
Abstract
This article addresses the assumption that pathways to recovery from substance abuse and dependence, and the language used to define one’s relationship to substances, translate to actual beliefs and behaviors in terms of substance use. We draw on social representation theory and use data from a large web-based study (N = 9,341) whose goal was to understand how individuals in recovery define what recovery means to them. We often hear people say that they are “in recovery,” and present findings now provide empirical evidence of the prevalent meanings of this ubiquitous expression. The belief that recovery is abstinence was broadly held in our sample, especially among those exposed to treatment and 12-step self-help groups and who define themselves as in recovery—and most (but not all) of such individuals are complete abstainers (no alcohol or drugs). In contrast, among the “self-changers” who did not attend treatment or self-help groups, the most common self-definition was used to have an alcohol or drug problem but don’t any more, half of whom believe that recovery is abstinence while half do not, and only one third are abstainers. Findings are of public health relevance, as it is estimated that among American adults alone, 10% report having had alcohol or drug problems but no longer do. In line with the central concepts of social representation theory, people’s pathways to recovery have a strong effect on how they define themselves and their behaviors and beliefs, but it is not universal.
Keywords
Introduction
This article addresses the assumption that pathways to recovery from substance abuse and dependence translate to actual beliefs and behaviors in terms of substance use. Our conceptual framework draws on social representation theory to guide our hypotheses. We use data from a large web-based study (N = 9,341) whose goal was to understand how individuals in recovery define what recovery means to them.
Social Representation Theory
Social representation theory is a comprehensive social-psychological theory of how concepts, ideas, beliefs, and knowledge are developed and transmitted within a social unit through communication and language (Moscovici, 2001). Briefly, social representation theory shows (a) how collectives such as groups, organizations, social networks, or societies develop and transmit concepts, beliefs, and knowledge to individuals who interact and communicate within them; (b) how individuals’ language, ideas, and knowledge are shaped by what they learn from communicating within these collectives; and (c) how individuals’ language and behavior are also influenced by non-logical and other factors (Moscovici, 2001). We draw on this theory selectively, as we conceptualize how the dominant collectives of relevance to substance abuse have developed in the United States and given rise to specific language that, in turn, is learned and internalized by the participants.
The collectives of interest here include the dominant pathways to recovery: formal substance abuse treatment programs, informal 12-step self-help groups, other addiction self-help groups, and self-changers (i.e., no help-seeking). The language we consider is derived from the terms that these collectives historically used to describe their participants, their beliefs, and their prescribed behaviors. The U.S. policies and practices related to substance abuse primarily follow a disease model, which is abstinence-oriented; under this paradigm, alcoholics are seen as permanently lacking the ability to control their drinking once they take a drink, so that lifelong abstinence is recommended. In contrast, many European countries follow harm reduction policies that emphasize the controlled use of substances to minimize the negative consequences of unsafe alcohol or drug use (European Monitoring Centre for Drugs and Drug Addiction, 2011), and this approach has been adapted in a small way in the United States as well. Thus, we begin with a brief description of the development of the concept of recovery and the centrality of abstinence as they historically unfolded in the United States, to illustrate how the “social representation” of recovery and abstinence are used now by various pathways to recovery. We then present our hypotheses about the linkages between pathways to recovery, language to self-define one’s recovery status, beliefs about abstinence, and one’s actual substance use behavior.
The Development of the “Social Representation” of Recovery and Abstinence in the United States
“Recovery” from substance abuse specific language can be traced to Alcoholics Anonymous (AA), the 12-step self-help group founded in 1935—a time when there was little or no organized professionalized interest in alcoholism, and alcoholics were seen by many in the medical profession as hopeless. The major text of AA referred to abstinence from alcohol as necessary but insufficient for long-term recovery, which also required a new spiritual “way of living” (Alcoholics Anonymous: The Story of How Many Thousands of Men and Women Have Recovered, 1939, p. 97). AA gradually developed many local groups and members (Kurtz, 1979).
