
Abstract
This study extends existing literature on the balance of tangible and intangible support and services that older adults require for their social inclusion and dignified aging. The study makes a contribution to current literature on older adults’ social exclusion-inclusion in the context of Ghana from the lenses of critical gerontology, social exclusion theory, and human rights. A qualitative description approach was adopted, with a purposive sample of 18 older adults who provided data in individual interviews, and the data were analyzed thematically. Although Ghana has made some policy efforts at ensuring the well-being of older adults, findings of this study suggest that many older Ghanaians are forgotten, socially excluded, and falling through cracks in the social safety net. For their social inclusion, older adults require tangible and intangible forms of support that enable them achieve adequacy with basic needs, and social participation. An important form of tangible support older adults need is care, where they are provided with adequate food, clothing, housing, and income. Intangible forms of support that older adults need include guaranteeing them access to health care services where costs (of treatment, laboratory examination, or prescription medication) are not a structural barrier, and by supporting them with mobility and social and civic participation, where they participate in decision making, perform meaningful social roles, and have opportunities for social interactions. Policy and practice implications of the findings are discussed.
Plain language summary
This qualitative descriptive study used data provided by a sample of 18 older adults aged 60 years and older from the Tamale Metropolitan Assembly of Northern Region, Ghana, to explore society’s attitude toward older adults, and the types of support older adults require to feel socially include and live in dignity. The data were collected in individual interviews and analyzed thematically. Two main themes established in the data are we are forgotten and social inclusion. We are forgotten discusses feelings and experiences of neglect, deprivation, and being excluded, whereas social inclusion discusses tangible (such as guaranteed income) and intangible (such as free healthcare and bus rides) types of support that participants require to be socially integrated and live in dignity. The findings and their implications are discussed.
Introduction
It is important for all people to experience a sense of context and meaning throughout their life. When increasing demands for services and care arise, support from society needs to be designed to minimise anxiety and distress and to allow that a social life can be maintained. It is important to grant elderly women and men the right to “live until you die” and that everyday life … is active, understandable, manageable and meaningful. (Chi, 2014, p. 45).
Population aging in West Africa has become a topical issue for policy makers and researchers (Issahaku & Neysmith, 2013). Ghana is a typical example of these countries whose populations are aging (Kpessa-Whyte, 2018; Kpessa-Whyte & Tsekpo, 2020). Available statistics on Ghana’s demographic transition indicate that the population of older adults, defined as persons who are aged 60 years and above (Social Security and National Insurance Trust, n. d; Ministry of Gender, Children and Social Protection, 2010), increased from 200,000 in 1960 to 2 million in 2021 (Ghana Statistical Service, 2022). This steady rise in the population of older Ghanaians can be attributed to improvements in overall life expectancy. For instance, in 1960 the average life expectancy in Ghana was 47 years. Subsequently, Ghana’s average life expectancy rose to 51 years in 1980, 58 years in 2000, and 64 years in 2020 (World Bank, n. d). The upward trend in the average life span is the reason for the size of the population of older Ghanaians recorded in the most recent census; 2 million out of a total national population of 30.8 million (Ghana Statistical Service, 2022). With aging comes increased challenges related to health, socio-emotional care, activities of daily living (ADL), limited income, social isolation, and social participation (Ghana Statistical Service, 2014, 2019, 2022; Kpessa-Whyte, 2018; Kpessa-Whyte & Tsekpo, 2020; Kwankye, 2013). As a result, there is concern that unless stakeholders actively pursue policies that offer older adults opportunities to give and receive support, an increased number of older adults will become socially excluded (HelpAge International, 2008) and face increased risks for socioeconomic deprivation (Ghana Statistical Service, 2022; Kröger et al., 2019; World Health Organization, 2015, 2022). This is where the epigraph to the introduction (Chi, 2014) has resonance. Ghana has an aging policy whose goal is “to achieve the overall social, economic and cultural re-integration of older persons into mainstream society, to enable them as far as practicable to participate fully in the national development process” (Ministry of Gender, Children and Social Protection, 2010, p. 8). The policy commits to guaranteeing older adults’ human rights, including social participation, “support and care … security and freedom from exploitation” (Ministry of Gender, Children and Social Protection, 2010, p. 8). The Livelihood Empowerment against Poverty (LEAP) program and the National Health Insurance Scheme (NHIS; Ministry of Gender, Children and Social Protection, 2010, 2018) are programs that are supposed to give practical meaning to provisions of the aging policy. However, these programs support only a minority of older Ghanaians (Handa et al., 2014; Kuuire et al., 2017; Ministry of Gender, Children and Social Protection, 2018), while the majority fall through the cracks. In addition, there are concerns that, increasingly, the informal systems are not responding adequately to the support needs of older adults, and thus are exposing them to social exclusion and deprivation (Aboderin, 2003, 2004a; Braimah & Rosenberg, 2021; Coe, 2017, 2019; Nkansah et al., 2021; van der Geest, 2016).
The purpose of this study is to explore society’s attitude toward older adults in Ghana, and older adults’ socioeconomic support expectations for social inclusion and dignified aging. The main question of the study is: What is the general attitude of the Ghanaian society toward older adults, and what types and sources of support do older adults require for social inclusion and dignified aging? The study explores this question through a qualitative description research approach and with critical gerontology (Estes & Grossman, 2007; Holstein & Minkler, 2007; Moody, 1993) augmented by human rights perspectives (Cox, 2015; Harbison, 2022) and social exclusion theory (Levitas et al., 2007; Walsh et al., 2021) as a theoretical framework. The current study is novel in that, although some studies have explored older adults’ health care expectations (Gyasi, 2018; Issahaku & Sulemana, 2021) and their experiences with isolation and neglect (Braimah & Rosenberg, 2021; Nkansah et al., 2021; van der Geest, 2016), no study has addressed the question proposed here and with the approach adopted in this study. The study therefore contributes to discussions on the social exclusion-inclusion of older adults and dignified aging in Ghana. For this study, society is used to refer to the public governmental and non-governmental systems as well as communities, families, and individual actors (Nukunya, 2016), support refers to tangible and intangible assistance through which needs are met and well-being promoted (King, 2017; Lyons & Zarit, 1999; McCamish-Svensson et al., 1999), and dignified aging refers to the process by which older adults are enabled to realize “their potential for physical, social and mental well-being … to participate in society … to extend healthy life expectancy and quality of life for all people as they age.” (Chi, 2014, p. 46).
