
Abstract
This study, positioned within the interdisciplinary fields of health informatics, technology acceptance, and digital health, aims to (1) explore digital health literacy (technophobia and eHealth readiness) influencing the adoption of telemedicine in emerging markets by extending a well-known technology acceptance model (TAM), and (2) examine the moderating effect of trustworthiness on telemedicine adoption in emerging markets. A quantitative approach was employed using a self-administered questionnaire as the research tool. The survey was conducted in Thailand, representing an emerging market context. Based on 281 samples of Thai respondents, the results reveal that eHealth readiness significantly positively impacts perceived ease of use. Additionally, perceived usefulness was a key driver of telemedicine adoption in emerging markets. Likewise, technophobia shows a significant negative impact on perceived ease of use but does not show a significant negative effect on perceived usefulness. The results of moderation analysis show that trustworthiness partially moderates the relationship between perceived ease of use and telemedicine adoption, such that higher levels of trustworthiness strengthen the positive impact of perceived ease of use on telemedicine adoption. These findings indicate that enhancing eHealth readiness and maintaining the ease of use of telemedicine platforms are critical strategies for promoting telemedicine adoption in emerging markets while technophobia seems to be a significant barrier that deters the perception of ease of use. This research offers useful insights for policymakers and healthcare practitioners seeking to effectively adopt telemedicine in various socio-economic contexts.
Plain language summary
Telemedicine allows patients to consult doctors, receive diagnoses, and access healthcare without traveling to a clinic or hospital. It is especially helpful in developing countries where access to healthcare services may be limited due to distance, infrastructure, or a shortage of medical professionals. However, not everyone adopts telemedicine easily. This study explores how digital health literacy, trust, and psychological factors influence the use of telemedicine in Thailand, a developing country. The research highlights two key aspects of digital health literacy: technophobia (fear or discomfort with using technology) and eHealth readiness (preparedness to use digital health services). The study found that people who are more prepared to use technology are more likely to find telemedicine easy to use. In contrast, individuals who experience technophobia are less likely to adopt telemedicine because they perceive it as difficult to use. Another important factor is trustworthiness—whether people believe telemedicine platforms are reliable and secure. The study shows that trust can strengthen the link between how easy telemedicine is to use and a person’s willingness to adopt it. However, trust does not significantly affect how useful people perceive telemedicine to be. These findings suggest that increasing digital skills, reducing fear of technology, and building trust in telemedicine systems can encourage its adoption in developing countries. Practical steps include providing training programs to improve digital literacy, designing user-friendly platforms, and ensuring strong security measures for patient data. This research offers valuable insights for healthcare providers and policymakers to improve telemedicine services, making healthcare more accessible and efficient for people in developing regions.
Keywords
Introduction
Telemedicine has been realized as one of the innovative healthcare approaches to the delivery of healthcare services, especially in areas where there are limited accessibilities due to various barriers such as geographical distance, inadequate infrastructure, and a shortage of healthcare professionals. Telemedicine provides an opportunity to fill the gap by overcoming geographical and logistical barriers that have obstructed the delivery of timely and effective healthcare services (Nitisha et al., 2023; Schürmann et al., 2025). As a result of the COVID-19 pandemic, healthcare systems worldwide have had to rapidly adjust by including telemedicine in conventional healthcare services to decrease physical contact and lower the risk of virus transmission. In other words, the COVID-19 pandemic emphasized telemedicine’s capability to deliver important healthcare to communities, which resulted in a global increase in the use of telemedicine (Omboni et al., 2022; Shen et al., 2021).
Although the benefits of telemedicine are clear, increasing the telemedicine adoption rate, especially in the context of emerging markets, faces various challenges. These challenges encompass various technological obstacles, one of which is digital health literacy. Several factors fall under digital health literacy (Alawiye, 2024; Arora et al., 2024; Bali, 2019). The first factor, technophobia, refers to which refers to the fear or anxiety about using technology, can significantly hinder the adoption of telemedicine, especially in populations less familiar with digital technologies (AlQudah et al., 2021). Developing economies, where digital literacy levels may be lower and access to technology may be less extensive, are particularly susceptible to this psychological barrier (Al-Samarraie et al., 2020; Arora et al., 2024). Users may avoid participating in telemedicine platforms due to the anxiety associated with unfamiliar technology, thereby restricting the potential reach of telemedicine services (Nitisha et al., 2023). Furthermore, eHealth readiness, which refers to the preparedness of individuals and healthcare systems to adopt electronic health services, may also play an important role as one of the determinants in enhancing the perception and adoption of telemedicine (Hsiao et al., 2023). eHealth readiness encompasses various issues such as digital literacy, infrastructure accessibility, and confidence in using online health information (Alawiye, 2024). In numerous emerging markets, the introduction of telemedicine is hindered by gaps in infrastructure, such as unstable internet access and restricted availability of digital devices (Antwi & Opoku-Mensah, 2021). Additionally, the presence of infrastructure alone does not guarantee the successful adoption of digital technology in healthcare. The absence of digital literacy and reluctance to embrace change among healthcare providers and patients might create additional challenges in the adoption process (Gunasekeran et al., 2021). Previous research has demonstrated the widespread use of models such as the Technology Acceptance Model (TAM) to comprehend the adoption of various information systems and technologies (Brown et al., 2022).
