
Abstract
This study, drawing on a resource—based view and information processing theory as a foundation, aims to examine the influence of total quality management on corporate sustainability directly and through the mediating role of business process integration, knowledge sharing, and the moderating role of innovative culture. Data was collected from 286 managers and supervisors of selected private hospitals in Ethiopia using a structured questionnaire and convenience sampling. Data analysis is conducted using SmartPLS4. The result of this study demonstrate that total quality management significantly influences corporate sustainability, both directly and through the mediating role of knowledge sharing and business process integration. Moreover, this study found that innovative culture has a moderating role in the relationship between total quality management and corporate sustainability. However, innovative culture is not moderating the relationship between knowledge sharing and corporate sustainability. This study focuses only on private hospitals in Ethiopia and data is collected from managers and supervisors using convenience sampling technique. Therefore, the findings cannot be generalized and may not be extended to public hospitals. Further research should test the model in different socio-economic and cultural settings, as well as in public hospitals. The findings of this research have practical implications for managers and policymakers in the private healthcare sector during decision-making and strategic planning.
Plain language summary
Previously, little research examined the role of TQM and CS in emerging economies’ healthcare sectors, particularly Ethiopia. This study uses the resource-based view (RBV) and information processing theory to examine TQM and CS. The study also looks at how business process integration (BPI) and knowledge sharing (KS) affect the relationship between KS and CS and how innovative culture (IC) affects the relationship between TQM and CS in a few private hospitals in Ethiopia. We used convenience sampling to acquire data from 110 Ethiopian private hospital managers and supervisors. We examined the data with SPSS 23 and Smart-Pls 4. This study shows that TQM improves CS significantly. This study also demonstrated that KS and BPI mediate TQM-CS. IC moderates the link between TQM and CS in private hospitals, according to this study. In contrast, IC does not appreciably moderate the KS-CS relationship. This work advances resource-based theory, information processing theory, healthcare TQM, and CS literature. The study sheds light on implementing TQM in healthcare in emerging economies. These findings also improve the quality management and healthcare literature.
Keywords
Introduction
Now a days, the healthcare industry is facing challenges due to degradation of biodiversity, resource inconsistency, political instability, and an uncertain and dynamic environment (Aburayya et al., 2019; Obeng et al., 2024). Moreover, the healthcare industry faces numerous challenges in service delivery, patient satisfaction, sustainability issues and resource utilization (Nguyen & Nagase, 2019). Furthermore, opportunities and threats are constantly changing as a consequence of environmental turbulence, and patients` preferences also change. Based on, the United Nations Sustainable Development Goals (UNSDGs) the present study focuses on Sustainable Development Goal 3 (SDG 3), which is related to good health and wellbeing and SDG10, related to reduce the inequalities (Pakkan et al., 2023). Moreover, this study aimed at addressing the problem mentioned above by incorporating total quality management (TQM) and corporate sustainability (CS).
Furthermore, previous research on TQM and CS has predominantly focused on one particular aspect of sustainable performance, specifically the economic dimension or financial performance (Ali AlShehail et al., 2022; Mukenga & Awolusi, 2023; Olayiwola et al., 2024). Conversely, regarding the social aspect of sustainability, limited research has explored the correlation between TQM and stakeholder benefits (Abbas, 2020). In terms of environmental performance, some empirical studies have found TQM’s contribution to environmental sustainability, such as green innovation (Jum’a et al.’, 2024). However, only a limited number of research has investigated the association between TQM and various aspects of sustainability performance, including environmental, social, and economic sustainability (Hudnurkar et al., 2023; Nazarian et al., 2024), indicating the need for further study.
There were also studies by Abd Alhasan et al. (2022), Jum’a et al. (2023), and Jum’a et al. (2024) that looked into the relationship between TQM and CS. The studies used operational performance in the textile industry, quality culture in small and medium-sized businesses, and environmental management practices in the manufacturing industry as moderating variables, respectively. Other research by Abbas (2020), Albloushi et al. (2023), and Ali AlShehail et al. (2022) also looked at the link between TQM and CS. These studies used different mediating variables to help explain the relationship, such as knowledge management, green innovation in the manufacturing industry, and service innovation in the public service sector, respectively. While there is some research on TQM and CS in the healthcare industry, there are still no empirical studies investigating the moderating role of IC in the relationship and mediating mechanism of BPI and KS. This study aims to address this knowledge gap
Moreover, despite the gradual increasing attention in the field of TQM and CS research, there remains a dearth of studies that explore the role of KS, BPI, and IC in the association between TQM and CS. Furthermore, there are studies on TQM in healthcare industry with various variables, but there is a scarcity of robust empirical research examining the impact of TQM on the promotion of CS within distinct organizational contexts (Albloushi et al., 2023). Prior scholars such as Acquah et al. (2023), Ali AlShehail et al. (2022) and Abbas (2020), suggested future studies to investigate the relationship between TQM and CS in the service industry as opposed to manufacturing. Furthermore, Albloushi et al. (2023) and Fok et al. (2023) also proposed further research in this relationship, specifically in the healthcare industry in emerging economies. Thus, this study aims to address the call for further research from previous scholars and bridge the gap.
Furthermore, Lee and Lee (2022) revealed that TQM can enhance environmental sustainability through the reduction of pollution and resource utilization in the healthcare industry. TQM can also enhance the economic sustainability of the healthcare sector by promoting efficiency and productivity, while also reducing costs, medical errors, and risks (Khalil & Muneenam, 2021). Maintaining the social sustainability of the healthcare industry is also heavily reliant on prioritizing the well-being of patients and communities (Zehir & Zehir, 2023). Moreover, the interconnectedness of patients, suppliers, and organizations is a result of the healthcare sector`s active social sustainability (Hussain et al., 2018).
Consequently, the novelty of this research lies in creating a detailed research model that incorporates KS, BPI, and IC in the association between TQM and CS utilizing RBV and IPT in the private healthcare sector of Ethiopia. Employee knowledge sharing and business process integration, or the integration of information within the organization, can enhance CS. Furthermore, since TQM is about continuous improvement, integrating IC within the organization can lead to CS (Razzak, 2022). However, the private healthcare system has not adequately scrutinized and analyzed the integration of KS, BPI, and IC in the relationship between TQM and CS. Therefore, this research aims to bridge the gap in existing literature and address the need for additional study on the association between TQM and CS.
