
Abstract
Public attitude and knowledge of antibiotics are determinants of rational use of antibiotics and prevention of antimicrobial drug resistance. This study assessed perception and use of antimicrobials among staff members of a University in Southwestern Nigeria. Descriptive cross-sectional study among 450 staff members of Osun State University in Southwestern Nigeria using multistage sampling method was carried out. Semi-structured self-administered and pre-tested questionnaires were used in data collection. Data were analyzed using the SPSS software Version 17.0. Binary logistic regression models for the outcome variable of composite knowledge and attitude scores toward antimicrobials and their possible predictors were done and level of significance was set at p values ≤ .05 and confidence interval of 95% for all inferential analyses. Mean age of respondents was 26.8 (±11.1) years, and 331 (73.6%) had up to tertiary-level education. One hundred eighty-three (40.7%) and 267 (59.3%) had good and poor knowledge scores, respectively; 175 (38.9%) had positive attitude whereas 275 (61.1%) had negative attitude toward the use of antibiotics. About 279 (62.0%) were informed about judicious use of antibiotics, 398 (88.4%) had ever used antibiotics in the past 1 year with the Ampicillin and Cloxacillin combinations being the most commonly used. Eighty-eight (22.1%) used antibiotics for more than 10 days as at the last use. Predictors for having good knowledge and attitude include age, educational status, and ever having used antibiotics. Inadequate knowledge and attitude toward antibiotics were observed, and this necessitates sustained health education campaign to stakeholders on rational use of antibiotics, especially toward prevention of antimicrobial resistance.
Introduction
The advent of antibiotics has been recognized as one of the greatest innovations that transformed medical and health care, most especially the treatment and outcome of infectious diseases. The issue of antimicrobial resistance now receives attention from stakeholders worldwide to avoid regressing to the pre-antibiotic era, and this may have been responsible for dedication of the theme of WHO day in 2011 to the use of antimicrobials.
As expected, antibiotics among other antimicrobials are on the Nigerian essential drug list and were probably the most commonly prescribed anti-infective agents by both public and private health-care sectors. Rational use of medicines means that “patients receive medications appropriate to their clinical needs, in doses that meet their own individual requirements, for an adequate period of time, and at the lowest cost to them and their community” (WHO, 1987). Irrational use includes use of antibiotics for non-bacterial illnesses and non-adherence to recommended dosing regimens, hence preventing desired therapeutic outcomes from being achieved and potentially increasing antimicrobial resistance (WHO, 2011a).
For young and economically productive age group of people such as a university community, self-medication could be a problem, leading primarily to antibiotic resistance (Dancer, 2004; WHO, 2011b; You et al., 2008). Overuse of antibiotics for many infections, for example, upper respiratory tract infections (URTI), has been reported although the majority of these infections are caused by viruses against which antibiotics have little or no clinical benefit (Gonzales, Steiner, & Sande, 1997; Ochoa et al., 2000).
The escalation of antibiotic resistance poses a significant threat to human health globally. The World Health Report of 2007 highlighted the issue of antibiotic resistance as one of the major threats to public health security in the 21st century. Unfortunately, newer antibiotics that would combat the menace of antibiotic resistance have not been developed, thus constituting public health challenges to concerned stakeholders (Wenzel, 2004). People infected with an antibiotic-resistant organism are more likely to have longer hospital stays and require treatment with second- or third-line drugs that may be less effective, more toxic, and more expensive (Farrell et al., 2005; Levy, 2005).
Although national campaigns have been carried out with the aim of modifying public misconceptions regarding the effectiveness of antibiotics for all types of illnesses, and thus prevent the development of antibiotic resistance (Andre, Vernby, Berg, & Lundborg, 2010; Curry et al., 2006; McNulty, Boyle, Nichols, Clappison, & Davey, 2007a; Woodhead & Finch, 2007), the general public had been reported to have misunderstandings and a lack of knowledge about antibiotics. This has been happening despite national educational campaigns addressing the appropriate use of antibiotics (McNulty, Boyle, Nichols, Clappison, & Davey, 2007b; You et al., 2008).
