
Abstract
This study aims to investigates the design and development of Immersive Virtual Reality Systems (IVRS) to enhance social interaction and communication skills among children with Autism Spectrum Disorder (ASD) in Thailand. Given the challenges of limited access to specialized care, the IVRS platform offers an innovative, home-based alternative for improving conversational skills in school settings without direct therapist involvement. Our mixed-methods research included 10 participants and combined quantitative analysis using the Social Communication Questionnaire (SCQ) with qualitative insights from interviews with parents and therapists. The quantitative results did not show statistically significant improvements, but qualitative feedback highlighted the platform’s effectiveness in enhancing social interaction and communication skills. The findings suggest that the IVRS platform could serve as a valuable supplementary tool for therapists. Additionally, design considerations for improving the platform’s usability and engagement are discussed, providing valuable lessons for further development of Immersive Virtual Reality Systems for ASD. This research represents an innovative advancement in ASD therapy in Thailand, offering insights for future implementations.
Plain Language Summary
This study explores the use of Immersive Virtual Reality Systems (IVRS) to improve social interaction and communication skills in children with Autism Spectrum Disorder (ASD) in Thailand. Designed for home use without a therapist, the IVRS simulates social scenarios with friends and teachers in school settings. The mixed-methods research, involving ten participants, revealed that while quantitative results did not show significant statistical improvements, qualitative feedback from parents and therapists highlighted the platform’s effectiveness in enhancing social interactions. The findings suggest that IVRS can serve as a valuable supplementary tool, offering practical support for children with ASD to develop essential social skills.
Keywords
Introduction
Autism Spectrum Disorder is a neurological and developmental disorder that affects social interactions, communication skills, behavior, and cognitive development (American Psychiatric Association, 2013). The prevalence of ASD has been steadily increasing worldwide, with individuals affected across a broad spectrum of severity. Notably, individuals with ASD may require significant assistance in daily living skills (DLS) due to considerable difficulties in both verbal and gestural communication abilities (Maenner et al., 2013; Park et al., 2012).
In Thailand, it is estimated that there are approximately 370,000 people with autism, but only 15% have access to medical care (Department of Mental Health, Ministry of Public Health, 2014). This lack of access to specialized care presents significant challenges, particularly in the educational system, where autistic individuals often struggle to understand social stimuli and navigate unpredictable social environments (Lüddeckens, 2021). Moreover, higher rates of school refusal behaviors are observed among autistic individuals compared to their neurotypical peers (Munkhaugen et al., 2017). Traditional therapy for ASD, often involving direct behavioral interventions, can be difficult to deliver consistently due to the high cost and limited availability of qualified therapists (Bekele et al., 2013). Therefore, innovative and practical interventions are critically needed to support individuals with autism.
Recent years have seen the emergence of virtual reality (VR) technology as a promising tool in various fields, including healthcare (Orlosky et al., 2017), surgical training (Pulijala et al., 2018), and psychiatry (Mishkind et al., 2017). Previous studies have demonstrated VR’s potential in supporting autistic individuals, such as observing the mental state of autistic children (Dhamodharan et al., 2020) and enhancing their social and cognitive abilities (Didehbani et al., 2016). However, studies specifically focused on leveraging VR to facilitate school-based conversational skills among autistic children remain scarce. This research gap is particularly relevant given the COVID-19 pandemic, which has drastically reduced the availability of traditional in-person therapy sessions. To address this gap, our study evaluates the effectiveness of an Immersive Virtual Reality Systems (IVRS) platform designed for home use without direct therapist involvement. This platform aims to replicate social scenarios involving friends and teachers in a school setting, thereby maintaining and enhancing the social and communicative abilities of children with ASD amidst such challenges.
The objectives of this research are to investigate the potential advantages and disadvantages of utilizing IVRS as an alternative therapy approach to improve the social interaction and communication skills of children with ASD, particularly when traditional in-person therapy sessions are not possible. Specifically, the study aims to: (RQ1) Evaluate the effectiveness of the IVRS platform in enhancing the social interaction and communication skills of children in Thailand; and (RQ2) Identify the most suitable system design features for parents and therapists. By addressing these research questions, this study aims to assess the utility and challenges of the IVRS platform in a therapeutic context for children with ASD in Thailand. Additionally, the study seeks to gather evidence on the platform’s efficacy and design preferences, contributing to the broader understanding of technology-assisted interventions for ASD and providing a foundation for future research and development in this field.
Literature Review
Autism Spectrum Disorder
Autism spectrum disorder, also known as autism, is a developmental disorder that typically emerges during the early stages of development. It is characterized by noticeable differences in communication and social interaction skills and a restricted range of behaviors, activities, and interests that are often repetitive and stereotypical in nature. The Diagnostic and Statistical Manual of Mental Disorders classifies ASD into three severity levels, with the third level representing the most severe form where individuals require significant assistance with daily living skills (DLS) due to considerable difficulties in both verbal and gestural communication abilities (American Psychiatric Association, 2013). Individuals with milder forms of ASD, considered to have higher functioning levels, can communicate verbally but still struggle with sensory processing and interpreting social cues. Consequently, autistic children tend to have lower daily living skills compared to their peers with similar IQ levels (Maenner et al., 2013; Park et al., 2012). As a result, individuals diagnosed with ASD may experience feelings of being overwhelmed and anxious in unfamiliar or crowded places, such as public transit systems, educational facilities, and retail stores.
Social Skills Interventions and Autistic Children
Despite numerous research efforts and reviews conducted on the treatment and education of autistic children, there is currently no universally accepted standard method for this diverse group (Masi et al., 2017). However, within the range of evidence-based interventions, certain factors have emerged as crucial for improving communication skills and encouraging voluntary social interaction. These factors include the child’s interests and the creation of a supportive environment that mirrors real-life situations. Social skills interventions increasingly employ situated, naturalistic techniques instead of direct instruction, emphasizing self-observation, peer conflict resolution, and the use of naturally occurring stimuli as prompts for social interactions rather than relying solely on teacher-spoken antecedents (Ke et al., 2018). Situated, naturalistic interventions take place in less-controlled environments, incorporating children’s individual inclinations and desires and seamlessly integrating them (Wong et al., 2015). Autism research is shifting away from cognitive theoretical explanations and toward social motivation as a substantial contribution to the social difficulties reported in people with ASD. As a result, effective social skills programs must capitalize on and nurture children’s interest and motivation in social knowledge and interaction. This can be achieved by emphasizing the importance of social stimuli in relation to problem-solving tasks or by appealing to the children’s natural interest in the stimuli and the task at hand. Creating and exploring an authentic and individually significant learning setting tailored to autistic children holds great promise for development and research (Chevallier et al., 2012).