In 1949, physicians in Minnesota integrated 12-step recovery ideas from AA into a professionally based, abstinence-oriented alcohol treatment program called Hazelden (see McElrath, 1987). Their approach became known as the Minnesota Model and spread throughout the United States. Its growth was reinforced by the American Medical Association’s decision in 1956 to redefine alcoholism as a primary disease that needed to be treated, which in turn led to treatment being reimbursable by health insurance. By the 1980s, the majority of professional substance abuse treatment programs in the United States utilized 12-step AA ideas and practices, were abstinence-based, and sent their patients to AA meetings during treatment and as a form of aftercare (Brigham, 2003). However, a minority of alternative, non-abstinence-based treatment programs do exist in the United States—such as medication-assisted approaches (giving prescribed drugs to reduce craving, for instance) or harm reduction (initially introduced to treat injection drug users). Individuals following such approaches are less likely to embrace 12-step language to describe their status, instead seeing themselves, respectively, as in medication-assisted recovery or as having had an alcohol or drug problem.
AA ideas and practices also diffused to the larger general culture in the United States—depicted in movies, television shows, novels, and so on, to the extent that the image of a member speaking at a self-help group meeting is well known in this country: “My name is Bill and I’m an alcoholic,” says the member to his peers sitting in front of him in a circle. Furthermore, more than 90 other 12-step self-help groups have imitated AA’s model both for substance use addiction (such as Cocaine Anonymous or Marijuana Anonymous) and other problems such as gambling (Gamblers Anonymous) or sex addiction (Sex Addicts Anonymous; see White & Madara, 1995). Thus, the concepts of abstinence and recovery as used by 12-step self-help groups became widely known in the general U.S. culture.
Beginning in the 1980s, alternative non-12-step self-help groups developed in reaction to AA’s emphasis on spirituality and other aspects (such as its concept of powerlessness, which was interpreted as unwise for women to embrace). The popular non-12-step groups for substance use problems are Women for Sobriety (WFS), Rational Recovery that became Smart Recovery, and Secular Organizations for Sobriety with its offshoot LifeRing (see Humphreys, 2004). These groups also espoused abstinence and used the term recovery.
Finally, not all individuals solve their alcohol or drug problems with professional treatment or support from self-help groups (Dawson, Grant, Stinson, Chou, et al., 2005/2006). This is described in the literature as “spontaneous remission” (Smart, 1975), “healed” (Abt Associates Inc. & Heart Research Associates, 2010), or “natural recovery” (Sobell, Ellingstad, & Sobell, 2000), which we denote here simply as “no help-seeking.”
Hypotheses
Our conceptual model aims to partially explain the relationship between the key pathways to recovery and current abstinence status (Figure 1). We posit that pathways relate both to self-definition and to beliefs about abstinence belonging in one’s recovery definition, and that self-definition is associated with these beliefs. These self-definitions and beliefs dictate current abstinence status. The pathways we consider are exposure to 12-step groups, to treatment, to non-12-step groups, and to no help-seeking (“natural recovery”). The self-definitions involved here are in recovery, recovered, in medication-assisted recovery, and used to have an alcohol or drug problem but don’t now. The key hypotheses to be tested statistically are as follows:

Explaining the relationship between recovery pathways and substance use behavior.
Per social representation theory, treatment graduates, 12-step members, and those attending non-12-step support groups have been exposed to strong messages about abstinence and will have adopted the language of recovery; thus, they will say they are “in recovery” or “recovered.” Social representation theory would hold that this language plays a role in shaping beliefs and behavior, specifically, the belief that recovery involves abstinence and the behavior of total abstinence from alcohol and drugs. We thus hypothesized that exposure to treatment, exposure to 12-step and non-12-step support groups, and use of the terms in recovery or recovered to signal one’s status regarding alcohol and drug use, each will be associated with abstinence beliefs and behaviors. However, we did not expect a perfect match. For example, not all treatment graduates or 12-step exposed individuals will have embraced the view that total abstinence is required (Dawson, Grant, Stinson, & Chou, 2006); they may have attended one of the non-abstinence-oriented programs, or they felt the message they received at an abstinence-based program or at AA was not a good match for their situation. In social representation theory, this could be understood as either a bias or predisposition against abstention.
It is less clear how those who do not seek help, or those using language other than in recovery or recovered as their self-definition, feel about the inclusion of abstinence in their beliefs and behaviors about recovery. For example, the broad literature on natural recovery variously designates non-help-seekers as having “remitted” from a substance abuse or dependence diagnosis, as having reduced their substance use to “moderate” levels and/or as having achieved abstinence. Similarly, those “in medication-assisted recovery” could be taking prescribed anti-craving medications (like naltrexone) to help them reduce their alcohol or drug use, or take drugs like antabuse or methadone to help them abstain. We expected soft endorsement of abstinence beliefs and behaviors among the non-help-seekers compared with the help-seekers and those who self-define as “in medication-assisted recovery.”