According to Venkatesh and Davis (2000), TAM posits that two vital factors, which are perceived ease of use and perceived usefulness are key determinants of an individual’s intention to use a new technology. Nevertheless, in the context of telemedicine, other psychological and contextual factors, such as technophobia and eHealth readiness, may significantly impact the adoption of health-related technology, especially in healthcare and telemedicine within emerging markets (Dehzad et al., 2014; Hsiao et al., 2023; Sukardi et al., 2021). Whereas TAM has been effective in explaining technology adoption in various contexts, applying it in healthcare frequently requires extending TAM to include variables that address the unique challenges and dynamics of this sector (Alsyouf et al., 2023). An extension of the Technology Acceptance Model (TAM) that includes unique factors such as technophobia and eHealth readiness may help us better understand the complexities involved in telemedicine adoption in an emerging market context. Furthermore, we have not thoroughly explored the role of trustworthiness in moderating the relationship between perception factors and telemedicine adoption. Trust in technology is of importance in the healthcare industry, where sensitive personal data is involved. In the absence of this trust, even useful technologies like telemedicine may struggle to achieve extensive adoption (Rahman et al., 2020; Yulaikah & Artanti, 2022).
To fill these gaps, the study aims to extend the application of TAM by including two critical factors, which are technophobia and eHealth readiness, to better understand the telemedicine adoption situation in emerging markets. In addition, this study explores the moderating role of trustworthiness on the relationships between telemedicine perceptions and intention to adopt telemedicine. The research aims to provide valuable insights for policymakers and healthcare professionals working to promote the effective implementation of telemedicine in a variety of socioeconomic contexts. This study contributes to the interdisciplinary fields of health informatics, behavioral technology adoption, and the sociology of health and illness, particularly in the context of emerging economies.
We organize the remainder of this paper as follows: Section 2 details the theoretical foundation and conceptual framework, exploring existing literature on technology adoption models, technophobia, eHealth readiness, and trust. Section 3 outlines the study’s research methodology. Section 4 presents the data analysis and research findings. Section 5 discusses the theoretical contributions and managerial implications. Section 6 provides the conclusion, while part 7 addresses the limitations of the study and suggests directions for future research.
Literature Review
This section reviews the relevant literature by first discussing technology adoption in the telemedicine context through the lens of the Technology Acceptance Model (TAM). It then elaborates on three critical constructs—technophobia, eHealth readiness, and trustworthiness—as essential extensions to TAM in understanding telemedicine adoption, particularly in emerging markets.
Technology Adoption in the Telemedicine Context
The realization of telemedicine as an innovative healthcare delivery method allows for the provision of medical services without the need for physical presence. Telemedicine can help healthcare providers deliver healthcare services to patients in remote, rural, or underserved areas. By exploiting the advances of digital technologies, telemedicine enables healthcare providers to conduct consultations, make diagnoses, and even administer treatments across distances, thereby making healthcare more accessible and efficient. Integrating telemedicine into healthcare services not only improves patient outcomes by ensuring timely access to care, but it also optimizes resource utilization within healthcare systems. Previous research has endeavored to explore and understand what factors enhance the adoption of telemedicine by examining several factors on both the healthcare provider and patient sides. Several factors impact the adoption of telemedicine, and by understanding these factors, healthcare policymakers, and providers can develop effective strategies that foster the integration and acceptance of telemedicine services.
The Technology Acceptance Model (TAM) developed by Davis (1989) is one of the most extensively used frameworks to explain new technology adoptions, including health-related technologies like telemedicine, because of the model’s simplicity and predictive power. According to TAM, perceived ease of use (PEOU) and perceived usefulness (PU) are two key determinants influencing the likelihood of adopting new technologies. PEOU describes the degree to which a person believes that using a particular system or technology will be free of effort. PU refers to the degree to which an individual believes that using the system or technology will enhance their job performance or daily activities (Davis, 1989). Both factors shape an individual’s attitude toward adopting technology, which in turn influences their behavioral intention to adopt it (Davis, 1989; Venkatesh & Davis, 2000). Previous studies have used and expanded the TAM to explain telemedicine adoptions in healthcare. For example, the study of Kamal et al. (2020) investigated factors affecting the acceptance of telemedicine services by including additional variables such as trust and facilitating conditions. In their context, “trust” primarily referred to the users’ confidence in the telemedicine services provided and the security of the system. The findings reveal that perceived ease of use and perceived usefulness are the important determinants of telemedicine adoption. Furthermore, trust and the availability of essential infrastructure play significant roles in improving acceptance rates. Orruño et al. (2011) applied a modified TAM to assess the adoption of teledermatology by healthcare professionals and found that perceived usefulness, ease of use, social influence, and trust were crucial factors in driving the adoption of the technology. Zhou et al. (2019) conducted a study to explore the factors influencing elderly patients’ intentions to adopt and use telemedicine systems in China with an extended TAM. The findings suggest that factors such as medical service satisfaction, perceived ease of use, and information quality significantly influenced the acceptance of telehealth systems.