VR for Social Skills Training
Children with autism often struggle to develop social skills and experience anxiety when attempting to practice those skills in real-world situations. Virtual Reality (VR) technology has emerged as a valuable tool for enhancing the social abilities of autistic children in real-world settings. By providing a safe and controlled environment, VR allows them to practice and improve their social skills without the anxiety associated with making errors or facing rejection that is commonly experienced in in-person interactions (Fernández-Herrero et al., 2018). Repetition plays an essential role in developing social skills, and utilizing innovative technologies for social skills training has proven effective. Autistic children have shown positive responses to computerized interventions, resulting in notable learning advancements through diverse training programs that utilize technology, such as animated shows, video-based instruction, technology-assisted learning, digital gaming, and immersive virtual environments (Knight et al., 2013).
The unique features of VR technology allow for repeated exposure and practice in a safe and controlled virtual environment (Kandalaft et al., 2013). VR-based learning environments are non-threatening and offer diverse scenarios, enabling participants to learn through experiential methods rather than memorization-based approaches (Bellani et al., 2011; Newbutt et al., 2016b). VR systems create computer-generated, three-dimensional, and realistically simulated environments, providing immersion and a feeling of presence similar to being physically present in the real world (Burdea & Coiffet, 2003; Cipresso et al., 2018; Slater, 2009). In the context of ASD, VR applications have been explored for both treatment and assessment purposes. VR training programs focus on social skills, emotional recognition, anxiety, and phobias, employing desktop-based VR devices and implicit measures like eye tracking, which have demonstrated effectiveness in enhancing social competence and bringing about improvements in individuals diagnosed with autism (Parsons, 2016; Parsons & Mitchell, 2002).
The benefits of technology-based educational programs are gaining recognition, with increasing interest and evidence supporting the use of interactive computer-based technologies to revolutionize learning and enhance the independence and overall well-being of autistic children (Walsh et al., 2017). Technology-based educational programs offer several advantages, including prompt and consistent feedback, active learning, adaptive modification of social expectations, effective use of visual cues and multimodal interactions, and cost-effective and time-efficient individualized instruction (Wong et al., 2015).
Platforms of Virtual Reality for Children With ASD
Researchers have conducted studies using VR as a therapeutic method for treating autism. Examples include virtual settings that teach appropriate behavior in specific situations, immersive games for practicing conversational skills, systems for understanding facial expressions and emotions, collaborative virtual environments for communication skills practice, and social skills training systems utilizing virtual agents, Hoque et al., 2013; G. Lorenzo et al., 2016; Ramachandiran et al., 2015; Stewart Rosenfield et al., 2019; Zhao et al., 2016). Eye-tracking technology has been utilized in immersive VR environments to understand visual attention responses, revealing differences in visual engagement between children with ASD and typically developing peers (Alcañiz et al., 2022). Such diversity in VR applications not only highlights its potential in supporting children with ASD in multifaceted ways but also points to the importance of integrating VR into the broader spectrum of autism therapy and education.
Building upon this foundation, recent studies have further expanded the scope, investigating VR platforms for children with ASD across various countries including Malaysia, the USA, Spain, Qatar, Italy, Iran, and Kazakhstan. These studies, engaging a varied number of participants from 2 to 55, utilized a range of VR technologies, including the picture exchange communication system, collaborative virtual environments, augmented reality, machine learning, eye-tracking technology, and desktop VR-CPT. Findings indicate a diverse impact of VR on children with ASD. For instance, in Malaysia, participants showed a preference for specific virtual environments like a virtual toilet, while in the USA, children with autism exhibited significant engagement with VR games, demonstrating the platforms’ potential to enhance social and communication skills. Another study in Qatar highlighted the effectiveness of desktop Virtual Reality Continuous Performance Test (VR-CPT) in outperforming typically developing peers in assessment scores. However, the use of desktop VR-CPT, as opposed to head-mounted displays (HMD), did not fully immerse participants in the simulated classroom environment. This partial immersion could potentially limit the effectiveness of the VR intervention since full immersion is often crucial for eliciting more genuine responses and interactions within the virtual setting. Another critical limitation identified was the omission of participants’ mood or emotional states as a factor in the analysis. Emotional and mood states can significantly influence attention and engagement with the VR tasks, affecting the intervention’s efficacy. The variability in the emotional responsiveness of children with ASD requires careful consideration in designing and evaluating VR-based interventions (Banire et al., 2021). Frolli et al. assessed the efficacy of traditional emotional training versus Virtual Reality (VR) training in improving social skills among children with ASD. The study aimed to determine which method more quickly enhances the acquisition of social tasks. Results showed that VR-based intervention led to faster learning, especially in tasks involving secondary emotions and contextual emotional understanding. The immersive and interactive nature of the VR experience, along with the direct exposure to simulated social scenarios, likely contributed to the enhanced learning outcomes observed in the VR group (Frolli et al., 2021). Meanwhile, in Iran, the use of HTC VIVE virtual reality headsets indicated that VR could be effective in improving musical phrase playing abilities among children with ASD. Notably, an adaptive Immersive Virtual Reality Training System called “My Lovely Granny’s Farm” has been developed to provide therapy to individuals with ASD in the comfort of their homes, leveraging their interest in static objects and the adaptive IVRS. The system revealed that children’s attention was focused on static objects and details, underscoring the diverse applications and benefits of VR technology in supporting children with ASD (Soltiyeva et al., 2023).
These studies collectively highlight VR’s potential as a complementary tool for therapy and education in ASD, pointing toward its capability to offer safe, engaging, and varied environments for skill development and interaction. However, these studies were conducted in specific settings. Therefore, the findings may not be universally applicable to other cultural or geographical contexts. In response, this current research aims to extend the exploration of VR as a therapeutic tool for ASD by evaluating the IVRS platform’s efficacy within Thailand’s cultural and social context (Table 1).
Comparison of Virtual Reality Platforms for Children With ASD.

Purpose of the Study
The purpose of this study is to investigate the potential advantages and disadvantages of utilizing Immersive Virtual Reality Systems as an alternative therapy approach to improve the social interaction and communication skills of children with autism spectrum disorder when in-person therapy sessions are not possible, such as during the COVID-19 pandemic. The study’s specific goal is to construct and evaluate a VR platform that can be simply operated at home by parents without the assistance of a therapist. The research questions guiding this study are as follows:
RQ1: What is the effectiveness of the IVRS platform in enhancing the social interaction and communication skills of children in Thailand?
RQ2: What is the most suitable system design for parents and therapists to use?
By addressing these research questions, this study aims to demonstrate the effectiveness of the IVRS platform in improving the social interaction and communication skills of children with ASD in Thailand. In addition, the study aims to identify the system design features that are most practical and user-friendly for both parents and therapists. The study’s ultimate goal is to establish the IVRS platform as a successful tool for treating children with ASD in Thailand, benefiting not only the children but also their parents and therapists. The study’s findings and insights can also be applied to future IVRS implementations in the treatment of ASD in children, providing helpful guidance for future research and development in this field.