Finally, there are those who do not use any derivations from the term recovery as their self-definition and instead say that they used to have a problem but don’t now. Because they eschew the popular language of recovery, we hypothesized quite weak levels both for the belief that recovery is abstinence and for current abstention.
Method
Sample
The 15-min online survey was available on the web from July 16 to October 31, 2012 (final N = 9,341). To recruit a heterogeneous sample that would reflect the diversity of pathways to (and individuals in) recovery, intensive and diverse outreach methods were used. This included partnering with 59 regional and national recovery organizations (listed on the study website at http://www.WhatIsRecovery.org), attending September Recovery Month events across the country, and posting announcements about the study throughout the recruitment periods in Craigslist, recovery magazines and radio programs, newspaper health sections, and so on. Sample ads, emails, articles, and fliers were made available to more than 400 formal and informal research partners. For a more complete description, see Subbaraman, Laudet, Ritter, Stunz, and Kaskutas (in press).
Measures
The online web survey tool, Survey Gizmo, was used to create the instrument. The study was approved by the Institutional Review Board at the Public Health Institute, Oakland, CA. Respondents first completed informed consent screens; responses were anonymous and confidential.
Questions analyzed here from the web-based survey focus on pathways to recovery, self-definition, beliefs about abstinence in recovery, and current substance use behavior. Other variables that describe the sample are shown in Table 1 and include demographics, substance use history, and recovery history.
Sample Characteristics (N = 9,341).
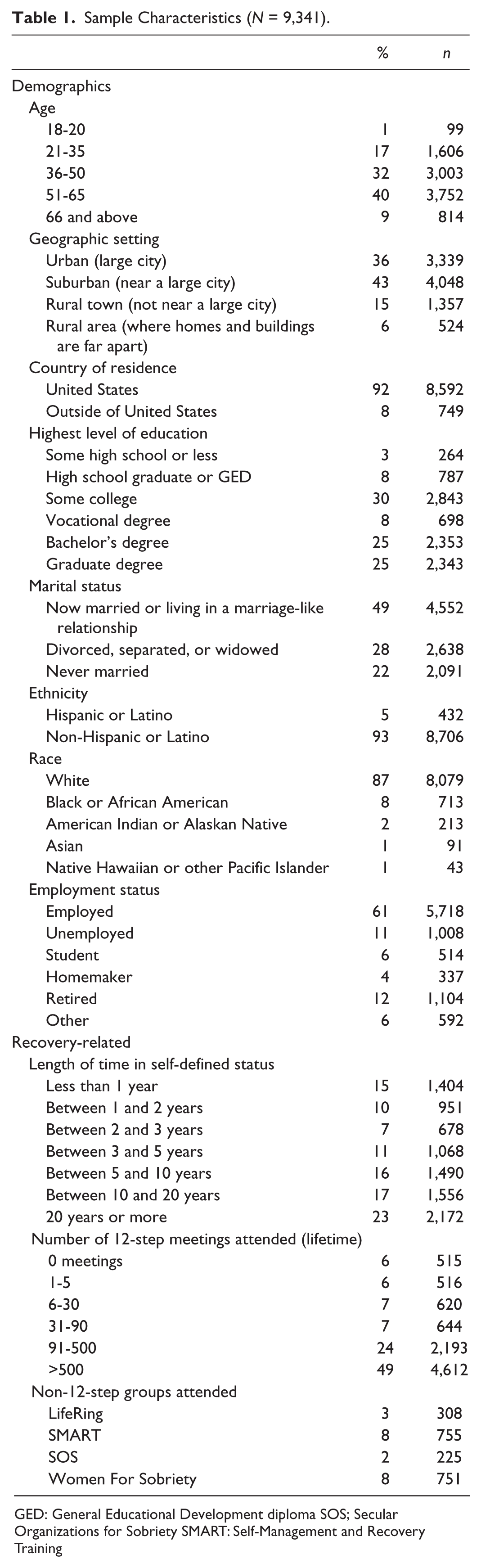
GED: General Educational Development diploma SOS; Secular Organizations for Sobriety SMART: Self-Management and Recovery Training
To measure respondents’ help-seeking pathways to recovery, we asked whether they had attended treatment, which specific 12-step groups they had attended (AA, Narcotics Anonymous, Cocaine Anonymous, Marijuana Anonymous, and Methamphetamine Anonymous), and which specific popular non-12-step groups had they attended (LifeRing, SMART Recovery, SOS, WFS). For analysis, we created indicator variables indicative of exposure to 12-step groups, to non-12-step groups, and to treatment, as well as an indicator to capture no help-seeking (“natural recovery”: no treatment, 12-step, or non-12-step group exposure).
