
Abstract
Students with autism spectrum disorders (ASDs) in Saudi Arabia are provided with the educational services they need in their local schools, but a standardized checklist is needed to measure the level of progress and the benefits acquired through the educational programs. This study aimed to standardize a version of Saudi performance norms on the Autism Treatment Evaluation Checklist (ATEC) to explain the raw scores that students with ASDs have obtained, using a sample of teachers and parents. The number of respondents in the study was 334 teachers, and 206 parents. Descriptive statistics, internal consistency, confirmatory factor analysis, reliability coefficients and percentiles were used for analyses. The study found that the ATEC had suitable indicators of validity and reliability, and the percentile ranks were extracted for interpreting the raw scores of the ATEC.
Keywords
Introduction
ASDs is defined as developmental disorders that have a profound impact on social interaction, verbal and nonverbal communication. These disorders appear before the age of 3 years, affecting the achievement of the child’s education. These children also exhibit frequent stereotypical behaviors and the lack of acceptance of daily change, but also the desire for routine and unusual reactions to school experiences (Alotaibi & Almalki, 2016; Alqurashi, 2017; Hemdi & Daley, 2017; U.S. Congress, 2011). Children with ASDs are characterized by stereotypical behaviors, largely because of poor communicative skills, self-centeredness and inability to communicate with their social environment. Full preoccupation with a specific subject is commonplace for children with ASDs (Hume et al., 2019; Nah et al., 2018, Nowell et al., 2019).
The communicative abilities of the individuals with ASDs, ranging in type and severity, vary greatly from both expressive and receptive language to complex verbal and linguistic fluency. The individuals with ASDs are observed to fail to develop expressive language. Those who have acquired the expressive language have difficulty initiating and maintaining interaction and social participation with others as a result of their extraordinary implementation of the language in different social situations. Students with ASDs also suffer from deficiencies in nonverbal communication, which are associated with the delay in their linguistic development. The absence of nonverbal behaviors such as gestures is early indicators of ASDs (Alqahtani, 2012; Angulo-Jiménez & DeThorne, 2019; Haimour & Obaidat, 2013; Hume et al., 2019; Omar, 2014; Wilson et al., 2019).
Since 1996, the interest of the Ministry of Education in Saudi Arabia has been on the children with autism category, that was when King Faisal Specialist Hospital and Research Center recorded cases of children showing autism and needing special care. The Ministry of Education then formed a committee in which the Ministry of Labor and Social Affairs and Doctors at the specialist hospital participated. It was agreed that there are children with autism at the Educational Programs, Institutions and Centers of the Ministry of Labor and Social Affairs (Al-Khashrami, 2003). Since then, a series of procedures have been used in the diagnosis and evaluation processes for children with autism disorders, which include transfer to a pediatric neurologist and the application of the International Classification of Diseases, Tenth revision (ICD.10) lists. The diagnostic lists provided in the Diagnostic and Statistical Manual of Mental Disorders (DSM-4) under the supervision of trained professionals have been used (Al-Khashrami, 2003). However, until the year 2002, the diagnosis of autism disorders in Saudi Arabia was limited to the estimates of clinicians who rely on the available diagnostic norms in DSM-4 and ICD.10, although the most appropriate diagnostic procedures are checklists and assessment norms that were not available in Saudi Arabia until that time. Al-Shammari and Al-Sartawi (2002) were able to verify the validity and reliability of the Childhood Autism Rating Scale (CARS), which was developed by Schopler et al. (1980).