Technophobia eHealth Readiness and Trustworthiness
Other psychological and contextual factors, such as technophobia, eHealth readiness, and trustworthiness, may play important roles in affecting the adoption and continued use of health-related technology like telemedicine. While trust often refers to a general willingness to rely on a system or service, trustworthiness specifically denotes the inherent qualities of the technology or platform that elicit such confidence, encompassing aspects like security, reliability, and data privacy (Watermeyer et al., 2022; Wing, 2020). Extending beyond the conventional constructs of perceived ease of use and perceived usefulness in TAM may provide a more comprehensive understanding of the factors that impact the adoption and continued use of telemedicine, especially in the emerging market context, where limited effective infrastructures and people possess limited digital literacy.
Technophobia is a psychological condition characterized by irrational fear or anxiety about using new technology. Numerous factors, including cognitive, emotional, and behavioral components, affect technophobia, which involves negative attitudes toward technological advancements (Nestik et al., 2019). Technophobia can be apparent in several ways, such as a hesitance to use digital applications, unease with new technological advancements, or an avoidance of any type of technology-based engagement (Khasawneh, 2015; Kotzé et al., 2016). Technophobia is not only a dislike of technology. It frequently refers to irrational fear that can lead to resistance to adopting new technologies, even if they have clear advantages (Kotzé et al., 2016). Technophobia can hinder the adoption and use of telemedicine in certain contexts. Patients who possess technophobia may be unwilling to be involved with telemedicine platforms. A previous studies revealed that to reduce technophobia, providing sufficient training and support is one of the key strategies that need to be implemented (Karahanna & Straub, 1999; Turan, 2019).
eHealth readiness refers to the preparation of healthcare organizations, professionals, and patients to embrace and proficiently use electronic health technologies (Jennett et al., 2005; Mauco et al., 2021). Positive attitudes toward telemedicine and an increased probability of its adoption correlate with greater levels of eHealth readiness (Gagnon et al., 2012). On the one hand, insufficient digital literacy by patients or potential users can lead to less probability of adopting new technologies, especially in emerging markets where disparities in technology access are more evident (Khoja et al., 2013). Khoja et al. (2007) developed an eHealth readiness assessment tool for healthcare organizations. They emphasized the assessment of technology, human, and organizational elements before the implementation of eHealth solutions. This method ensures that healthcare providers are sufficiently prepared to handle the complications of digital health platforms, later increasing the likelihood of effective adoption and usage. eHealth readiness also includes the digital literacy of healthcare professionals and patients, as well as the availability of supportive infrastructures. Insufficient eHealth readiness can lead to important challenges, including resistance to technology adoption and poor user experience, and eventually lead to the failure of telemedicine initiatives (Tamburis et al., 2012).
Trustworthiness in the context of health-related technology like telemedicine can be referred to as the degree to which patients have confidence in the privacy, safety, security, and reliability of the technology being used (Templeton, 2010). Trustworthiness plays an important role in the adoption of telemedicine. This is because healthcare encompasses personal information; therefore, patients need to be confident that their personal information and medical records are confidential. Prior studies have revealed that increased levels of trust result in enhanced adoption and utilization of telemedicine services (Bahari et al., 2024; Du et al., 2022).
Extending TAM by including psychological and contextual factors such as technophobia, eHealth readiness, and trustworthiness will provide a more comprehensive approach to better understanding the telemedicine adoption situation. Healthcare providers and policymakers can make it easier for people to accept and use telemedicine systems by reducing technophobia, improving eHealth readiness, and building trust. All of these things are important for making sure that telemedicine can fully realize its potential in improving healthcare access, quality, and efficiency, especially in developing countries where problems like poor infrastructure and differences in digital literacy are more common. Addressing these concerns may narrow the disparity in the adoption of telemedicine, ensuring that a wide range of communities can take advantage of the progress made in digital healthcare.
Hypothesis Development
In this section, we develop hypotheses based on the theoretical foundation and previous research discussed earlier. We design each hypothesis to examine the relationships between key variables influencing telemedicine adoption, particularly in emerging markets where psychological barriers, infrastructure limitations, and varying levels of digital literacy may play significant roles.