The primary reason for conducting this study in Ethiopia is that, even though there have been improvements in providing high-quality health services during the last 30 years, progress has been sluggish and has not met global goals (Tessema et al., 2024). Ethiopia has been implementing several strategies and programs to increase patient satisfaction and enhance healthcare services (Croke, 2020). Nevertheless, significant attention is required for Ethiopia`s healthcare sector due to the country’s second-most populous status in Africa and internal and regional instability (Utino et al., 2023). The administration has prioritized enhancing the delivery of high-quality healthcare to the general public as a solution to this issue through high amount of budget and resource allocation (Alemayehu et al., 2023; Tofik et al., 2023). However, the increase in instability in neighboring countries, internal issues, a lack of proper resource use, and strategic planning hindered Ethiopia’s healthcare system’s success.
The managerial and theoretical implications of this study, which could lead to the implementation of human resource reforms in Ethiopian private hospitals, underscore its significance. The outcome of this research also significantly contributes to the strategic planning and decision-making of healthcare managers and policymakers. The research findings will also support the healthcare sector in reassessing its service processes to meet the goals of UNSDG 2030 and African Union Agenda 2063. Furthermore, this study adds knowledge to the healthcare literature regarding the relationship between TQM and CS, as well as theories of resource-based view and information processing.
The paper has the following structure: First, after the introduction, this paper will formulate assumptions through a comprehensive assessment of existing literature on the topic, and then construct a conceptual model based on the hypotheses. Furthermore, the research approach is explained. The third part involves testing the model and presenting the result. The final section of the paper presents the discussions, together with an analysis of the practical and theoretical contributions, limitations, recommendations for further research, and a conclusion.
Theoretical Background
Resource–Based View (RBV)
The RBV (Barney, 1991) posits a close relationship between corporate strategic resources and the long-term competitive advantage of the healthcare industry. Private hospitals can utilize TQM and knowledge as intangible resources to achieve corporate sustainability. Gürlek and Çemberci (2020) claim that organizations have the potential to gain a competitive edge through the strategic allocation of resources toward SDGs. TQM may enhance a healthcare`s performance by managing and developing knowledge that promotes the development of certain assets within the private hospital culture (Maravilhas & Martins, 2019). Moreover, according to RBV, the healthcare industry fosters innovative culture and corporate sustainability by utilizing intangible resources such as TQM, KS, and BPI that can support the healthcare sector to be competitive.
The RBV proposes that implementing TQM and knowledge as an intangible asset at different levels of the organization results in distinct resources and capabilities that enhance innovation and sustainability (Azeem et al., 2021). Furthermore, the deep ingraining of TQM and KS in an organization`s operational procedures pose significant challenges to the process of transferring them within the healthcare sector. Furthermore, TQM and knowledge pose challenges to replication, making it difficult for competitors to precisely imitate and build a strong and unique culture as a basic skill that enhances CS (X. Li et al., 2019).
Information Processing Theory (IPT)
IPT facilitates the exchange of information among staff, patients, and stakeholders such as government and insurance companies (Galbraith, 1973). According to IPT, effective organizational strategies should align with an organization’s capacity to manage and disseminate information to hospital staff and stakeholders in order to adapt and thrive in a dynamic environment and enhance organizational performance. To achieve successful firm performance, it is essential to align information processing requirements with the capabilities of both internal (doctors, nurses, and other medical staff) and external (NGOs, government, and insurance companies; Gales et al., 1992). Moreover, organizations, that use TQM as an intangible resource can improve corporate sustainability by sharing information about new technologies, innovation and competitors through organizational learning. According to Renger and Czirfusz (2022), there is a claim that integrated forms of care with quality management possess the capability to amalgamate many elements, such as resources, healthcare provision, care, rehabilitation, and health promotion, which can foster CS. Thus, this theory supports the mediating role of BPI the association between TQM and CS.
Total Quality Management (TQM)
Oluwajinmi and Longe (2023) define TQM as a strategic approach that aims to achieve patient satisfaction by implementing high-quality standards across all departments within the organization. Healthcare organizations are relatively new to the concept of TQM, which is based on principles set by quality pioneers such as Deming and Juran (Getele & Jean, 2020). In the healthcare industry, TQM is defined as a comprehensive strategy that aims to implement changes in the characteristics and attributes of all individuals, including professionals, physicians, nursing, technicians, and patients, for continuous improvement (Yang, 2020). Implementing TQM is critical for healthcare organizations to improve the quality-of-care services, improve management practices, foster organizational commitment, and improve patient satisfaction (Grossu-Leibovica & Kalkis, 2023; Tonjang & Thawesaengskulthai, 2022).
Furthermore, Abbas (2020) asserts that many quality models, including the European Foundation of Quality Management (EFQM) and the Malcom Baldrige National Quality Award (MBNQA), delineate the principles of TQM in both production and service sectors. However, this study used the American model of MBNQA, which incorporates six components of TQM such as leadership, strategic planning, customer focus, process management, human resource management, and information and analysis (Abbas, 2020; Nazarian et al., 2024). To foster continuous improvement in service quality, the private hospitals in Ethiopia need to apply these TQM components as part of their organizational culture.
Corporate Sustainability (CS)
CS refers to the reduction of adverse environmental effects, the advancement of social accountability, and the pursuit of economic, environmental and social sustainability (Cantele et al., 2024; Davenport et al., 2019). The fundamental principle underlying CS is the “triple bottom line of sustainability” concept introduced by Elkington (1998). This framework emphasizes the need to consider social, environmental, and economic factors when making sustainable decisions for the healthcare industry. CS and healthcare are closely intertwined, as environmental conditions directly influence the general population’s well-being (Urban & Maboko, 2020). Despite the design of health, their ecological footprint can negatively impact human well-being (Dion & Evans, 2024). The primary focus of hospitals is to both enhance public health and minimize their environmental footprint, which is part of UNSDG 7 (clean and accessible energy; Kanneganti et al., 2017).
