the context of the pandemic. We observed two extremes to the responses when exploring willingness to donate plasma. While 41% were not willing to donate plasma, 38% were willing to donate. The rest of the participants were unsure and indicated “maybe” as their response. The major motivation behind the inclination toward donation was the desire to help other coronavirus patients to recover faster, reported by 76% of those willing to donate. Moreover, 41% of total participants reported health concerns that hindered their ability to donate, such as diabetes, pregnancy, and low weight. This finding should be held with much caution as the information on blood plasma donation was not always clear and this could have affected the overall attitude and willingness to donate. Moreover, as this medical option did not become widely popular and has since been selectively implemented nationally and internationally, we have not delved into the analysis of this measure in detail hereafter.
Participant’s reported age had a significant positive correlation with current mood, r(509) = .11, p = .01, willingness to donate plasma, r(508) = .26, p < .0001, and lifestyle changes, r(453) = −.11, p = .02. However, since the age distribution was highly skewed we did not explore it further. Results of ANOVA tests examining the relationship between levels of worry and other variables are reported below.
Determinants of Worry
Worry was found to significantly vary across gender, F(1, 509) = 11.43, p = .001. Figure 2 showcases that women (M = 2.50, SD = 1.17) reported significantly higher states of worry than men (M = 2.12, SD = 1.17).

Distribution of levels of worry and across gender.
As seen in Figure 3, reported feelings of worry significantly differed depending on the current mood during the time of the call, F(2, 508) = 42.68, p < .0001. Participants who reported a negative current mood (M = 3.25, SD = 1.14) had the highest levels of worry, followed by mixed feelings (M = 2.44, SD = 1.18), and positive mood (M = 1.99, SD = 1.11). Post hoc pairwise comparisons highlighted that all three mood groups significantly differed from each other.
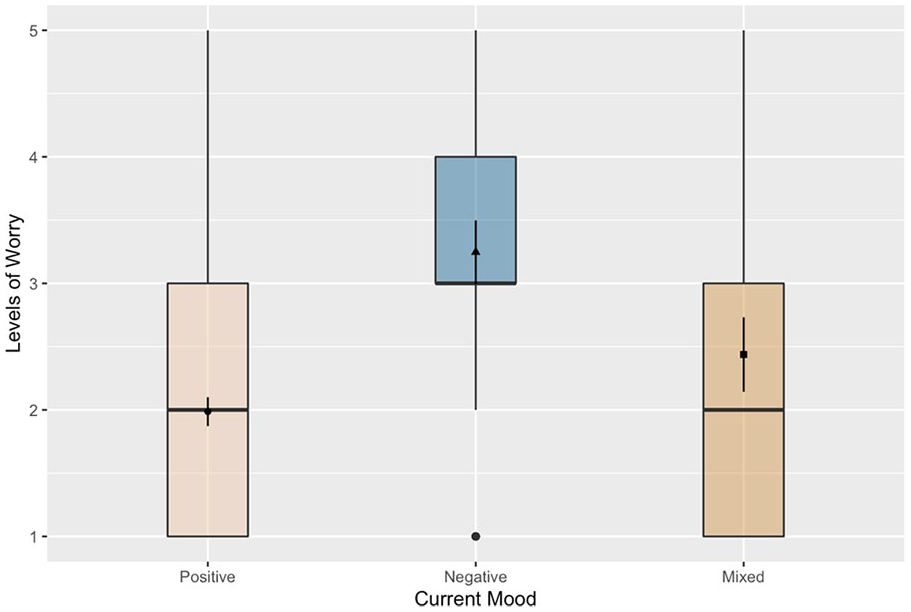
Distribution of levels of worry and current mood.