Procedure for Development of Platform
System Features
The MoonnicVR platform has a number of features that are specifically designed to help children with ASD improve their conversational skills in a variety of scenarios in their daily lives. These features provide children with a realistic and immersive experience, allowing them to engage in conversations and practice their abilities in many circumstances. The MoonnicVR primary system features are as follows:
Computational Design
The computational design of the MoonnicVR platform involves the integration of various software tools and technologies. Autodesk Maya 2020.4 is used to create the virtual environment, including 3D models, textures, and animations. Unity version 2021.3.19 serves as the game engine and facilitates software development and integration of the virtual environment, virtual characters and interactive elements (see Figure 1). The Meta Quest 2 virtual reality headset provides an immersive experience for children with ASD and allows them to interact with the virtual environment and characters. MySQL 8.0 serves as the database management system responsible for storing and analyzing the anonymized data collected during the interactions. The interaction of these elements creates an immersive VR platform that enhances the conversational skills of children with ASD.
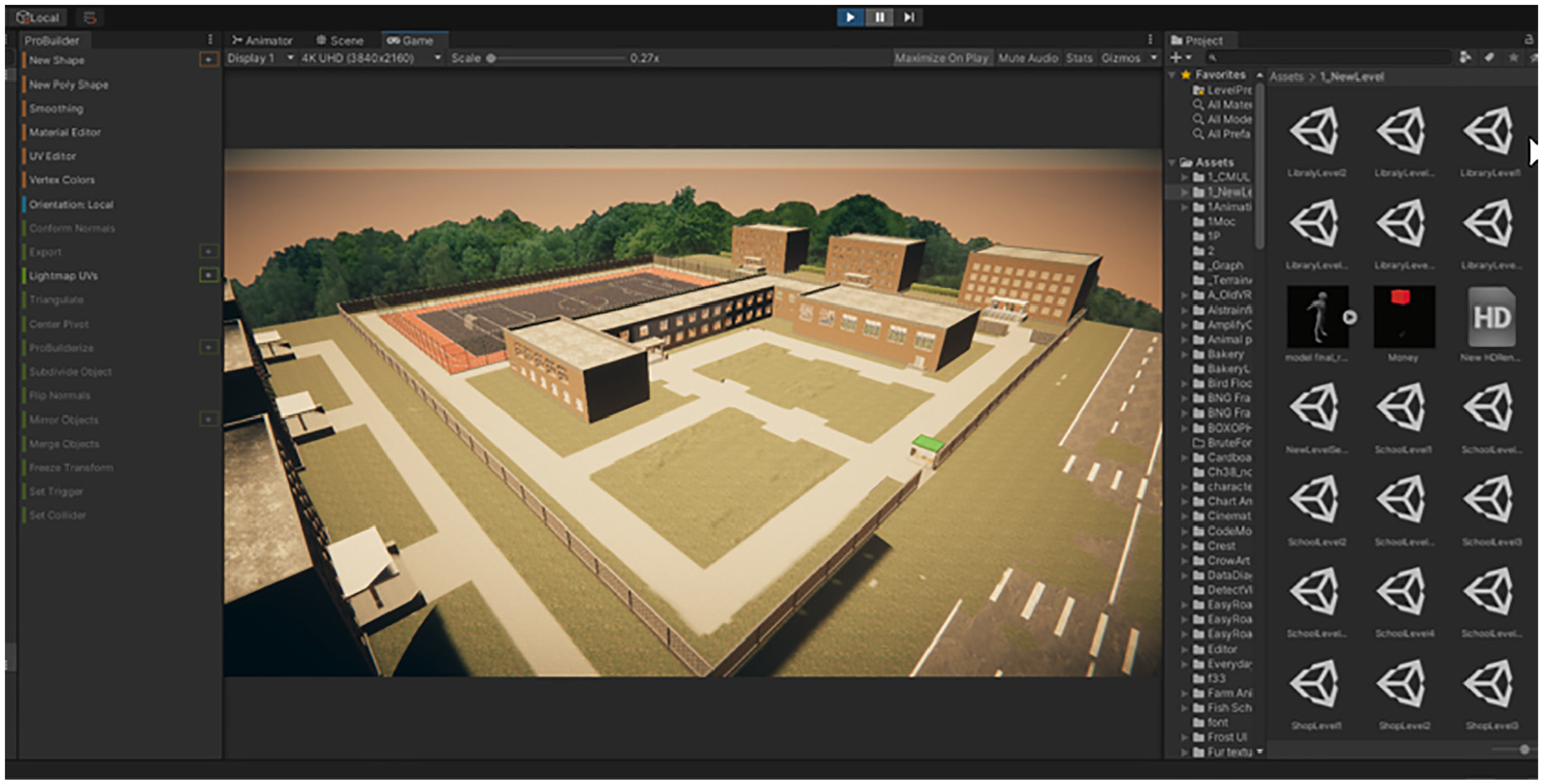
Work process in the unity game environment.
To construct the virtual environment, the researchers utilized Autodesk Maya, a software tool known for its capabilities in designing realistic landscapes, buildings, classrooms, and other elements commonly found in schools. Special attention is paid to intricate details such as lighting, textures and object interactions to provide an especially realistic experience for children with ASD. The virtual characters representing teachers, classmates, and others are carefully designed to resemble real people and exhibit authentic facial expressions and body language (see Figure 2).

The virtual character interacting within the system.
Real-Time Feedback and Coaching Design
The system includes a real-time feedback, assessment, and coaching mechanism to continuously monitor and evaluate each child’s progress. It records and analyzes the child’s conversations in various circumstances, highlighting areas for improvement and delivering immediate feedback. The method gives instructions for parents and therapists to help the child achieve the objectives of the tasks (Figures 3 and 4). Parents and therapists actively participate with the child in these instances, providing positive feedback along with guidance to help them deal with specific situations.

Design of the system providing guidelines to assist the child.

Design of the user interface for parents and therapists to mentor.
Upon completion of each task, parents and therapists can record the child’s behavior and performance, indicating one of three levels of response rate: (1) 100% response rate, (2) 50% response rate, or (3) no response. These responses are subsequently recorded in the database for further evaluation. This reporting tool allows for the collection of vital data on the child’s progress and behaviors, which contributes to a clearer understanding of their development. Additionally, parents and therapists have real-time access to the system, allowing them to monitor the development of the child and provide continuing coaching and support. This seamless integration of real-time coaching fosters collaboration by actively integrating parents and therapists in directing the development of the child’s conversational skills across varied situations.
Educational Design
Empirical studies and reviews of treatment or educational methods for children with autism spectrum disorder have not yet identified a universally recognized optimal method that is effective across different age groups (Masi et al., 2017). Traditional approaches have often involved direct behavioral therapy (Ke et al., 2018). However, establishing effective human-to-human interaction for children with autism can be challenging, making Immersive Virtual Reality Systems a promising educational tool (Ramachandiran et al., 2015; Soltiyeva et al., 2023). The therapy proposed in this study is based on the hypothesis of conditioned response in a real-life environment, in which the child’s behaviors are reinforced with rewards to help them develop necessary skills. Additionally, therapists can provide guidance and assistance within the system.