Subsequently, some attempts were made to develop local norms for diagnosing autism spectrum disorders in Saudi Arabia based on international norms, available literature, and available norms in DSM-IV-TR; DSM-5; DSM-4; ICD.10, as reflected in studies by Jaber (2018), Al-Zarea (2005), and Qutb (2012). More efforts were put to adapt international norms in Saudi Arabia, such as in the Humaidan (2007) study that aimed to identify the implications of the validity and reliability of the Saudi version of the psycho-educational scale (third edition). To assess children from the age of 2.5 to 7 years old with Autism spectrum disorders, Psychoeducational Profile-Third Edition (PEP-3) was developed by Schopler et al. (2005). On the same scale, Al-Kindy (2009) conducted a study to prepare a Saudi-Jordanian version of the scale, and Al-Tamimi and Ahmed (2010) investigated the psychometric properties of the second version of the Gilliam scale for autism on a sample from the Saudi environment. In another study, Al-Tamimi (2012) verified the validity and reliability of the present checklist of early identification of Autism disorder (Modified Checklist Autism in Toddlers, M- CHAT) in children under the age of 2 years, and Al-Atwi (2015) developed a Saudi version of the second edition of the Childhood Autism Rating Scale for those with high performance. The Childhood Autism Rating Scale, CARS2-HF2 which aims to diagnose children with autism with high performance and to determine the severity of autism, from simple to medium, or severe. This was prepared by Schopler et al. (2010), and the version that the researcher adapted is one of the three versions of the scale: the Standard version (CARS2-ST), the High-Performance version (CARS2-HF), and the Parents and Care Providers version (CARS2-QPC). Al-Harbi and Audah (2018) verified and checked the significance reliability and validity of the first field of Scale for the diagnostic observation of autism the Autism Diagnostic Observation Schedule (ADOS) prepared by Lord et al. (2000) and Lord et al. (2002). The first domain contained: social communication.
Researchers have long been keen to provide multiple measures to diagnose autism. Over the past 25 years, there has been considerable interest in developing checklists to evaluate the effectiveness of treatments and interventions provided to individuals with autism, due to the importance of this aspect of care. These checklists complement the diagnostic tools used in the early stages of screening and determination of eligibility. The Autism Treatment Evaluation Checklist (Rimland & Edelson, 1999) was developed to evaluate the effectiveness of autism treatments in four aspects of individuals with autism, namely speech/language and communication, sociability, sensory and cognitive awareness, and physical/health behavior.
The Autism Treatment Evaluation Checklist (ATEC) has attained world recognition and was therefore translated into 17 different languages. Since developed, the ATEC has been the most widely used in the field and no other tools appeared to compete with it in evaluating autism treatments and interventions, except for the Mental Synthesis Evaluation Checklist (Braverman et al., 2018) that evaluates the effect of interventions on the speech/language of autistic individuals, which is one of the four aspects of the ATEC.
The ATEC has good psychometric properties in terms of validity and reliability, as revealed by several cross-cultural studies in Thailand (Sunakarach & Kessomboon, 2018, 2022), Iran (Memari et al., 2013), and India (Ghosh et al., 2015; Sapra et al., 2016). It correlated with the Childhood Autism Rating Scale (Geier et al., 2013), which indicated that it has concurrent validity. Research revealed its effectiveness in evaluating the progress of interventions (e.g., Jarusiewicz, 2002; Klaveness et al., 2013; Lonsdale et al., 2002; Rezaei et al., 2018; Weerkamp-Bartholomeus, 2015; Williams et al., 2001; Xu et al., 2018). It also proved effective in assessing interventional effects and tracking behavioral development over time (Jagadeesan et al., 2022; Magiati et al., 2011; Mahapatra, Khokhlovich, et al., 2018). Finally, studies that reviewed autism checklists revealed that it has good psychometric properties (e.g., Hanratty et al., 2015; McConachie et al., 2015).
Very few studies were conducted to validate the ATEC in the Arab environment. Abo-Zaitona (2008) established the checklist’s validity and reliability in Jordan using a sample of 190 participants whose ages ranged between 5 and 13 years. More specifically, the researcher established the checklist’s content validity, discriminative validity, and internal consistency (correlations among items and their respective dimensions). The checklist also proved to have concurrent validity by correlating with the Jordanian version of the Autistic Behavior Checklist (r = 0.74). As to reliability, the checklist yielded an alpha coefficient of .98 for the total score and alpha coefficients of .88 to .96 for the four dimensions. It also yielded inter-rater reliability of .96 for the total score and of .89 to .94 for the four dimensions. In Saudi Arabia, two studies validated the ATEC. The first study was conducted by Al-Backer (2016) to find out the correlation between the CARS and the ATEC. The study was conducted on 40 children who were previously diagnosed with autism at King Khalid University Hospital in Riyadh. The results of the study did not reveal correlation between the CARS and the ATEC. The researcher thus recommended that further research be conducted to validate the ATEC and establish its correlation with other well-established measures. The second study was conducted by Abaoud et al. (2020) to explore the psychometric properties of the ATEC to adapt it for use in the Kingdom of Saudi Arabia. Teachers of 363 autistic children from four age groups in Riyadh completed the ATEC for the participating children. Content validity was then determined by submitting the checklist to qualified referees who agreed on the items with percentages, the least of which was 90%. The internal consistency was established by calculating correlations among items and their respective subscales and among subscales and the total score. The construct validity was also established using exploratory factor analysis of the ATEC subscales and exploring the correlations among the ATEC and the educational stage of the participants. The checklist’s reliability was established by the Alpha Cronbach method. The data revealed that ATEC was completely valid and reliable and therefore could be used in the Saudi context. The results indicated that the Saudi version of the ATEC that was tested in the study could be used to determine the extent to which children with autism benefit from the interventions provided to them in their special educational programs.