For effective control and prevention of generalized resistance, countries need to ascertain public knowledge and attitude toward this course with a view to planning policies and programs that would address these problems. A study among multicampus and multicollegiate university community, which consist of staff of different age group and background, could bring out possible risk factors associated with antibiotics misuse. It is against this backdrop that this study assessed the knowledge, perceptions, and use of antibiotics among staff members of a university in Southwestern Nigeria.
Materials and Method
This study was a descriptive cross-sectional study of perceptions and use of antimicrobials among staff members of Osun State University in Southwestern Nigeria. The university runs the collegiate system with six campuses in the following towns: Osogbo (main campus and the capital city and commercial nerve center of Osun state), Okuku, Ejigbo, Ikire, Ipetu-Ijesa, and Ifetedo. The university runs programs ranging from agriculture to engineering and the health sciences. In each campus, staff employed by the university and students coexist in the same community. Each of the six campuses has its own university health center staffed with doctors, nurses, and other health related workers. The study population is the entire workforce of Osun State University. The institution’s staff strength is about 600.
Using the formula for the calculation of sample size for a population less than 10,000 (Olawuyi, 1996), a sample size of 383 was calculated using a knowledge prevalence rate of 48.1% (Awad, Eltayeb, Matowe, & Thalib, 2005). This number was increased to 460 to take care of possible non-response from this study after addition of extra 20%. A multistage sampling method was used in selecting participants into this study. In the first stage, four campuses were chosen out of six by simple random sampling using simple balloting. Questionnaires were proportionately allocated to each campus, namely, Osogbo, Ipetumodu, Ikire, and Ejigbo based on staff population strength. In Stage 2, a list of all departments per colleges was obtained from the administrative college unit.
Based on the university record of 3:2 ratio of academic to non-academic staff, three academic and two non-academic departments were randomly selected from the list using simple balloting. Questionnaires were proportionately allocated to each department. In Stage 3, in a department, a list of all members of staff was obtained from the head of department. A systematic sampling of one in three staff was selected from the sample frame until the desired number was obtained. In case the list was exhausted in a department and there are still a number of participants to recruit, another department was chosen by simple random sampling to complete the systematic selection at departmental level.
Research instruments were semi-structured self-administered questionnaires. The questionnaires were pre-tested among 20 members of staff of the nearby Federal Polytechnic Ede. These research tools were validated by adequate training of research assistants all of whom could fluently speak the local language, translation of questionnaire into local (Yoruba) language, and back translation into English. In addition, there was an agreement on careful choice of local words for some key research words—for the sake of uniformity in data collection. The questionnaires were divided into four sections. Study variables include socio-demographic characteristics of respondents, knowledge about antibiotics, attitude toward use of antibiotics, and practice of the use of antibiotics. Ethical clearance was obtained from the Osun State University, College of Health Sciences Ethical Review Committee. The heads of selected departments and respondents were assured of confidentiality of findings from the study while written informed consent was obtained from every respondent.
The SPSS Version 16.0 software was used for data entry and analysis. Validity of data was ensured by double entry and random checks for errors and outlier values. Relevant frequency distribution tables and summary indices were generated. Composite knowledge and attitude scores were computed with regard to antibiotics, by scoring 1 for each correct answer and 0 for an incorrect answer. These scores were then summed up and divided by the total number of test items to arrive at an average/mean knowledge score per person. Knowledge was graded as follows. From the 14 items on knowledge in the questionnaire, right answers were graded with a score of 1 and wrong answers were graded as 0, thus the minimum obtainable score was 0 and the maximum was 14. The average (mean) score of 7, which is also equal to 50% of the score obtained, was used to divide the respondents into those having good knowledge (those who scored 8 and above) and poor knowledge (those who scored between 0 and 7). Attitudes were graded as “positive and negative.”