Prior research has highlighted technophobia as a critical barrier to the adoption of new technologies (Khasawneh, 2015; Wang et al., 2023). Technophobia, often rooted in fear and anxiety associated with technological change, is considered a significant psychological impediment to technology acceptance (Guo et al., 2013; Venkatesh, 2000). According to Gelbrich and Sattler (2014), the negative impact of technophobia is particularly pronounced among individuals with limited prior exposure to the technology in question. Technophobia can adversely influence users’ perceptions in two key areas. First, it is likely to reduce perceived ease of use, as individuals experiencing anxiety toward technology may view telemedicine systems as complicated or overwhelming. Second, it may diminish perceived usefulness, as technophobic individuals may fail to recognize or appreciate the benefits of telemedicine due to their discomfort or lack of engagement with the technology (Kotzé et al., 2016). Building on this rationale, the following hypotheses are proposed:
Prior studies confirmed the relationship between eHealth readiness and health-related technology acceptance and adoption (AshaRani et al., 2021; W. L. Lee et al., 2021). The study by M. A. Lee et al. (2022) found that technology readiness is one of the key determinants of healthcare information technology. Individuals with higher levels of eHealth readiness are more likely to perceive such technologies as easy to use. When people are well-prepared—possessing adequate knowledge, digital skills, and access to necessary infrastructure—they are more likely to find telemedicine systems accessible and user-friendly (Mauco et al., 2021). Furthermore, they are better positioned to recognize the benefits of new technologies, such as improved convenience, efficiency, and access to healthcare services. Based on this reasoning, the following hypotheses are proposed:
According to TAM (Davis, 1989), the key factors influencing an individual’s intention to use technology are their perception of how easy it is to use (Perceived ease of use: PEOU) and their perception of how valuable it is (Perceived usefulness: PU). When people realize a technology is easy to use, they are more likely to appreciate its benefits. Perceiving a technology as user-friendly increases the likelihood of finding it beneficial, as simplicity of use improves the entire user experience and reduces the effort needed to obtain desired results (Venkatesh & Davis, 2000). Kamal et al. (2020) found that perceived ease of use and perceived usefulness both have a positive impact on the adoption of telemedicine technology in the context of health-related technologies. Therefore, we hypothesize:
As discussed in the literature review, trustworthiness plays a crucial role in the adoption of health-related technologies, particularly in telemedicine where data privacy and reliability are paramount (Shaver, 2022; Yulaikah & Artanti, 2022). Trustworthiness refers to users’ confidence in a system’s secure and consistent performance. In the context of telemedicine, the absence of physical interaction between patients and providers places even greater importance on trust. Building on this foundation, we propose that trustworthiness may moderate the relationships between perceived ease of use (PEOU), perceived usefulness (PU), and telemedicine adoption. When users perceive a telemedicine system as trustworthy, the positive effects of both ease of use and usefulness on adoption intentions are likely to be amplified (Hsiao et al., 2023; Huang, 2021). Accordingly, the following hypotheses are proposed:
The summary of hypotheses is illustrated in Figure 1.
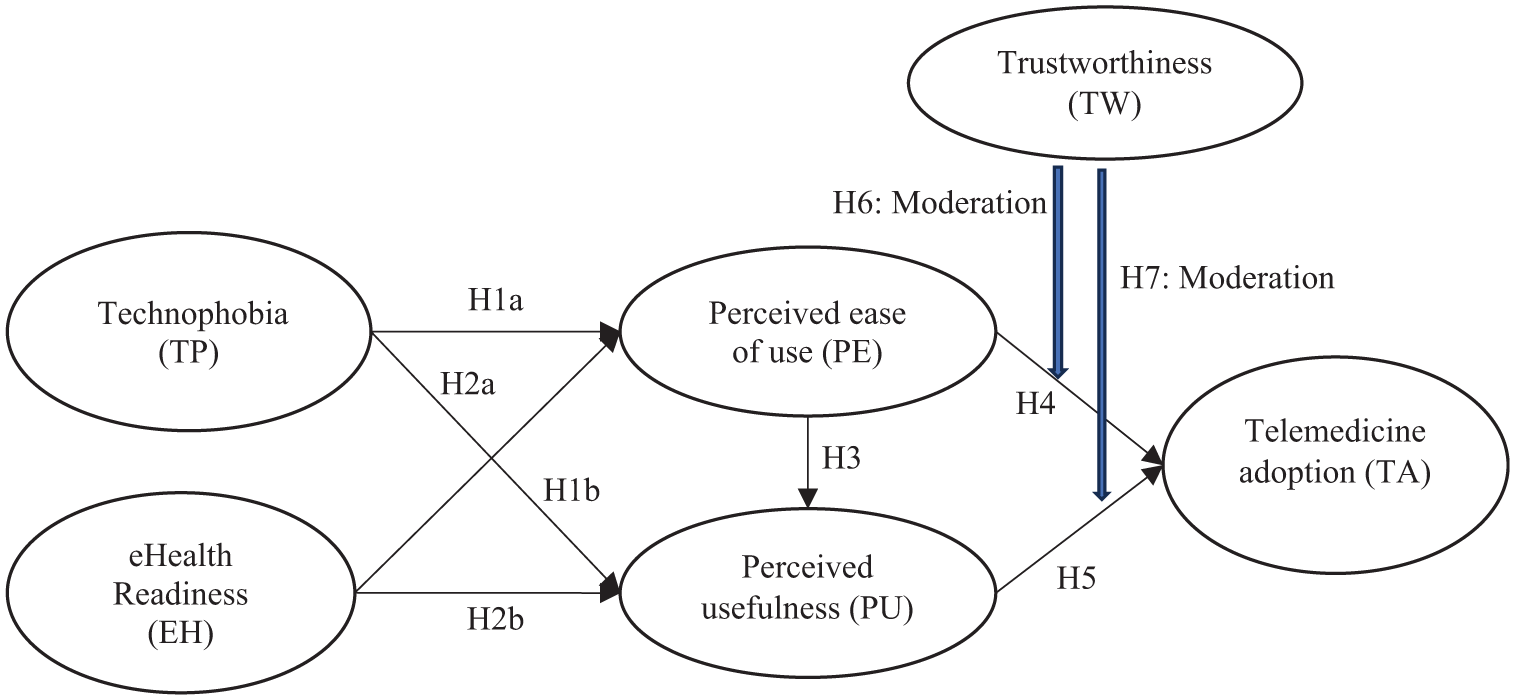
The conceptual framework of this study.
