
Abstract
Pressure injuries are considered an adverse quality care indicator among hospitalized patients. Despite the importance of routine assessment and pressure injury prevention strategies, nurses may often neglect them. In Ethiopia, pressure injury risk assessment tool such as the Braden Scale has not been reported or implemented in hospital settings. to examine the feasibility of the Braden Scale by assessing the knowledge and attitude of nurses before and after an educational intervention, and testing three delivery methods: printed, oral, or a combination. A quasi-experimental cluster study, on a sample of 145 nurses was conducted. The Participants were selected from units with patients often bedridden and more likely to develop a pressure injury during their hospital stay. Data was collected using structured self-administered questionnaires. A Wilcoxon signed-rank test and independent group test (one-way ANOVA and Kruskal-Wallis test) were used to analyze the data. 68.3% of nurses, were female, with a mean age of 29.4 + 4.9 years and 66.7% had no prior information about the Braden Scale. The overall mean scores change of the pre-to-post educational intervention for knowledge and attitude was statistically significant, p < .001, with a large effect size, 1.95 and 0.81, respectively. nurses attending a brief educational program are feasible and, as a result, are more knowledgeable and have a more positive attitude about utilizing the Braden Scale. Future research is needed on how educational programs such as the ones provided increase the acceptability and implementation of the Braden Scale in practice settings.
Plain language summary
Understanding the Braden Scale helps involve nurses in patient assessments to identify pressure injury high-risk individuals and prioritize preventive measures. Effective pressure injury prevention strategies include routine risk and skin assessments; however, most nurses may often neglect them. In Ethiopia, the Braden Scale has not been reported or implemented in hospital settings. The researchers studied the knowledge and attitude of the nurses about the Braden Scale before and after education intervention and tested the effectiveness of the three education delivery methods (reading printed, oral presentation, or combining both approaches). The study was conducted on a sample of 145 nurses, selected from units with patients often bedridden and more likely to develop a pressure injury, to assess the nurses understanding, and willingness to use the scale. Out of 145 nurse participants, around 2/3 (68.3% n = 99) of the participants were female, with an average age of 29.4 + 4.9 years, the majority 65.5% (n = 95) were between the ages of 23 and 29, and 66.7% (n = 67) had no prior information about the Braden Scale. The overall average scores change in knowledge and attitude before and after the educational intervention was found significant, with a large effect size (d = 1.95 and 0.81), respectively. This study has identified nurses who attend a brief educational program about Braden Scales are more knowledgeable, and have a more positive attitude about utilizing the pressure injury risk assessment tool, feasible for resulting significant change. Future research is needed on how educational programs such as the ones provided increase the acceptability and implementation of the Braden Scale in practice settings. In-service training for nurses, focusing on pressure injury risk assessments, is essential to update their knowledge, and improve patient outcomes, experts should also consider integrating a pressure injury risk assessment score in the nursing process format.
Introduction
Pressure injuries are a common occurrence in patients who are immobile and remain a global health concern with various levels of severity and prevalence rates across different healthcare settings (F. Coyer et al., 2017; Eberlein-Gonska et al., 2013; Kröger et al., 2009). The global prevalence of pressure injury is 12.8%, which indicates the significance of this adverse health occurrence (Z. Li et al., 2020). The pressure injury prevalence increases with age (Zhang et al., 2021) and is highest in low to middle-income countries, where prevalence rates approach 31.3% (Kaddourah et al., 2016). Pressure injury is considered an adverse health occurrence, a negative quality care indicator, and a patient safety risk during hospitalization; thus, it is referred to as hospital-acquired pressure injury (Latimer et al., 2016; Razmus & Bergquist-Beringer, 2017). The incidence of hospital-acquired pressure injury ranges from 0.63% to 8.4% worldwide (Amir et al., 2017; Eberlein-Gonska et al., 2013; Jenkins & O'Neal, 2010; Jiang et al., 2014; Z. Li et al., 2020). It is more commonly associated with various medical devices such as endotracheal and nasogastric tubes (F. M. Coyer et al., 2014), which may reflect a greater illness severity.