The chi-square test was used to demonstrate relationships between relevant categorical variables. Binary logistic regression models for the outcome variable of knowledge and attitude toward antimicrobials (grouped into good and poor) and its possible predictors were done, whereas level of significance was set at p values ≤ .05 for all inferential analyses.
Definition of Terms
Knowledge means familiarity, awareness, or understanding gained through experience or study. It is a sum or range of what has been perceived, discovered, or learned. It may include facts, information, descriptions, or skills acquired through experience or education. It can refer to the theoretical or practical understanding of a subject.
Attitude depicts the way a person views something or tends to behave toward it, often in an evaluative way. It may be also be described as a position of the body indicating mood or emotion.
Perception can simply be defined as the act or faculty of apprehending by means of the senses or the mind, cognition, and awareness.
Results
Table 1 shows personal data of respondents. Mean age of respondents was 26.8 (±11.1) years, with 219 (48.7%) falling into the 21 to 40 years age group. Two hundred seven (46.0%) of the respondents were male, 117 (26.0%) had up to secondary-level education, 331 (73.6%) had up to tertiary-level education, and 335 (74.4%) were Christians.
Personal Data of Respondents.
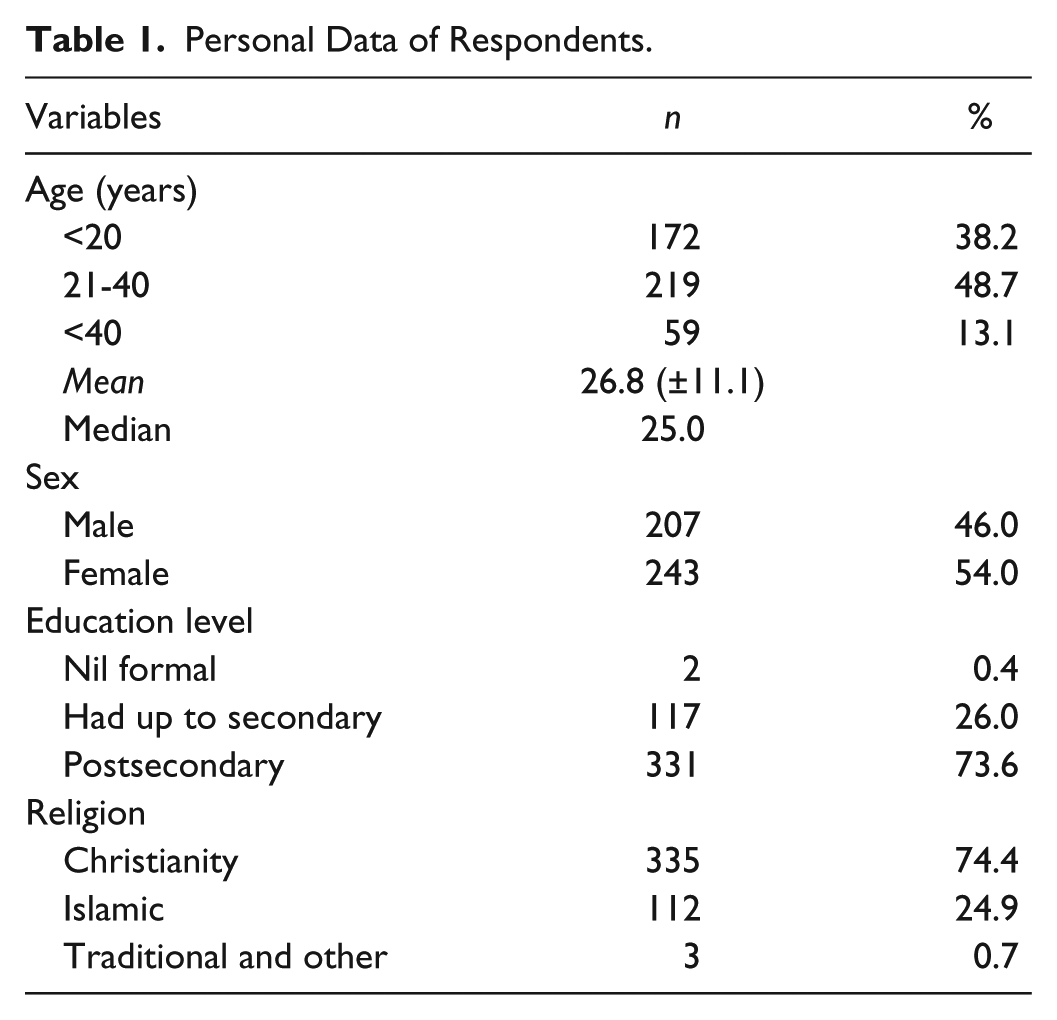
Figure 1 shows knowledge and attitude scores to the use of antimicrobials. One hundred eighty-three (40.7%) had good scores whereas 267 (59.3%) had poor knowledge scores to the use of antimicrobial drugs. One hundred seventy-five (38.9%) had positive attitude whereas 275 (61.1%) had negative attitude toward the use of antimicrobials.

Knowledge and attitude to the use of antibiotics (%).
Table 2 shows pattern of rational use of antibiotics among respondents. Two hundred seventy-nine (62.0%) were informed about judicious or rational use of antibiotics. Major sources of information include health-care workers (153, 34.0%), radio/TV (74, 16.5%), and friends (49, 10.8%).
Rational Use of Antibiotics.

Three hundred ninety-eight (88.4%) had ever used antibiotics.
