
Abstract
There is a lack of research on stigma as a socio-cultural, religious, and moral phenomenon. This study aimed to test a Dynamic Stigma Model of Mental Illness (DYSMO) among a cohort of outpatients. We used structural equation modeling techniques to examine hypothesized relationships within the DYSMO in a cohort of 330 participants. Confirmatory factor analysis produced a model with five latent variables and 17 indicators. All factor loadings were significant at p = .05). Mediation analysis on the full structural model produced standardized fit indices that include the following: (χ2/df = 335.403 (105)), p = .000; RMSEA = 0.08 (90% CI: [0.072, 0.092]; CFI = 0.921; SRMSR = 0.059; TLI = 0.90). Overall, the study revealed that religiocultural, and structural violence perspectives can promote and damage perceptions about mental illness.
Plain language summary
Not only does stigma affect people with mental illness (PWMI), but also their family relatives, and all who care for them. There have been many studies on stigma over the years. However, researchers have a gap in studying the stigma of mental illness as a sociocultural, religious, and moral phenomenon. The purpose of this study was to test a model named the “Dynamic Stigma Model (DYSMO)” among a convenience sample of 330 persons receiving care in Ghana. The cross-sectional study examined relationships within the newly developed stigma model using statistical analysis techniques. The analysis found that religious and cultural beliefs positively influenced extreme social injustice, otherwise known as structural violence towards PWMI. The study also revealed that existing religious and cultural belief systems influenced how much a person appraised stigma as positive or negative. The study further found that stigma perceptions of PWMI influenced their anticipation of discrimination and subsequent social withdrawal, especially when in public places. Overall, the study revealed that factors such as religious, cultural, and structural violence can promote and damage perceptions about individuals with mental health problems. All stakeholders, including mental health practitioners, policymakers, and community members, must gain increased awareness and knowledge of the role religious and cultural beliefs play in the perpetuation and outcomes of mental illness stigma.
Background
Despite the mounting burden of mental health problems and the substantial distress for individuals and the public, society appears to make minimal effort to address the issues due to widespread stigma (Hoftman, 2017). Stigma is characterized by unfavorable attitudes and behaviors that prevent certain people from social acceptance and participation in communal activities (Goffman, 1963). According to Dudley (2000), the negative stereotypes that society ascribes to certain persons make them feel different and inferior to other members of society. The Dynamic Stigma Theory (Gyamfi, 2024, p. 7) posits that six (6) major factors impact individual stigma perceptions and subsequent appraisal. The theory postulates that (1) public stigma leads to sustained self (internalizing) attitudes and behaviors among PWMI, (2) public stigma directed at PWMI constitutes a “violence” and “infringement” on human rights that is likely to affect the family and professional caregivers alike, and who may potentially displace the threat of perceived stigma onto the PWMI. (3) religiocultural belief systems, structural violence perspectives, and stigma attitudes and behaviors are learned and socially transferred onto the offspring over time. Therefore, they can be unlearned if society wants to. (4) there is an existing stigma cycle (known as the stigma web) that is underpinned by invisible power differentials that force close friends, relatives, intimate partners, and formal and informal caregivers to displace public stigmatizing attitudes onto the individual with a mental health problem, prompting the stigmatized person to initiate reactive coping mechanisms. The reactive coping mechanisms that the stigmatized individual initiates create a whirlpool of negative events termed stigma whirlpool, that sink the individual further down the social ladder, leading to stagnation, termed stigma battle fatigue, and resulting in further perpetuation of stigmatizing tags toward the PWMI, which ultimately affect care outcomes and life chances. (5) the concept of “stigma” is dynamic; therefore, stigma processes may evolve. (6) Stigma stress perception appraisal is associated with rejection and injustice sensitivity and leads to sustained internalization of stigma processes with increased anticipation of discrimination within the social space, leading to reactive coping mechanisms (for survival).
Religiocultural beliefs about mental illness promote negative public perceptions and attitudes of stigma toward people with mental illness (PWMI) (Caplan, 2019; Wesselman & Graziano, 2010). These beliefs attached to mental illnesses (if predominantly negative) lead to the stigma that adversely impacts the availability of appropriate social support systems for PWMI (Wesselmann et al., 2015). “Religiocultural beliefs” constitute complex social phenomena that create and sustain traditional systems of values, morals, and sacred practices that uphold peculiar perceptions, attitudes, and behaviors of a people towards one another through governance and other established social organizations” (Gyamfi, 2024, p. 7). Religiocultural perspectives constitute aspects of the moral paradigm of society that works against PWMI and seeks to preserve and justify existing social disparities. According to Vygotsky (1987 [1934]), the acquisition of attitudes and behaviors happens within social processes immersed in society’s culture and socio-religious practices. Vygotsky’s sociocultural theory supports the view that religion and culture influence and modify society’s perceptions and attitudes, including extreme social marginalization or structural violence.