To assess self-definition, we asked “which category best describes how you define yourself now, with respect to your prior alcohol or drug use: in recovery, recovered, used to have an alcohol or drug problem but don’t any more, or in medication-assisted recovery.”
To measure respondents’ beliefs about substance use in recovery, we asked, which of the following statements most closely matches your personal definition of recovery in terms of substance use: (1) no use of any substance—drug or alcohol, (2) no use of any substance—drug or alcohol—except as prescribed by your doctor, (3) no use of substance of choice but some use of other substances, (4) moderate or controlled use of any substance—drug or alcohol, (5) moderate or controlled use of alcohol, or (6) moderate or controlled use of drugs.
From these responses, we created a two-category beliefs variable reflecting the belief that recovery is abstinence (categories 1 and 2 above) versus not (any other category).
Using their answer to the self-definition question, we then asked respondents “how long have you considered yourself to be in recovery/recovered/used to have a problem/in medication-assisted recovery”; seven time categories were offered, anchored by less than 1 year and 20 years or more.
Current substance use was assessed for alcohol and drugs separately: For alcohol, we asked, “which category best describes your drinking status?” There were 16 possible categories: (a) never drank alcohol, (b) still drinking alcoholic beverages, (c) sober (seven timeframes: less than a year, a year but less than 2 years, 2 years but less than 3 years, 3 years but less than 5 years, 5 years but less than 10 years, 10 years but less than 20 years, 20 years or more), (d) moderate or controlled use of alcohol (seven timeframes, as in (c) above). For drug use, we asked, “which category best describes your drug use? By ‘drug use,’ we mean taking drugs that were not prescribed to you OR taking prescribed drugs more than directed?” There were nine categories: never took any drugs like that, still taking some drugs like that, quit taking drugs like that (seven timeframes, as in (c) above). From these two questions about alcohol and drug use, we computed a dichotomous measure of composite current substance use: abstains from alcohol and drugs (never drank alcohol or sober, and never took any drugs like that or quit taking drugs like that) versus does not abstain from alcohol or drugs (any other response).
Analysis
SPSS version 19 was used. Cross-tabulations were conducted, and chi-square tests of significance were reported. No specific pairwise comparisons were done. When studying relationships with recovery pathways, we conducted four separate chi-square tests for each of the dichotomized pathway variables (exposed to 12-step groups, yes/no; exposed to treatment, yes/no; exposed to non-12-step groups, yes/no; and no help-seeking, yes/no), which allowed us to compare the pattern of responses for those having taken a particular pathway with those not having taken that pathway. In contrast, a single four-category variable was used when studying relationships with respondents’ self-definition (in recovery/recovered/in medication-assisted recovery/used to have a problem but don’t now), so that we could determine whether there was a statistically significant relationship between the self-definition variable and another variable of interest (such as belief or behavior); thus, we did not statistically compare those who consider themselves to be in recovery with those who say they are recovered, and so on.
Specifically, four separate chi-square tests were conducted to study the relationships between each of the four recovery pathways and the single four-category self-definition variable (Table 2), the dichotomous belief variable (Table 3), and the dichotomous behavior variable (Table 7). Single chi-square tests were conducted to study the relationships between the four-category self-definition variable, the dichotomous belief variable (Table 4), and the dichotomous behavior variable (Table 5). To study how beliefs relate to behavior, we conducted a single chi-square test between the dichotomous belief variable and the dichotomous behavior variable (Table 6).
Self-Definition Based on Recovery Pathway: Proportion in Each Pathway Using Each of Four Self-Labels.