Common antibiotics used the last time by respondents included Ampicillin+Cloxacillin (88, 19.6%), Ampicillin (46, 10.2%), Cotrimoxazole (39, 8.7%), Ciprofloxacin (32, 7.1%), Tetracycline (23, 5.1%), Amoxicillin (15, 3.3%), and Metronidazole (12, 2.7%) while antimalarials were believed and mentioned to be antibiotics among 21 (4.7%) respondents. Average number of days that respondents used antibiotics was for more than 10 days among 88 (22.1%) respondents. The last antibiotics used was prescribed by a doctor among 277 (69.6%) of the respondents.
Among those not prescribed by a doctor, 81 (18.0%) respondents self-prescribed, 30 (6.7%) of the respondents had chemists and non-doctor health-care workers prescribe for them, and 5 (1.1%) of the respondents got their friends to prescribe for them. Only 307 (77.1%) completed their last dose of antibiotics. Reasons for non-completion of last dose were that ailment subsided, non-affordability, respondents got better, respondents did not just like taking drugs generally, respondents did not buy enough drugs right from the start, side effects mostly nausea, and fear of side effects. One hundred eleven (27.9%) did a laboratory test before they commenced treatment the last time they used antibiotics. Seventy-nine (19.9%) said they used two antibiotics at a time whereas 35 (8.7%) used more than two at a time. Common reasons for using more than one antibiotics together include works faster, wants ailment to go faster, doctors prescribed it, effectiveness and quick relief, and for broad coverage. Two hundred six (51.8%) sometimes buy and use antibiotics by self while 186 (41.3% of all respondents) sometimes prescribe antibiotics to others.
Table 3 shows binary logistic regression models for the outcome variable of knowledge and attitude toward antimicrobials (grouped into good and poor for knowledge, and as positive and negative for attitude) and its possible predictors. In Table 3 (Section A), for the variable “Age Group” using 41 years and above as reference, respondents aged 20 years or less were about five times (1/0.189) less likely to have good knowledge of antimicrobials than those who were 41 years and above (odds ratio [OR] = 0.189, 95% confidence interval (CI) = [0.091, 0.393], p < .001). Similarly, respondents who were aged between 21 and 40 years were about three times (1/0.316) less likely to have good knowledge than those who were 41 years and above (OR = 0.316, 96% CI = [0.163, 0.615], p = .001)
Binary Logistic Regression Models for the Outcome Variable of Knowledge and Attitude Toward Antimicrobials (Grouped Into Good and Poor) and Its Possible Predictors.