Participants in the system gain points for performing activities, with each mission consisting of many tasks tailored specifically to improve the communication abilities of children with ASD in everyday life. Table 2 provides a summary of these tasks. The system creates a secure and exploratory setting in which participants can hone their social communication skills. Their parents and therapists guide them through the monitoring system. The user’s interaction with the virtual environment plays a crucial role in facilitating learning, as the use of VR games for educational purposes offers a highly interactive learning experience unlike traditional teaching environments (Checa & Bustillo, 2020). By utilizing this approach, the system aims to improve communication skills and promote interactive learning for children with ASD, especially in their interactions with friends and teachers during the school day (Figure 5). The revised missions additionally aim to include Thai cultural norms and values, particularly when it comes to interacting with teachers. The virtual reality program can assist children with ASD in navigating social interactions in a culturally appropriate way by placing an emphasis on respect and politeness.
Task Descriptions in the Mission.


Children interacting with the mission “Greeting with Teacher.”
Research Design
This study utilized a mixed-methods sequential explanatory design to assess trends and relationships through quantitative data and explore the underlying mechanisms behind these trends with qualitative data (Creswell & Clark, 2017). The quantitative component involved data collection through the Performance Evaluation in the Platform and the Social Communication Questionnaire. The qualitative component comprised semi-structured interviews with parents and therapists to gather in-depth insights.
To collect data, researchers from Chiang Mai University, the Rajanagarindra Institute of Child Development, and the Banprajan Child Center in Chiang Mai Province designed and developed the IVRS platform known as MoonnicVR, with funding from the National Innovation Agency of Thailand. The project was divided into two stages: software development and testing. In the first stage, the prototype for treating children with Autism Spectrum Disorder was designed and developed at the university with the assistance of academic members from the Faculty of Public Health, the College of Arts, Media, and Technology, and the Faculty of Humanities. Subsequently, the platform was evaluated with ASD child therapy experts at the Banprajan Child Center. This private center, located in Chiang Mai, Thailand, specializes in the treatment of children with ASD.
Participants
Prior to the commencement of the study, the Research Ethics Committee of the Faculty of Public Health at Chiang Mai University granted ethical approval No.ET023/2021, ensuring that the study adhered to ethical rules and regulations. The study included eight boys and two girls with Autism Spectrum Disorder who attended both public and private schools in Chiang Mai, Thailand. The participants ranged in age from 8 to 12 years old. To be included in the study, participants were required to provide documentation of their ASD diagnosis from a licensed doctor.
Selection criteria for participants included their ability to operate the system’s equipment, such as the VR headsets and controllers, which necessitated fine-motor skills. Participants were also required to actively engage in the study for at least 20 min without experiencing considerable physical discomfort. Additionally, an official diagnosis of ASD, as documented by a medical professional, was mandatory. Informed consent was obtained from the participants’ parents or legal guardians, ensuring they were fully informed about the study’s purpose, procedures, and potential risks. Moreover, verbal consent was collected from the participants, highlighting their willingness to engage in the study.
Initially, 13 participants were recruited. However, due to factors such as scheduling conflicts and the withdrawal of consent, the final sample size for data analysis was adjusted to include 10 participants: 8 boys and 2 girls. Detailed demographic and characteristic information about the participants is presented in Table 3, offering a comprehensive overview of the study’s participant composition.
Demographic of Participant Characteristics.

Note. ASD = autism spectrum disorder; TD = tic disorder; CP = cerebral palsy.
Instruments and Measurement
The Immersive Virtual Reality System
The MoonnicVR immersive Virtual Reality System was used as the primary instrument in this study. The system required the usage of a Meta Quest 2 VR headset with 6DOF (six degrees of freedom) tracking capability. This tracking capabilities allowed for the observation of hand motions, head rotations, and spatial placement. Child participants engaged with the device by holding two wireless controllers and wearing a head-mounted display. These components allowed the system to detect the position of the hands in space as well as the position of the fingers. Using their personal laptops, therapists were able to provide coaching and monitor the child’s progress. Furthermore, researchers and parents were able to observe the treatment process. The data shown on the child’s monitor was synchronized with the laptops used by therapists, researchers, and parents, enabling for real-time monitoring and analysis of the child’s interactions inside the virtual environment.
A particular research area with adequate space was set up at the Banprajan Child Center to protect the safety of the children and prevent collisions with things that could potentially cause injury (refer to Figure 6). The area provided a controlled environment to conduct the study and ensured the safety of the participants.
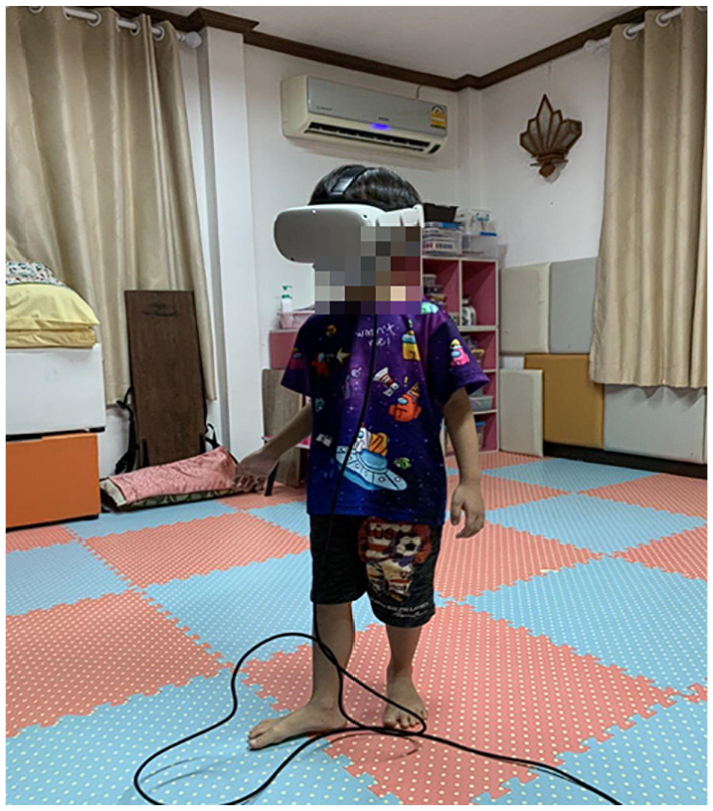
Testing the system with children diagnosed with ASD.
Performance Evaluation in the Platform
The participants were provided with account profiles to log in and use the MoonnicVR platform. The platform recorded data on the participant’s performance, which was visualized in graphs representing the therapist’s evaluation of the participant’s response rate for each task of the mission. To facilitate visualization, a scoring system was used where a response rate of 100% was assigned 2 score points, a response rate of 50% was assigned 1 score point, and a response rate of 0% was assigned 0 score points. Each mission in the study consisted of five activity tasks, and statistical data was collected over a period of 2 months, with one session per week. To measurement the Platform begin by using descriptive statistics to summarize and visually present the performance evaluation results. Graphical representations, the line graphs for total score are also valuable for illustrating trends over time.