Research Method
To examine the factors influencing telemedicine adoption in emerging markets, this study extends the Technology Acceptance Model (TAM) by incorporating two key psychological and contextual variables: technophobia and eHealth readiness. It also investigates the moderating role of trustworthiness in the relationships between perceived ease of use, perceived usefulness, and the intention to adopt telemedicine. A quantitative research approach was employed to test the proposed model, using a self-administered questionnaire as the research instrument, along with a cover letter outlining the research objectives. To ensure consistent understanding of the term “telemedicine,” participants were provided with a clear working definition before completing the survey. The definition used in the survey was: “Telemedicine refers to the use of digital technology, such as video calls, online messaging, and mobile apps, to provide healthcare services remotely. This includes consultations, diagnoses, and follow-up care that take place without the need for patients and healthcare providers to be physically present in the same location.” This definition was provided to all participants at the beginning of the survey to ensure that their perceptions of telemedicine aligned with the study’s focus.
Participants were recruited through an online self-administered questionnaire platform using non-probability convenience sampling. The questionnaire was disseminated via publicly accessible digital channels in Thailand, including Facebook health-related groups, LINE open chat communities, and university networks. The survey was distributed using Google Forms and SurveyMonkey to ensure accessibility across devices. The recruitment targeted Thai individuals aged 18 to 64 years. Participants were selected based on the following criteria: having access to telemedicine services, a basic familiarity with digital technology, and the ability to understand and complete the questionnaire in Thai or English. Individuals over 65 years of age were excluded due to potential challenges with digital technology and online self-administered surveys. This aimed to minimize cognitive and usability barriers and ensure informed consent and data reliability. Inclusion criteria for participation also required respondents to be Thai citizens capable of understanding and responding to the questionnaire, to ensure demographic variation among Thai respondents with access to digital health services. The survey was distributed to a diverse group, ensuring variability in demographics such as age, gender, education level, and income. Data collection was conducted over a period of approximately 2 months in late 2024. In total, 281 responses were collected. To ensure the sample’s quality and relevance, we applied a screening process to exclude incomplete or invalid responses, ensuring that only participants with prior exposure to digital health services such as using telemedicine apps, online medical consultations, or mobile health platforms were included in the analysis. All participants provided informed consent prior to completing the questionnaire, and anonymity was ensured given that no personal identifying information was collected, which increases the validity of research findings and lessens respondent bias. The study protocol was reviewed and approved by an institutional ethics committee (details withheld for peer review), in accordance with the Declaration of Helsinki. The research design minimized participant risk, and the societal benefits of the findings were judged to outweigh any potential harm.
To develop the measures of six constructs in this study (technophobia, eHealth readiness, trustworthiness, perceived ease of use, perceived usefulness, and telemedicine adoption), the authors adopted the measures from previous studies. A five-point Likert scale, ranging from 1 = strongly disagree to 5 = strongly agree, measures all constructs in this study. Technophobia was measured by five items modified from Sinkovics et al. (2002) and Martínez-Córcoles et al. (2017). eHealth Readiness was measured by six items modified from Bhalla et al. (2016) and Yusif et al. (2017). Trustworthiness was measured by six items modified from M. A. Lee et al. (2022) and Stallings et al. (2022). To evaluate perceived ease of use and perceived usefulness, a seven-item measure is adapted from Akther and Nur (2022). For telemedicine adoption, a three-item measure is modified from Hoonsopon et al. (2025). The detailed constructs and measurement items are shown in Table 1.
The Constructs and Measurement Items of this Study.

Results
Sample Profile
Most of the sample is female (60.5%). Most respondents are aged between 16 and 35 years (57.7%). In terms of education, the largest group holds a bachelor’s degree (48.0%), followed by those with a master’s degree or higher (30.6%). The income distribution shows that most respondents earn between 20,001 and 30,000 Baht per month (33.1%), and the largest group by occupation consists of private sector employees (33.1%). Most respondents use hospital or healthcare services 2 to 3 times a year (47.7%), and the majority spend an average of 1,001 to 3,000 Baht per visit (44.8%). When visiting hospitals or medical facilities, the majority usually go alone (53.0%), followed by those who go with family (34.9%). Table 2 details the sample profile.
Sample Profile.

Hypothesis Testing
To verify the conceptual model of this study and to test the proposed hypotheses, structural equation modeling (SEM) techniques are employed. According to Anderson and Gerbing (1988), a two-step approach consists of a measurement model analysis and a structural model analysis. The authors began to analyze the measurement model to ensure the reliability and validity of the constructs in this study. Then, we test the structural model to evaluate the hypothesized relationships among the variables.