Despite the importance of the ATEC to evaluate the effectiveness of treatments and interventions provided to individuals with autism and its excellent psychometric characteristics across cultures, there has been dearth of research deriving its explanatory criteria. It could not find but one study (Mahapatra, Vyshedsky, et al., 2018) which provided criteria for a group that was monitored and voluntarily completed the ATEC assessments during a period of 4 years from 2013 to 2017. Therefore, the researchers seek in this study to provide Saudi criteria for the ATEC based on parents’ and teachers’ ratings. This would allow for interpretation of the results according to an approved reference. It would make possible cross-cultural comparisons with future research. Hopefully, this research endeavor would enrich the literature on this important tool.
Materials and Methods
Participants
The study population consisted of all teachers of students with ASDs (including the parents of the students) in all special education programs approved by Riyadh city, Saudi Arabia, whose number is about 457 teachers according to the Ministry of Education statistics, and 445 parents. All of them were invited to participate in completing the ATEC in order to assess and evaluate the effects of the intervention given to students with ASDs. The number of respondents in the study was 334 teachers (e.g., 79.43% of the total number of autism spectrum disorders teachers), and 206 parents (e.g., 46.29% of the total number of parents). Among the teachers sampled for the study were some male principals n = 4 (1.1%), and female principals n = 19 (5.2%), male-teachers n = 155 (42.7%), and female-teachers n = 185 (51%).
Their responses to the ATEC were n = 268 (73.8%) male-students n = 95 (26.2%) female-students, whose ages ranged between (2 > 6) represented n = 77 (21.2%), (6 > 9) represented n = 99 (27.3%), (9 > 12) represented n = 159 (43.8%), and (<12) represented n = 28 (7.7%). Guardians who participated represented n = 88 (42.7%), mothers who participated represented n = 91(44.2%), and others such as aunts and uncles n = 27 (13.1%). Their responses consist of an estimate of n = 168 (81.6%) male-students, and n = 38 (18.4%) female students, whose ages ranged between (2 > 6) representing n = 61(29.6%), and (6 > 9) representing n = 75 (36.4%), (9 > 12) representing n = 52 (25.2%), and (<12) representing n = 18 (8.7%).
Instrument and Procedures
The study used the ATEC developed by Rimland and Edelson (1999) of the Autism Research Institute in California, to assess the effectiveness of different treatments to children and adults with ASDs and to help parents in determining whether their children benefit from a specific treatment or intervention. Parents and teachers use ATEC to monitor or track the progress of their children over time, even without introducing a new treatment. It mainly provides scores for its sub-parts, in addition to its overall score by comparing treatment and intervention effects and the extent of improvement at a later date. It consists of 77 items distributed over four sub-scales: Speech/Language/Communication (14 items), Sociability (20 items), Sensory/Cognitive Awareness (18 items), and Health/Physical/Behavior (25 items). Response points for the first three sub-metrics consist of three points 0 to 2. The fourth sub-measure, response points consist of four points from 0 to 3.
When applying the ATEC study instrument in their local environment, the researchers obtained the written permission from the Autism Research Institute in California, USA, with the aim of extracting the Saudi norms for the ATEC. Before applying the checklist, the Arabic version available among many other languages on the official website of the Autism Research Institute was identified (online). Then, the checklist’s accuracy of translation was reviewed by three translators who are in the educational field, experienced, fluent and possessing a high level of proficiency in both Arabic and English. They recommended to change some words to adapt with the local cultural context, which were: “Explains what he/she wants” to “Explains what his/her want,”“Speech tends to be meaningful/relevant” to “Speech tends to be meaningful/pertinent,”“Does not wave ‘bye bye’” to “Does not wave Salamu Alaykum,” and Looks at pictures (and T.V.) to “Looks at the pictures and television.”