Galtung (1969) named and described structural violence as psychological violence associated with indirect acts constraining human societal actions. In this study, “structural violence” has been defined as the effect of historically rooted power differences (visible or invisible) embedded in religious, cultural, and political systems that enable the justify public stigmatizing behaviors toward marginalized persons, skewing their life chances and denying them of existing social services (including employment, access to education, and health services) in favor of persons regarded as “superior” in society.
Society regards PWMI as inferior (Ahmedani, 2011; Barke et al., 2011). For this reason, contemporary researchers should discuss stigma from the perspective of structural violence.
Even though Galtung describes structural violence as largely silent, invisible, and somewhat inherent in the social structure, Chopra (2014) identifies factors such as recognizable institutions, existing ideologies, relationships, discriminatory laws, classism, gender inequality, and racism as being among the forces that shape structural violence in the social order. Chopra (2014) further argues that even though social power affects everyone within a social structure, those at the bottom end, for example, PWMIs suffer most in terms of disease, death, unemployment, lack of education, homelessness, inaccessibility to healthcare, and poverty. One is likely to trace the marginalizing power of social institutions to ideological inclinations that promulgate discriminatory laws with a direct or indirect constraining effect on the abilities of marginalized groups such as PWMI in society (Cogburn, 2019; Gyamfi, 2022, 2024; Gyamfi, Forchuk, & Luginaah, 2024). Therefore, the consequence of structural violence could embody social suffering and accompanying inequality, an oppressive regime associated with unending pain in the psyche of PWMI.
Structural violence negatively impacts PWMI as it empowers existing social influences to legitimize and justify social inequalities and other disparities in the social order. According to Galtung (1990), cultural influences legitimize social inequity leading to structural and cultural violence.
Stigma is an outcome of historically rooted negative societal attitudes and behaviors that come in the form of discriminatory acts embedded in religiocultural and structural violence perspectives (Gyamfi, 2024). Stigma is a response to stress and esteem-related appraisal of experienced, anticipated, perceived, or personal endorsement of societal actions due to existing power relational differences. These stigma outcomes may be characterized by labeling (tagging), stereotyping behaviors (attribution and categorization based on tags), prejudice (negative cognitive and emotional evaluative attitudes), separation and status loss, and social exclusion (setting one aside from social events/activities) (Gyamfi, 2022, 2024).
Mental illness-related stigma exists in various forms including (1) public stigma (society’s endorsement of mental illness stereotypes and prejudices), (2) self-stigma (product of internalized public stereotypes and prejudices), (3) stigma by association (public labeling and stereotyping due to one’s close relationship with a stigmatized person), (4) structural stigma (the product of discriminatory policies from both private and governmental institutions that restrict the opportunities or options for PWMI) and (5) family-orchestrated (familial) stigma (the labeling, and stereotyping from client’s own family). Over the years, researchers have put forward various theoretical approaches to addressing stigma, including Goffman (1963), Link (1987), Link and Phelan (2001), Corrigan (1998, 2000), and Major and O’Brien (2005). Yet stigma issues continue unabated.
The identity threat model of stigma (Major & O’Brien, 2005) posits that perceived public attitudes (discrimination) and personal factors determine the extent to which people with mental illness perceive and appraise stigma as stressful, independent of diagnosis and clinical symptoms (Rüsch, Corrigan, Powell, et al., 2009; Rüsch, Corrigan, Wassel et al., 2009). Appraisal is a subjective yet cognitive process that stigmatized persons encounter daily. According to Lazarus and Folkman, a cognitive appraisal comprises the “process of categorizing an encounter and its various facets, with respect to its significance for wellbeing” (Lazarus & Folkman, 1984, p. 31). When one encounters a potentially stigmatizing situation, he or she appraises the situation in two ways. First by using primary appraisal mechanisms where the individual assesses the situation, ascertains the enormity of the problem, and concludes as to whether the situation is (1) a threat, likely to affect the self-esteem and well-being negatively, (2) a loss; damage that has occurred already, or (3) a challenge; which can offer an opportunity for growth (Lazarus & Folkman, 1984; Major & O’Brien, 2005). Second, after the individual evaluates the situation, they then initiate a secondary appraisal to determine whether they have the resources (such as social networks, family and close friends, knowledge, health, energy, financial resources, or self-esteem) to deal with the problem at hand (Lazarus & Folkman, 1984; Major & O’Brien, 2005). The lack of appropriate resources for dealing with social difficulties may lead PWMI to experience stress, low self-esteem, or diminished well-being. However, it appears that no two stigmatized persons experience, perceive, or appraise stigma the same way due to individual and cultural differences (Bracke et al., 2019; Gopalkrishnan, 2018).