Literature Review
Social Support
Support has been conceptualized as the flow of psychological and material resources and services through prevailing social networks to enhance a person’s overall well-being (Bernal et al., 2003; Cohen, 2004). Cohen (2004) identified three types of resources transmitted in a supportive network of relationships; instrumental (e.g., financial help or help with daily tasks), informational (e.g., advice or help with problem-solving guidelines), and emotional (e.g., caring, comforting, empathizing, or providing assurance). Support is also conceptualized as formal and informal based on its source (Cantor, 1979; Lyons & Zarit, 1999; McCamish-Svensson et al., 1999; Mumtaz, 2022). McCamish-Svensson et al. (1999) use the term formal support to refer to services and/or resources funded and provided by publicly mandated agencies “or otherwise privately financed services” whereas informal support “refers to services rendered by family, friends and others who are not part of the state or municipal public care system” (p. 164). In a synthesis of the literature on social protection, Mumtaz (2022) defined informal support as informal and privately arranged interventions by family, friends, neighbors, community groups, and religious organizations that provide material and socioemotional support to those most in need of assistance. Formal and informal support are known to have beneficial effects on overall health and subjective well-being (Bigonnesse & Chaudhury, 2020; Cohen, 2004). According to Cohen (2004), supports have a positive effect on overall well-being by acting as a buffer against stress and by promoting “positive psychological states (e.g., identity, purpose, self-worth, and positive affect)…” (p. 677).
Older Adults and Social Support
Empirical literature on support for older adults can be organized around two themes; the types of support older adults need and receive or do not receive, and the impact of support or lack of support on the well-being of older adults.
Types of Support Older Adults Need
Literature on the types of support older Ghanaians need and receive or do not receive is currently limited but instructive. Among the few studies, one study found that older adults needed support with activities of daily living (ADL), feeding/food security, and water and sanitation services (Braimah & Rosenberg, 2021) but did not have it. The strength of this study is that it collected data from a sizable sample of 43 older Ghanaians through interviews and sharing circles (Braimah & Rosenberg, 2021). According to Braimah and Rosenberg (2021), only a few female and rural participants reported receiving support with feeding from their informal networks, and cash assistance from the LEAP program. Older Ghanaians also need an income stream to meet their healthcare, housing, and nutritional needs, but lack financial support (Nkansah et al., 2021). In a sample of 12 participants, Nkansah et al. (2021) found that almost everyone was neglected; excluded from social networks, lacked decent housing, and lived in loneliness. Nkansah et al.’s (2021) study used a relatively small sample, however, their findings resonate with those of Braimah and Rosenberg’s (2021) study. Together, these findings suggest that older Ghanaians do not get the support that they need, and confirm the conclusion made by the Ghana Statistical Service (2022) that many older Ghanaians live in multidimensional poverty.
In large measure, the international literature has explored the types of support older adults need for social inclusion and dignified aging. Studies have elucidated older adults’ need for formal and informal support, such as informational, task-related, and mobility services (Naaldenberg et al., 2011) and opportunities for social participation in the community (Bacsu et al., 2014; Nelson & Rosenberg, 2022). In some of these studies older adults have expected opportunities to join friendship and sharing circles, and for self-employment, as this would promote dignity and independence (Bacsu et al., 2014). In addition, older adults do need to have strong connections with family, neighbors, the religious community, and public assistance programs to enhance dignity and life satisfaction. For example, in one US study, older adults wanted more closeness with family, neighbors, the Church, and social security programs from which they would receive instrumental and non-instrumental support (Bryant et al., 2001).
Older Adults and Social Care
Another focal area of research is older adults’ need for care. Existing research has explored whether and how much care older adults receive and what type of care they prefer to receive from formal and informal sources. Among the questions explored are whether formal care services substitute or complement informal care (Litwin & Attias-Donfut, 2009) and whether older adults prefer formal to informal care (Lee et al., 2022; Naganathan et al., 2016; Rapolienė & Gedvilaitė- Kordušienė, 2022; Wee et al., 2015). An important finding in some of the studies is that many older adults are faced with unmet care needs, whether they expect care from formal or informal sources (Kröger et al., 2019; Verver et al., 2018). Research in Africa especially highlights the unmet health care needs of older adults, which is due to non-functional health insurance programs or non-enrollment on these programs as well as the absence of geriatric specialists (Gyasi, 2018; Parmar et al., 2014; Saka et al., 2019). Some studies have shown that older adults receive or expect care from both formal and informal networks, especially “in situations of greater need” (Litwin & Attias-Donfut, 2009, p. 71). However, in other studies, older adults either prefer formal over informal care or vice versa. For example, in one West African study, older adults expected care solely from family and kin as a filial obligation (Ene et al., 2022), while in a Hong Kong study older adults preferred formal care services over informal care (Bai, 2019). Other studies suggest that familiarity informs older adults’ determination of the type and source of care they need. For example, a Canadian study found that older adults who were currently receiving care primarily from the formal system preferred this type of care, and vice versa (Lee et al., 2022). Some research has also shown that older adults prefer the type of care that enhances their dignity, independence, and self-determination over other health and safety considerations (Naganathan et al., 2016; Rapolienė & Gedvilaitė- Kordušienė, 2022; Wee et al., 2015).
Impact of Support
Extant research has also explored the impact of formal and informal support on older adults’ well-being and life satisfaction (Abramowska-Kmon et al., 2023; T. Shen et al., 2022; Y. Shen & Yeatts, 2013). Some multi-country studies have found that regular receipt of informal support improves the subjective well-being of older adults, and that perceptions of the amount of support received make a difference in levels of subjective well-being (Abramowska-Kmon et al., 2023). Formal and informal support also has beneficial effects on older adults’ mental health, overall health, and life satisfaction. One study found that formal and informal support contributed to improved overall quality of life of older adults, but informal support had a relatively greater effect (T. Shen et al., 2022). In another study researchers found that a strong connection to social networks greatly improved the quality of life of older immigrants (Nakash et al., 2021). If the presence of social support has beneficial effects, then its absence may bring negative consequences. This point has been highlighted in the literature. In general, the research shows that a lack of social support is associated with physical health deficits and psychological distress due to loneliness, food insecurity, poor hygiene, and indecent housing (Braimah & Rosenberg, 2021; Gyasi, 2019; Gyasi, Phillips, & Abass, 2019; Gyasi, Phillips, & Meeks, 2019; Gyasi et al., 2019; Nkansah et al., 2021).