Note. Variables in this model—sex, religion, age group, educational status, have been informed about antimicrobials, ever used antimicrobials.
Statistically significant.
For the variable “Educational Status” using high educational status as reference, respondents with low educational status were about two times less likely (1/0.440) to have good knowledge of antimicrobials than those with high educational status (OR = 0.440, 95% CI = [0.256, 0.755], p = .003). For the variable “Ever Used Antimicrobials” using Yes as reference, respondents who had not used or who do not know whether they have used antimicrobials were about three times less likely (1/0.363) to have good knowledge of antimicrobials than those who have used antimicrobials (OR = 0.363, 95% CI = [0.169, 0.779], p = .009). Thus, predictors for having good knowledge of antibiotics in this model included age, educational status, and ever having used antibiotics.
In Table 3 (Section B), for the variable “Educational Status” using high educational status as reference, respondents with low educational status were about 1.3 times less likely (1/0.778) to have positive attitude toward antimicrobials’ use than those with high educational status, although this was found not statistically significant (OR = 0.778, 95% CI [0.465, 1.300], p = .338). For the variable “Ever Used Antimicrobials” using Yes as reference, respondents who had not used or who do not know whether they had used antimicrobials were about three and a half times less likely (1/0.271) to have positive attitude toward antimicrobials’ use than those who had used antimicrobials (OR = 0.271, 95% CI [0.116, 0.630], p = .002). Thus, predictors for having positive attitude toward antimicrobials use in this model include educational status and ever having used antibiotics.
Discussion
This study reported good knowledge and attitude scores among two fifths and poor knowledge and attitude scores on antibiotics among a little less than two thirds of the respondents. This inadequate knowledge and attitude support other studies (Kim, Moon, & Kim, 2011; Ling Oh et al., 2010). Considerable bodies of evidence from many studies have demonstrated widespread problems in knowledge, attitudes, beliefs, and behaviors among consumers, which influence their antibiotic usage (Emslie & Bond, 2003; Hawkings, Butler, & Wood, 2008; McNulty et al., 2007a; Parimi, Pereira, & Prabhakar, 2002; Vanden Eng et al., 2003). Poor knowledge on antibiotics may determine attitude to its use and eventual practice of use of antibiotics. In as much as resistance to antibiotics is possible following poor compliance from poor attitude to its use, such issues should be taken as a matter of importance.
Studies have also suggested that adequate knowledge of appropriate antibiotic use was a predictor of a good attitude and behavior (Ling Oh et al., 2010; Parimi et al., 2002). However, some studies have reported high general awareness about antibiotics (Andre et al., 2010; McNulty et al., 2007a, 2007b; You et al., 2008), although better awareness may not necessarily imply appropriate attitude in relation to antibiotics use (Ling Oh et al., 2010). This may support good knowledge rather than just awareness of antibiotics.
About two third of our respondents were informed about judicious or rational use of antibiotics whereas less than a third of them could describe them correctly. In a related study, three quarter had heard of antibiotics although only a quarter of the respondents described them correctly (Mwambete, 2009). The electronic media and health workers being leading sources of information about antibiotics is an expected positive development because an average household in Nigeria have access to TV and radio in their homes while the University health center is accessible to all University staff.
Most respondents have used antibiotics in the past 1 year; this supports other studies (Awad et al., 2005; Mwambete, 2009). The penicillins are the two leading antibiotics used, and this supports another study (Malaysian Statistics on Medicine, 2005). Penicillins like many other antibiotics are easily accessible as over-the-counter drugs, which may be sold without doctor’s prescription or query to use. The implication of this is that antibiotic may be used without following due prescription.