For ethical considerations in the current study, the researchers completed the official form in the relevant authorities of the Ministry of Education (2020) in Saudi Arabia. After granting the researchers approval, the researchers contacted the participants and informed them that their participation is voluntary, while the information they provided is confidential and will be used only for the research purposes. They were also informed that they can withdraw from the experiment without any risk or punishment.
Content Validity
The researchers presented the Arabic version of the ATEC available on the website of the Autism Research Institute to 10 specialized experts in order to measure the accuracy of the scale when applied in the Saudi environment. All the experts are experienced in the field of autism spectrum disorders, measurement and diagnosis in special education and psychology in the colleges of education in Saudi universities. The idea was to measure the validity of the content of the ATEC, suitability of its phrases, absence of linguistic errors, and to ensure the appropriateness of its subscales for the purpose of the study. The result was the expert’s agreement at a high rate of more than 90%, which ATEC maintained in its 77 items; the researchers later modified the items as requested by the experts and used it for the experiment.
Internal Consistency
To calculate the internal consistency, the researchers calculated the Pearson Correlation Coefficient between the scores of the sample participants (teachers) on each item with the total score of the ATEC and with the total score for each of the main subscale of the ATEC to which those items belong. The results revealed that all the values of the coefficients of the first- subscale items with the total score for the checklist ranged between .291 and .424, and their correlations with the total score of the subscale they belong to, ranged between .397 and .804, all of which are statistically significant values at .01 level of significance.
With regard to the second subscale, it is clear that the values of the coefficients of the correlation of the items with the total score of the ATEC ranged between .333 and .007, and most of them are statistically significant values at .01 level, except for items 1 and 15, which were statistically significant at .05 level; while paragraphs 3, 8, 14, and 18 did not correlate with the total of the checklist, and their correlations were with the total score of the subscale that they belonged to. They ranged between .304 and .460 and all are statistically significant values at the .01 level.
With regard to the third subscales, it became clear that all the values of the coefficients of the correlation of its items with the total score of the checklist ranged between .349 and .558, their correlations with the total score of the subscale to which they belonged ranged between .532 and .758, all are statistically significant at .01 level. With regard to the fourth subscale, it becomes clear that all the values of the correlation coefficients of the total degree of the checklist ranged between .528 and .695, and their correlations with the total score of the subscale to which they belong to, ranged between .626 and .809, all are statistically significant at .01 level. This indicates that ATEC has an internal consistency (Cortina, 1993).
As for the sample of the parents, the results came in all the values of the coefficients of the four subscale items. The first subscale in the total score of the subscale ranged between .540 and .760, all are statistically significant at .01 level; with regard to the second subscale, it is clear that all the values of the correlation of its items with the total degree of the subscale ranged between .198 and .481; all are statistically significant at .01 level. With respect to the third subscale, it is clear that all the values of the standards of the correlation of its paragraphs with the total score of the subscale ranged between .498 and .788; all are statistically significant at (.01 level; with regard to the fourth subscale, it is clear that all the values of the standards of the correlation of its paragraphs with the total score of the subscale ranged between .251 and .666 and all are statistically significant at .01 level, and this indicates that ATEC has an internal consistency (Cortina, 1993).
Confirmatory Factor Analysis (CFA)
To extract the validity indices of the Saudi version of the ATEC, the Confirmatory Factor Analysis (CFA) was conducted. CFA depends on structural equation modeling and allows researchers to identify and test the validity of certain statistical hypothesized models based on theory and/or previous analytic research (MacCallum & Austin, 2000). CFA was conducted in the present study using the statistical program AMOS V25. This analysis was conducted to test four-factor model (Speech/Language/Communication, Sociability, Sensory/Cognitive awareness, and Health/Physical/ Behavior) that was hypothesized by the developers of the checklist. This model was built to represent the checklist’s four dimensions and their associated items as shown in Figure 1. Thus, the main objective of the CFA is to verify the goodness of fit between the hypothesized model and the data of the current sample. A set of statistical indices were adopted to establish the fit of the model:
Chi-square (χ2): its value should be small and statistically insignificant—its high sensitivity to the sample size—its assumption of the normal distribution of the model variables—it is possible to use alternative statistical indices, for example, adopting the ratio between the value of χ2 and degrees of freedom that should be less than 3.