The review suggests that there is a dearth of literature on society’ attitude toward older adults in Ghana, and older adults’ expectations for social inclusion and dignified aging. The limited literature indicates that older adults have unmet care and support needs, and are therefore socially excluded. The current study therefore fills an important knowledge gap.
Theoretical Framework
A human rights lens (Cox, 2015; Harbison, 2022) and social exclusion theory (Levitas et al., 2007; Walsh et al., 2021) in combination with critical gerontology perspectives (Estes & Grossman, 2007; Holstein & Minkler, 2007; Moody, 1993; van Dyk, 2014) provide a framework for this study to explore society’s attitude toward older adults and the support they require for dignified aging. Critical gerontology is grounded in the traditions of critical theory (Moody, 1993). The thrust of critical gerontology is the “emancipation of older people from all forms of domination … identifying possibilities for emancipatory social change, including positive ideals for the last stage of life” (Moody, 1993, p. xv). Critical gerontology goes beyond the biomedical and psychoanalytic views of older adults and analyzes how social forces shape older adults’ experiences so as to advocate for change in social policy and practice (Donnelly & Torres, 2022; Estes & Grossman, 2007). According to Grenier and Sussman (2022), the critical gerontology lens highlights how macro structural processes of society construct older adults as dependent, and economically and socially impoverishes them through age-based stereotyping, stigmatizing, and exclusion. Critical gerontology thus challenges what is versus what ought to be for the well-being of older adults. For this study, the critical gerontology lens will help to explore society’s attitudes toward older adults and the types of support required for dignified aging.
The human rights framework (Cox, 2015; Harbison, 2022) and social exclusion theory (Levitas et al., 2007; Walsh et al., 2021) augment critical gerontology perspectives as a framework for the study. Human rights principles call for protection, security, and support for all persons, especially vulnerable older adults, to ensure their dignity and social, economic, political, and cultural inclusion (Cox, 2015; Harbison, 2022; HelpAge International, 2008). Social policy and practices that are informed by a human rights framework would guarantee that “everyone, regardless of where they live or who they are…” (Cox, 2015, p. 6) is socially included and has their needs met. This is where social exclusion theory enters into the discussion. Social exclusion theory helps to understand how, when, and where people are socially excluded or included, with their needs met or not met. Social exclusion points to situations of constricted and contraction in networks of support, depletion in resources and opportunities for resource generation, and a lack of access to services in which “states, societies, communities and individuals” are implicated (Walsh et al., 2021, p. 12). More broadly, Walsh et al. define social exclusion in older age as involving “…interchanges between multilevel risk factors, processes and outcomes … its complexity, impact and prevalence are amplified by old-age vulnerabilities … constrained opportunities … inequities in choice … services … and civic participation…” (2021, pp. 11–12). Levitas et al. (2007, p. 9) also describe social exclusion as demonstrating a “lack or denial of resources … and the inability to participate in the normal relationships and activities, available to the majority of people in a society…,” with income poverty, health problems, and discrimination or stigma as associated factors (Gee & Walsemann, 2009; Levitas et al., 2007). Social exclusion has several dimensions. These include economic exclusion, which is characterized by a lack of employment, income poverty, and material deprivation (Van Regenmortel et al., 2016), institutional exclusion – barriers to or a lack of access to services (Scharf et al., 2005; Scharf & Bartlam, 2008), exclusion from social relations (Burholt & Aartsen, 2021), and exclusion from political or civic activities, which is marked by a lack of opportunity to participate in civic activities and political decision making (Kneale, 2012; Scharf et al., 2005; Scharf & Bartlam, 2008). Burholt and Aartsen (2021) have elaborated on the social relations dimension of exclusion, defining this type of exclusion as “a situation in which people are disconnected from adequate levels and quality of intimate relationships, social networks, social support, and/or social opportunities to participate in the wider society” (p. 78).
Methodology
Design
This study used a qualitative description approach (Ayton, 2023; Doyle et al., 2020; Sandelowski, 2000, 2010) to study society’s attitude toward older adults, and older adults’ perceptions and expectations of support for social inclusion and dignified aging. This approach focuses on describing the “who, what, where and how,” rather than explaining (Ayton, 2023, p. 49; Sandelowski, 2000, 2010), and is a pragmatic approach for describing “experiences from a subjective perspective” (Doyle et al., 2020, p. 445; Kim et al., 2017). Qualitative description research aligns with constructionism, critical theories, and a stance of multiple views of reality (Kim et al., 2017; Sandelowski, 2000, 2010). The approach is adopted for this study as it aligns with the researcher’s ontological position that reality is shaped by the beliefs, conventions, experiences, and practices of the social context. The approach is also suitable for this study because it allows for flexibility in sampling of participants and data collection and analysis strategies. For example, this approach allows for purposive sampling, semi-structured face-to-face individual interviews, and thematic and qualitative content analysis (Ayton, 2023; Doyle et al., 2020; Kim et al., 2017; Sandelowski, 2000, 2010).