Social Communication Questionnaire
The Social Communication Questionnaire (SCQ) was employed as a tool to evaluate the social communication skills of the participants within the context of the Virtual Reality Systems for Autism. The SCQ is a widely recognized and validated instrument used in autism research and clinical practice. It consists of 40 yes-or-no questions and can usually be completed within 20 min by the parent or primary caregiver. The questionnaire collects information regarding the participant’s social and communicative abilities, as well as behavioral characteristics related to ASD. Parents are asked to report measures of the individual’s social communication behavior over the most recent 2-month period. The SCQ was administered as a pre- and post-intervention evaluation tool to assess any changes or improvements in the participants’ social communication skills over time.
Interview With Parents and Therapists
Semi-structured interviews were conducted with a purposive sample of five parents and three therapists involved in the study. These participants were selected based on their active engagement with the Immersive Virtual Reality Systems platform and their willingness to provide detailed feedback. The use of semi-structured interviews allowed for flexibility in discussing a range of topics while ensuring that all relevant aspects of the platform’s effectiveness and usability were covered.
An interview guide was developed to structure the conversations and ensure consistency across all interviews. This guide included open-ended questions designed to elicit detailed responses about the participants’ experiences with the IVRS platform. The key questions are shown in Appendix 1.
Research Procedure
The study’s methodology was organized into four sequential phases: Recruitment, Preparation, Intervention, and Analysis, each critical to the research process. An overview of the research procedure is shown in Figure 7.
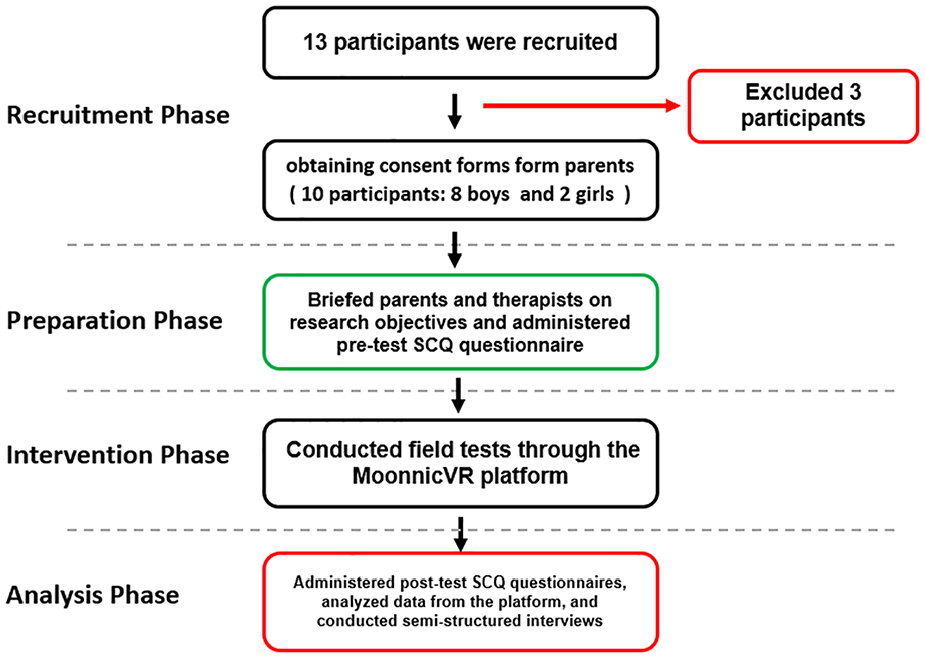
Overview of research procedure.
The research process was designed to maintain scientific rigor, ensuring that the collected data provided a reliable and valid assessment of the IVRS platform’s capacity to improve social communication skills in children with ASD. The combination of quantitative and qualitative methodologies facilitated a robust and comprehensive analysis, culminating in an integrated understanding of the platform’s efficacy.
Result
Result of Performance Evaluation in Platform
The performance evaluation results for participants 1 to 10 during the intervention phase are depicted in Figure 7. This phase covered a training period of 2 months (approximately 8 weeks). The study included four missions, each consisting of five activity tasks. Each week, the children repeated each mission three times, spending 2 weeks per mission. In the graph, the Y-coordinate represents the total score points for the response rate of the entire mission, while the X-coordinate indicates the number of training sessions conducted during the intervention phase (one session per week). The blue line graph represents the performance evaluation for the “Conversation with Friend” mission, and the red line graph represents the “Conversation with Teacher” mission.
Descriptive statistics analysis of the visualization of individual participants’ performance during the intervention phase indicates a general trend toward improvement, particularly in responding to friends, for individuals 1, 2, 3, 6, 8, and 9. With the exception of participant 2, there was notable improvement in performance in responding to teachers. Participants 4, 5, 7, and 10 did not show significant improvement during the intervention period. However, it is important to note that the overall intervention outcomes did not achieve statistical significance (p-value > .05). This lack of significance could be attributed to several factors. Firstly, the small sample size of 10 participants limits the power of the statistical tests, making it challenging to detect significant effects. Secondly, variability in individual responses and the relatively short duration of the intervention (8 weeks) may not be sufficient to capture significant changes in social interaction skills. Future studies with larger sample sizes and extended intervention periods are recommended to better understand the potential impact of IVRS on ASD therapy.
It should be highlighted that data for participant 5 in week five and participant 8 in week three are absent due to their non-attendance in those sessions. Overall, the intervention outcomes indicate a slight trend of improvement; however, statistical significance was not achieved. Participants demonstrated better performance in missions involving interactions with friends compared to those involving conversations with teachers, a finding also suggested by previous studies (Chen et al., 2021). It is critical to acknowledge the impact of missing data, particularly for participant 5 during week five and participant 8 during week three, due to their absences. This gap presents a limitation in our analysis, requiring a conservative approach to interpreting the participants’ progress throughout the intervention. By choosing not to impute or extrapolate data for these absent sessions, we endeavored to preserve the integrity and authenticity of our findings (Figure 8).

Results of the performance evaluation for participants 1 to 10.
Pre- and Post- Intervention Social Communication Questionnaire
The pre- and post-intervention Social Communication Questionnaire scores demonstrated a numerical reduction in autism spectrum disorder symptoms following the 2-month intervention, with SCQ scores about eight times lower. The SCQ scores of the participants are presented in Tables 4 and 5, where “Y” represents the score reduction. Participants 1, 2, 3, and 10 exhibited a reduction in ASD symptoms, while participants 4, 6, and 7 did not show a significant difference. Participant 8, however, displayed a slight increase in symptoms.
Result of Pre- and Post-Intervention SCQ score.

The Results of the Wilcoxon Signed Rank Test.

Statistical analysis was conducted to assess the mean scores of the pre-intervention (score = 18.30, SD = 3.33) and post-intervention (score = 17.10, ds = 3.98) SCQ assessments. The non-parametric Wilcoxon Signed-Rank Test was employed to determine if there was a statistically significant difference between the two sets of scores. The results indicated no significant difference, with a p-value of .121. This lack of statistical significance may be due to the small sample size, which reduces the power to detect changes. Additionally, the relatively short intervention period may not be sufficient to observe significant improvements in social communication skills. These findings suggest that while qualitative data indicate positive trends, more extensive studies are required to statistically validate the effectiveness of the IVRS platform.