Pressure injuries cause a considerable burden as they contribute to greater patient suffering, which may result in life-threatening infections, pain, poor quality of life, impaired recovery, higher mortality rates, and increased healthcare costs (F. M. Coyer et al., 2014). The cost of pressure injury treatment in the United States is estimated to be $11 billion annually (Kane et al., 2017), accounting for a substantial portion of the annual healthcare budget in most countries (Bennett et al., 2004; CEC, 2017; Severens et al., 2002; Soldevilla Agreda et al., 2007). Despite the costs and patient burden of pressure injuries, most are avoidable with early identification using a risk assessment tool and applying appropriate preventive strategies (Gage, 2015; Guy et al., 2013).
The presence of pressure injury is a sensitive quality indicator of nursing care. Nurses are responsible for assessing and identifying patients at high-pressure injury risk (Hunter et al., 2014) and implementing appropriate evidence-based prevention strategies (Latimer et al., 2016; Sving et al., 2014). Studies have shown that the involvement of nurses in pressure injury prevention and quality improvement projects results in a significant reduction of hospital-acquired pressure injuries (Elliott et al., 2008; Fabbruzzo-Cota et al., 2016).
Research suggests that nurses use clinically validated pressure injury risk assessment tools for accurate pressure injury risk prediction. Many pressure injury risk assessment tools have been developed, including the Braden Scale. The Braden Scale is a consistent and precise predictor of pressure injury occurrence in high-risk hospitalized patients (Elliott et al., 2008). Additionally, in many hospitals, the Braden Scale is administered by nurses and integrated into nursing assessment (Mwebaza et al., 2014; Qaseem et al., 2015; Samuriwo & Dowding, 2014) and is also easy to use for pressure injury risk person identification (Kumar et al., 2012). All pressure injury risk assessment tools are based on the most common predisposing factors, such as low sensory perception, physical activity, mobility, nutritional status, high skin moisture, and pressure/shear. These factors have been identified as prominent factors which place the person at higher risk for pressure injury development (Hommel & Santy-Tomlinson, 2018).
The presence or absence of a pressure injury is one metric used to measure the quality of nursing care (Mwebaza et al., 2014). Nurses play a key role in preventing and managing pressure injury. In addition, they are directly involved in risk assessment and preventative strategies before they occur (Qaseem et al., 2015; Samuriwo & Dowding, 2014). Nurses should perform a pressure injury risk assessment and skin inspection during or soon after hospital admission and repeat on a routine basis among patients at higher risk, such as those who are immobilized or if their clinical status deteriorates (Kumar et al., 2012). Pressure injury prevention protocols include systematic and ongoing skin assessment, combined with the implementation of evidence-based pressure injury preventive measures that include skin care, support surface, keep moving, incontinence management, and nutritional assessment (Hommel & Santy-Tomlinson, 2018). These have resulted in lower cumulative incidence rates and milder grades of pressure injury (F. Coyer et al., 2015). Moreover, one study showed a significant (>73%) reduction in pressure injury prevalence in cardio-thoracic ICU after the intervention of quality improvement programs for the front-line healthcare staff including nurses (Gupta et al., 2020).
Despite the availability of risk assessment tools and prevention strategies, optimal reductions in the prevalence rates of pressure injury are often not achieved. Reasons include poor knowledge regarding pressure injuries and poor performance by nurses in assessing, planning, and implementing pressure injury prevention strategies (Latimer et al., 2016). There is also a poorly documented skin assessment by nurses about pressure injury characteristics, staging, and intervention planning (D. Li, 2016). Utilization of evidence-based assessment tools is often not performed but relies on outdated knowledge and experience to make decisions about pressure injury intervention care (Samuriwo & Dowding, 2014). Many nurses are unwilling to adopt evidence-based methods for identifying or managing pressure injuries (Källman & Suserud, 2009). In Ethiopia, there is a lack of literature discussing the Braden scale, a tool used for PI risk assessment. Limited published resources have highlighted gaps in knowledge and practices related to pressure injury prevention (Ebi et al., 2019; Muhammed et al., 2020; Nuru et al., 2015). A study conducted in a particular region of Ethiopia revealed that about 91.5% of nurses displayed inadequate knowledge of PI prevention, which is frequently linked to insufficient training (Ebi et al., 2019).