Levels of worry were also found to significantly differ when comparing those who made lifestyle changes after recovering from coronavirus to those who did not make any changes, F(2, 504) = 14.93, p < .0001. Participants who did not make any lifestyle changes (M = 1.72, SD = 1.01) reported significantly lower levels of worry than those who did (M = 2.32, SD = 1.22) and those who preferred not to answer (M = 2.75, SD = 1.23). This relationship between worry and lifestyle changes can be found in Figure 4. Lifestyle changes were also found to be linked with sleep comfort levels, F(2, 504) = 5.32, p = .005. Lower sleep comfort levels were reported by participants who indicated making lifestyle changes (M = 3.82, SD = 1.26) when compared to those who did not make any lifestyle changes (M = 4.22, SD = 1.08). The difference between those who did not make changes and those who preferred not to answer (M = 3.63, SD = 1.09) was also significant according to the post-hoc comparisons test. Figure 5 highlights that while the difference in sleep comfort was found to be significantly different between the two groups, it is important to note that both groups reported fairly high levels of comfort.
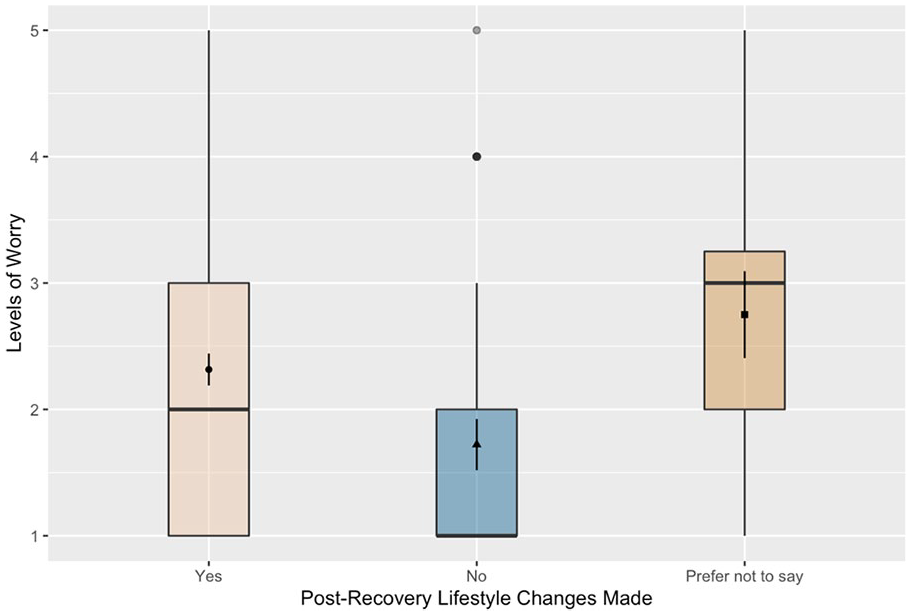
Distribution of levels of worry and lifestyle changes.

Distribution of sleep comfort and lifestyle changes.
Figure 6 showcases that worry also significantly differed depending on perceived discrimination reported by the respondents, F(2, 508) = 14.14, p < .0001. Pairwise comparisons highlighted that those who preferred not to answer (M = 2.89, SD = 1.14) the question on discrimination had significantly higher levels of worry than those who answered yes (M = 2.16, SD = 1.22) and those who answered no (M = 2.11, SD = 1.18).

Distribution of levels of worry and perceived discrimination faced.
Among protective factors, levels of worry significantly differed when comparing those who reported having adequate medical care and those who did not, F(1, 508) = 5.07, p = .02. Participants who stated adequate medical care as a protective factor (M = 2.13, SD = 1.19) reported lower levels of worry than those who did not report adequate medical care (M = 2.38, SD = 1.23), as seen in Figure 7. Reported levels of worry differed significantly (F(2,507) = 14.56, p < .001) between those who were willing to donate plasma (M = 1.98, SD = 1.13) and those who were not (M = 2.58, SD = 1.27). According to post hoc pairwise comparisons, there was also a significant difference between those who were not willing to donate and those who were unsure/undecided (M = 2.07, SD = 1.09). These findings can be seen in Figure 8 and indicate those who were less worried were more willing to donate plasma when compared to those who indicated higher levels of worry. However, it is important to note that overall levels of worry were quite low (M = 2.24, SD = 1.22).