In the first step of a two-step approach, the measurement model analysis, both convergent and discriminant validity, was examined by the confirmatory factor analysis (CFA) to confirm the goodness of fit of the measurement model. Convergent validity exists when item factor loadings exceed 0.7 and item-squared multiple correlations are greater than 0.5 (Awang, 2015). There is discriminant validity when the square root of the AVE for each construct is greater than its model correlations. The authors revised the measurement model based on suggested modification indices, ensuring all factor loadings met the recommended thresholds. The final measurement model demonstrated an acceptable fit to the data (Chi-square = 509.753, df = 304, CMIN/df = 1.677, GFI = 0.880, RMSEA = 0.049, CFI = 0.966, NFI = 0.920). Based on the data shown in Tables 3 and 4, both convergent and discriminant validity are acceptable for the measurement model. Most factor loadings exceed 0.7, with Composite Reliability (CR) values above the 0.7 threshold for all constructs, and AVE values above the recommended 0.5 level for most constructs. The square root of AVE for each construct generally exceeds the squared correlations with other constructs, indicating discriminant validity. Overall, the CFA results suggest that the measurement model is satisfactory for further path analysis.
Measurement Model Results.

Discriminant Validity.
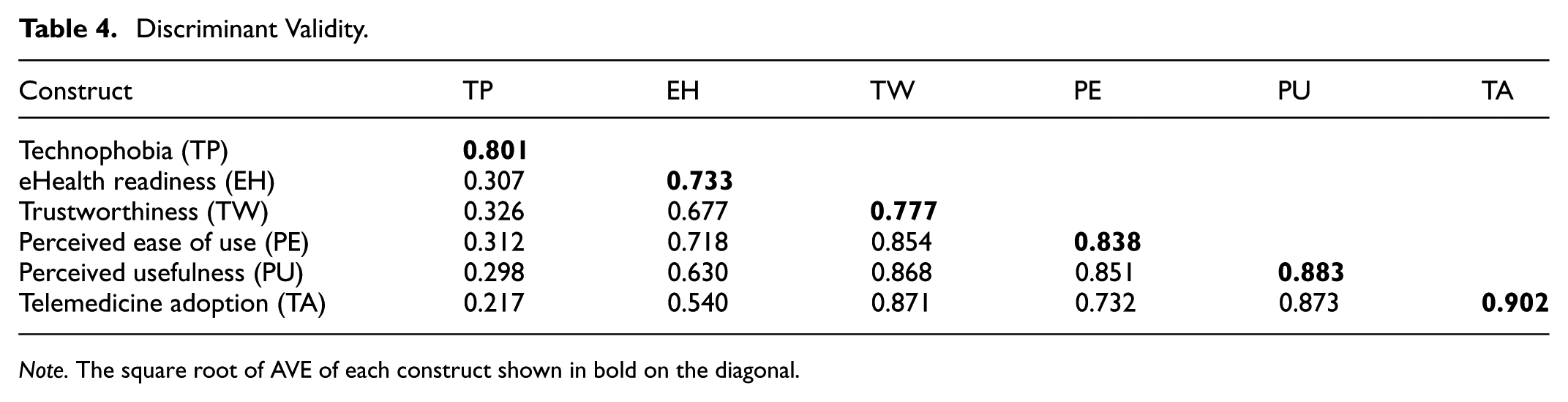
Note. The square root of AVE of each construct shown in bold on the diagonal.
In the second step of a two-step approach, the structural model analysis, the authors examined the proposed hypotheses by considering the path coefficients derived from the analysis. The demographic variables, which are sex, age, education, and income, were included in the model as the control variables to account for their potential influence on the relationships between the main constructs. The results reveal that technophobia shows a significant negative impact on perceived ease of use (b = −0.132, p < .05) but not on perceived usefulness (b = −0.035, p = −.800). Therefore, H1a is supported and H1b is not supported. For H2a and H2b, eHealth readiness significantly positively impacts perceived ease of use (b = 0.755, p < .001) but not on perceived usefulness (b = 0.052, p = .506). Therefore, H2a is supported and H2b is not supported. Perceived ease of use (PE) shows a significant positive impact on perceived usefulness (PU; b = 0.794, p < .001). Therefore, H3 is supported. Considering the path coefficients of PE and PU on telemedicine adoption (TA), PE does not show a significant positive impact on TA (b = −0.158, p = .139). Therefore, H4 is not supported. On the other hand, PU significantly positively impacts TA (b = 0.627, p < .001). Therefore, H5 is supported.
We employed the moderation analysis to examine the moderating roles of trustworthiness (TW) in the relationships between PU, PE, and TA. The authors initially calculate the interaction terms of PU and TW as well as PE and TW by using product mean centering techniques (Aiken & West, 1991). We then incorporated these interaction terms into the structural model to determine if trustworthiness moderates the effects of PU and PE on TA. There is some evidence that trustworthiness (b = 0.121, p = .087) affects the link between perceived ease of use and telemedicine adoption. More trustworthiness makes the positive effect of perceived ease of use on telemedicine adoption stronger, but it doesn’t affect the link between perceived usefulness and telemedicine adoption (b = −0.089, p = .207). Therefore, H6 is supported. H7 is not supported. Figure 2 and Table 5 summarize the results of hypothesis testing.

The path coefficient for all hypotheses of interest in the study.
Hypotheses Testing.

p < .1. ***p < .01.