Research suggests that the quality of nursing care is highly correlated with a positive attitude toward pressure injury prevention strategies, which is influenced by knowledge and personal behavior (Beeckman, Defloor, Schoonhoven, & Vanderwee, 2010; Demarré et al., 2012; Nuru et al., 2015; Qaddumi & Khawaldeh, 2014). In Ethiopia, one study reported that over 50% of bedside nurses had adequate knowledge, favorable attitudes, and were optimistic regarding pressure injury prevention practices (Dilie & Mengistu, 2015). This contrasts with another report in northwest Ethiopia, where nurses demonstrated inadequate knowledge and poor practice regarding pressure injury prevention strategies (Nuru et al., 2015).
Despite the availability of multiple evidence-based validated pressure injury risk assessment scales, they are not currently being used in practice settings in Ethiopia. The objective of this study is to evaluate the impact of educational interventions on Ethiopian staff nurses’ knowledge and attitudes regarding the use of the Braden Scale for assessing pressure injury risk. Additionally, the study aims to identify the most effective method of delivering educational interventions (oral, written, or a combination of both) to improve Ethiopian staff nurses’ knowledge and attitudes toward the Braden Scale and pressure injury risk assessment.
Methods
Study Design and Setting
A quasi-experimental cluster design was conducted in three government-owned hospitals in Addis Ababa, Ethiopia. All three were teaching and referral hospitals and had similar specific units/wards where higher-risk patients for pressure injuries are admitted, including adult general ICU (both medical and surgical), orthopedic, internal medicine, general surgery, and neurology.
Study Population
Participant recruitment took place in specific units after IRB approval and after the purpose of the study was explained. Inclusion criteria included nurses working in medical or surgical ICU, orthopedic, internal medicine, general surgery, or neurology units and directly involved in patient care. Participants had to be working full-time as nursing staff or as a supervisor. The participants also received printed information explaining the purpose of the study and, if there were no questions, were asked to provide their written informed consent for study participation.
Sample Size and Sampling Methods
The sample size was calculated using the G-power software program, using the F-test family repeated measures with the values: Power (1 − β error probability) = 80%, Effect size f (V) = 0.25, the α error probability = .05, number of groups = 3, number of measures = 2, non-sphericity correction € = 1 were considered. The final calculated total sample size (159) was proportionally allotted for each hospital Tikur Anbessa Specialty Hospital = 59, Saint Paul’s Hospital Millenium Medical College = 63, and Menelik-II Referral Hospital = 37; and was based on a total number of nurse staff. The nurse participants were selected randomly from the specific units using simple random sampling technique. In order to choose the participants, a list of names of all nurses from each chosen unit was created, and then random samples were selected.
Data Collection
Data Collection Instruments
The data were collected using self-administered structured questionnaires adapted from the literatures (Abed, 2016; Ahmed Ahmed Qalawa & Ata, 2016; Beeckman, Defloor, Demarré, et al., 2010; Edward et al., 2022). The instrument contained three sections: socio-demographic data and knowledge and attitude questions regarding the Braden Scale.
Socio-demographic characteristics included age, gender, education level, monthly income, years of work experience, bedside work experience, experience with pressure injury care, the workload nurse-to-patient ratio, special training, and access to reading material about pressure injuries.
Knowledge questions regarding the total Braden Scale and sub-scales were adapted from the literatures with a Cronbach alpha coefficient of .83 (Abed, 2016; Ahmed Ahmed Qalawa & Ata, 2016; Braden & Maklebust, 2005; Brown, 2004; Edward et al., 2022). This instrument contained 12 multiple-choice items with response rates recorded as correct, incorrect, or do not know. Knowledge questions consisted of the definition of the Braden Scale, the reason for use, and assessment components (sensory perception, mobility, activity, moisture, nutrition, and friction/shear) and their rating score. Correct responses were scored as “1” and incorrect as “0,” ranging from 0 to 17 points. We used the total sum of the correct answers and converted them into percentages ranging from 0 to 100. Using Bloom’s cut-off points, the knowledge level was classified into three categories: high = 80 to 100%, moderate = 60 to 79%, and low = less than 59%. Higher scores reflected better knowledge of the Braden Scale (Khaled et al., 2020).