Established literature shows that anticipated discrimination stops people from applying for employment, training, or education or making close relationships (Ucok et al., 2012). Anticipated discrimination is a coping strategy and differs from experienced discrimination (Gabbidon et al., 2013). For instance, while experienced discrimination usually acts as a precursor to internalized stigma (Asrat et al., 2018), internalized stigma appraisal leads to rejection concerns and future anticipated discrimination outcomes (Rivera et al., 2021; Schauman et al., 2019) that can lead to coping strategies (adaptive or maladaptive) including social withdrawal and self-esteem challenges (Gyamfi, 2024). So far, a recent scoping review of the literature by Gyamfi, Forchuk, Booth, and Luginaah (2024) revealed that no stigma model (both globally and in Ghana) had examined the influences of religiocultural beliefs and structural violence in predicting patient stigma perception appraisal and outcomes. Therefore, we tested a theoretical stigma model (the Dynamic Stigma Model) that explains and establishes mental illness stigma as a violence-related phenomenon that originates from the public.
Key concepts of the Dynamic Stigma Model as conceptualized and defined by Gyamfi (2024, p. 7) are as follows: (1) Religiocultural beliefs are the complex social phenomena that create and sustain traditional systems of values, morals, and sacred practices that uphold peculiar perceptions, attitudes, and behaviors of a people toward one another through governance and other established social organizations. (2) Structural violence is the effect of historically rooted power differences (visible or invisible) embedded in religious, cultural, and political systems that enable and justify public stigmatizing behaviors toward marginalized persons, skewing their life chances and denying them of existing social services (including employment, access to education, and health services) in favor of persons regarded as “superior” in society. (3) Stigma is the product of historically rooted public attitudes and behaviors (i.e., religiocultural and structural violence perspectives) that characterize labeling, stereotyping, prejudice, cognitive separation, status loss, and discrimination that lead to responses of stress and esteem-related appraisal of experienced, anticipated, perceived or personal endorsement of societal actions due to existing power relational differences. (4) Stigma perception appraisal involves experiencing, identifying, paying attention to, evaluating, and interpreting information from one’s environment based on available resources, emotions, and the meaning of the experiences to the individual. (5) Coping mechanisms involve conscious and unconscious strategies or processes to adjust or tolerate internal and external stressful situations that may be positive or negative, which the individual undertakes after appraising a situation as threatening their self-image, well-being, or survival. Below (Figure 1) is the proposed stigma model of mental illness that was tested among a population of Out-patients in Ghana using structural equation modeling techniques.
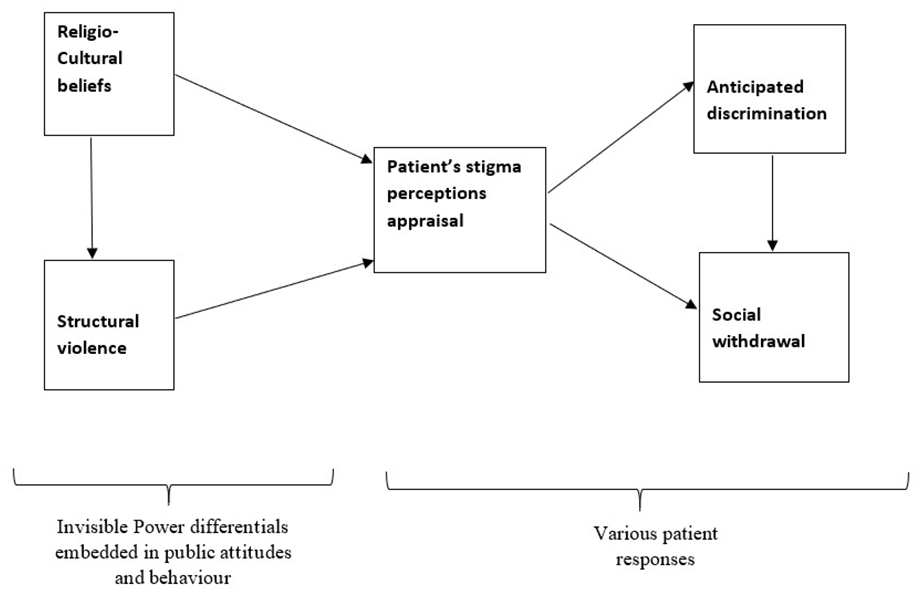
The proposed dynamic stigma model of mental illness.