Methods
Participants
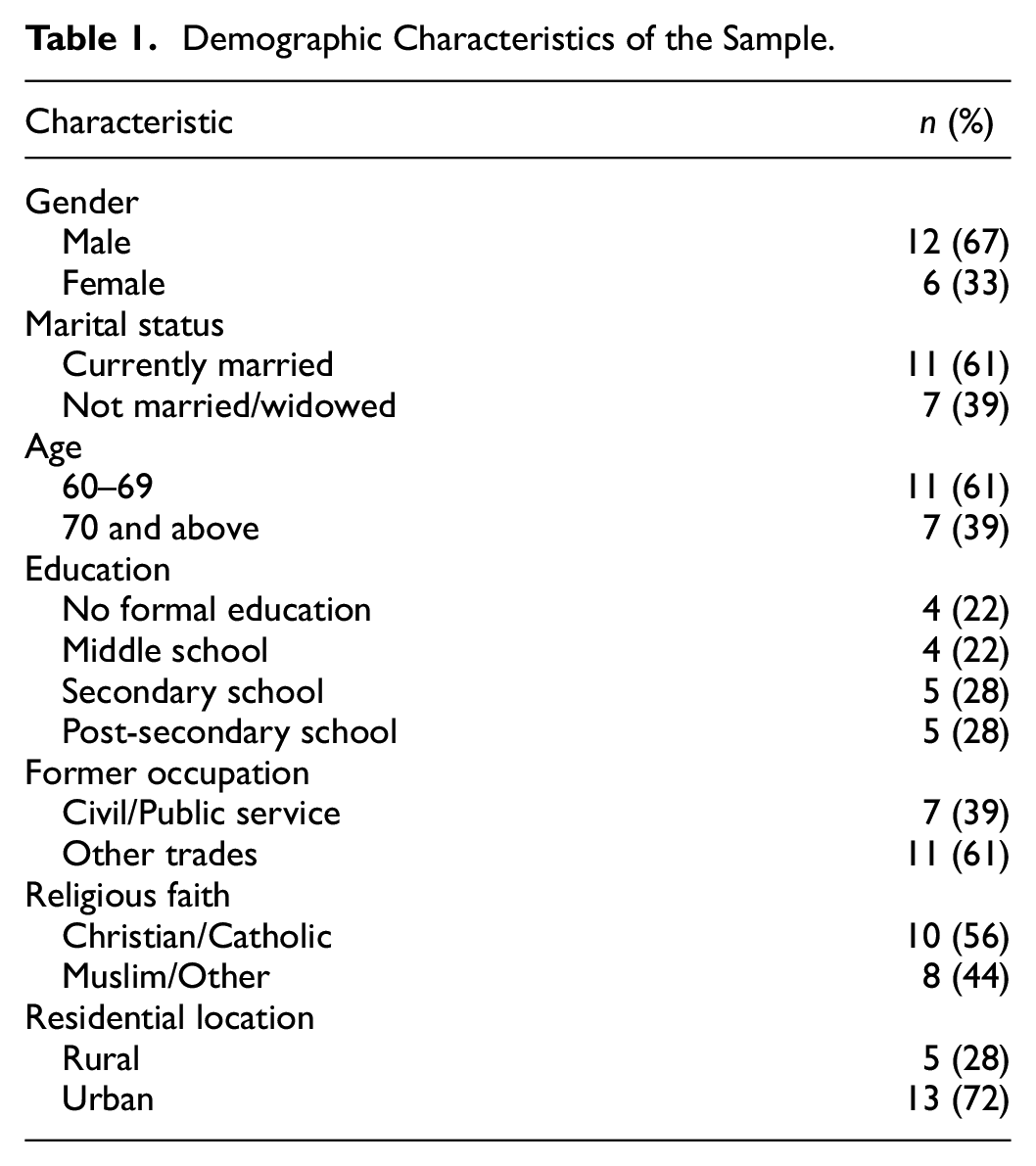
Participation in the study was open to persons aged 60 years and older in the Northern Region, Ghana, who were healthy enough to engage in an interview. For practical and pragmatic reasons, such as time and monetary constraints, a sample of 18 participants recruited from the Tamale Metropolitan Assembly was used for the analysis. Qualitative exploratory studies are usually judged by the richness of data provided by each participant, not necessarily by sample size (Ayton, 2023; Boddy, 2016; Braun & Clarke, 2022; Doyle et al., 2020; Kim et al., 2017; Robinson, 2014; Sandelowski, 2010). For this study, data provided by 18 participants were judged to be sufficient to address the research question. Outreach to common community spaces, together with snowball techniques, was used to solicit participation. Through these purposive sampling strategies, the sample captured important characteristics of older adults in the study area. Table 1 presents participants’ characteristics.
Demographic Characteristics of the Sample.
Data Collection
The dataset for this study was part of data obtained between May and July 2018, a period predating the outbreak of the corona virus disease, 2019 (COVID-19) pandemic. Flexible interviews were conducted with participants in mutually determined convenient spaces to gather data. The three focal questions that allowed for a dialog with participants were: (1.) In general, how will you describe society’s attitude toward people of your age cohorts who are regarded as older adults? Prompt: By society, you can talk about governmental and non-governmental agencies and policies as well as families and communities. (2.) In general, what types of support do you expect from the formal systems of the Ghanaian society for older adults like you? Prompt: You can describe the types of support you expect from government and other agencies for older adults. (3.) In general, what types of support do you expect from the informal systems of Ghanaian society for older adults like you? Prompt: You can talk about the types of support you expect from families, friendships, religious groups, and community groups for older adults. Fourteen participants were interviewed in English, while four participants were interviewed in Dagbani (widely spoken in the study area). The researcher was fluent in the languages used for the interviews, so did not encounter any communication difficulties with participants during the fieldwork. Many of the interviews were conducted in participants’ homes, while others were held at locations that qualified as participants’ workplaces. The interviews lasted between 50 min and 1 hr, and each interview was audio-recorded. The English interviews were transcribed verbatim, while the Dagbani interviews were transcribed with the help of an expert in Dagbani literacy.
Data Analysis
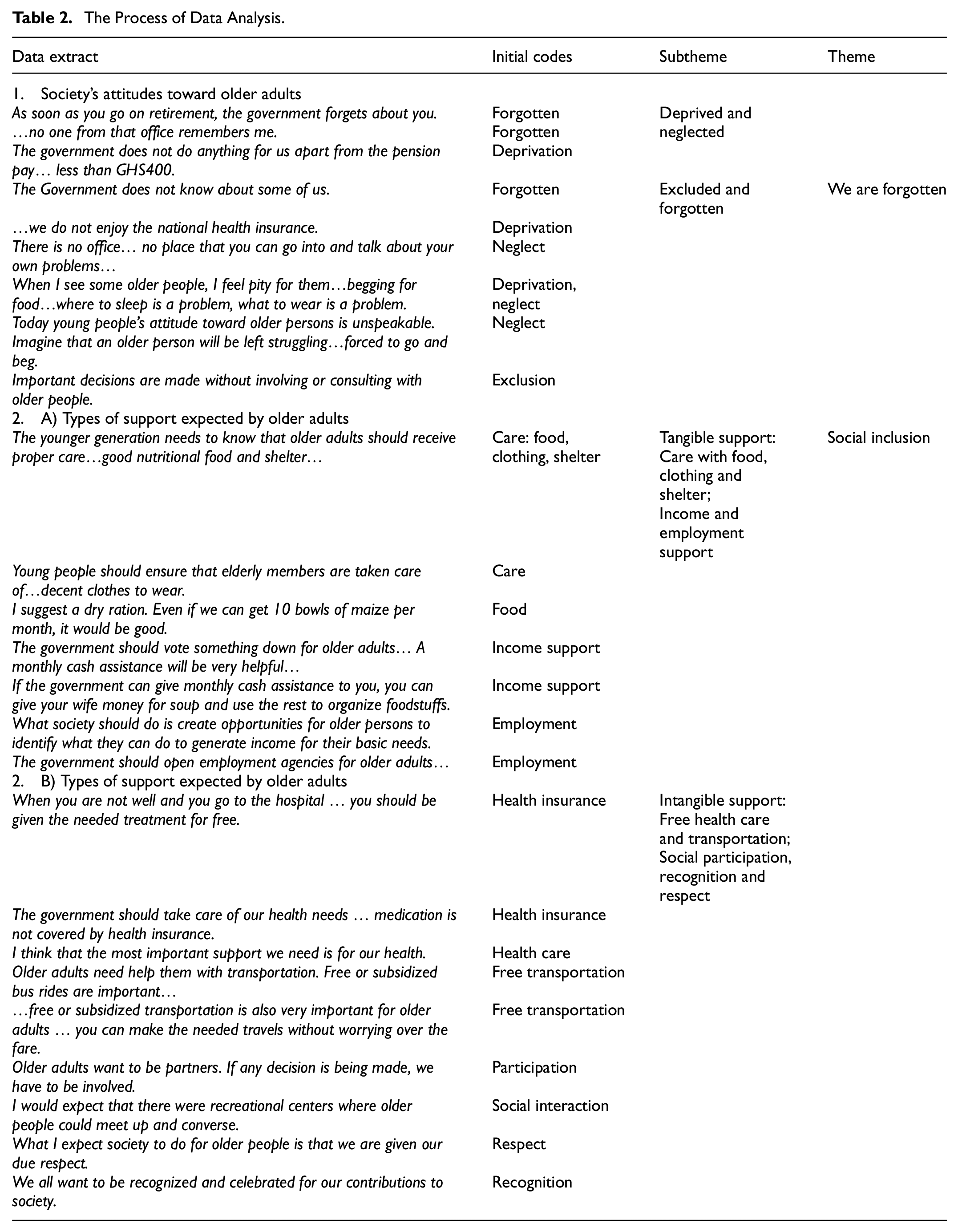
The transcribed data were imported into NVivo software (version 12), and the thematic analysis framework (Braun & Clarke, 2006, 2019, 2022) guided analysis of the data. Thematic analysis is a flexible and reflexive approach to qualitative data analysis which enables a deeper comprehension and reduction of data into main themes and subthemes for interpretation and conclusion drawing (Braun & Clarke, 2006, 2022). Using thematic analysis, the researcher followed some six steps to render the data comprehendible. These included: first, familiarize with the data; second, generate initial codes; third, search for potential themes; fourth, review potential themes; fifth, define and name themes; and sixth, report the findings (Braun & Clarke, 2006; Naeem et al., 2023). To familiarize with the data, the researcher dived into the contents of the transcripts, which enabled discernment of important responses by participants. Keywords and quotes that captured these important experiences, perceptions, or views of participants were noted through this familiarization process. Initial codes were then generated, with the keywords and selected quotes forming the basis. Codes are short phrases or words that are assigned to portions of data that represent significant patterns of meaning or preliminary themes (Braun & Clarke, 2006, 2019, 2022; Naeem et al., 2023). The researcher then focused on searching for themes, or theme development. This involved sorting through and collating or combining codes to establish meaning categories or patterns – themes and subthemes. The next phase of the analysis involved a review and refinement of the tentative themes in relation to the research purpose and questions, to ensure that all coded data were captured in the themes, and that the themes largely represented the data accurately. Finally, the main themes were named, along with subthemes, and reported as findings of the study. Table 2 presents the process of data analysis. It shows how the data were coded, which led to the naming of the themes.