A modified 11 items Likert-type scale of the attitude instrument is produced. The content part adapted from Beeckman, Defloor, Demarré, et al. (2010), Beeckman, Defloor, Schoonhoven, and Vanderwee (2010), Attitude toward Pressure ulcer Prevention instrument with the Cronbach alpha = .79, and from Moore and Price (2004) the five points scale has been adapted (Moore & Price, 2004). The original Attitude questions had 13 items covering 5 domains (personal competency, items 1, 2, 3; priority, items 4, 5, 6; impact, items 7, 8, 9; and responsibility, items 10, 11; and confidence, items 12, 13) with each item scored as 1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree. For the modified scale used in this study, only the first 11 items of the attitude questions were used (the 2 confidence items were removed) as they were not in line with the objective and each five-point scale refers to: strongly disagree = “1”, disagree = “2”, neither disagree nor agree = “3”, agree = “4”, and strongly agree = “5”; and reverse rating for negative questions (items 3, 4, 5, 7, 8, 10), total sum measure ranges from 11 to 55 points with a higher score reflecting more positive attitude. We measured with a total mean score of the Likert scale items (11 items), which had been previously validated for PI prevention (Beeckman, Defloor, Demarré, et al., 2010; Beeckman, Defloor, Schoonhoven, & Vanderwee, 2010). Using Bloom’s cut-off point of the total sum, the attitude was grouped into three categories (positive attitude = 44–55, Neutral = 33–43.5, negative attitude = <33 points; Ünver et al., 2017).
Data Collection Procedure
Data collection was carried out similarly for each of the three hospitals. Questionnaires were distributed to participating nurses before the educational intervention session. After a 2-week time frame, the educational program was provided. After the educational intervention, the second questionnaire was distributed within 1 month to the same nurses who completed the pretest.
Education Intervention
Among the three participating hospitals, each received a randomly selected mode of educational intervention delivery. The researcher implemented the educational intervention using three distinct strategies: distributing reading material, delivering an oral presentation with poster support, and combining both approaches. One hospital received written materials for the intervention; another received an oral presentation delivery; the remaining hospital received a combination of written and oral presentations. The nurses in that hospital all received the same intervention on using the Braden Scale for pressure injury risk assessment. This helped to avoid contamination of interventions across units. The principal investigator provided the education intervention at each of the three hospitals. The intervention was conducted in a quiet place near the nurses’ station. All three nursing shifts were provided with the intervention over 1 week for the selected units at each hospital. The educational session for those assigned to the written information group was provided with a printout in the form of a brochure. Nurses who received the oral presentation were provided verbal instruction on the Braden Scale. Those who received the combination intervention received a written brochure and oral poster presentation. Each method of delivery had the same content and was delivered in the same manner for all sessions. The two groups’ oral presentations took approximately 45 min to receive this intervention component. For the written material, the Principal Investigator stayed for about 15 min to answer any questions raised about the Braden Scale. After the educational sessions, the post-intervention survey was conducted. The post-test included the same question as the pretest.
Data Management and Analysis
Descriptive and inferential statistical analyses were conducted. Data were entered into the Epi.info version 4.6, software and transported to SPSS version 26. Data were checked for normal distribution, outliers, and missing data before analysis. The data on inspection and testing using the Kolmogorov-Smirnov test showed an abnormal distribution requiring a non-parametric test. Independent sample t-tests were used to compare knowledge and attitude scores concerning socio-demographic characteristics. A paired sample t-test and one-way ANOVA were used to compare the knowledge and attitude score changes from before and after education interventions and to compare the three educational delivery methods. The Wilcoxon rank test, Mann-Whitney U-test, and the Kruskal Wallis test were used for non-parametric analysis. For the groups that met the assumptions of normality and homogeneity of variance (p > .05), paired t-test was utilized. Statistical significance was determined with a p-value less than .05.
Ethical Approval and Consent to Participants
Ethical Approval was obtained from IRB of the College of Health Science, Saint Paul’s Hospital Millenium Medical College, and Addis Ababa city health office, with Protocol No: 040/20/Nursing, Ref. No.pm23/27 and Ref. No. A/A/A 281/227, respectively. All methods were carried out in accordance with relevant guidelines and regulations or declarations of Helsinki. Thus, all participants received printed information explaining the purpose of the study and, provided their written informed consent for study participation.
Results
A total of 159 questionnaires were distributed to three government-owned hospitals: Tikur Anbessa Specialty Hospital (59), Saint Paul Millenium Medical College Hospital (63), and Menelik-II Referral Hospital (37). The completed questionnaires were collected from each hospital: Tikur Anbessa Specialty Hospital (58), Saint Paul Millenium Medical College Hospital (62), and Menelik-II referral Hospital (25). With 145 (91.2%) completed questionnaires returning. Fourteen (8.8%) were excluded due to a lack of participation at both time points (pre-post-education sessions; Figure 1).