Study Hypotheses
The study tested the following hypotheses to ascertain whether:
(1) Religiocultural beliefs about PWMI have a significant relationship with societal structural violence behaviors towards PWMI.
(2) Religiocultural beliefs have a relationship with stigma perception appraisal among PWMI.
(3) Structural violence is positively related to stigma perception appraisal among PWMI.
(4a)Stigma perception appraisal is positively related to anticipated discrimination and social withdrawal behavior among PWMI.
(4b)Stigma perception appraisal is positively related to social withdrawal behavior among PWMI.
(5) Religiocultural beliefs are positively related to anticipated discrimination among PWMI.
(6) Structural violence is positively related to social withdrawal behavior of PWMI.
(7) Anticipated discrimination positively relates to social withdrawal behavior of PWMI (see Figure 2 below for details).

Hypothesized regression paths of the dynamic stigma model.
Figure 2 shows regression relationships (paths) between religiocultural beliefs, structural violence, stigma stress perception appraisal, anticipated discrimination, and social withdrawal. Note that H1 expresses the regression effect of Religiocultural beliefs (RCB) on Structural violence (SV); H2 defines the regression effect of RCB on Stigma Perception Appraisal (SPA); H3 denotes the regression effect of SV on SPA; H4 signifies the mediation effect of SPA on Anticipated discrimination (AD) and social withdrawal (SW); While H5 and H6 represent direct effects of RCB and SV on AD and SW respectively, H7 signifies a direct regression effect of AD on SW.
Methods
Design of the Study
This study was a cross-sectional design that examined predictors of mental illness stigma perceptions appraisal among participants by testing hypothesized relationships within a dynamic stigma model developed by the scientist. Using a cross-sectional design enabled the first author to test relationships among many variables in a large population within a limited time frame (one-point data collection) and with a reasonably inexpensive budget (Munnangi & Boktor, 2021; Setia, 2016).
Research Setting
The study was conducted in two public Psychiatric Hospitals in Southern Ghana. Ghana is a Low-Middle Income Country located in West Africa, along the Gulf of Guinea and the Atlantic Ocean, with a total land area of about 239,000 square km. There are three Psychiatric Hospitals, all situated in the Southern part of the country (along the coast). Two of these hospitals are in Accra, the capital city and the other is in the Central Region of Ghana (about 100 miles away from the capital). The total bed capacity of the three hospitals amounts to about 1,500 (average, 5.5 beds per 100,000 population). Despite the few beds available, each hospital can admit up to about 1,200 patients (Jack et al., 2013). In Ghana, psychiatrists and psychiatric nurses offer mental health care, including clinical mental health officers, psychologists, community psychiatric nurses, community psychiatric officers, social workers, occupational therapists, and health assistants.
Sampling
Target Population
For this study, the target population was outpatients in two psychiatric hospitals in Southern Ghana (namely, the Ankaful Hospital and Pantang Hospital). Outpatients are mostly individuals who live in the community, have recovered from severe symptoms of mental illness, and are seeking ongoing reviews and further treatment (rehabilitation) at the Outpatient Department (OPD).
Inclusion Criteria
To be part of the study, individuals were expected to be out-patients aged 18 years and above who could articulate their perceptions and experiences in English. Participants with stable mental health status who offered informed consent were recruited for the study.
Exclusion Criteria
Outpatients experiencing an exacerbation of their underlying mental illness (relapsed) were not involved in the study.
Sampling Method
Non-probabilistic convenience sampling technique was used to recruit participants for the study at the OPD of the two psychiatric hospitals. The research team collaborated with the health care providers at the OPD in the study settings to recruit participants. Individuals were included in the study after they had clearly understood the content of the information sheet and consented to it. While there is no agreed-upon method to calculate sample size for the SEM analysis in the literature, researchers have suggested the minimum sample size required for SEM statistical analyses should be a minimum of 200 participants (Kline, 2015). While authorities such as Nunnally (1994) propose 10 cases per variable, Schumacker and Lomax (2016) suggest a rule of thumb of 20:1 (i.e., 20 participants per indicator or parameter) as convenient. The current study’s hybrid model had five factors and 22 known indicators. Therefore, in this study, in order not to overly sample participants, a 15:1 principle was applied to achieve an adequate sample size of 330 participants. This helped to nullify the possible impact of outliers on statistical power. In all, 330 participants were recruited for the study. To achieve the set sample size, the two hospitals were weighted equally because each has a bed capacity of about 500. Therefore, an average of 165 PWMI were recruited from each hospital, resulting in a sample of n = 330 participants.