Knowledge Sharing (KS)
KS means exchanging of knowledge, experiences and best practices among healthcare professionals, organizations, and patients (Mahmoud et al., 2024). KS can assist in identifying and resolving problems, reducing errors and waste, and fostering innovation (Agrifoglio et al., 2021; Wu et al., 2022). Furthermore, instantaneous KS is especially beneficial in remote regions (Nouri Khaneghah et al., 2024). Moreover, enhanced patient outcomes, decreased medical errors, and more individualized care have been associated with the exchange of knowledge and best practices (Malik et al., 2024). In the healthcare industry, KS is crucial for enhancing the quality of care, promoting innovation, and guaranteeing cost-efficient operations (Kosklin et al., 2023). Thus, in order to enhance healthcare delivery systems, the healthcare industry must remain committed to cultivating settings that promote and facilitate the exchange of knowledge at all levels (Monazam Tabrizi, 2023).
Business Process Integration (BPI)
BPI in healthcare refers to the alignment and unification of various administrative, clinical, and operational processes within and across healthcare organizations (Park & Moon, 2024). The goal of BPI in healthcare is to enhance coordination, reduce inefficiencies, and improve patient outcomes. Effective management of medical supplies, equipment, and pharmaceuticals required by healthcare organizations is contingent upon the implementation of efficient supply chain management, which is facilitated by business process integration (Ajegbile et al., 2024). Moreover, implementing process integration guarantees the availability of appropriate supplies and equipment at the required time, minimizing patient care delays and preventing expensive crises caused by inadequate stock (Dănescu & Popa, 2020). For instance, the immediate distribution of a patient’s test results to all relevant healthcare centers enables prompt and effective modification of treatment regimens (Sarkar, 2022).
Innovative Culture (IC)
As emphasized by Texeira-Quiros et al. (2022), enhancing the preparedness of healthcare institutions to innovate is crucial to address forthcoming difficulties such as population aging, workforce deficiencies, and diminished funding. Successful innovations typically exhibit two essential characteristics: they are both user-friendly and highly appealing (Igweh et al., 2020; Merviö, 2020). Enhanced comprehension of the interaction between many aspects that contribute to innovation at every stage of the innovation process, across a range of healthcare contexts, can assist healthcare managers in effectively incorporating innovation into their organizational structure (Gabriele, 2015). A progressive culture in healthcare is vital for tackling the sector’s intricate difficulties, optimizing patient outcomes, increasing efficiency, and minimizing costs (Kumi, 2023). A multitude of elements and trends are fostering an expanding culture of innovation, encompassing technological integration, patient-centered care, data-driven decision-making, and interdisciplinary collaboration (Akdemir et al., 2020).
Hypotheses Development
The Relationship Between TQM and CS
Compared to environmental and economic sustainability, social sustainability has not gotten as much emphasis as it should, particularly in emerging economies (Vafadarnikjoo et al., 2020). As emphasized by Nakhate and Kajale (2020), social sustainability and sustainable healthcare in the healthcare industry are heavily reliant on the interconnectedness of patients, suppliers, and organizations. However, it will be less successful to satisfy various stakeholder groups by concentrating only on economic sustainability (Mehedi & Jalaludin, 2020). Previous research has demonstrated the influence of TQM on CS (Hudnurkar et al., 2023; Nazarian et al., 2024; Tasleem et al., 2018).
According to RBV, a healthcare competitive advantage is dependent on its resources and skills (Barney, 1991). The RBV framework widely views TQM as a valuable asset because it incorporates unique organizational process and routines that significantly improve overall performance. This makes it a principal skill that may maintain a firm’s competitive edge and long-term corporate sustainability (Assensoh-Kodua, 2019). Moreover, IPT plays an intriguing role in facilitating the exchange of information based on the implementation of TQM methods in business. The reason for this is that TQM is a profound understanding of procedures and frequently a transformation in the organization’s culture, which rivals are unable to swiftly imitate (Posen et al., 2023). Therefore, the literature review suggests the following hypothesis:
H1: TQM has a significant and positive influence on CS.
The Influence of TQM on KS
TQM and KS are crucial concepts in the healthcare industry, focusing on enhancing the quality of treatment and services provided to patients and stakeholders (Chletsos & Saiti, 2019). Knowledge management is believed to enhance patient safety in hospitals. According to prior research findings (Abbas & Kumari, 2021; El Amrani, 2023; Kosklin et al., 2023), TQM significantly influences knowledge sharing and yields a positive and substantial outcome. However, there is a dearth of literature regarding the relationship between TQM and KS in the private healthcare sector of emerging economies. Moreover, Lebcir and Sideras (2021) emphasized that learning and knowledge sharing are important for implementation of TQM in the healthcare industry. Consequently, the subsequent hypothesis is proposed:
H2: TQM has a significant and positive influence on KS.
The Relationship Between TQM and BPI
Various scholars present differing perspectives on TQM and BPI. Some researchers have proposed that TQM and BPI are complementary and mutually reinforcing due to their shared concepts and goals, such as process orientation and customer focus. Some believe that TQM and BPI are incompatible and contradictory due to their differing assumptions and techniques, such as incremental versus radical change and bottom-up versus top-down engagement (Stravinskiene & Serafinas, 2020). Prior research does not provide a unified conceptual framework for combining BPI and TQM efforts to enhance organizational performance. However, according to the IPT, the healthcare sector with TQM practices can foster BPI through integration of processes with suppliers, employees, and patients to minimize costs and increase patient satisfaction. As a result, the following can be proposed:
H3: TQM has a significant and positive influence on BPI
The Relationship Between KS and BPI
The healthcare industry should prioritize internal and external process integration to reduce costs and improve efficiency and effectiveness in service delivery by utilizing intangible resources such as knowledge and TQM. RBV is a key theory that explains how BPI and KS help businesses stay ahead of the competition by turning implicit knowledge into explicit knowledge that helps them adapt to a changing environment. KS plays a role in facilitating BPI by allowing the transfer of information between medical professionals and stakeholders (Bitkowska, 2020). Nevertheless, there is a dearth of scholarly investigation into the association between KS and BPI. Therefore, it can be hypothesized that:
H4: KS has a significant and positive influence on BPI.
The Relationship Between BPI and CS
The key components of CS in the healthcare industry are environmental, economic, and social sustainability (Shahzad et al., 2019). Integrating internal and external business processes with resources improves an organization’s environmental, social, and economic sustainability (Tushman & Nadler, 1978). BPI entails restructuring and harmonizing processes to attain optimal performance, whereas CS concentrates on generating value while reducing environmental and societal effects (Mendling et al., 2018). There is little study on the association between BPI and CS. Therefore, this study aims bridge the knowledge gap. As a result, the following can be proposed:
H5: BPI has a significant and positive influence on CS.