The Process of Data Analysis.
Ethical Considerations
This study met all the requirements for the ethical conduct of research involving human participants and reporting findings. The Interdisciplinary Committee on Ethics in Human Research (ICEHR) of the author’s home institution provided ethics clearance for this study (approval # to be provide). Participation in this study was voluntary. All participants were taken through a consent process to know their rights and obligations in the study, following which they gave consent either by signing or thump-printing the consent form. Culturally mandated protocols of respect for older adults, including how to approach, greet, and introduce a topic, were followed, and each participant was given CAD10 (or GHS35) as a token of appreciation. A draft of this paper was presented at a virtual International Conference and feedback was received from an academic audience.
Findings
We Are Forgotten
There was a strong negative evaluation of society’s attitudes toward older adults, which pointed to a sense of older adults being forgotten. Subthemes that communicated this theme were deprived and neglected and excluded and forgotten. Many participants described experiences that made them feel neglected and forgotten by the formal and informal systems. For many, there was frustration over the kind of treatment they expected and how they were actually treated, which resulted in some older adults living in pity. It was clear that the government is not doing enough for older adults, whether they had worked in the formal sector (civil/public service) or in the informal sector (other trades). For example, the following quotes show how those who have worked in the formal sector felt the government has neglected or forgotten them after their retirement: As soon as you go on retirement, the government forgets about you; you see, the government forgets about you, in terms of your income and other needs. (Male, 65 years old). I worked in the market, doing sales work, for 10 years. I then came to the regional administration and worked for 22 years as a janitor. And when I retired from the regional office, they did not give me anything as a sendoff, and no one from that office remembers me. (Female, 72 years old). The government does not do anything for us apart from the pension pay. And the pension pay is, do you know how much I am receiving at the end of the month? It is less than GHS400. (Female, 74 years old)
Some participants’ experiences suggested that the government does not know about many people like them, either because government services are not targeted to them or because those services do not reach them. According to one participant: Government does not know about some of us. If the government knew about me, I could go to them and say that I need help. Even if they could give me a few hours of work to earn some income that would help. But government does not seem to know about me. (Female, 71 years old).
Indeed, the fact that older adults between 60 and 69 years do not enjoy any cost exemptions on the NHIS was interpreted to mean that those within this age group are forgotten by the policy. For example: There is the national health insurance, where the government should have taken care of all the elderly by giving them preferential treatment [cost exemptions]. However, we do not enjoy the national health insurance. (Male, 65 years old).
To not feel forgotten, some participants expected that there would be places designated for them, where they would go and express themselves freely, discuss their challenges, and seek solutions. On the contrary, as one participant put it: You do not even know where to go. There is no office, there is no place that you can go into and talk about your own problems and that kind of thing. There is no specialized area created, even in the hospital, to say that when older people come in this is where they have to receive treatment. These things are not present. (Male, 69 years old).