The last antibiotics used by respondents were prescribed by a doctor among about two thirds of our respondents. This supports another study (Mazińska & Hryniewicz, 2010). However, in another study (Ling Oh et al., 2010), only about one third took these drugs without prescription, and this portrays the level of restrictions placed generally on drugs most especially antimicrobials in some countries, to prevent occurrence of antimicrobial resistance. It is the duty of the community pharmacist to enlighten the clients on correct dose and time of taking these drugs most especially when clients do not bring prescription before buying the antibiotics.
Majority of our respondents claimed they completed their last dose of antibiotics, and among reasons for non-completion of last dose were that the ailment subsided and they got better. This disagrees with another study in which three quarter said they would stop taking a course of antibiotics when they felt better (Kim et al., 2011), and another in which a little over half said they would stop (You et al., 2008). Our findings however agree with a study in which only few (13%) said they would stop (McNulty et al., 2007b). These could only lead to more and more resistance to common antibiotics. Antibiotic resistance has increased dramatically over the past 10 years; in many countries, penicillin resistance to Streptococcus pneumoniae is nearly 50%, with resistance to other drugs rising as well (Hueston & Dickerson, 2001). The need for continuous health education campaign on judicious use of antibiotics and other antimicrobial is important. “Judicious use” is using an antimicrobial drug appropriately and only when necessary.
The fact that an appreciable proportion of our respondents sometimes buy and use antibiotics as self-medication and even prescribe antibiotics to others portrays some element of self-medication. This constitutes potential threat to rational use of antibiotics and occurrence of antibiotic resistance. In a similar supportive study, more than one third of the respondents wrongly self-medicate themselves with antibiotics once they have a cold (Ling Oh et al., 2010), a condition that may not be susceptible to antibiotics. Thus, educational interventions are needed to promote prudent use of antibiotics among the public.
In this study, some respondents took different or multiple antibiotics simultaneously to treat one illness, suggesting polypharmacy. This supports another study (Rambhade, Chakarborty, Shrivastava, Patil, & Rambhade, 2012). This situation may have been caused by clients themselves who may believe that illnesses would go faster (Kim et al., 2011) or due to their poor knowledge about antibiotics as discussed or even due to the inappropriate prescriptions by health-care workers.
Predictors for having good knowledge of antibiotics in this model include age, educational status, and ever having used antibiotics, whereas predictors for having positive attitude toward antimicrobials use in this model include educational status and ever having used antibiotics. This supports other studies (Kim et al., 2011; Ling Oh et al., 2010). As documented, a higher educational level has been associated with better knowledge and attitude (Parimi et al., 2002; You et al., 2008) and even better understanding and interpretation of events.
A limitation to this study was that questions asked regarding the use of antibiotics were retrospective in nature, and the probability of a recall bias is there. However, knowledge and attitude questions were examined in the present study. The simple language in which the practice questions were asked also created avenues for easy understanding of the questions and reduction of bias in responses to the nearest minimum. Misinterpretation or misrepresentation of names of drugs could have also been a limitation to this study, but respondents were asked to freely give names of drugs they have used and not to make choice from a given or reference list.
Conclusion
This study assessed the perceptions and use of antibiotics among the staff members of a university in Southwestern Nigeria. Good knowledge and positive attitude scores were found among two fifths whereas poor knowledge and negative attitude scores on antibiotics were among two thirds of the respondents, and these depict inadequate knowledge and attitude to use of antibiotics. Various factors constituting irrational use of antibiotics were prominent. We recommend organized, continuous, and sustained health education campaign programs on antibiotics’ use and targeting stakeholders including prescribers and consumers to promote prudent use of antibiotics among the public.
Footnotes
Acknowledgements
Authors hereby appreciate the management and staff members of Osun State University for their full participation as well as cooperation toward the conduct of this self-funded study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.