Discussion
This research endeavors to broaden the scope of the Technology Acceptance Model to gain deeper insights into the acceptance of telemedicine within emerging markets. By incorporating three additional constructs—technophobia, eHealth readiness, and trustworthiness—this study aims to enhance the explanatory capability of TAM. The goal is to provide a more thorough understanding of behavioral intentions in digital healthcare environments, which are often characterized by inconsistent digital infrastructure and diverse levels of digital literacy. This strategy aligns with recent scholarly recommendations to adapt TAM to fit the specific needs of healthcare and culturally distinct settings (Alsyouf et al., 2023; Huong & Long, 2021; Xie et al., 2025).
The findings reveal that technophobia significantly reduces perceived ease of use (PEOU), while its influence on perceived usefulness (PU) is not statistically significant. This partially aligns with earlier studies suggesting that anxiety or fear associated with technology can create cognitive and emotional barriers that diminish perceived usability (Khasawneh, 2015; Kotzé et al., 2016; Nestik et al., 2019). Technophobia has been particularly salient in older adults and less digitally literate populations (Di Giacomo et al., 2019; Steelman & Tislar, 2019). However, its lack of influence on PU in this study may reflect a contextual shift in user priorities, especially during or after the COVID-19 pandemic, where functional necessity may override psychological discomfort (Hsiao et al., 2023; Omboni et al., 2022). In such critical periods, individuals may tolerate usability challenges if the technology offers timely and accessible health services—a notion supported by crisis-driven adoption theory (Clipper, 2020; Elahi et al., 2021). Furthermore, the results indicate that while technophobia may initially hinder user engagement and comfort with telemedicine interfaces, it does not inherently prevent users from recognizing the potential advantages of such platforms. This suggests that perceived usefulness may be more closely related to anticipated health outcomes or convenience than to purely emotional responses (Hsiao et al., 2023; Saigí-Rubió et al., 2022; Zhou et al., 2019).
The analysis confirms that eHealth readiness positively influences PEOU, which is consistent with prior studies emphasizing that digital preparedness enhances technology usability perceptions (Alsyouf et al., 2023; Huong & Long, 2021). Individuals with greater exposure to digital tools, access to ICT infrastructure, and prior training are more likely to find telemedicine systems intuitive and less intimidating (Borges do Nascimento et al., 2023; Rahman et al., 2020). However, the non-significant relationship between eHealth readiness and PU indicates that being digitally ready does not necessarily equate to perceiving the system as clinically effective or beneficial. This gap highlights a broader challenge in eHealth literature: that usability is not always synonymous with perceived value (Kalayou et al., 2020; Kifle et al., 2010; Saigí-Rubió et al., 2022). This finding implies that technical readiness must be complemented with quality assurances, such as clinical validation, certification, and integration with standard care pathways.
Trustworthiness was found to moderate the relationship between PEOU and telemedicine adoption, strengthening the association when trust in the system is high. This finding is consistent with a growing body of research emphasizing the importance of trust in digital healthcare environments, where sensitive health data and remote care raise concerns about privacy, safety, and reliability (Juravle et al., 2020; Touchie et al., 2021; Yulaikah & Artanti, 2022). In line with Ilie and Turel (2020), our results suggest that usability alone is not enough; it must be accompanied by institutional and technological trust for users to move from intention to actual adoption (Van Velsen et al., 2016). Interestingly, the non-significant moderation effect of trust on the PU–adoption relationship suggests that even when users trust the system, their perceptions of usefulness may not be substantially enhanced. This aligns with recent evidence suggesting that PU is driven more by performance expectations and clinical outcomes than by affective factors like trust (Hull et al., 2023; Kalayou et al., 2020). Users are more likely to evaluate usefulness based on whether telemedicine improves access, reduces wait times, or facilitates continuity of care (Harst et al., 2019; Zhu et al., 2023), rather than whether the system is trustworthy per se. Hence, trust may be more critical in influencing usability-related outcomes than outcome-related.
This study makes several important theoretical contributions. First, by integrating technophobia and eHealth readiness, it broadens the applicability of TAM in healthcare contexts and aligns with calls for context-sensitive extensions of the model (Ahadzadeh et al., 2015; Kim & Park, 2012). The inclusion of trustworthiness as a moderator also introduces an interactionist perspective, emphasizing that user perceptions are not static but influenced by systemic and emotional cues. Second, this model contributes to the emerging literature on digital health adoption in low- and middle-income countries, where infrastructural, psychological, and cultural variables differ significantly from those in the Global North (Alsyouf et al., 2023; Gagnon et al., 2012). By contextualizing TAM in Thailand, this study enhances external validity and cross-cultural generalizability.
The findings of this study yield several practical implications for policymakers, healthcare providers, and telemedicine platform developers. First, reducing technophobia should be a strategic priority, particularly among older adults and first-time users. This can be achieved through public awareness campaigns, patient-centered education programs, and empathetic onboarding processes that demystify technology use and promote positive emotional engagement (Schroeder et al., 2023; Yoon et al., 2021). Second, enhancing eHealth readiness requires a concerted effort to build digital literacy through community-based workshops, interactive mobile applications, and health-literate tutorial content, especially targeting rural and underserved populations where infrastructure and awareness may be lacking (Aggarwal et al., 2021; Fernandes & Saragiotto, 2021). Third, fostering trust in telemedicine platforms necessitates the implementation of robust trust-building mechanisms. These include technical measures such as end-to-end encryption, transparent data governance policies, and demonstrable compliance with international medical data standards (e.g., ISO, HIPAA), which are crucial to addressing user concerns about privacy and reliability (Scheibner et al., 2021). Lastly, designers and decision-makers must acknowledge that perceived usefulness is influenced not only by system usability but also by the quality and integration of healthcare services, clinical efficacy, and alignment with patient needs. As such, sustainable adoption will depend on the integration of telemedicine with broader healthcare systems, supported by continuous quality audits, clinical outcome evaluations, and mechanisms for capturing and acting on patient feedback (Ezeamii et al., 2024; Kissi et al., 2020).