The Relationship Between KS and CS
Alketbi and Ahmad (2023) proposed the implementation of CS, knowledge management, and sustainable development not only in manufacturing sector but also in sectors such as healthcare. In healthcare industry, KS refers to the dissemination of medical knowledge using collaborative communication methods to enhance healthcare workers` knowledge, skills, and capabilities. There is a dearth of study on how to effectively promote knowledge sharing activities within healthcare organizations. KS improves CS by focusing on a culture of KS among healthcare sectors employees (Marjerison et al., 2022). Organizations that have successful information management systems view KS as their societal obligation (Barao et al., 2017). Accordingly, it can be hypothesized that:
H6: KS has a significant and positive influence on CS.
The Mediating Role of KS in the Relationship Between TQM and CS
The direct association between KS, CS, and TQM, provide evidence of the mediating role of KS. Hassis et al. (2023) revealed KS as a crucial factor that promotes innovation and is essential for attaining CS in a dynamic and competitive environment. Prior research findings reveal that knowledge management, which includes KS, mediates the link between TQM and CS (Hussain, 2020; Mohsin et al., 2024). Moreover, research by Zehir and Zehir (2023) found that TQM positively impacts the financial performance of hospitals, with CS playing a mediating role in this relationship. Furthermore, Quddomi et al. (2020) revealed the mediating role of knowledge management in the association between TQM and CS.
As emphasized by RBV, knowledge is an intangible strategic resource that enhances competitive advantage and continuous improvements. Furthermore, KS within the organization can enhance a culture of organizational learning, which enhances innovation and achieving sustainable goals. These sustainability-related improvements can become a source of competitive advantage, as they are rare, valuable, and difficult for competitors to imitate (Hudnurkar et al., 2023). In essence, KS enables the effective application of TQM principles, which in turn can enhance CS, in line with the RBV’s emphasis on leveraging unique organizational resources for competitive advantage (Zaid & Sleimi, 2023). Therefore, in this study, it can be hypothesized that:
H7: KS has a mediation role between TQM and CS.
The Mediating Role of BPI in the Relationship Between TQM and CS
The direct relationships between TQM and CS provide evidence of the mediating role of BPI. According to the resource-based view, organizations that use TQM as a tool can improve sustainability, particularly economic sustainability, by enhancing information sharing within the organization and stakeholders (Barney, 1991). Furthermore, IPT asserts that integrating information among employees and stakeholders with total quality management in healthcare can boost patient satisfaction and sustainability performance (Galbraith, 1973; Gales et al., 1992). However, there is a research gap regarding BPI as a mediator in the association between TQM and CS. Thus, the current research aims to fill this research gap. Therefore, it can be hypothesized that:
H8: BPI has a mediation role between TQM and CS.
The Moderating Role of IC the Link Between KS and CS
Pedersen et al. (2018) suggested that business model innovation, which entails altering how a company generates and provides value, might impact CS positively or negatively, depending on the organization’s core principles. Some research suggests that there may be a negative or nonexistent relationship between TQM and an innovative culture (Hudnurkar et al., 2023). Vandavasi et al. (2020) found a strong and favorable relationship between KS and innovative culture. As emphasized by Theodora and Latief (2020), KS has a major impact on innovation. According to J. Li et al. (2021), innovative culture strengthens the positive impact of KS on CS. KS may not foster sustainable practices without an innovative culture (Tian & Wang, 2023). Leaders often place a high value on KS within an organization when they endorse and support innovation. Consequently, it can be hypothesized that:
H9: Innovative culture has a moderating role in the relation between KS and CS.
The Moderating Role of IC in the Link Between TQM and CS
Researchers have identified TQM practices as key contributors to the promotion of innovation (Daoud Ben Arab, 2022; Texeira-Quiros et al., 2022). According to Shuaib and He (2023), certain researchers have found that the relationship between TQM and innovation may not consistently exhibit statistical significance. Previous studies have yielded inconclusive results concerning the relationship between TQM and innovation (Khalfallah et al., 2022). Hussain (2020) revealed that innovation serves as a partial mediator in the association between TQM and the financial performance of organizations. Furthermore, Ali AlShehail et al. (2022) demonstrated that service innovation serves as a partial mediator in the association between TQM and sustainability. Moreover, the strategic planning of the healthcare industry regarding service quality and the perception of innovative culture significantly influence the application of TQM. Urban and Toga (2017) have noted that integrating IC into a broader framework significantly contributes to generational viability through the improvement of sustainable practices. Thus, it can be hypothesized that:
H10: IC has a moderating role between TQM and CS
Based on the above-mentioned explanations, the conceptual model is illustrated as Figure 1 below:

Conceptual model.
Methodology
Study Procedure and Sample
First, according to Ali et al. (2022), the healthcare system in Ethiopia consists of three levels: tertiary (specialist hospitals, specialty centers), secondary (general hospitals, specialty clinics), and primary (primary hospitals, medium clinics). Based on this information, out of 116 private hospitals reached, only 110 expressed a willingness to participate in responding to research questions. Self–administered questionnaires with an attached consent form were distributed, using convenience sampling method, to managers and supervisors of 110 private hospitals from 30 December 2023 to 28 February 2024. A cross-sectional study in primary, secondary, and tertiary hospitals in Adama, Hawassa, and Addis Ababa, Ethiopia.
Second, to avoid convenience sampling bias, data is collected from individuals based on availability rather than demographic representation, potentially leading to bias and distorted outcomes. Convenience sampling bias was mitigated by incorporating participants with diverse features or geographical areas. In fact, the study used convenience sampling to select hospitals, focusing on private hospitals due to their superior total quality management and sustainability practices compared to public hospitals in Ethiopia’s health care industry. Convenience sampling in this study involved engaging managers and supervisors of private hospitals who were on duty during data collection (Teimouri et al., 2018). Furthermore, self-administered questionaries were given to managers and supervisors of private hospitals that adhere to at least the ISO 9000 standard so that satisfactory results can be achieved regardless of the approach taken (García-Fernández et al., 2022). Indeed, self-administered sampling techniques minimize interviewer bias compared to face-to-face or online questionnaires and allow respondents to complete the research questionnaires at their own pace (Christensen et al., 2014).