The Root Mean Square Error of Approximate (RMSEA): it should be between 0.09 < 0.05.
Comparative fit Index (CFI): it should be greater than 0.90.
Goodness of fit Index (GFI): it should be greater than 0.80.
Adjusted Goodness of Fit Index (AGFI): it should be greater than 0.80.
Root Mean Square Error of Approximation: a value of less than 0.05 indicates an exact fit of the hypothesized model with the data of the sample—a value between 0.05 and 0.080 indicates a great fit—a value greater than 0.090 indicates misfit and rejection of the model.
The results of the CFA revealed the model’s fit indices shown in Table 1. The results showed that the value of χ2 was 100.331 at a degree of freedom of 51 and a probability of .000, so the ratio between χ2 and the degree of freedom was 1.967, which is less than 3. The values of the RMSEA, the CFI, the GFI, and the AGFI were 0.085, 0.90, 0.93, and 0.90 respectively. By comparing these indices with the criteria adopted by the current study for goodness of fit, the four-factor model is acceptable (Kline, 2015). The four factors were found to be distinctive, but related to each other.
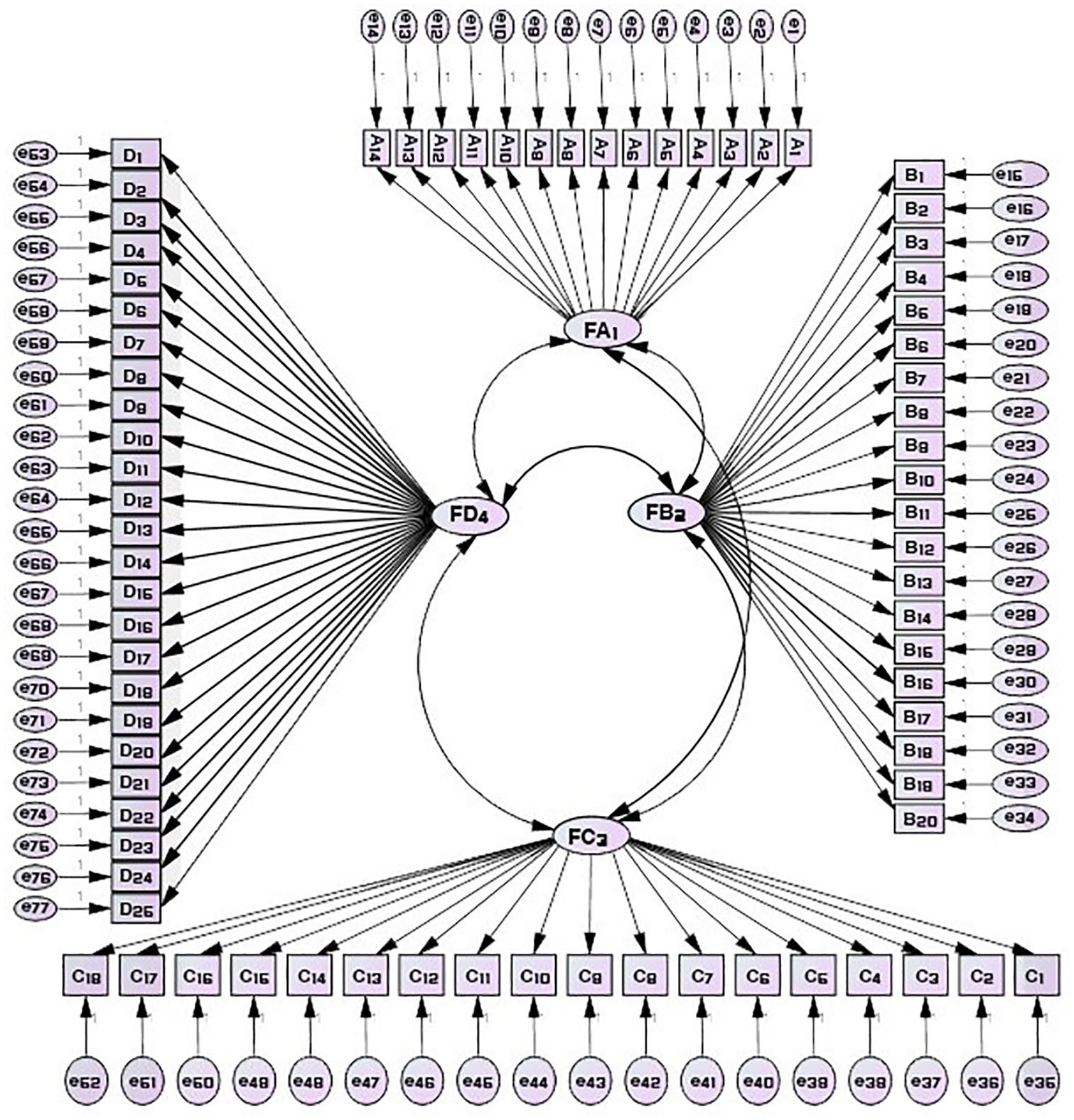
The four-factor model of the ATEC.