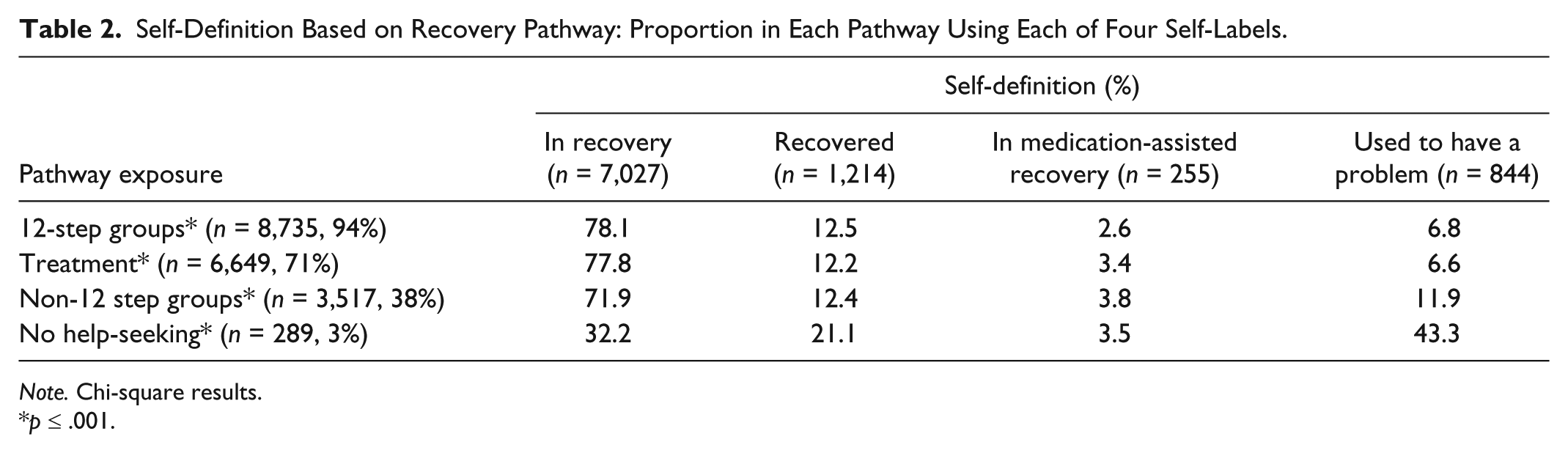
Note. Chi-square results.
p ≤ .001.
Substance Use Belief Based on Pathway: Proportion Within Each Recovery Pathway Who Believe That Recovery Is Abstinence Versus Not.

Note. Chi-square results.
p ≤ .001.
Substance Use Belief Based on Self-Definition: Proportion Within Each Type of Self-Definition Who Believe That Recovery Is Abstinence Versus Not.

Note. Chi-square results.
p ≤ .001.
Substance Use Behavior Based on Self-Definition: Proportion Within Each Self-Definition Who Abstains From Substance Use (Both Alcohol and Drugs) Versus Not.

Note. Chi-square results.
p ≤ .001.
Substance Use Behavior Based on Beliefs About Recovery: Proportion Within Each Belief Classification Who Is Abstaining Versus Not.

Note. Chi-square results.
p ≤ .001.
Results
Description of Sample (N = 9,341)
More than half of the sample is female, and almost half are older than 51 years of age. About a third live in urban settings, 43% in suburbs, and 21% rural. Most of the respondents (92%) came from the United States. It is a highly educated sample, with half having a college degree. About half are married or in a partnered relationship. The majority are non-Hispanic (93%) and White (87%), although minority representation is strong in terms of the number of Native American and African American respondents (n = 213 and n = 713, or 8% and 2%, respectively). Sixty-one percent are employed.
The dominant primary substance of choice (not shown) was alcohol (59%), followed by methamphetamines and heroin (7% each); cocaine, crack, and marijuana (5% each); prescription drugs (3%); and opiates other than heroin (4%). Three quarters of the respondents define themselves as in recovery, with smaller proportions self-defining as recovered (13%), used to have an alcohol or drug problem but don’t any more (3%), or in medication-assisted recovery (9%; see Table 2). Almost a quarter of the sample has been in recovery for 20 years or more; only 15% reported being in recovery less than a year, 10% between 1 and 2 years, 18% between 3 and 5 years, and about equal proportions (16%-17%) reporting between 5 and 10 years and between 10 and 20 years (results not shown).