Third, determination the required sample size for non-probability sampling and unknown populations presents a challenge in accurately estimating the overall population. In light of this, Cochran (1977) and Tessema et al. (2024) suggested a sample size of 384 with a margin of error of 5% and a confidence level of 95%. Furthermore, as stated by Memon et al. (2020), studies conducted at the organizational level, involving top-level executives such as supervisors and CEOs, may have a smaller sample size of 160 to 300 compared to studies conducted at the individual level, involving individuals such as patients and employees, when using more than one variable to statistically analyze using PLS-SEM. Consequently, managers and supervisors received a total of 384 structured questionnaires, yielding 286 responses, signifying a response rate of 74.5%. Thus, this response rate is considered sufficient for this study (Rahman, 2023).
Measurement Instrument
All constructs were assessed utilizing existing scales from the literature. The study employed self-administered questionnaires from reputable sources to ensure the reliability of the instruments used to evaluate the study population. The research questionnaires were adopted from widely acknowledged organizational studies, which provided a robust framework for evaluating the study’s characteristics (Sahranavard et al., 2024). This study utilized a total of 24 items to measure TQM, with six dimensions (leadership, strategic planning, customer focus, process management, human resource management, and information and analysis) each consisting of four items adapted from Nazarian et al. (2024). The four items used to measure KS were adopted from Azeem et al. (2021). The BPI was measured using five items, adopted from Narayaman et al. (2015). CS using 13 items, incorporating three dimensions: economic (4 items), environmental (4 items), and social sustainability (5 items) were adopted from Nazarian et al. (2024). Four items for measuring IC were adopted from Azeem et al. (2021). The measurement items were selected and modified to align with the aim of the research and to fit the healthcare context (see Appendix 1). All items were measured with a five-point Likert scale: from 1(strongly disagree) to (5 strongly agree).
Data Analysis
Partial least square structural equation modeling (PLS-SEM) was used with Smart-PLS version 4 to examine the association between study constructs (Hair et al., 2021). Pls-SEM is very appropriate for this research due to its small sample size and predictive accuracy, especially in the analysis of complex research models defined by several structures and indicators (Willaby et al., 2015). Moreover, Pls-SEM has the benefit of concurrently evaluating both the measurement and structural model outcomes (Jattamart & Kwangsawad, 2021). According to Hair et al. (2021), PLS-SEM indicates findings for content validity, as well as composite reliability (CR) and average variance extracted (AVE). In conclusion, considering the aforementioned factors, it is possible to declare that Pls-SEM was the most suitable tool for this research.
Result
Demographic Information
Table 1 indicates that most of the respondents are managers (185) and supervisors (101), which is 64.7% and 35.3%, respectively. Regarding the gender of respondents, males (154) and females (132) represented a ratio of 53.8% and 46.2%, respectively. In terms of age, 108 respondents, or 37.8%, are between the ages of 41 and 50, while 24 respondents, or 8.4%, are between the ages of 20 and 30. The respondents represent primary hospitals (31), secondary hospitals (155), and tertiary hospitals (100), accounting for 10.8%, 54.2%, and 35%, respectively.
Demographic Information.

Common Method Bias (CMB)
Research hypotheses were evaluated using numerical data, so it’s crucial to check for data bias. Moreover, a survey raises the potential for CMB to influence the data. Nevertheless, Harman’s single factor analysis (Podsakoff et al., 2012) effectively addresses this problem. Podsakoff et al. (2012) state that the first construct in Harman analysis should explain less than 50% of the variance. So, the results indicate that the initial unrotated components reported 29% of the variance, proving that there was no bias in the data.
Endogeneity Test
The first-order construct was initially assessed within the model containing the endogenous items. However, the analysis excluded Items PM1 from process management, SP2 from strategic planning, ECS4 from economic sustainability, and ENS1 from environmental sustainability due to their failure to meet the minimum requirements for item loadings on those constructs. Moreover, Smart PLS 4 employed with two-stage approach to estimate higher-order constructs. The two-stage method improves parameter recovery for paths in the path model that (1) link external constructs to the higher-order construct and (2) link the higher-order construct to an internal construct (Sarstedt et al., 2020).
Moreover, it is crucial to test the endogeneity of the model. Hult et al. (2018) and Irfan et al. (2023) have suggested that there are better ways to fix endogeneity in analyses and tests that can identify variability. Based on the Gaussian copula method with Smart-PLS 4, a p-value of more than .05 indicates that the residual correlation between the endogenous variable and the predictors is not statistically different from zero (Becker et al., 2022). Therefore, when applying the Gaussian copula methodology through bootstrapping, the p-values are above .05, indicating the absence of endogeneity (see Table 2).
Endogeneity Test.

Note. cIndicates the copula term in the model.
Measurement Model Assessment
First, this study examined the internal consistency and reliability of the items, using Cronbach`s alpha (CA) and composite reliability (CR). Table 3 indicates values of CA and CR above the minimum threshold of 0.70 (Sarstedt et al., 2020). As a result, there is no issue with the data’s internal consistency and reliability.
Evaluation of Measurement Model.

Note. n = 286. CA = Cronbach’s alpha; VIF = variance inflation factor; CR = composite reliability; AVE = average variance extracted.
Second, convergent validity (CV) was assessed which refers to the degree to which a measure has a positive correlation with other measures that at the same time measure the same construct (Hair et al., 2021). CV was assessed using average variance extracted (AVE). When the construct exhibits an AVE value of 0.50 or above, it indicates that, on average, the variables it measures account for more than 50% of the variation (Hair et al., 2019). An alternative method for examining an item`s CV is to check its outer loadings. In this case, the outer loading value for every component is greater than 0.70 (Hair et al., 2021).
Third, after CV, the discriminant validity (DV) was assessed using Fornell and Larcker’s criteria. Table 4 illustrates how the Fornell and Larcker (1981) evaluation criterion assesses the comparability of each AVE construct in the correlation matrix by examining its bivariate correlations with all divergent components, employing the square root method. Thus, the finding of this study indicated that there was no discriminant validity issue (see Table 4).
Fornell and Larcker Criterion.