Distribution of levels of worry andadequate medical care.

Distribution of levels of worry and willingness to donate plasma.
Discussion
This study attempted to add to the relatively less explored literature on recovering from COVID-19 and focused on psychosocial correlates beyond pathological diagnostic categories (Olufadewa et al., 2020). Given the proliferation of COVID-19 in everyday life and the high rates of infection, it was important to investigate psychosocial attributes that are overlooked in distress research focusing on clinical measures of anxiety, depression, and the like (Cai et al., 2020). Findings highlight several indicators of the recovery journey which can inform mental health assistance and rehabilitation initiatives.
Recovery and Levels of Worry
Meta-analytic reports have now underlined high rates of pandemic related anxiety and worry globally (Salari et al., 2020). Yet, our findings showed that self-reported worry during recovery was lower than at the time of diagnosis, with majority participants reporting positive mood. This indicates a positive shift toward a more relieved and relaxed mental state, possibly because the uncertainty and fear of contracting the virus and its potential threat was already out of the way, corroborating findings from other contexts (Pérez-Fuentes et al., 2020). Sun et al. (2021) reported a similar trend among recovering patients where initial feelings of fear, distress, rejection, and anxiety were replaced by calmness, resilience, and gratitude through the recovery phase. Additionally, most of the participants for this study had been in home isolation, thereby indicating less severe COVID symptoms, which could also be related to lower rates of worry. However, this is an important finding which adds to the overall picture on COVID recovery, by representing patients who do not experience acute symptoms and therefore hospitalization, which is often the case in regions with limited medical resources and high viral caseloads (Bhadoria et al., 2020).
Adding to meta-analytic findings from studies with the general population, women were found to be more worried post-recovery (Kowal et al., 2020; Salari et al., 2020). Worry was also associated with current mood with those indicating positive mood showing lower levels of worry. This is not surprising given that affect states are usually correlated with worry and stress in general (McLaughlin et al., 2007) and specifically with respect to the pandemic. Pérez-Fuentes et al. (2020) reported a similar pattern of anticipatory stress from threat of the virus which was closely related to negative affect states which further predicted irritation and apprehension. A rapidly growing body of research has highlighted the debilitating consequences of the ongoing pandemic. Yet, these preliminary indicators of a self-reported sense of coping, among recovering COVID patients is a significant finding that adds to the understanding of resilience to this disaster. Much of the anxiety around the virus could be related to the fear of infection and anticipated threat from the virus, and sustained mental health follow-ups can add to this naturally occurring post disease growth.
Lifestyle changes and related worry
An interesting finding was that levels of worry differed significantly across participants who reported making lifestyle changes during and after their recovery. Those who made these changes seemed to be more worried than those who did not. Making lifestyle changes was also associated with sleep post-recovery, with those who reported lifestyle changes also indicating poorer sleep. This has been reported previously by Solomou and Constantinidou (2020) who found a similar pattern of increased anxiety associated with following personal hygiene measures and health precautions concerning the pandemic. A certain degree of worry about contracting the disease again or infecting others could be related to following precautionary measures and making positive lifestyle changes more thoroughly. This may not be a bad thing, since a certain level of concern can motivate people to follow health protocols (Siebenhaar et al., 2020). However, compliance messaging and health intervention programs need to consider that recovered patients or survivors of COVID-19 may be overburdened with a sense of worry which could drive their lifestyle changes (Olufadewa et al., 2020). Worrying during the spread of an infectious disease can mediate the relationship between information seeking and compliance to safety protocols (Liu, 2020). While compliance to protocols is essential during a pandemic, our findings highlight the need to convey clear information and a sense of support and confidence in compliance messages, which could encourage healthy lifestyle changes but help alleviate related stress and worry. Our findings are supported by Harper et al. (2020) who report a similar functional nature of negative emotions like “fear” that can facilitate compliant behaviors and thereby challenge the psychopathological diagnostic approach to understanding COVID related distress. Yet the authors caution mental health professionals to be mindful of these negative affective responses that can lead to excessive and maladaptive behavioral changes.