Some palpable signs that participants gave to indicate that older adults were neglected and forgotten by their offspring included being wretched and pitiable, such as not having food to eat, a place to sleep, or clothes to wear, as illustrated in the following: When I see some older people, I feel pity for them. They go about searching and begging for food to eat, and even where to sleep is a problem, what to wear is a problem. Even in their own family homes, they thrive on meagre resources and this is very bad. (Male, 63 years old). Today young people’s attitude toward older persons is unspeakable. Somebody has many of these young people but they are of no use. There are cases where someone has up to six children and somebody without a child is better off. Imagine that an older person will be left struggling to the point where he calls his children to ask them to give him money to buy food. Then the parent is forced to go and beg and you complain that your father is going round begging. (Male, 78 years).
Not being consulted when important decisions are being made, whether or not these decisions affect older adults directly, was another way in which participants felt excluded and forgotten. Some participants blamed this on the arrogance of young people who think that, with their university degrees, they know it all, or know better than older adults. One participant put it as follows: I think society should reflect and know that older adults have something to bring to the table. Important decisions are made without involving or consulting with older people. Young people and the leaders feel big that they have obtained university degrees; they are graduates, and are holding their PhDs. So, you an illiterate old man or old lady, what do you know about this modern world? But is it not said that old age is wisdom? (Female, 70 years old).
Social Inclusion
Social inclusion was the other theme named from the data. This theme captures the types of support and services that participants required to change their situation from exclusion to inclusion and integration. The two subthemes of social inclusion are tangible types of support and intangible types of support.
Tangible Types of Support
Care in the form of support with food, clothing, and shelter (i.e., where to sleep) was an important type of tangible support discussed in the data. Participants identified good nutritional food, a place to sleep (or housing), and adequate clothing as essential for a life of dignity in older-age, and there was a general sense that many older adults require assistance to have these on a sustained basis. This form of support was expected primarily from the informal support system of family, friends, and neighbors, perhaps because participants did not know of any publicly funded housing services or food and clothing assistance programs. Children or offspring, commonly referred to as “the younger generation,” and extended family members were identified as the expected sources of this type of support. Two participants are quoted to illustrate the point as follows: The younger generation needs to know that older adults should receive proper care. They should be able to provide good nutritional food and shelter for their older parents to make them have a sense of dignity. I know a few older people; when I look at them, I do not feel happy. (Male, 61 years). Within the extended family, young people should ensure that elderly members are taken care of. For example, give these people appropriate and decent clothes to wear. Even your old clothes that you no longer need, give him. It will be helpful. (Male, 78 years old).
However, one participant expected that the government and/or other organizations should also support older adults with food supplies, emphasizing that food insecurity is a huge issue for many older adults, especially during the lean (or off-farming) season. The participant put it as follows: I suggest a dry ration. Even if we can get 10 bowls of maize per month, it would be good. Some of these Christian organizations do this from time to time. For example, the Adventist Development and Relief Agency used to provide food rations to older people. But I do not know if they are still around. (Male, 63 years old).
An important component of tangible types of support was the idea of a guaranteed monthly income for older adults. There was a general expectation that the government would provide a monthly cash assistance to older adults. The general view was that, with the political will, the government could take a census of older adults in the system and make a budgetary allocation so that everyone would be accounted for. Some of the participants were aware of the LEAP program but advocated for something different because they had reservations about the LEAP program. According to one participant: The government should vote something down [make a budgetary allocation] for older adults. The government should take count of the number of older men and women in the system, and provide them with income support. A monthly cash assistance will be very helpful for older people in Ghana. The current LEAP program is not sufficient, and is even politicized. It does not work. (Male, 63 years old).
There was the sense that a guaranteed monthly income support would give older adults peace of mind and prolong their lives, as they could afford foodstuffs and healthcare services. The following quotes illustrate the point: They should support older people like me with a regular income. Financial support is required to help us pay for health care services and many other things. (Female, 74 years old). If the government can give monthly cash assistance to you, you can give your wife money for soup and use the rest to organize foodstuffs. This would be helpful. If there is peace of mind for an older person, you see that they can live much longer. (Male, 68 years old).
However, one participant cautioned that some older adults may not enjoy the full benefits of a cash assistance, explaining that: Sometimes, if you give money to older adults, their family relations can borrow the money and not pay back. If they do not pay back, what can you do? (Male, 63 years old).
Employment opportunities whereby older adults were able to do part-time work or be self-employed was another type of tangible support in the data. Participants explained that some older adults were still capable of applying their skills to earn some income, and an opportunity to work would make them socially included and augment whatever would come from a guaranteed income program. It was clear that participants expected support for part-time or self-employment to come from governmental and nongovernmental sources. Examples of what participants could do to earn income included being employed at daycare centers for children, garbage removal for the city council, animal rearing, and weaving. Two participants are quoted to illustrate the point as follows: What society should do is create opportunities for older persons to identify what they can do to generate income for their basic needs. This is the appropriate thing to do. There are some older persons who can engage in some ventures to generate income, such as animal rearing or weaving, if they get support. (Male, 75 years old). The government should open employment agencies for older adults. This will encourage us to keep fit and give us money to sustain ourselves. For example, government could establish daycare centers for children, and employ older women as caregivers. This is something we can do well. In addition, some of us are still strong enough, and could be engaged by the city council to oversee the cleanliness of the city. (Female, 71 years old).
Intangible Types of Support
Intangible types of support is the second subtheme of social inclusion. Whereas tangible support provides material care as well as income and income-generating opportunities to older adults, intangible support provides them access to services without costs. One form of intangible support identified in the data is free health care and transportation services. Free healthcare was a highly expected social inclusion support among participants, and they expected that the government would provide them with this support. It was apparent in the data that participants wanted full coverage on the health insurance scheme, including free enrollment and cost absorption so that they would not have to pay for medical treatment, prescription medication, and laboratory examination. Illustrations of this point include the following: The government should give older adults a concession somewhere, such as in healthcare. I mean, when you are not well and you go to the hospital, you should not be asked to pay anything. You should be given the needed treatment for free. (Male, 62 years old). The government should take care of our health needs. For our national health insurance, we pay GHS5 for the annual renewal. However, sometimes you go to the hospitals and they tell you that this medication is not covered by health insurance. What do you expect the older person to do? Do you mean he should die before his time? (Male, 72 years old). We older people. I think that the most important support we need is for our health. When you are sick and you do not have money to go to the hospital, you need something that can take you there. If you are going to the hospital, you need money and yet you do not have it. So, we need support with healthcare; if you go to the hospital, either you are treated for free or the cost is subsidized for you. (Female, 61 years old).