Qualitative Results
The qualitative component of our study was systematically conducted through face-to-face interviews with five parents and three therapists, all directly involved with the use of the Immersive Virtual Reality Systems platform. These interviews aimed to delve into the participants’ insights and perspectives regarding the platform’s effectiveness in enhancing the social interaction and communication skills of children with Autism Spectrum Disorder. Additionally, participants were encouraged to offer suggestions for the platform’s enhancement as a therapeutic tool. The interviews followed a semi-structured format, allowing for consistency across interviews while providing the flexibility to explore specific areas in more depth. Each interview lasted approximately 30 to 45 min and was audio-recorded with participants’ consent, with detailed notes taken during the interviews.
We employed a rigorous thematic analysis approach to analyze the qualitative data obtained from the interviews. The analysis process was carried out in several stages, ensuring a comprehensive and transparent examination of the data. All interviews were transcribed verbatim, resulting in detailed transcripts that captured both verbal and non-verbal cues, such as pauses and emphases. The research team members familiarized themselves with the data by reading and re-reading the transcripts, a crucial initial step for gaining a deep understanding of the content and context of the interviews. We then conducted an open coding process, systematically examining each transcript to identify significant statements and phrases related to the research questions. Codes were assigned to these text segments, representing key concepts and ideas, which were then grouped into broader categories to identify patterns and themes.
This process involved iterative discussions among the research team to ensure consistency and accuracy in theme development. The themes were reviewed and refined through multiple cycles of analysis, cross-checked with the original data to ensure they accurately reflected the participants’ views, and any discrepancies were resolved through team discussions. The final step involved defining and naming the themes, providing clear descriptions and labels that captured the essence of each theme. We ensured that the themes were distinct and comprehensive, covering all relevant aspects of the data. The final themes provided a rich narrative on the perceived impact of the IVRS platform on children’s developmental progress and offered actionable insights for future enhancements. These themes are presented in the results section, supported by direct quotes from the participants to illustrate the findings. A summary of the qualitative results from both parents and therapists is shown in Appendix 2.
Perceiving Improvements in Social Interaction and Communication Skills
Parents and therapists consistently emphasized the IVRS platform’s significant impact on enhancing children’s social interaction and communication skills. Notable advancements were observed in children’s understanding of manners, cultural norms, and communication etiquette, particularly within the Thai cultural context. Parents observed improvements in their children’s ability to initiate and sustain conversations, express emotions more openly, and participate more actively in social activities. One parent highlighted the platform’s role in these developments, stating, “My child has shown remarkable improvement in interacting with friends and understands the importance of using proper manners, respecting authority, and showing politeness when talking to teachers” (P1). Furthermore, the integration of cultural nuances into the IVRS platform was highly valued. Another parent shared, “It’s not just about communication; it’s about culturally appropriate communication. Witnessing my child bow slightly when greeting their teacher, a gesture deeply ingrained in our culture but often overlooked, was a moment of pride and a testament to the platform’s effectiveness” (P3).
A therapist echoed this sentiment, noting, “The platform has been instrumental in teaching children the nuanced aspects of social communication that are often challenging for them. I’ve seen firsthand how children who struggled with basic greetings are now able to approach and converse with their peers and adults with confidence” (T1). Additionally, another therapist highlighted the platform’s role as a supplementary tool to traditional therapy, cautioning against its use as the sole treatment method. “While the IVRS platform has shown promising results in enhancing social skills and cultural understanding, it’s crucial to remember that each child with ASD is unique, with specific needs and challenges. The platform can serve as an effective complementary tool, enriching the therapeutic landscape. However, it cannot replace the personalized, one-on-one interactions and interventions provided in traditional therapy settings. For instance, a child might excel in virtual scenarios but still face challenges in unscripted, real-world interactions. Therefore, as we integrate innovative solutions like IVRS, continuous evaluation and adjustment of therapeutic approaches are essential to cater to each child’s evolving needs” (T2).
Instances Reflecting the Impact of the IVRS Platform on Social Interactions
Parents provided vivid accounts of the positive changes they observed in their children’s social interactions, attributing these improvements to the IVRS platform. “My child’s behavior toward friends and teachers has improved significantly,” one parent noted (P2). They also mentioned the adoption of more appropriate language, “He’s using ‘krub’ and ‘thank you’ without being prompted, which he picked up during his sessions” (P5), and highlighted how these virtual lessons were applied in real-world interactions, “At the parent-teacher meeting, his teacher was surprised at his initiative to greet her first. It’s something we practiced in the VR environment” (P4).
Therapists corroborated these observations, underscoring the platform’s role in enhancing social skills that are critical in real-life interactions. “The virtual setting provides a safe space for children to practice social cues, which we’ve seen translate into more confident interactions in the classroom,” a therapist remarked (T1). Another therapist emphasized the broad impact, “Not only are they learning to use language more effectively, but they’re also understanding the timing and context for social interactions, which is often a challenge for children with ASD” (T3).
The consensus among both parents and therapists is that the IVRS platform serves as a valuable tool for improving social interactions among children with ASD. The direct application of skills learned in the VR environment to real-world scenarios underscores the platform’s practical effectiveness and potential as a complementary tool in ASD therapy.
Design Considerations for a Parent-Friendly Platform
Parents underscored the critical need for an IVRS platform that is navigable without therapist intervention, emphasizing a user-friendly design. “It’s crucial that we, as parents, can easily navigate the system. A clear interface and simple instructions make all the difference,” shared one parent (P2). Concerns were also raised about the hardware’s suitability for younger users, with one parent noting, “The headset was just too big for my child, and setting it up was more complicated than it needed to be” (P3). Suggestions for enhancing the platform included adjustable headsets for younger children and a more straightforward setup process for the Guardian system.
On the software side, the desire for an uncomplicated method to access and start the intervention program was a common theme. “We need a way to get into the program that doesn’t feel like a tech support task every time,” a parent expressed (P4). The importance of incorporating features for real-time progress tracking and performance feedback was also highlighted, with a parent stating, “Being able to see how my child is progressing in real time is invaluable. It helps us make decisions about what to focus on next” (P5).
Echoing parents’ sentiments, a therapist emphasized the platform’s potential for home use, “A parent-friendly interface and straightforward tracking can significantly enhance the therapeutic experience outside the clinic. It’s about empowering parents to take an active role in their child’s development” (T1). Another therapist added, “The feedback system isn’t just beneficial for parents; it informs our practice by highlighting areas where a child might need more support” (T2).
Suggestions for Enhancing the Effectiveness of the IVRS Platform
Feedback from participants, including both parents and therapists, pinpointed key areas for refining the IVRS platform to enhance its effectiveness. There was a unanimous call for simplifying the setup process. One parent stated, “Setting it up should be straightforward, akin to flipping a switch. The initial complexity detracted from our enthusiasm” (P5). Both therapists and parents advocated for a more intuitive interface, with a therapist remarking, “Children should find navigating the platform as easy as leafing through their favorite picture book” (T3).