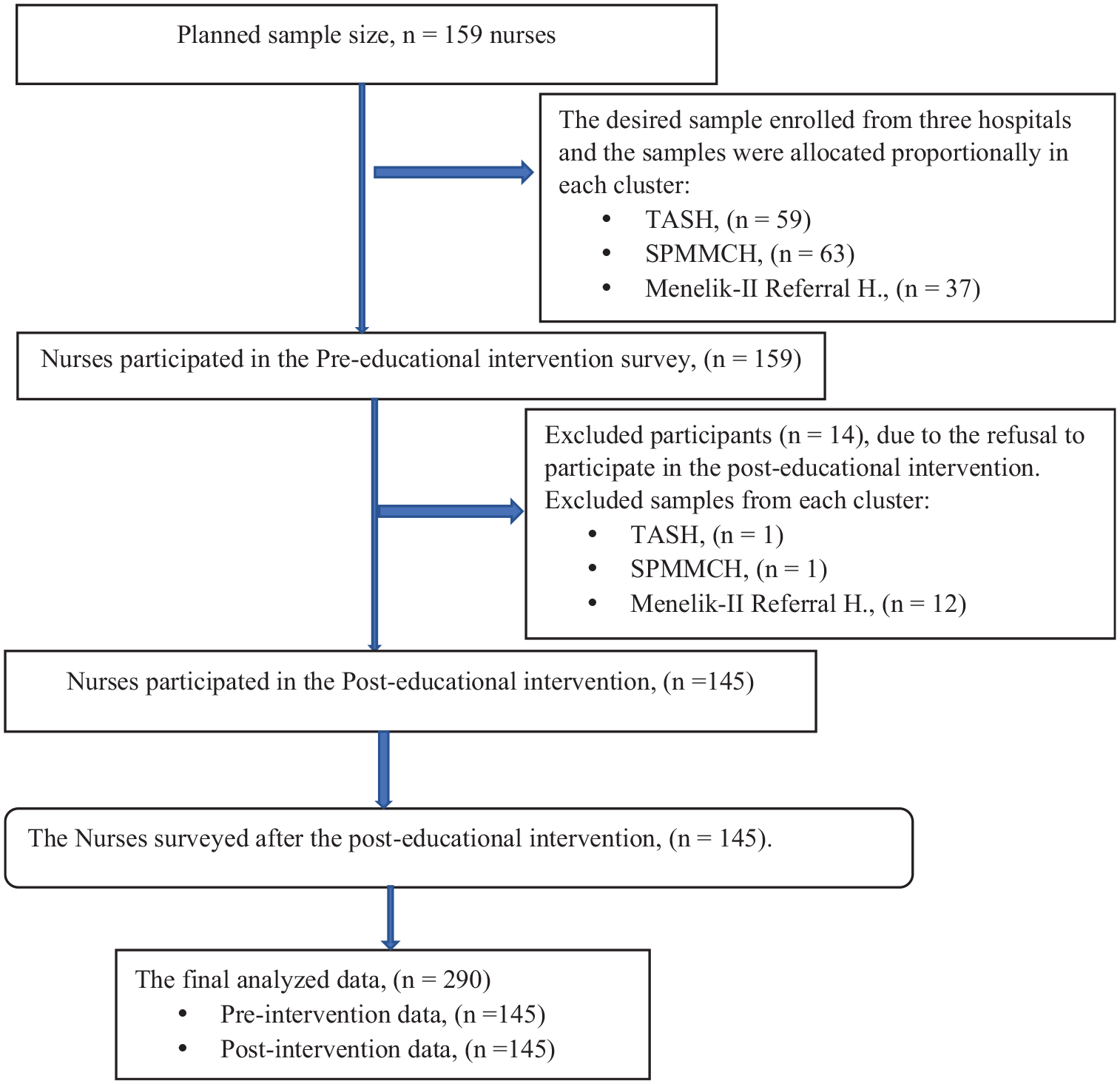
Flow chart for participant inclusion for analysis.