Social support and worry
Perceived support from friends and family was significantly associated with positive mood at the time of the call. Social support is an essential component of positive recovery, which has gained new meaning in the world of COVID-19. The pandemic has created stressful situations of isolation, loneliness and fear of contagion, which further exacerbates anxiety, depression, and other mental health concerns (Coelho et al., 2020). During the lockdown, people felt the need to talk to others and share their concerns, thus emphasizing the need to reach out to systems of social support (Roy et al., 2020). Therefore, having the support of friends and family and being connected to them seems to be particularly integral to the recovery process (Sun et al., 2021).
Availability of adequate medical care was a significant factor in the differing levels of worry, with those who had medical care showing lower levels of worry. General health anxiety is correlated with anxiety around the virus and there has been a reported fear around inadequate and overrun medical facilities (Coelho et al., 2020; Thombs et al., 2020). Our findings highlight that the availability of medical support is a relevant and significant protective factor associated with reduced levels of worry among recovering coronavirus patients. Wang et al. (2020) similarly reported that confidence in doctors’ abilities to diagnose and treat the virus as well as satisfaction with health information were significantly related to lower levels of depression and anxiety among survey participants in China. Healthcare, especially during an ongoing pandemic, is effective when it is sustained and accessible (“COVID-19 showed us. . .”, 2020; Associated Press, 2020). Those who have recovered from the disease continue to live through the pandemic and therefore need the assurance of sustained care to relieve anxiety and ensure coping.
Worry and plasma donation
We also found that those who were more worried were less willing to donate plasma. Our results support previous findings that anxiety is a common theme in non-donors’ accounts of why they do not donate blood (McVittie et al., 2006). Additionally, most of the respondents who were willing to donate reported their reason as wanting to help other COVID positive patients. Prosocial motivations have been found to be a frequently self-reported factor in relation to reasons for blood donation in general (Bednall & Bove, 2011). Pandemics often create a sense of shared fate and suffering, which can accentuate prosocial behaviors toward others in the community, particularly toward those who are perceived to be going through the same experience (Van Bavel et al., 2020). Our findings are in line with this assumption. Varma et al. (2020) has also found that prosocial behavior led to greater positive affect and social connectedness during the pandemic. However, some studies have reported that prosocial behaviors during the pandemic are associated with heightened anxiety among adolescents (Alvis et al., 2020). Moreover, it is to be noted that almost the same number of respondents were unwilling to donate as those who were willing. This could be largely due to health concerns as 41% of participants reported risk factors such as diabetes, hyperthyroidism, and pregnancy that would make them ineligible to donate plasma. The lack of clear information on the blood plasma program and the general fear regarding blood donation could also be contributing factors.
Limitations of the study
There were several limitations to this study. Firstly, the participant pool was restricted to those who responded to the calls and were available and willing to interact. This eliminated many individuals who had been infected and were not contacted in the process resulting in a highly skewed sample in terms of age and gender (mostly between the ages of 20 and 60 and men). Nonetheless, since the program was in affiliation with Government medical agencies, we were able to reach out to participants (socio-demographically marginalized) who would otherwise not have access to mental health care services, and potentially be excluded from similar research. Thus, we were able to navigate issues with underrepresentation of disadvantaged groups in COVID-19 intervention and research (Gill et al., 2021; Lackland et al., 2020). Secondly, as this was an intervention based real-time data collection process, the forms were filled by counselors based on their telephonic conversations with participants, responding to the counselors instead of directly self-reporting. This is not ideal, but was the only way to reach a diverse population of COVID-19 patients in and around Delhi. Lastly, the multiple answer format preferred by counselors was prioritized instead of scaled measures and we followed an exploratory design to accommodate a wide range of potential factors and opinions, which may have restricted the analysis beyond preliminary correlations. As the calls were also meant to be follow up mental health checks, counselors were aware that intrusive or demanding scales would not be appropriate. We hope that some of the preliminary findings presented here can be taken up for further research on assistance and intervention for recovery from coronavirus.