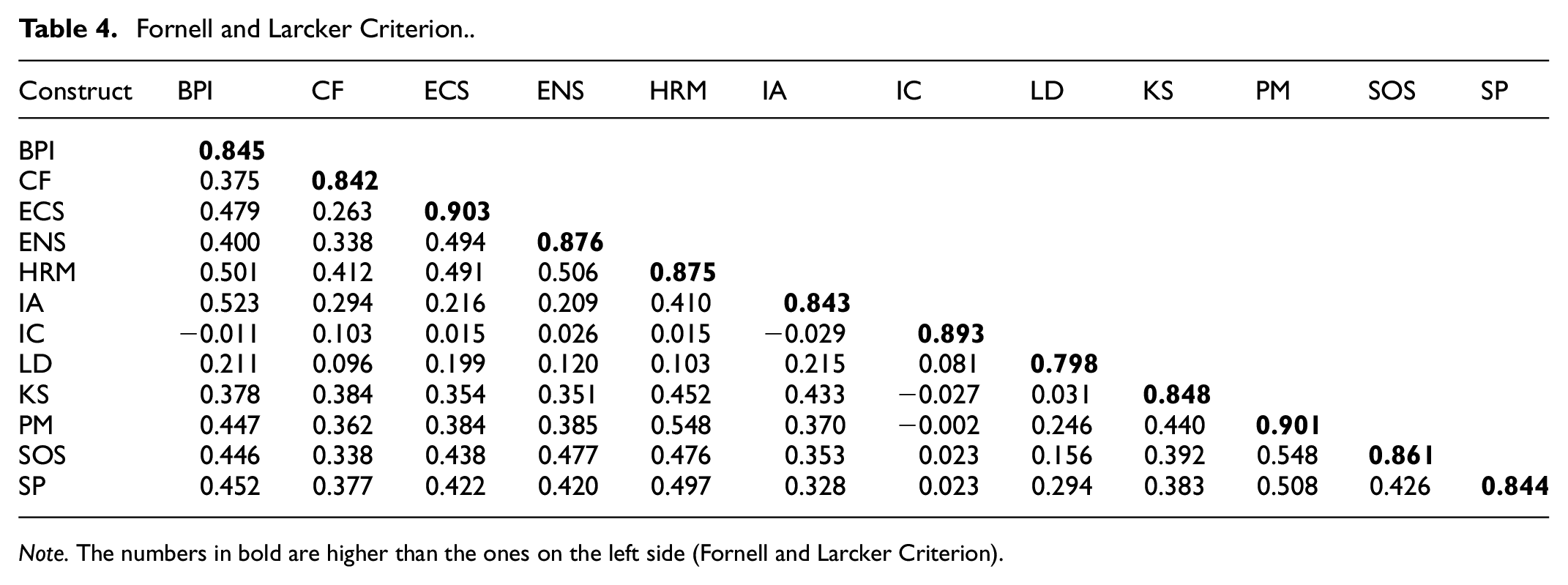
Note. The numbers in bold are higher than the ones on the left side (Fornell and Larcker Criterion).
Finally, previously mentioned methodology for assessing discriminant validity was insufficient. Therefore, heterotrait-monotrait ratio (HTMT) is utilized as an additional criterion to validate the presence of discriminant validity. As presented in Table 5, the HTMT value is within an acceptable range below 0.90, and the criteria have also been met (Henseler et al., 2015). Hence, there is no issue of discriminant validity.
Heterotrait-Monotrait Ratio (HTMT).

Structural Model Assessment
Table 6 and Figure 2 demonstrate that all direct effects of the predictor on the dependent variable are significant and supported, with the exception of hypothesis 4, which proved to be insignificant and unsupported. It was also found that KS and BPI played a part in the paths (TQM → KS→ CS) and (TQM → BPI→ CS), with values of (H7: β = .064, t = 1.860, p = .031) and (H8: β = .118, t = 2.669, p = .004), respectively. Therefore, we support hypotheses 7 and 8. Furthermore, the moderating role of IC in the path (IC × KS → CS) was found insignificant with value (H9: β = −.071, t = −0.069, p = .169). Thus, hypothesis 9 is unsupported. However, IC moderates the relationship between TQM and CS (IC × TQM → CS) with a significant value of H10 (β = .125, t = 0.109, p = .037). Thus, hypothesis 10 is supported.
Results of Hypothesis Testing.

Note. n = 286. BPI = business process integration; CS = corporate sustainability; IC = innovative culture; KS = knowledge sharing; TQM = total quality management.

Structural model assessment.
Second, model fit was evaluated and determined using the value of R2 (see Table 6). The coefficient of determination (R2) value is utilized to measure the explained variance of independent latent constructs for the related dependent variable. Values of 49.3%, 40%, and 31.5% found for CS, BPI, and KS, respectively, indicate substantial, moderate, and weak effects (Hair et al., 2021). Thus, total quality management explains 49.3% of the variance in corporate sustainability, a significant effect that surpasses the values of 0.401 and 0.315. Moreover, the 40.1% variance of BPI explains TQM. The value is larger than 0.315 but lower than 0.493, indicating a moderating effect. Finally, the 31.5% variance of KS explains TQM. The value is lower than 0.493 and 0.401, indicating a weak effect.
Third, Table 6 shows predictive relevance of the structural model through Stone-Geisser Q2 by running the blindfolding procedure (Geisser, 1975). The Q2 measures the extent to which the prediction is successful with a threshold value larger than zero. As reported in Table 6, the Q2 values of corporate sustainability (Q2 = 0.434), business process integration (Q2 = 0.389), and knowledge sharing (Q2 = 0.299) meet the requirements of the suggested value. These results indicate that the model is predictive and model fits the data well.
Finally, following predictive relevance, model fit analysis was conducted using SRMR and NFI. The value of SRMR for the estimated model is 0.061, below the threshold of 0.08 for model fit indices, suggesting a satisfactory match with the data, and the NIF value is 0.907, above the minimum requirement of 0.9 (Goretzko et al., 2024). Thus, model fit is accepted.
Discussion
The main goal of this study is to investigate the influence of TQM on CS directly and through the mediating, and moderating effects in Ethiopia’s private healthcare sector, using the resource-based view and information processing theory.