Nurse Participants’ Socio-Demographic Characteristics
Of the sampled 145 nurse participants, 68.3% were female, with a mean age of 29.4 ± 4.9 years. Most 65.5% (n = 95) were between the ages of 23 and 29. Their mean (sd) work experience duration was 6.3 ± 4.88 years. The nurses had similar bedside care experience, with a mean (sd) of 5.27 ± 3.9 years. The majority of participants, 89% (n = 129), were bachelor’s prepared, while 4.1% (n = 6) and 6.9% (n = 10) participants were diploma and master’s prepared, respectively. Their average monthly income was 6,504 ± 1,711birr, equal to 108 ± 29 US dollars ($), and approximately half, 50.3% (n = 70), were married. Most nurses, 67.2% (n = 98), had pressure injury care experience, but 94.5% (n = 137) had not received special training within the last 6 months. More than half, 51.1% (n = 74) of the nurses had a workload of 1:5 nurse-to-patient ratio. Regarding the respondents’ awareness of the Braden scale, 66.7% (n = 97) of the nurses had no information about it, even though 65.5% (n = 95) had access to reading material, or the internet.
Knowledge Score Between Before and After the Educational Intervention
Most nurses were unaware of the Braden Scale; 66.9% (n = 97) and 70.3% (n = 102) did not know the correct definition of the Braden Scale. Less than half, 44.1% (n = 64), understood the importance of the Braden scale for pressure injury risk assessment, while only 17.2% (n = 25) of nurses correctly identified the number of Braden parameters. In addition, 64.8% of the participants did not correctly answer the correct elements of the Braden Scale. Scores improved on the post-test, with 65.5% (n = 95) of nurses responding correctly to the Braden Scale definition to predict pressure injury risk. The importance of the Braden Scale also improved, with 80.7% (n = 117) identifying the correct answer that the Braden Scale is important to assess and predict pressure injury risk. A majority of participants, 63.4% (n = 92), also correctly identified the six Braden sub-scales, and 73.3% correctly stated the elements of the Braden Scale (i.e., sensory perception, mobility, activity, moisture, nutrition, and friction/shear). A similar percentage of nurses (13.8%, 24.1%, and 13.1%) had identified the correct pressure injury risk category expressed by very high risk, moderate risk, and no risk, respectively (Table 1).
Nurses’ Knowledge Assessment Questions Regarding the Braden Scale in Pre- and Post-Educational Intervention, 2021.

Note. The bold referes to correct answer.
In their overall knowledge scores, the pretest results showed 91.7% (n = 133) nurses scored less than 60%, indicated a low knowledge level, while 60% (n = 87) of them scored significantly greater than 80%, a high knowledge level on the post-test evaluation. Based on their score the nurses’ knowledge level is categorized to high (80%–100%), moderate (60%–79%), and low (less than 59%) knowledge level.
Nurses’ Attitude Towards the Braden Scale
A description of the nurses’ attitude toward the Braden Scale before and after the educational intervention in both time points is presented in table below. The participants’ attitudes improved from pre- to post-test, indicating great confidence in using the Braden Scale, and they were more optimistic about implementing it in clinical practice. Although a significant number, 62.1% (n = 90) of nurses strongly disagreed with being responsible for pressure injury risk assessment using the Braden Scale after the educational intervention (Table 2).
Description of the nurses’ attitude score toward the Braden Scale between pre- and post-educational intervention, 2021.

Note. SD = strongly disagree, D = disagree, N = neither disagree nor agree, A = agree, SA = strongly agree; sd = standard deviation.
The attitude scores of nurses after the education session were higher (median = 36) than before-educational intervention scores (Median = 31). According to Bloom’s cut-off point, the overall attitude score of the nurses is categorized to positive (44–55), neutral (33–43.5), and negative attitudes (less than 33) points. The pre-intervention attitude indicated a negative attitude, while the post-intervention became more neutral or positive.
Comparison of the Baseline Knowledge and Attitude Scores by Nurse’s Characteristics
There were no statistically significant differences in baseline (pre-educational intervention) knowledge or attitude scores when comparing nurse characteristics including gender, age, nursing education level, total work experience in years, bedside care experience in years, pressure injury care experience, having special training, workload (nurse-to-patient ratio), and have access of reading material.
Mean Comparison of the Knowledge and Attitude Score in Pre- To- Post-Education Intervention
The mean comparison of the participant’s knowledge and attitude score before and after receiving the educational intervention, there were significant improvements in knowledge and attitude scores from pre- to- post-test evaluation, p < .001, with a large effect size, 1.95, and 0.81, respectively (Table 3).