Conclusion
We as a global community are in the process of coping with and recovering from the unprecedented effects of COVID-19. Those who were directly affected by the virus have been susceptible to anxiety, stigma, and a sustained state of uncertainty. Our findings highlight some of the complex, yet positive, psychosocial indicators among recovering patients of COVID-19. While levels of worry seem to decline, the necessity of sustained medical care, the importance of lifestyle changes that continue to have an association with worry, and the relationships between social support and mood, indicate the complicated nature of recovery from this novel disease. The findings can inform mental health programs for immediate as well long-term recovery from COVID-19. Beyond mental health implications, our findings are also aligned with general policy suggestions for an informed transition to recovery from the pandemic. We emphasize the need to share information internationally and investigate the effects of the virus from a multi-sectoral and multidisciplinary approach that will enable us to be more prepared for similar future occurrences (Balachandar, et al., 2020; Fakhruddin et al., 2020). We want to highlight that recovering from the disease but living through the pandemic, can create many complex and contradicting psychosocial conditions; making positive lifestyle changes while also feeling a sense of worry, identifying or reporting discrimination and experiencing related worry, and so on. Yet, protective factors like medical care and support of friends and family are significantly related to lower levels of worry and positive mood respectively, thereby emphasizing the importance of sustained institutional and social support during and after recovery.
Footnotes
Acknowledgements
First and foremost, we would like to extend our sincere gratitude to the COVID Response team, a non-profit initiative providing free mental health support via helplines. The team was formed promptly by the coming together of several individual stakeholders with initiation from Mind Piper and supported by I Am Wellbeing, Sahay by SOCHARA, Project StepOne, TYCIA Foundation, and ACT Grants. We would like to thank Rajiv Agarwal, Ramni Kaushik, and Tamanna Edwards from Mind Piper; Akanksha Chandele, Akshita Dutta, and Pallavi Singh from I Am Wellbeing; Abu Huraira Shaikh from Sahay by SOCHARA; Arun Patre and T.S. Raghavendra Prasad from Project StepOne; Tabish Bilal and Eleena George from TYCIA Foundation; and Chirag Gandhi, Shrrinesh Balasubramanian, Bhavin P. Chhaya, Rahul Garg, and Venu Nair from ACT Grants. The counselors of the COVID Response team played a crucial role in data collection as well as in providing prompt assistance when required. The counselors’ commitment to helping others reflects a real desire to improve mental health outcomes in light of the COVID-19 pandemic, through the support provided in the calls and through our subsequent research. We are truly grateful for their involvement in the data collection process. Lastly we would like to acknowledge the contribution of Saransh Ahuja and other research interns who aided with data cleaning and analysis in the preliminary stages.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The mental health intervention by COVID Response was funded by ACT (Action COVID-19 Team) Grants, and a micro grant was received from Peace First.
Ethics Statement
The Ethics Review Committee, Mindpiper, consisting of senior psychiatrists and data experts approved the study (#CRMP0720SM) in line with the WHO ethical standards for research in public emergencies. To maintain optimal standards of data privacy and confidentiality, each counselor signed a non-disclosure, privacy, and confidentiality agreement. Additionally, the software and tools used for the intervention were compliant with the ethical standards and privacy agreement of the Delhi Government. No user details were shared, unless there was an emergency situation or a possibility of harm to the client or others.