Conclusion, Limitations, and Future Research Directions
This study enhances the current understanding of telemedicine adoption by expanding the Technology Acceptance Model through the incorporation of three key constructs: technophobia, eHealth readiness, and trustworthiness. Concentrating on an emerging market context—specifically Thailand—this research responds to an important need to understand the diverse barriers and facilitators of digital health adoption in regions characterized by limited digital literacy, infrastructural limitations, and varied user experiences. The results indicate that technophobia functions as a substantial psychological obstacle that adversely affects perceived ease of use, emphasizing the significance of resolving emotional and cognitive resistance to technology through user-focused design and educational initiatives. Conversely, eHealth readiness appears as a positive facilitator, reinforcing the role of digital literacy and infrastructural preparedness in developing favorable perceptions of telemedicine systems. While both technophobia and eHealth readiness directly impact perceived ease of use, their influence on perceived usefulness seems to be more complex, implying that additional contextual factors—such as the relevance, efficacy, and clinical integration of telemedicine services—may shape user perceptions of value and effectiveness.
Furthermore, this research underscores the moderating influence of trustworthiness, notably in augmenting the correlation between perceived ease of use and the acceptance of telemedicine. Confidence in the dependability of the system, the safeguarding of data, and adherence to ethical norms are particularly vital in healthcare settings, where personal data and virtual interactions are central. Nevertheless, trustworthiness exhibited a diminished impact on perceived usefulness, implying that technological integrity should be coupled with evident clinical advantages to optimize adoption rates. Collectively, these results offer an extensive framework for enhancing strategies for telemedicine implementation in emerging markets. They emphasize the necessity of creating comprehensive digital health approaches that are not only technologically sound but also psychologically appropriate, contextually relevant, and conducive to building trust. By considering both technological aspects and human factors, this study introduces viable practical and theoretical methods to overcome the digital gap and promote fair access to healthcare through telemedicine.
While this study makes notable contributions to understanding telemedicine adoption within emerging markets, it is important to acknowledge several limitations, each suggesting directions for future research. Firstly, the data were collected exclusively from respondents in Thailand. Although Thailand shares characteristics with other emerging economies—such as infrastructural challenges, evolving healthcare systems, and varying levels of digital literacy—cultural norms, governmental policies, and healthcare accessibility vary across countries. Prior research has indicated that cultural dimensions, including uncertainty avoidance, individualism, and power distance, can significantly impact technology acceptance (Metallo et al., 2022; Panicker, 2020). Therefore, caution should be exercised when generalizing these findings to other emerging markets. Future studies are encouraged to employ cross-national comparisons using multi-country samples to better capture cultural and regulatory heterogeneity in telemedicine adoption. Secondly, this study used a self-administered questionnaire distributed online, which may have introduced response biases, including social desirability bias and common method variance (Podsakoff et al., 2003). Respondents may have overestimated their readiness or understated their fears due to the sensitive nature of questions related to technophobia and trust. To address this concern, future research should consider adopting a mixed-methods approach—integrating qualitative interviews or focus groups—to triangulate findings and explore user attitudes in more depth and contextually grounded ways. Thirdly, although this study incorporated technophobia, eHealth readiness, and trustworthiness as key constructs extending the Technology Acceptance Model, the complexity of telemedicine adoption may involve additional psychological, institutional, and structural factors. Variables such as healthcare regulation diversity, data privacy legislation, technological anxiety, previous health system experiences, and perceived risk have been shown in prior literature to shape digital health technology adoption (A. T. Lee et al., 2025; Patel et al., 2022; Yao et al., 2022). Moreover, contextual factors such as digital health infrastructure investment and government incentives can mediate the adoption process (Patel et al., 2022). As such, future research should explore broader frameworks, such as the Unified Theory of Acceptance and Use of Technology or socio-technical systems theory, to provide more nuanced insights. Finally, the current study employs a cross-sectional design, which limits the ability to infer causality or track changes in user perceptions over time. Longitudinal research designs would be useful to observe how telemedicine adoption evolves, especially in response to external shocks or the gradual normalization of digital health services. Examining temporal dynamics could also reveal patterns of resistance, habituation, or attrition that are not visible in static analyses.
Footnotes
Acknowledgements
The authors acknowledge the support of their respective institutions and collaborators for contributing to this research. Special thanks to the survey respondents and research assistants for their invaluable contributions.
Ethical Considerations
The study was reviewed and approved by an institutional ethics committee, in accordance with the ethical standards outlined in the Declaration of Helsinki. All identifying details have been removed in accordance with the journal’s double-anonymized peer review policy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received partial funding from the National Research Council of Thailand (NRCT), Project No. N42A660902.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy restrictions related to participant confidentiality.