Summary of the Nurse’s Knowledge and Attitude Scores Toward the Braden Scale Before and After Educational Intervention, 2021.

Note:. Cohen’s D: effect size. sd = standard deviation; Std error = standard error; IQR = inter-quartile range.
The Knowledge and Attitude Score Among the Three Education Delivery Methods
The knowledge and attitude differences were compared by education mode of delivery for printed material, oral presentation, or a combination of both after education intervention. The nurses’ knowledge and attitude scores were higher after the education intervention, but there were no differences in how the information was presented (Table 4).
Summary of the Nurse’s Knowledge and Attitude Scores Toward the Braden Scale Among the Three Education Delivery Methods, 2021.

Note:. sd = standard deviation; Std error = standard error; IQR = inter-quartile range.
Discussion
This study tested knowledge and attitudes among Ethiopian staff nurses employed at three hospitals about the information on a pressure injury risk assessment tool, the Braden Scale, before and after an educational intervention using three delivery methods. Based on the results, approximately two-thirds of the participants were unaware of the Braden Scale. With the educational intervention, the participant nurses have improved their knowledge and awareness of monitoring pressure injuries. Scores improved in knowledge and attitude from pre- to post-test, with no difference observed in how the information was delivered. In addition, we found no differences in knowledge and attitude scores based on nurse characteristics.
Similar to our study, across most studies conducted on the Braden Scale or pressure injury risk assessment, there were changes in knowledge scores that occurred from pre- to post-education interventions (Gaballah & Salah El-Deen, 2021; Kaur et al., 2021; Mohamed & Weheida, 2015; Sarkar, 2018; Suma et al., 2021; Sutherland-Fraser et al., 2012). In India, a study evaluated the effectiveness of structured teaching programs on knowledge score change in the Braden Scale and observed significant changes from pre- to post-test. Other studies show similar findings on nursing students and nurses working in specialized areas such as perioperative and international settings (EL-Khadry et al., 2020). Notably, most of the literature and evidence on using the Braden scale for pressure injury risk assessment has come from high to middle-income countries, with little to no research conducted in low and middle-income countries and is an area for further research investigation.
Regarding knowledge of the Braden Scale, our study report is similar to prior studies conducted in Japan (38%), South East Nigeria (36.3%), India (Vijayapur; 40%), and district Hisar (India; 38.3%; Agorye et al., 2015; Kaur et al., 2021; Kohta et al., 2017; Nadagaddi et al., 2018). Furthermore, unlike ours, in a study report from the Hirsan district, more than 1/3 of the sample (38.3% of nurses) had previous experience with using Braden Scale for pressure injury risk assessment (Kaur et al., 2021). It may reflect differences in the educational system or training.
In prior studies, most nurses showed poor knowledge of the Braden Scale (Khong et al., 2020; Nuru et al., 2015; Qaddumi & Khawaldeh, 2014). For example, in Singapore, the highest proportion (85.6%) of the nurses scored less than 60% on knowledge of the Braden Scale, which is similar to our results. Another study conducted by Sarkar (2018) that examined pre- and post-test changes using an observational checklist revealed that a significant number of nurses (63%) had inadequate knowledge of the Braden Scale assessment, particularly during the pretest (Sarkar, 2018). A study conducted in Gondor, Ethiopia, less than 50% of nurses scored as having poor knowledge on the Braden Scale and PI risk assessment. In contrast to our findings, some reports from India have shown that a lower proportion, 16%, and 20.7%, of staff nurses, had inadequate knowledge of the Braden scale (Clady et al., 2019; Suma et al., 2021). Kaur et al. (2021) reported that no nurse in their study had poor knowledge of the Braden Scale, including during the pretest assessment (Kaur et al., 2021). This wide variation likely reflects differences in nursing education and training or resources available for implementing the Braden Scale.
Training on pressure injury prevention was low in the current study. In contrast to our findings, other studies in Nigeria, India, and Australia have shown that a significant number of nurses (ranging from 20% to 40%) received training on either Braden Scale risk assessment or general pressure injury prevention (Agorye et al., 2015; Nadagaddi et al., 2018; Sutherland-Fraser et al., 2012). Nurses reportedly received formal and specialized training on the pressure injury and risk assessment scales: in Nigeria (37.4%) and Australia (20%) in the last 2 years.