The need for clearer, more visual instructions for headset setup was emphasized by a parent: “Visual, step-by-step guides could alleviate the setup hassle, making it a smoother experience for non-tech-savvy users” (P4). Suggestions to expand the platform’s content to include a broader array of social scenarios aimed at equipping children for a wider range of interactions were common. “Adding scenarios that mimic everyday situations, like bullying at school,” was suggested by a therapist (T1). Participants also recommended integrating interactive games designed to reinforce communication skills, thereby making the learning process more engaging. “Games that simulate real-life conversations and encourage expressive language use could significantly enhance the learning experience,” noted another therapist (T2).
Furthermore, the need for even more diverse and challenging scenarios to better prepare children for complex social interactions was highlighted. “Incorporating scenarios that involve conflict resolution or understanding non-verbal cues could challenge the children and spur significant growth,” proposed a parent (P4). The idea of adding customizable scenarios that can be tailored to each child’s specific learning objectives or interests was also introduced: “Allowing parents or therapists to customize or create scenarios based on the child’s current learning focus could make the platform infinitely more valuable,” shared a therapist (T1).
Discussion and Finding
Autism Spectrum Disorder is a developmental disorder that typically appears before the age of 3 and persists throughout a person’s life, although symptoms may improve over time (Landa, 2008). The use of virtual reality technology in a learning environment has been recognized as an effective tool for advancing social skills in individuals with ASD. Previous studies have explored virtual reality-based learning approaches, such as embedding multimedia direct instruction in a virtual world (Glaser & Schmidt, 2022; Stichter et al., 2014). In this study, we introduced the Immersive Virtual Reality Systems platform, which was aimed at imitating social scenarios involving friends and teachers in a school setting with a purpose of improving behavioral and communication skills in children with ASD. This platform is the first of its kind in Thailand, catering to inclusive education and enabling equal access to education for all students, including those with special educational needs. To evaluate the usefulness of the IVRS platform, we collected both quantitative (SCQ and platform data) and qualitative (observations and interviews with parents and therapists) data while addressing the study’s objectives.
Regarding Research Question 1 (RQ1), The results indicate that the IVRS platform had mixed outcomes. The quantitative data from the pre- and post-intervention SCQ evaluations did not indicate a statistically significant difference according to the paired-samples t-test (p = .14), as shown in Table 4. Additionally, the evaluation data collected from the platform (Figure 7) did not demonstrate significant improvement and exhibited inconsistency in results depending on the participant. However, an overall trend of slight improvement was observed, particularly in participants’ performance during social interactions with friends, in contrast to conversations with teachers. Conversely, qualitative data obtained from interviews with parents and therapists consistently underscored the IVRS platform’s perceived effectiveness in enhancing social interaction and communication skills. Participants reported that the platform facilitated a deeper understanding of manners and cultural norms when communicating with teachers, a factor of particular relevance in the Thai cultural context, where polite language use and respectful expression of emotions toward elders are highly valued. Furthermore, the platform’s capacity for scenario repetition and customization, tailored to the preferences of parents and therapists, was highlighted as a potential tool for long-term skill improvement in children, as reported in previous studies Moon and Ke (2023) and G. G. Lorenzo et al. (2023).
However, it is worth noting that the positive effect in terms of social reciprocation was observed when participants immediately applied turn-taking skills in the physical world, which is consistent with previous research (Stewart Rosenfield et al., 2019). In addition, parents indicated that their children were able to differentiate and use acceptable language for greeting and conversation depending on whether they were conversing with a friend or a teacher. This distinction is very important in Thai culture, where honorifics such as “Krub” for boys and “Ka” for girls are appended at the end of sentences when communicating with elder people. The effectiveness of the IVRS platform was also observed in the school setting, aligning with the findings of Halabi et al. (2017).
Regarding Research Question 2 (RQ2), which aimed to explore the system design that is most suitable for parents and therapists to use, several aspects were considered based on the qualitative data. In terms of software usability, parents highlighted the necessity of a user-friendly interface with clear instructions to facilitate effortless navigation of the system. They emphasized the significance of a platform that clearly defines the goal and objective of each activity, ensuring that parents comprehend its purpose and how it contributes to their child’s development. However, challenges were encountered in accessing the application within the Meta Quest 2 operating system, and parents initially reported difficulties in setting up the Guardian virtual reality headgear. These issues were identified as limitations of the operating system and virtual reality headset technology, and have been addressed in several studies G. G. Lorenzo et al. (2023) and Bravou et al. (2022). To tackle these challenges and enhance the user experience, several adjustments and enhancements are proposed. For the software component, developing a more comprehensive tutorial or walkthrough at the application’s outset is recommended. This tutorial should provide step-by-step guidance on system navigation, including visual cues and interactive prompts, to facilitate understanding of the system’s functionality. Such an approach aims to simplify the operation of the VR environment, making it more accessible to parents and therapists without prior VR experience.
To enhance the theoretical underpinnings of this study, we have integrated relevant theoretical concepts, specifically the Social Motivation Theory of Autism (Burnside et al., 2017; Chevallier et al., 2012). This theory posits that social difficulties in individuals with ASD stem from a fundamental difference in social motivation rather than a lack of social skills. Our findings align with this theory Kourtesis et al. (2023) and G. G. Lorenzo et al. (2023), as the IVRS platform provided an engaging and less anxiety-inducing environment, which in turn enhanced the social motivation of children with ASD. The use of situated naturalistic interventions within the IVRS platform also aligns with educational theories that emphasize the importance of contextual learning and self-observation. These interventions, which occur in realistic and meaningful contexts, help children practice social interactions in a way that is both relevant and motivating. By grounding our findings in these theoretical perspectives, we not only support the observed efficacy of the IVRS platform but also contribute to a deeper understanding of how technology-assisted interventions can be effectively designed and implemented for ASD therapy.
Furthermore, it was discovered that the hardware components of the Meta Quest system were unsuitable for younger children below primary grade 3, as indicated in Figure 9, necessitating modifications to ensure a proper fit. The compatibility of the hardware with younger users presents a significant concern that could potentially affect the effectiveness of the IVRS platform as a therapeutic tool. Discomfort or difficulty in using the headset might detract from the immersive experience, thereby reducing the potential benefits of the intervention. To address this issue, future iterations of the platform could consider partnerships with hardware manufacturers to develop more adaptable headsets that can meet the diverse needs of younger users, as highlighted by Fransson et al. (2020) and Pellas et al. (2021). Additionally, integrating adjustable features or providing supplemental accessories specifically designed for children could enhance the overall user experience and engagement.

The Meta Quest 2 hardware was too big for the head.