Fit Indices of the Four-Factor Model of the Arabic Version of the ATEC.

Reliability of the ATEC
To verify the reliability of the ATEC, researchers used Cronbach’s Alpha coefficient. The results of the teachers’ sample showed that the reliability of the first subscale determined using Cronbach Alpha yielded .91, second subscale yielded .82, third subscale was .93 coefficient, and the fourth was .97. Also, the results of the parents’ sample revealed that the reliability of the alpha coefficient for the first subscale of the checklist is .88, second subscale yielded .75, third subscale is .93, while the fourth subscale yielded .89. The coefficient values indicated that the subscales of ATEC are reliable enough to be used for the study (Cortina, 1993).
Data Analysis
To achieve the aims of this study, Statistical Package for Social Sciences (SPSS) version 26 was used. The following statistical methods were also used: Frequencies and percentages to describe the sample. Percentiles to extract norms according to the percentages corresponding to the raw scores for Saudi society. Pearson correlation coefficient test to extract the validity of the consistency between the existing items and subscales and between the subscales and the overall scores of the checklist. Alpha Cronbach to extract the reliability of the study tool.
Results
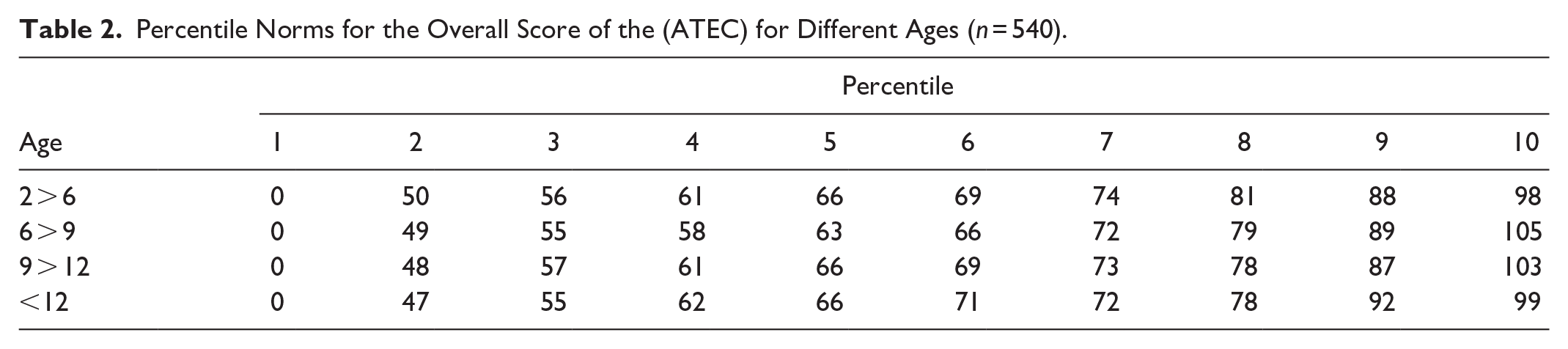
The study of the Saudi norms for performance on the ATEC according to age groups (2–13 and above) was analyzed and the raw scores obtained from students with ASDs in Saudi Arabia was interpreted. After confirming the psychometric properties of the checklist, the percentile norms for the Saudi image were derived from the ATEC according to the division of the test guide, which is 0:9–10:19–20:29–30:39–40:49–50:59–60:69–70:79–80:89–90:99; and the comparison is made according to the corresponding percentages of the Raw Scores. Tables 1 to 6 show the norms for the total score on the checklist and the norms of the total sample for the four subscales.