This is a severe sample, with 97% of the respondents meeting Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for alcohol or drug dependence (not shown). As for beliefs about the definition of recovery in terms of substance abuse, 87% endorsed the belief that recovery is abstinence, 13% do not (see Table 3). Most of the respondents are currently abstaining from alcohol and drugs (83%; see Table 5).
In terms of pathways to recovery, only 3% (n = 289) are non-help-seekers (see Table 2, “no help-seeking”). Almost all the respondents (94%) had attended 12-step groups, most had been to treatment (71%), and there is large representation of exposure to non-12-step groups (38%). Twelve-step meeting attendance in this sample was quite high (Table 1), with almost half reporting having gone to more than 500 meetings in their lifetime and almost a quarter reporting 91 to 500 meetings. Exposure to non-12-step groups was low as a proportion of the sample, but yields fairly large numbers, with the highest exposure for SMART and WFS (8%; ns = 755 and 751, respectively; Table 1).
Relationship Between Recovery Pathway and Self-Definition
Among those exposed to treatment, about 78% self-define as in recovery, 12% as recovered, 3% as in medication-assisted recovery, and 7% as used to have a problem (Table 2). Similar choices for self-definition were found for those exposed to 12-step groups. Among those exposed to non-12-step groups, a similar pattern obtains, but with 72% self-defining as in recovery, 12% as recovered, and 12% as used to have a problem. However, among those reporting no help-seeking, only about one third self-define as in recovery and one-fifth as recovered, with more than 40% choosing the term used to have a problem. These differences are highly significant (p < .001), consistent with our hypothesis of a relationship between recovery pathway and self-definition (Hypothesis 1a).
Relationships With Recovery Belief
A high proportion of those exposed to treatment, 12-step and non-12-step groups, hold the belief that recovery is abstinence (more than 80%; Table 3). However, among the non-help-seeking group, the beliefs about recovery in terms of abstinence are equally split, with half saying recovery is abstinence and half believing that recovery does not require abstinence. The differences are highly significant (p < .001), supporting our Hypothesis 1b of a relationship between recovery pathway and recovery beliefs regarding abstinence.
More than 90% of those who self-define as in recovery (and 85% who self-define as recovered) hold the belief that recovery is total abstinence (Table 4). However, only 69% of those in medication-assisted recovery hold that view, and 58% of those who describe themselves as used to have a problem believe that recovery is abstinence. The relationship between self-definition and recovery and recovery beliefs about abstinence is highly significant (p < .001), as set forward in Hypothesis 2.
Relationships With Current Substance Use Behavior
In terms of the correspondence between self-definition and current abstinence (Table 5), we find that more than 85% of those who self-define as in recovery or recovered report that they are not using alcohol or drugs. Among those who self-label as in medication-assisted recovery, the majority (about 60%) are current abstainers. However, the group who self-defines as used to have a problem are split in terms of their current behavior: Half are abstaining and half are not. The relationship between self-definition and current abstinence is highly significant (p < .01), supporting Hypothesis 3a.
The majority of those who believe that recovery is abstinence from alcohol and drugs are consistent with their behavior regarding substance use, as 93% report current alcohol and drug abstinence (Table 6). Thus, only 7% holding that belief are inconsistent in terms of their belief and behavior. Furthermore, the relationship between recovery beliefs about abstinence and actual substance use behaviors is highly significant (p < .001), as proposed in Hypothesis 3b.
The last analysis considered the relationship between recovery pathway and current substance use (Table 7). More than 85% of those exposed to treatment report current abstention, and similar proportions report abstinence among those exposed to 12-step groups and non-12-step groups. Slightly more than one third of those in non-help-seeking group report current abstinence from alcohol and drugs, with the majority (64%) not reporting total abstinence. Recovery pathway and current substance use are strongly associated (p < .001), consistent with Hypothesis 3c.
Substance Use Behavior Based on Pathway: Proportion Within Each Pathway Who Abstains From Substance Use (Both Alcohol and Drugs) Versus Not.

Note. Chi-square results.
p ≤ .001.
Discussion
Consistent with social representation theory’s view that social collectives influence individuals’ language, self-perception, beliefs, and behaviors, all six of our hypotheses were supported: Pathways to recovery are strongly related to self-definition, abstinence beliefs, and abstemious behavior. These results highlight the value of theory-driven hypothesis testing, and more importantly, they demonstrate the key role that recovery-based approaches play in how those exposed to these collectives frame their recovery. Ours is the first such large-scale study to empirically show this.