Surprisingly, no significant issues related to symptoms such as nausea, dizziness, sweating, or pallor were reported. The children adapted well to the virtual reality environment and enjoyed their experience during the training sessions in our application. However, several studies Newbutt et al. (2016a), Bauer et al. (2022), and K. L. Williams et al. (2024) have found that some children experienced discomfort and cybersickness. These issues may arise from sensory conflict, visual-vestibular mismatch, low frame rates, and latency (Caserman et al., 2021; Ramaseri Chandra et al., 2022). To address these problems, several strategies can be employed: designing activities that minimize rapid or unnatural movements to reduce sensory conflict, synchronizing visual and vestibular inputs to ensure smooth and consistent motion, and developing on PC-based systems to allow high VR applications to run at a high and consistent frame rate (preferably 90 FPS or higher; Rebenitsch & Owen, 2021). Selecting high-end virtual reality hardware can also help reduce latency (Stauffert et al., 2020). Additionally, optimizing the software to reduce latency and improve motion tracking accuracy could further minimize the risk of cybersickness.
To enhance the usability of the hardware, incorporating visual step-by-step guides for headset setup could alleviate the hassle for non-technical users. Simplifying the setup process to be more intuitive, akin to flipping a switch, could significantly increase the system’s accessibility and appeal. Furthermore, ensuring that the software interface is user-friendly and provides clear instructions for navigation and operation is crucial. This would not only make the platform easier to use but also ensure that users can fully leverage its capabilities without requiring extensive technical support. Another solution involves developing the platform using mixed reality technology such as HoloLens 2, Magic Leap 2, and Apple Vision Pro, which have shown fewer instances of these problems (Mosher & Carreon, 2021). Although the cost of such hardware is currently high, future trends indicate a potential decrease in cost.
Regarding the virtual environment design, the development process involved collaboration with specialists from the Rajanagarindra Institute of Child Development and Banprajan Child Center. Because this was the first time working with children with ASD, various prototypes were created and evaluated prior to working with the children. This strategy ensured that the system design was appropriate and effective for the intended target group. In designing the virtual environment, virtual characters, and visual scene color palettes, valuable knowledge and experience were obtained.
The specialists advised that the virtual scenes should not contain excessive objects or fast animations of other children, taking into account the fears and sensitivities commonly observed in ASD children, as noted in previous studies (Pronovost et al., 1966; Z. J. Williams et al., 2021). For instance, in our system, we avoided adding loud noises and a large number of children to the school environment, considering the specific sensitivities of ASD children. In terms of virtual characters, the specialists advised designing the characters’ visual appearance with calming colors, soft, soothing tones, and facial expressions that clearly and exaggeratedly convey emotions. Our animators, being new to working with ASD children, made several modifications, as shown in Figure 10. Finally, the specialists suggested avoiding the use of red, yellow, and white colors in the scene, based on studies by Grandgeorge and Masataka (2016) and Nair et al. (2022), and recommended keeping single-color soft furnishings fairly plain.

Several prototypes of virtual character design in the system.
Conclusions
This study investigated the use of Immersive Virtual Reality Systems as an adjunct therapeutic technique to enhance social interaction and communication skills in children with Autism Spectrum Disorder, with a focus on interactions with friends and teachers within a school setting. During the COVID-19 pandemic, our goal was to develop and evaluate a system that parents could use at home without needing therapist intervention. This system provided a high level of immersion and engagement, allowing children to practice and rehearse scenarios within the safe and controlled environments of their homes or rehabilitation centers. Based on our findings and lessons learned during the development of the tool, we summarize the following points:
- The user interface should clearly outline goals, coaching methods, assessment methods, and enable monitoring of the children’s progress.
- The IVRS cannot be used as the primary tool for intervention but serves as an effective supplementary tool for parents and therapists.
- The virtual reality tool is not suitable for children below Primary 3 due to hardware constraints, such as unsuitable headset size.
- No significant health issues of motion sickness, such as nausea, dizziness, sweating, or pallor, were reported; children could easily adapt to its use, developing on PC-based systems to allow high VR applications to run at a high and consistent frame rate.
- The design of the virtual environment and characters should feature calming colors, soft, soothing tones, and facial expressions that clearly and exaggeratedly convey emotions.
- It is important to avoid adding excessive objects or fast animations of other children, considering the fears and sensitivities commonly observed in children with ASD, and to refrain from introducing loud noises and a large number of children to the school environment.
Practical Implications
The deployment of Immersive Virtual Reality Systems offers significant implications for supporting children with Autism Spectrum Disorder in developing social interaction and communication skills. Our study revealed notable qualitative improvements in participants’ understanding and application of social norms and cultural etiquette, particularly within the context of Thai culture. Parents reported observing their children employing manners and respect in interactions, a direct outcome attributed to their engagement with the IVRS platform. This evidence underscores the platform’s potential as a valuable tool for educators and therapists, suggesting its integration into existing therapeutic practices to complement traditional interventions. Feedback highlighted the necessity for user-friendly interfaces and intuitive navigation, emphasizing the demand for platforms that facilitate ease of use without professional oversight. The study’s qualitative data also suggested areas for enhancement, including the integration of diverse and challenging social scenarios to better mirror real-life interactions. Such improvements could significantly bolster the platform’s effectiveness, offering children a broader spectrum of social experiences to explore and learn from.
Limitation and Future Research
This research into the effectiveness of Immersive Virtual Reality Systems in enhancing social interaction and communication skills among children with Autism Spectrum Disorder provides significant insights but also has limitations that affect the generalizability and reliability of the findings. A primary limitation is the reliance on self-reported data from interviews with parents and therapists, which, while adding qualitative depth, introduces potential biases that can affect the objectivity of the outcomes. Additionally, the study’s specific cultural context in Thailand limits the generalizability of the findings, as cultural nuances significantly influence social interactions and communication norms. Consequently, the applicability of our results to other settings may be reduced. The study employed purposive sampling to meet specific requirements, which inherently limits generalizability. Furthermore, the small sample size of 10 participants constrains the extrapolation of our results to the wider ASD population.
Future research would benefit from larger and more diverse sample sizes to enhance representativeness. Strategies to achieve this include diversified recruitment through engaging with a variety of educational institutions, autism support groups, and community organizations across different regions. Expanding the sample size will allow for more robust data analysis and generalization. Longitudinal studies should be conducted to observe long-term effects and improvements. Additionally, incorporating objective measures alongside self-reported data can validate findings and reduce bias, utilizing standardized behavioral assessments and observational metrics. Exploring technological advancements such as artificial intelligence and generative AI could further personalize the user experience, creating adaptive learning scenarios that evolve based on the child’s progress and interactions. By addressing these limitations and adopting these strategies, future research can build on our findings and contribute to a more comprehensive understanding of the effectiveness of IVRS in supporting children with ASD.
Footnotes
Appendix 1
Acknowledgements
The authors would like to express their gratitude to everyone who participated in this study. The research would not have been possible without the participation and cooperation of the parents, therapists, and children. Their efforts are deeply appreciated and sincerely acknowledged.
Ethical Considerations
This study was approved the ethics by the Research Ethics Committee of the Faculty of Public Health at Chiang Mai University Document No. ET023/2021.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by Chiang Mai University and the National Innovation Agency (NIA), Thailand.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to ethical considerations and in compliance with Research Ethics but are available from the corresponding author on request.