We found no difference in knowledge of the Braden Scale when considering nurses’ socio-demographic characteristics, work-related experience, and history and years of nursing. This is consistent with prior studies conducted in Belgium, India, and Nigeria (Demarré et al., 2012; Edward et al., 2022; Suma et al., 2021). Even though the comparisons were among different categories of nurses, between nurses and nurse assistants, among nurse students, and among staff nurses (before and after the structured teaching program), their characteristics did not change the overall knowledge score on pressure injury risk assessment. However, other studies from India and Indonesia have shown significant knowledge differences due to nurse age, education, and additional training on pressure injury risk assessment (Kaur et al., 2021; Pandhare & Dhudum, 2018; Sari et al., 2021).
Although many studies, including ours, had shown a difference in knowledge score from pre- to post-intervention, no significant differences were reported utilizing different education methods (printed material, oral presentation, and combination of both; McEvoy et al., 2021). A randomized controlled trial conducted by Farshbaf-Khalili et al. (2021) on surgical nurses compared knowledge scores regarding pain management using two education-delivering methods. Nurses in the electronic learning group scored significantly higher in knowledge than those in the lecture format (Farshbaf-Khalili et al., 2021). Providing education in cost-effective ways is essential for nurses to utilize evidence-based practice, such as pressure injury risk assessment, and is an area for further research.
In the current study, we showed significant differences in attitude scores on the Braden Scale between pre- and post-educational intervention. Similar to knowledge, however, there were no attitude differences that occurred due to nurse characteristics or mode of educational delivery. Few studies have been conducted on nurse attitudes related to the Braden Scale or pressure injury risk assessment. Aslan and Yavuz Van Giersbergen (2016) conducted a study in Turkey to assess nurses’ attitudes toward pressure injury prevention. They reported no significant variations in attitude scores based on characteristics except for the last training received. Al-Busaidi et al. (2019) reported that attitude has a significant positive correlation with working experiences in implementing evidence-based practice by nurses (Al-Busaidi et al., 2019). A study by Farshbaf-Khalili et al. (2021) had also shown a significant change in attitude scores after using different education methods, with higher attitude scores toward pain management in the e-learning group than in the lecture group (Farshbaf-Khalili et al., 2021).
Several studies have reported that attitude positively correlates with knowledge of pressure injury prevention and recommends continuing education to improve attitude (Demarré et al., 2012; Grešš Halász et al., 2021).
Strengths and Limitations of the Study
This study is one of the first studies in Ethiopia to examine nurse knowledge and attitudes on the Braden Scale to identify pressure injury risk. Findings from this study indicate that a simple education intervention can change both knowledge and attitudes and serves as a director for future interventions.
The study had several strengths including the use of a quasi-experimental cluster design, utilizing nurses working in three referral hospitals. Because the cluster design was used we were able to avoid contamination between the different educational delivery groups.
The nurses were also very similar across all three hospitals, with no significant differences in work experience or socio-demographics which strengthen our findings.
The study also had limitations such as not being able to be generalized to all nurses working in other types of hospitals in Ethiopia such as private, smaller, or rural hospitals.
Conclusion and Recommendations
The educational intervention provided was successful in positively changing the knowledge and attitude of nurses, regarding the Braden Scale and it is potential use in clinical settings for identifying pressure injury-risk patients. All educational delivery methods were equally effective, indicating that further research is required to identify the most cost-effective one feasible in resource-limited countries such as Ethiopia. It is suggested that in-service training for nurses, focusing on pressure injury risk assessments is essential to enhance their knowledge and improve patient outcomes. Health institutions should consider adopting international pressure injury prevention guidelines, including the Braden Scale, to ensure effective prevention practices. Nurse experts should also consider integrating Braden Scale scoring into the nursing process format as a unified entity.
Footnotes
Acknowledgements
The authors are highly grateful for all who have direct or indirect contributions to completing this study, especially the nurses who were willing to give their time to participate.
Ethical Considerations
Approval was obtained from IRB of College of Health Science (CHS), Saint Paul’s Hospital Millenium Medical College (SPHMMC), and Addis Ababa city health office, with Protocol No: 040/20/Nursing, Ref. No.pm23/27 and Ref. No. A/A/A281/227, respectively.
Consent for Publication
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.