For example, the belief that recovery is abstinence was broadly held in our sample, especially among those exposed to 12-step approaches, be it via treatment (which, in the United States, is usually 12-step based) and/or via 12-step fellowships. In contrast, opinions were mixed among the non-help-seekers, who were just as likely to define recovery as allowing for some use of substances as they were to define recovery as abstinence. Similarly, most of those exposed to treatment and to 12-step and popular non-12-step groups were abstaining from alcohol and drugs, whereas the majority of the non-help-seekers were using some substance(s).
The latter raises the question of potentially lower problem severity among the non-help-seeking group, who may not feel a need to abstain because their problems had not been severe enough to have required help. This is an alternative explanation to their not abstaining due to lack of exposure to the beliefs and language encountered in support groups or treatment. To study this, we conducted a post hoc comparison of DSM-IV dependence diagnosis rates between the non-help-seekers versus those exposed to some form of help-seeking: 88% of the non-help-seekers had a dependence diagnosis, compared with 98% of the help-seekers (p < .0001; not shown). Thus, although the rate of dependence is a bit lower for the non-help-seeking group, this is hardly a “low-severity” population. Future analysis of these respondents will look in-depth at their ages, and how long they have been in their self-defined status, to begin to get a handle on how well this fairly severe group has been able to “hold on” to their moderated substance use. The latter is an ongoing open question in the substance abuse field, as it confronts the dominant disease model paradigm that alcoholics cannot control their drinking and so must abstain completely.
One’s self-definition (i.e., in recovery, recovered, used to have a problem, or in medication-assisted recovery) also seems to matter in terms of beliefs and behaviors. For example, more than 40% of those who self-define as used to have a problem believe that the definition of recovery allows for some substance use, and only 49% in this group are total abstainers. Nonetheless, 9% of the individuals who self-define as in recovery do not believe that recovery is total abstinence and 11% are not abstaining completely. Based simply on anecdotal evidence (e.g., observations of individuals in the media or at recovery meetings and events who use the term in recovery and say they do not drink or use drugs), and guided by social representation theory, strong relationships between 12-step-oriented exposures and both abstinence beliefs and behavior would be expected; that is, when people say they are in recovery, they would define recovery as abstinence, and would be abstaining from all substances: Our data show that while most do, this is not universal. While this would otherwise be understood in social representation theory as a non-logical factor, perhaps the lack of perfect congruence between beliefs about abstinence and abstemious behavior should be expected, as some have argued that alcohol and drug dependence are chronic relapsing medical diseases similar to diabetes and hypertension (McLellan, Lewis, O’Brien, & Kleber, 2000). When seen through the lens of a chronic illness, an individual may believe in abstinence yet be unable to “hold onto” it, especially in the period of early recovery (Denzin, 1987). Unlike an acute illness that can be treated in a single episode, an abstinent recovery from a chronic disease can be difficult to achieve—and even harder to sustain—without continuous monitoring and management. Thus as a chronic illness, it would be “nonlogical,” per social representation theory, to expect 100% abstinence rates, even among those who believe that recovery requires abstinence.
To explore this further, we conducted post hoc analyses to study how substance use relates to one’s self-label as being in recovery? About half (54%) of those who are currently using alcohol and drugs say they are in recovery (not shown). This is similar to what was reported in a study of former drug users, which reported that 56% of those who currently used drugs said they are in recovery (Laudet, 2007). Thus, while most individuals who say they are in recovery are abstaining, about half of those who are not abstinent, nonetheless, say they are in recovery. This clearly shows that the use of the term in recovery usually, but not always, translates to abstinence. Service providers thus cannot assume that those who speak in terms of recovery language are necessarily abstaining—or that those who avoid such language are necessarily using substances.