Hypothesis 1 anticipated a positive and significant influence of TQM on CS, and the result indicates a positive and significant association. The study findings of Hudnurkar et al. (2023) and Nazarian et al. (2024) also supports result of the current research. The result of this research implies that TQM can improve CS in the private healthcare industry by fostering a culture of quality, excellence, and responsibility. Furthermore, the current research outcome has a significant practical implication for healthcare policy makers and managers in their decision making and strategic planning. Moreover, this hypothesis`s finding respond to the need for further research in other service sectors, including healthcare, and shows significantly consistent with the findings in the other service sectors (Acquah et al., 2023; Albloushi et al., 2023; Ali AlShehail et al., 2022). The result of this research revealed that the finding of TQM and CS in the service sector can be applicable in the healthcare sector.
Hypothesis 2 proposed that TQM has positive and significant influence on KS, and the findings of this study supported the hypothesis, which aligns with the results of prior researches by Abbas and Kumari (2021) and El Amrani (2023). Implementing TQM in private hospitals helps improve knowledge sharing, which is vital for the staff to learn and innovate. The finding indicates that the relationship between TQM and KS in private healthcare is significant, which is in line with finding of other service sectors (El Amrani, 2023; Kosklin et al., 2023). Therefore, the healthcare industry can apply the findings of TQM and KS effectively.
Hypothesis 3 hypothesized that TQM has a positive and significant influence on BPI, and the finding of this study support the association and is in line with the theoretical framework of information processing theory. Hypothesis 4 stated that KS has a significant and positive influence on BPI. However, our finding contradicts the stated hypothesis and previous research findings of Bitkowska (2020). Hypothesis 5 expected that BPI has a significant and positive influence on CS, which is align with the findings of this study. The healthcare sector can achieve economic sustainability by integrating processes with healthcare professionals and NGOs to provide inexpensive services to society while also improving efficiency and productivity.
Hypothesis 6 postulated the impact of KS on CS, and the result revealed a positive relationship between KS and CS. This result is in line with the research findings of Marjerison et al. (2022) and Oxenswärdh (2019). This research result confirms that KS can improve economic sustainability by boosting efficiency, productivity, and social sustainability in the healthcare sector while maintaining the safety and well-being of patients, communities, and staff.
Hypothesis 7 suggests that KS is partially mediating the link between TQM and CS. The result supports this suggestion and aligns with the prior results of Abbas (2020) and Nazarian et al. (2024). This research shows that the private healthcare industry can enhance CS by using TQM and facilitating knowledge sharing among healthcare professionals and stakeholders, including NGOs, the government, and insurance companies. KS practices strengthen the implementation of TQM principles, leading to enhancements in the environmental, social, and economic aspects of sustainability (Park & Hong, 2022).
Hypothesis 8 The finding the current research is supported Hypothesis 8, which is consistent with the theoretical framework of information processing theory, indicating that BPI can improve TQM by facilitating information sharing among hospital staff to promote CS. The implementation of TQM in the healthcare industry relies on the organizational culture and the ability to share information across personnel and stakeholders and insurance companies (Gales et al., 1992).
Hypothesis 9 posited that IC moderates the association between KS and CS in the private healthcare industry. However, hypothesis 9 revealed that IC is not moderating the relationship between KS and CS. The result of present research contradicts previous research finding of Arsawan et al. (2020). This study revealed that IC can’t strengthen or weaken the relationship between KS and CS; rather, other factors such as organizational culture and organizational learning might moderate the relationship since KS depends on the KS culture of the healthcare staff. The possible explanation for this finding is that CS involves multifaceted factors beyond KS, such as stakeholder engagement and supply chain management. IC might reach a point of diminishing returns. However, factors like leadership support, organizational culture, and market demands play a more significant moderating role.
Hypothesis 10 hypothesized that IC moderating the association between TQM and CS. The finding of this research support hypothesis 10. This study’s finding revealed that an innovative culture influences the relationship between TQM and CS, which is consistent with prior study finding by Hudnurkar et al. (2023). This research result has made a unique contribution to existing knowledge in the private healthcare industry. The possible explanation for hypothesis 10’s finding is that the application of TQM concepts in the private healthcare sector can foster corporate sustainability, and the incorporation of an innovative culture within the organization strengthens the potential to optimize the healthcare sector’s sustainability performance, including economic, environmental, and social sustainability.
Theoretical Implication
The present study makes a valuable contribution to the existing body of knowledge on total quality management through multiple avenues. First, the study’s finding support and contribute to the RBV and IPT, considering TQM and KS as intangibles, can assist in achieving corporate sustainability and sustainable development goals. Thus, these theories shed light on the existing literature.
Second, this study introduces a novel approach by integrating BPI, KS, and IC into an existing TQM and CS model in private hospitals in emerging economies. This study aims to present a more concise and coherent explanation of the mechanisms through which TQM improves CS by utilizing RBV and IPT. Furthermore, the utilization of this study in private hospitals within emerging economies enhances its originality.
Third, the findings of this research add knowledge to the literature on healthcare in emerging economies. Specifically, this research contributes to the literature on total quality management and corporate sustainability. Furthermore, the result of this research answers the call made by prior researchers and contributes to the literature of healthcare by filling the gap regarding the application of TQM and CS in the healthcare industry of the emerging economy.
Managerial Implication
The current research would help managers and supervisors of private hospitals understand the importance of total quality management in enhancing corporate sustainability. The results of this study revealed that implementing total quality management as an intangible resource is possible to achieve the UNSDGs 2030, AU 2063, and CS. To foster CS, private hospital managers and supervisors should incorporate TQM components and concepts such as continuous improvement, process management, customer focus, information and analysis, leadership, and human resource management. Furthermore, private hospital management should be able to identify both the immediate strengths and weaknesses, as well as the long-term strategies and capabilities of potential competitors. This will let the private hospital managers respond quickly to competitors` actions to achieve stronger corporate sustainability.
Moreover, the study’s findings on KS and BPI, when combined with TQM practices, could serve as a viable strategy for gaining a competitive advantage, leading to sustainable performance in economic, social, and environmental domains. Therefore, managers should view TQM and knowledge as intangible organizational resources, particularly tacit knowledge that potential competitors cannot replicate. Furthermore, the results of this research are crucial for managers to use for policy and decision-making. From a practical perspective, understanding the connections under research is a valuable contribution, as it could also offer insights for developing strategies to build a more flexible and adaptable healthcare system in countries with emerging economies.