Participants also expected that there would be a public transit system that provided them with free or subsidized bus rides. They emphasized that free or subsidized bus rides would enable them to make necessary long or short-distance travels across the country to maintain ties with loved ones without worrying over transport fares. The following illustrates the point: Older adults need help them with transportation. Free or subsidized bus rides are important, especially if you are going on a long journey, like from here in Tamale to Accra or Kumasi, to visit family or friends. The fares are high and always increasing. (Male, 72 years old). As I have said before, free or subsidized transportation is also very important for older adults. If this is provided, you can make the needed travels without worrying over the fare. (Male, 61 years old).
Social participation, recognition, and respect is another form of intangible support that illustrated the theme of social inclusion. There was a high expectation of opportunities for social participation where participants wanted to be involved in decision-making and to participate in interactional and recreational activities. For example, there was the expectation that government/public officials would periodically interact with older adults and hold discussions that would shape social policy. This form of engagement would not only tap into the wisdom of older adults, it would make them feel recognized and valued. The following is an illustration: Older adults want to be partners. If any decision is being made, we have to be involved. We also want the authorities and public officials to visit us in the community. Once in a while, they should come and we sit down and chat with them. The government should create venues in the districts where these meetings can take place. If this is done, you know, older people would have a sense of belonging. It will show that somebody has them at heart, that you are concerned about their well-being. (Female, 70 years old).
In addition, participants expected to have social or recreational centers in their communities, where older adults could go for socialization activities, with a hot lunch on the side. These socialization activities would not only give a structure and routine to older adults, it would also relieve them of isolation and loneliness. The following is an example of how this point was captured in the data: I would expect that there were recreational centers where older people could meet up and converse. They would interact, talk, and then get a good meal to eat in the afternoon. Then, when it is about four o’clock pm, you start going to your house, wherever you are coming from. You would be happy that you are able to air out your feelings in the company of your peers. But if you sit at home all day long nursing a problem alone, you are not able to get it off your head. Therefore, if the government would help in this area, recreational centers should be created. (Female, 63 years old).
There was also an expectation that family members and other people in their informal networks would engage in more frequent interactions with older adults. The point was made that even something as basic as a greeting or a visit to check on the older adult was important in making them feel socially included. The following are examples of the point: You do not have to give anything when you visit the older person. But if, say, in the morning, you go and say “good morning mother or grandma.”“Oh, mother, did you sleep well? Grandma, are you okay?” This is something significant. (Female, 72 years old). In truth, what we would want you to support us with is, “good evening, good morning.” So, if you do not have that support within your reach, it is worrisome. (Male, 80 years old).
Further to the above, participants expected that social events would be organized in their communities where they would be honored, and they expected this from formal and informal sources. The point that older adults needed respect and that occasions that celebrate older adults give them a sense that they matter was highlighted in the data, as illustrated in the following: What I expect society to do for older people is that we are given our due respect? As an older person, if you give me respect, you have given me everything. (Male, 60 years old). Currently, there is the annual senior citizens’ day celebration. However, the invitation to the event is limited to a select few. We all want to be recognized and celebrated for our contributions to society. (Female, 72 years old). I expect the government to see me as, to recognize me as somebody who has contributed to the growth of the country in my own small way. Therefore, all I need is recognition from the government. (Male, 62 years old).
Discussion
This study extends existing literature on the balance of tangible and intangible support and services that older adults require for their social inclusion and dignified aging (Bacsu et al., 2014; Bai, 2019; Flett & Heisel, 2020; Litwin & Attias-Donfut, 2009; Naaldenberg et al., 2011; Naganathan et al., 2016; Nelson & Rosenberg, 2022; Rapolienė & Gedvilaitė- Kordušienė, 2022; Wee et al., 2015). The study makes a contribution to current literature in the context of Ghana from the lenses of critical gerontology (Estes & Grossman, 2007; Holstein & Minkler, 2007; Moody, 1993), social exclusion theory (Levitas et al., 2007; Walsh et al., 2021), and human rights (Cox, 2015; Harbison, 2022). Although Ghana has made some policy efforts at ensuring the well-being of older adults (Ministry of Gender, Children and Social Protection, 2010, 2018), findings of this study suggest that many older Ghanaians are forgotten, socially excluded, and falling through cracks in the social safety net. Being forgotten means that older adults experience deprivation and neglect by both the formal and informal systems of support for their wellbeing. As the theory holds, social exclusion robs people of social, economic, political, and cultural resources necessary for well-being and fulfillment (Burholt & Aartsen, 2021; Gee & Walsemann, 2009; Levitas et al., 2007; Ogg & Myck, 2021; Walsh et al., 2021).
The social exclusion of older Ghanaians manifests in various ways. In a significant way, they are excluded from opportunities to earn or receive income that is adequate for a decent livelihood. While many of them do not have retirement pensions (Alhassan Issahaku & Neysmith, 2013), the few who have pensions receive a monthly stipend that is woefully inadequate. Older adults’ income deprivation is linked to their exclusion from essential services such as health care. As is demonstrated in this study, older Ghanaians face significant barriers to accessing health care services, in part due to income poverty (Ghana Statistical Service, 2019, 2022), but also due to ageism and an inequitable distribution of health care resources across geographic regions of the country (Issahaku & Sulemana, 2021). The prevailing health insurance scheme provides premium exemption for adults aged 70 years and older, which means that those who are between 60 and 69 years old are excluded. Moreover, because the NHIS does not cover prescription medication and laboratory examinations, it excludes many older people from accessing health care because they cannot afford the costs (Gyasi, 2018; Issahaku & Sulemana, 2021; Kuuire et al., 2017). Consistent with previous research in West Africa (Parmar et al., 2014), the findings indicate that older adults who are susceptible to social exclusion are less likely to be covered by health insurance schemes and to access health care services.
The informal system of communities and families is also implicated in the exclusion of older Ghanaians, as they fail to ensure that older adults’ basic needs of food, clothing, and shelter are met. Recent research has highlighted the neglect of older adults by families and communities in Ghana as a growing phenomenon (Braimah & Rosenberg, 2021; Nkansah et al., 2021). An earlier work by Aboderin (2004b) had pointed to a steady decline in care for older adults by kin and offspring in the country. Coe (2017) has made a telling statement on the neglect or abandonment of older adults by their children. According to Coe, in contemporary Ghana, because the system of filial obligation that mandated children to support their older parents has lost its “persuasive power,” older adults “can be abandoned and neglected” (2017, p. 150).