Tables 2 to 7 explained the interpretation of the grades that students received according to the performance on the ATEC, based on their ages. To evaluate the effects of the intervention provided to students with ASDs, the raw grades were converted into percentile levels that were divided into four age levels corresponding to 9% levels, ranging from simple to acute according to the increase in the value of the ratings viewed for evaluation on the checklist. This study also included the sub norms for the sample of teachers and parents according to the subscale and the overall grade, and they are attached in 10 tables. For more information, please refer to the link (https://cutt.us/xy6pt).
Percentile Norms for the Overall Score of the (ATEC) for Different Ages (n = 540).
Raw Scores and Percentiles of the ATEC for Various Ages (n = 540).

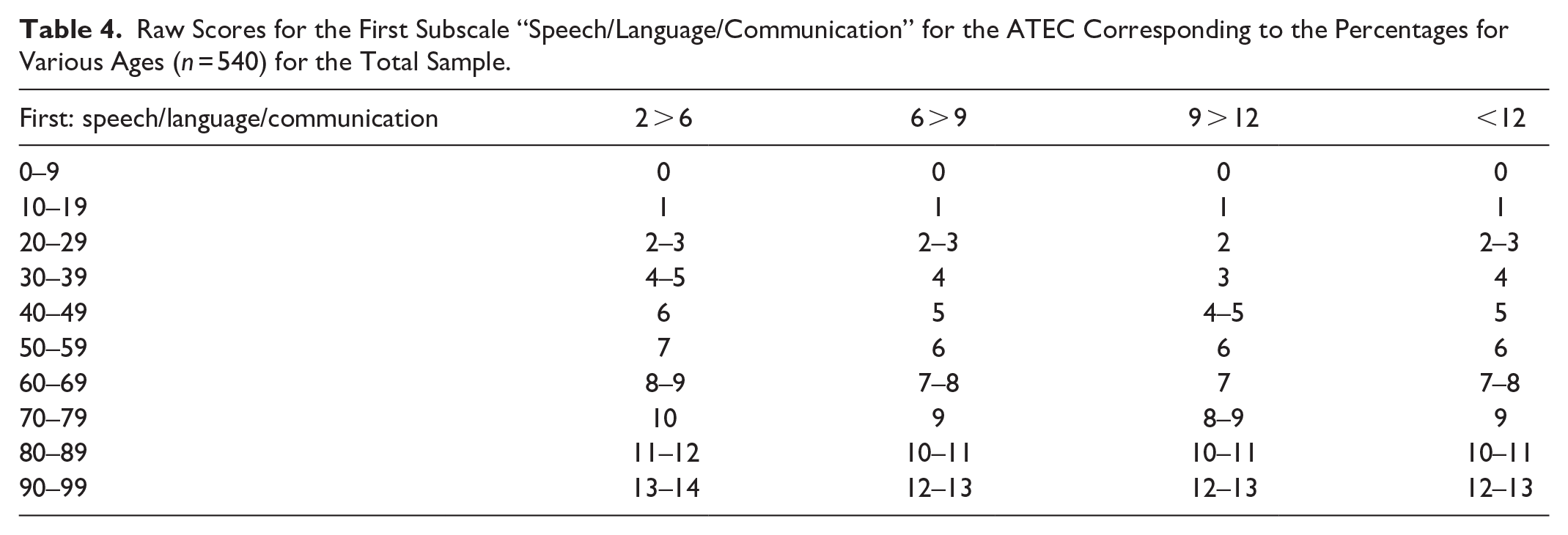
Raw Scores for the First Subscale “Speech/Language/Communication” for the ATEC Corresponding to the Percentages for Various Ages (n = 540) for the Total Sample.
Raw Scores for the Second Subscale “Sociability” for the ATEC Corresponding to the Percentages for Different ages (n = 540) for the Total Sample.

Raw Scores for the Third Subscale “Sensory/Cognitive Awareness” for the ATEC Corresponding to the Percentages for Different Ages (n = 540) for the Total Sample.