Indeed, as more than 40% of those who had not (yet) sought help for their alcohol or drug problem do not self-identify as in recovery or recovered, providers also should be cautious in assuming that all of their clients are even comfortable with the term in recovery. In addition, perhaps addiction scientists should consider using another term than “natural recovery” to refer to individuals who have not sought treatment or attended mutual aid groups; one term we suggest for consideration, which avoids the term recovery entirely, is “self-changers.” However, research is needed to determine what language such individuals are more comfortable with. In Granfield and Cloud’s (1996) studies of self-changers, nearly two thirds rejected self-identification terms involving the words “recovery” or “recovered,” and most reported that they saw themselves in “some other way” (p. 50), which included their contemporary roles (e.g., as father, husband, worker). Some of their respondents explicitly rejected the disease model paradigm, whereas in contrast, Granfield and Cloud argue, those who participate in self-help groups “engage in a long-term, self-labeling process which involves continuous reference to their addiction” (p. 51). In a small qualitative study funded by the Substance Abuse and Mental Health Services Administration (Abt Associates Inc. & Heart Research Associates, 2010), the participants who were self-changers often described themselves as not in recovery and used some other term, such as “healed”: They viewed the disease as past and no longer directly affecting their present lives.
Here, we found that many with the pathway “no help-seeking” (i.e., the self-changers) chose the self-definition used to have a problem, which in turn was associated with non-abstinence beliefs and less abstinence. These individuals would not have been as exposed to the language of recovery as the help-seekers, and thus may not believe that they have a loss of control over their drinking or that they have a permanent “disease”; thus, they do not have to abstain, and they do not need to attend ongoing support groups. In contrast, those exposed to treatment or mutual aid groups are exposed to the disease concept and the idea that it is a permanent condition involving loss of control if one tries to drink; this leads to self-identification in reference to the disease state (e.g., in recovery as opposed to having had a problem in the past), to abstinence behavior, and to a need for ongoing participation in mutual help groups to sustain the abstinence.
Our recruitment effort reached a fair number of individuals in medication-assisted recovery (n = 255), an understudied group about whom we know very little. More than two thirds of this group believe that recovery is abstinence, almost as many (60%) are total abstainers, and 22% are abstaining from drugs only. Future analysis of our data from this group will examine how one’s specific substance of choice (alcohol or a particular drug) relates to the medication-assisted recovery self-definition and to current substance use behaviors; however, our brief online survey did not ask what medications were taken, and this remains an area in need of more research.
Finally, we note that the analyses presented here did not use sophisticated statistical modeling, focusing instead on chi-square tests of association and on the sheer magnitude of the differences. However, multiple mediation techniques have become available (see Preacher & Hayes, 2008) that also will allow us to determine the actual proportion of the relationship between recovery pathways and abstinence that is explained by one’s self-definition and one’s beliefs about recovery. The work conducted here demonstrates the necessary preliminary relationships that must exist prior to conducting formal tests of multiple mediation. The extent that abstinence can be explained by recovery pathways has service and policy implications, because it will show both the power and the limitations that recovery-oriented collectives represent.
Limitations
The study has at least four major limitations. Despite our broad and deep recruitment effort to reach individuals with different substances of choice and varying pathways out of substance abuse and dependence, we cannot claim that the sample is representative of the population of individuals who used to have a problem with alcohol and drugs. The scope of the questions explored is limited, due to the need for a brief survey that would be completed online without financial incentives. Third, the study is cross-sectional, so causality between self-definition or beliefs and behavior cannot be determined. Fourth, substance use is based on self-report.
Importance of Study Findings
This is the first large-scale investigation of how the language of recovery relates to actual beliefs and substance use behaviors among individuals who used to have alcohol and drug problems. Importantly, the study is consistent with anecdotal evidence and with the limited prior data on this population. We often hear people saying they are in recovery, and present findings now provide empirical evidence of the prevalent meanings of this ubiquitous expression. And for most, it means that they are abstaining from alcohol and drugs. However, our data also show that use of this term does not always signal abstinence, highlighting the importance of testing our assumptions, and demonstrating that there is still much to learn about how the language of recovery is interpreted and applied. Related, the study provides empirical confirmation of a strong link between abstinence-oriented beliefs and behaviors. This highlights the importance of language in developing abstinence-oriented beliefs (and, in turn, abstemious behavior) among those with alcohol or drug problems. Findings are of public health relevance, as it is estimated that 10% of American adults (23 million people) report having had alcohol or drug problems but no longer do (The New York State Office of Alcoholism and Substance Abuse Services [OASAS], 2012); the worldwide estimate may be similar, but is unknown.
Footnotes
Authors’ Note
The authors thank the study participants and research partners for their seminal help with the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by a grant from the National Institute of Health, NIAAA R01 AA017954-01A1.