Consistent with the dictates of critical gerontology which calls for a redress of injustice, deprivation, and discrimination meted out to older adults at all levels of society (Estes & Grossman, 2007; Holstein & Minkler, 2007; Moody, 1993), findings of this study call for social inclusion practices. Social inclusion is characterized by meaningful social roles, social participation, healthy interpersonal relationships, and a sense of belonging, acceptance, and opportunity (Abbott & McConkey, 2006; Cobigo et al., 2012; McCausland et al., 2021; Overmars-Marx et al., 2014; Simplican et al., 2015). Inclusion is known to promote improved quality of life in the general population and among older adults (McCausland et al., 2021; van Asselt-Goverts et al., 2015). For their social inclusion, older adults require tangible and intangible forms of support that enable them achieve adequacy with their basic needs, and social participation. An important form of support older adults need is care, where they are provided with adequate food, clothing, and housing. Older adults’ vulnerability to deprivation of these forms of care is highlighted in the literature on late-life poverty (Ghana Statistical Service, 2019, 2022; Mudrazija & Butrica, 2023; Weiss-Dagan & Timor-Shlevin, 2024), food insecurity (Kandapan et al., 2023; Kansanga et al., 2024; Selvamani & Arokiasamy, 2022; Ziliak & Gundersen, 2021), and homelessness (Grenier, 2021; Grenier et al., 2016, 2017; Grenier & Sussman, 2022). The literature suggests that an increasing number of older adults are poor, food insecure, and homeless, which the findings of this study support. Given that income poverty is fundamental to these experiences among older adults, a steady flow of income through a combination of cash transfers and part-time employment (Bai, 2019; Datta et al., 2023; Dwyer et al., 2023) are identified as tangible support that would uplift older Ghanaians. This point has been noted by HelpAge International (2008), which emphasizes that “Older adults in Africa need a basic income generated either through employment or through social cash transfers such as social … pensions, disability grants or child care grants” (p. 2).
Intangible support is also required for the social inclusion of older Ghanaians. An important way of ensuring older adults’ social inclusion and promoting dignified aging without putting anything tangible in their hands is by guaranteeing them access to health care services where costs (of treatment, laboratory examination, or prescription medication) are not a structural barrier, and by supporting them with mobility. Existing research shows that, of all barriers to accessing health care services among older adults, cost is topmost (Dake & van der Wielen, 2020; Gyasi, 2018; Kuuire et al., 2017; Morgan et al., 2022; Parmar et al., 2014). Therefore, insurance programs which, without discrimination, absorb the costs of health care for older adults, and a public transit service that gives them free bus rides, are crucial for their access to health care services, and their social inclusion. Intangible support for the social inclusion of older adults would also come in the form of social and civic participation (Cobigo et al., 2012; McCausland et al., 2021; Overmars-Marx et al., 2014; Simplican et al., 2015), where older adults participate in decision making, perform meaningful social roles, and have opportunities for social interactions through which they are recognized, respected, and celebrated. Periodic interactions with public officials and community leaders, either in policy forums or on celebratory occasions, and recreational resources that enable peer-to-peer interactions are some of the ways in which this type of support could be extended to older adults. Social/civic participation not only enhances the emotional well-being of older adults by alleviating isolation and loneliness (Braimah & Rosenberg, 2021; Flett & Heisel, 2020; Gyasi, Phillips, & Abass, 2019), it upholds their human rights and dignity (Chi, 2014; Harbison, 2022).
Study Limitations
An important critique of this study is the overrepresentation of male participants (67%) and urban residents (72%) in the sample. Sample composition matters for the diversity of experience and perspective among participants. The data are also limited by issues of bias since purposive sampling is driven by researcher judgment and a predetermined set of criteria (Denieffe, 2020). Some readers may also have concerns about the size of the sample; however, 18 is a reasonable sample, and sample size is not as much a concern in qualitative research as there is need for a sample that reflects important characteristics of the population of interest and provides rich data (Boddy, 2016; Robinson, 2014). Perhaps the context of the interviews also introduced limitations into the data. While over 50% of participants were interviewed in their homes and in English, some of the interviews were conducted in a local language and while the participant was weaving or attending to a family shop. It is possible that some of these participants had divided attention which interfered with the flow of their thoughts and responses to the interview. In addition, although the researcher was fluent in the local language used in the interviews, it is possible that some meaning was lost in the process of cross translation from the local language to English. Therefore, readers are advised to interpret and apply these findings with caution.
Conclusion and Implications
In some significant ways, older Ghanaians are socially excluded and forgotten. They experience income poverty, care deprivation or neglect, and lack access to health care services, transportation, and social/civic participation. To enhance the social inclusion and dignified aging of older Ghanaians, tangible and intangible types of support and services are needed from formal and informal sources of the society.
An important policy implication of this study is the need for a cash transfer program that gives older adults a guaranteed monthly income. A cash transfer program targeted to all older adults who have no reliable source of income and who fall below a certain income threshold is required. Existing research shows that a well implemented cash transfer program is effective in alleviating poverty (Datta et al., 2023; Dwyer et al., 2023; Gachigi, 2023). The current LEAP program which is not specifically targeted to older adults and does not reach the majority of those in need does not satisfy the policy recommendation being made here. Another policy implication of the study is the need to create opportunities for part-time or self-employment for older Ghanaians. For those who are still capable yet are reduced to idleness and loneliness due to retirement or other reasons, an opportunity to work would keep them active and engaged while earning some income, and would go a long way in promoting their self-worth and dignity. An additionally important policy suggestion is the need for a health insurance scheme that not only provides free enrollment to older adults but also covers the costs of treatment, laboratory examination, and essential medications. Since these costs constitute a significant barrier to accessing health care services for older adults, a scheme that absorbs them would significantly enhance healthy and dignified aging. The current NHIS, which exempts only those aged 70 years and above from premium payments and does not absorb the catastrophic costs of health care, not only discriminates against older adults between ages 60 and 69 years, it also makes health care inaccessible for many older adults. A final policy implication that is worth noting is the need for social centers, where older adults could go for recreation and socialization. An opportunity for older adults to engage in peer-to-peer interactions and participate in political decisions and community celebrations would be significant in making them feel social inclusion and experience recognition and respect. A research implication of the study is in relation to the proposed cash transfer program. There is a need for a survey to determine a base amount for the transfer and an income cutoff point for eligibility. There is also a need for qualitative analyses on how best to implement the program without undue political interference.
Footnotes
Ethical Considerations
The Interdisciplinary Committee on Ethics in Human Research (ICEHR) of the Memorial University of Newfoundland provided ethics clearance for this study (ICEHR # 20171397-SW).
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data supporting this study are available upon reasonable request to the author.