Raw Scores for the Fourth Subscale “Health/Physical/Behavior” for the ATEC Corresponding to the Percentages for Different Ages (n = 540) for the Total Sample.

Discussion
The current study aimed at extracting norms for the Saudi version of ATEC, and to prepare tables of norms to interpret the raw score of these norms. The results revealed that the test yielded high indicators of validity and reliability. As the checklist grades were distributed naturally and were close to the moderate distribution, the performance norms’ tables were prepared on the ATEC according to age groups (2–13 and above). This explains the raw degree obtained by students with ASDs in Saudi Arabia using a representative sample consisting of (540) teachers and parents. The norms have been attached according to the four subscales that make up the checklist, namely: First: speech, language, and communication. Second: social interaction. Third: Sensationalism and cognitive study, Fourth: health/body/behavior. Norms appropriate for the theoretical concept in which the test has been prepared accordingly, that is, according to the phenomenon of performance of age advancement. The validity of its use was confirmed in the Saudi Arabian environment because of the availability of the necessary norms for the interpretation of the scores, while limiting the generalizing of the results to Riyadh City only. Through these Saudi norms, the ATEC was completed in this study by teachers and parents, who estimated the impact of the severity of the intervention on the autism status of their students or children, who are of different age groups, in addition to tracking the future course and severity of autism. These norms also allowed the measurement of annual or periodic improvement or lack of improvement, that is, the extent of improvement or deterioration in the situation.
These distributions also set norms for the autism pathway. They target teachers and caregivers in determining and tracking the severity of autism. When tracked annually, these distributions may work like childhood development charts that enable educators and caregivers to enter into informed discussions with therapists and parents regarding treatment efficacy. Parents can also use any of the four subscales independently to assess one or more aspects of the disorder Autism spectrum. Given the scarcity of literature on the norms for the ATEC, according to the research team’s knowledge, the researchers relied heavily on both the studies of Mahapatra, Khokhlovich, et al. (2018). According to studies by these authors, the main variable in the current study was the age variable as the norms were extracted from four age groups, while norms were not extracted according to gender because neither of the two previous studies extracted norms according to age, due to the absence of significant differences attributed to sex in those two studies, as well as the underrepresentation of females in the two studies.
It is noted from the results of the current study that the distribution of raw scores for the overall checklist scores over the hundreds is lower than the international sample scores in the study of Mahapatra, Khokhlovich, et al. (2018), as well as the language and communication subscale scores, in addition to health, body and behavior subscale. The scores of the social interaction subscale in the Saudi sample were higher, and the scores were close between the two samples in the subscale of Sensory/Cognitive awareness. Also, it is noted that the degrees of the sample of teachers and parents in the Saudi sample are close. The difference and variation in the results of the Saudi and international samples can be explained by the effect and effectiveness of the interventions in the four aspects of the checklist, as well as the many cultural differences between these multiple societies.
Implications and Limitations
The findings of the current study concluded that it is possible to use ATEC as a valid, reliable and interpretative reference checklist in assessing the treatment of individuals with ASDs in special education programs and other relevant authorities in Saudi Arabia. This will help to measure the level of the benefit they got from the interventions provided to them in their classes and clinics. Therefore, the relevant authorities in the Ministry of Education should work to approve and apply ATEC for students with ASDs.
Although the study used a large sample relative to similar studies in the region for the derivation of percentile norms of the Saudi version of performance of the checklist, the study sample was relatively small compared to other international researches. Therefore, the researchers recommend that future researches should use larger samples of teachers and parents all over the towns of Saudi Arabia. It is also important to conduct longitudinal studies with individuals with the ASDs and to verify the factual confirmation of the checklist. Despite this, this study, like other studies, is not without some determinants. Despite the current study sought to collect data from the largest possible number of teachers and parents of students with ASDs in all special education programs in Riyadh, the capital city of Saudi Arabia.
Footnotes
Acknowledgements
The authors extend their appreciation to the Researchers Supporting Project number (RSPD2024R705), King Saud University, Riyadh, Saudi Arabia, for funding this work.
Author Contributions
NA, AB, and SF contributed to conception and design of the study. MA organized the database and performed the statistical analysis. NA and AB wrote the first draft of the manuscript. NA, AB, and SF, and MA wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Data Availability Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Researchers Supporting Project number (RSPD2024R705), King Saud University, Riyadh, Saudi Arabia.