Furthermore, the study’s findings primarily refer to Ethiopia’s private healthcare sector, particularly in regions characterized by comparable socioeconomic circumstances and healthcare systems. Moreover, the research findings help managers shape policy and practice in emerging economies’ healthcare sectors by integrating total quality management practices into the healthcare system.
The study’s findings hold significant implications for healthcare institutions outside Ethiopia. By adopting TQM principles, these institutions can improve their environmental, social and economic sustainability, leading to better patient care and community health outcomes. TQM practices in other geographical locations can enhance service delivery and patient experience, particularly in emerging countries with limited healthcare resources.
Limitations and Future Recommendations
Apart from the previous notable contributions, the study has limitations that may provide insights for future research endeavors. This study focuses only on private hospitals in Ethiopia, an emerging economy, and data is collected from managers and supervisors using a convenience sampling technique. Therefore, the findings cannot be generalized and may not be extended to public hospitals. Application of TQM will vary across sectors and countries, as well as between developed and emerging economies. Future research should aim to validate this research across various sectors (i.e., banks and hotels) and cultural contexts (i.e., developed and developing). Furthermore, future researchers may expand the model to examine external factors, such as economic conditions, technological advancements, which could impact the effect of TQM practices on CS.
Secondly, this research is unable to compare the periods before and after the implementation of TQM. This constraint further limits the scope of the study. Longitudinal studies are recommended for assessing TQM procedures over time. Moreover, an intrinsic limitation of the cross-sectional study is its vulnerability to bias. Future studies should employ the longitudinal data collection method to mitigate the bias.
Thirdly, the current study explored the mediation and moderation paradigm by establishing a relationship between TQM and CS. Potential moderators such as leadership support, economic conditions, and technological advancement can expand this research model.
Conclusion
In Ethiopia`s private healthcare sector, the current research found a structural relationship between TQM and CS. It also empirically investigated KS’s and BPI’s mediating mechanisms, as well as IC’s moderating role. The current research revealed a significant association between TQM and CS, both directly and indirectly, as well as through the moderating role of IC. The current result enhances resource-based view and information processing theory by integrating TQM, BPI, KS, IC, and CS. Furthermore, the findings suggest that the corporate sustainability outcomes of the private healthcare sector rely on the implementation of TQM practices within the hospital, the culture of knowledge sharing, the integration of business processes between the hospital, suppliers, and patients, and the innovative culture of the healthcare system. Therefore, it is imperative for healthcare industry managers and supervisors to optimize the application of all aspects of TQM practices within their organization. Moreover, the results of this research support managers in constructing a strategic vision for long-term development based on sustainable growth, which is of utmost importance for private hospitals, particularly in countries like Ethiopia that are currently grappling with regional and internal instability.
Footnotes
Appendix
Research Questionaries.

| Constructs | Items |
|---|---|
| Total quality management | |
| Customer focus | 1. The hospital employees and managers are in close contact with patients. |
| 2. The hospital has an effective Patient management system. | |
| 3. Patients are supported to submit complaints and proposals for quality improvements. | |
| 4. The hospitals` objectives overcome patients’ expectations. | |
| Information and analysis | 1. The hospital has effective information and reporting system for all services. |
| 2. The management regularly provides quality data (errors, complains) to the workers. | |
| 3. Workers and managers can easily retrieve information about different products and services. | |
| 4. All departments coordinate with each other to implement and monitor quality improvements programs. | |
| Human resource management | 1. Every aspect of the organization incorporates the “total quality concept” in training processes. |
| 2. Every department of the organization engages in quality-related training for hourly employees. | |
| 3. The hospital has a provision to monitor the level of feedback provided to employees regarding their quality performance. | |
| 4. Effectiveness of quality circles or employee involvement-type programs in the organization. | |
| Leadership | 1. Management of hospital assume responsibility for quality performance |
| 2. Management in hospital actively participate in the continuous improvement programs. | |
| 3. Quality issues are reviewed in the Hospital`s management meetings. | |
| 4. Managers have objectives for quality performance. | |
| Process management | 1. The hospital continuously improves its delivery processes, to enhance the overall service quality development. |
| 2. Process improvement initiatives are shared among departments. | |
| 3. We evaluate services on the basis of efficiency, including cost and timeliness. | |
| Strategic planning | 1. The quality objectives are being set on patients’ needs and requirements. |
| 2. The hospital integrates public responsibility into performance improvements. | |
| 3. Every staff member in the hospital is aware of our strategic objectives and the action plans to be accomplished. | |
| Business process integration | 1. We regularly apply newly obtained knowledge into practice to solve different operational issues. |
| 2. The hospital quickly responds to patients` and suppliers` needs. | |
| 3. The hospital uses the acquired knowledge obtained to offer new /improved services to patients. | |
| 4. The hospital uses the knowledge obtained from experience and mistakes to improve operational and financial performance. | |
| 5. The hospital uses the acquired knowledge to develop strategies. | |
| Knowledge sharing | 1. The employee of the hospital participates in informal discussion to share knowledge. |
| 2. The employees of the hospital are using technological tools (e-mail, etc.) to transfer knowledge. | |
| 3. The employees of the hospital have frequent meeting sessions. | |
| 4. The employees of the hospital have frequent meeting sessions. | |
| Innovative culture | 1. Your hospital tries out new ideas. |
| 2. Your hospital is creative in its methods of operation. | |
| 3. Innovation is readily accepted in management. | |
| 4. Your hospital encourages and supports innovative activities. | |
| Corporate sustainability | |
| Economic sustainability | 1. The hospital offers quality services with low cost. |
| 2. The hospital effective operational performance has resulted in improved market share. | |
| 3. The hospital has experienced a significant increase in overall profit. | |
| Environmental sustainability | 1. The hospital handled or stored toxic waste responsibly. |
| 2. The hospital uses products with less environmentally damaging than previous years. | |
| 3. The hospital reduced environmental impacts of service process or eliminated environmentally damaging service process. | |
| Social sustainability | 1. The hospital regularly participates in social development programs, e.g., support to underprivileged and needy ones to improve the society. |
| 2. The hospital regularly provides opportunities to youngsters, e.g., training and development to promote their talent. | |
| 3. The hospital regularly provides financial and non-financial support to NGOS, medical institutions, and related organizations for healthy lifestyle. | |
| 4. The hospital provides financial and non-financial support to educational institutions for students learning and development. | |
| 5. The hospital encourages its employees to participate in voluntary activities. | |