Data Collection
Primary data were collected from the recruited outpatients once, using questionnaires administered by the first author and trained research assistants (RAs). The research team first collected socio-demographic data and followed with the questionnaires in other sections. The data collection process for each participant took about 90 min.
Instruments
Demographic Questionnaire
The demographic questionnaire comprised open and close-ended items. Open-ended questions in the demographic data were subsequently categorized, and each was given an appropriate code before they were entered into SPSS for analysis.
Regarding the main research tools, we gathered data using close-ended structured questionnaires in Likert scale format to elicit appropriate and situation-specific answers from the participants. These instruments include the Morality/Sin (MS) Scale, Blame/Unfairness Scale, Alienation Scale, Questionnaire on Anticipated Discrimination, and the Social Withdrawal Scale.
The Morality/Sin (MS) Scale
The current study used the 9-item MS scale of the Religious Beliefs about Mental Illness (RBAMI) instrument. Wesselman and Graziano (2010) to measure perceptions of PWMI about the extent to which society applies belief systems in explaining mental illness. The MS items include the following: “Moral weakness is the main cause of mental illness,”“People suffering from mental illnesses are not going to their places of worship enough,”“Mental illnesses result from an immoral or sinful lifestyle,”“People suffer from mental illnesses because they are not sorry for their sins,”“A person suffering from a mental illness is not relying on their faith or religious values like they should,”“A person suffering from a mental illness is not praying enough,”“People have mental illnesses because someone else sinned against them,”“Mental illnesses are a result of Original Sin,”“A person’s relationship with God has nothing to do with their suffering from a mental illness.” In the present study, the scale had a good internal consistency (α = .86).
The Blame/Unfairness Scale
We used the blame/unfairness scale of the Injustice Experience Questionnaire (IEQ) (Sullivan, 2008) to measure the structural violence perspectives of participants. Ranging from 0 = never, 1 = rarely, 2 = sometimes, 3 = often, and 4 = all the time. The scale items include the following: “I am suffering because of someone else’s negligence,”“It all seems so unfair,”“Nothing will ever make up for all that I have gone through,”“I feel as if I have been robbed of something very precious,”“I am troubled by fears that I may never achieve my dreams,”“I can’t believe this has happened to me.” In the current study, the blame/unfairness scale was reliable (α = .81).
The Alienation Scale
We used the Alienation sub-scale of the Internalized Stigma of Mental Illness Scale (ISMI) (Ritsher et al., 2003) to measure participants’ subjective experiences of feeling different from other members of society due to their mental health problems. The alienation scale consists of 6 items, rated on a 4-point, Likert-type scale ranging from 1 (strongly disagree) to 4 (strongly agree). The scale items comprise the following: “I feel out of place in the world because I have a mental illness”; “Having a mental illness has spoiled my life”; “People without mental illness could not possibly understand me”; “I am embarrassed or ashamed that I have a mental illness”; “I am disappointed in myself for having a mental illness” and “I feel inferior to others who don’t have a mental illness.” Higher total mean scores indicate strong feelings of alienation. In the current study, the scale’s reliability was very good (α = .92).
The Anticipated Discrimination in Interpersonal/Professional Relationships Scale (ADIPR) (Gabbidon et al., 2013) is part of the Questionnaire on Anticipated Discrimination (QUAD). It assesses the extent to which people with mental health problems anticipate discrimination across various social contexts based on how they appraised perceived stigma. The ADIPR is a 4-point 6-item Likert scale that ranges from 0 (strongly disagree) to 3 (strongly agree). The scale items consist of the following: “If a person I want to date or have an intimate relationship with knows I have a mental health problem, they will treat me unfairly,”“If people in my neighborhood know I have a mental health problem they will treat me unfairly,”“If children and teenagers in the community know about my mental health problem they will treat me unfairly,”“If work colleagues know I have a mental health problem they will treat me unfairly,”“If friends know about my mental health problem they will treat me unfairly,”“If my family knows about my mental health problem they will treat me unfairly.” The scale had a good reliability of (α = .66).
The Social Withdrawal Scale
The Social Withdrawal Scale (Ritsher et al., 2003) is a 4-point Likert scale that ranges from 1 (strongly disagree) to 4 (strongly agree). The scale includes six items and measures the situation where a person avoids social or public interactions as a response to the public’s actual or expected negative behavior. The scale consists of the following items: “I don’t talk about myself much because I don’t want to burden others with my mental illness,”“I don’t socialize as much as I used to because my mental illness might make me look or behave ‘weird’,”“Negative stereotypes about mental illness keep me isolated from the normal world,”“I stay away from situations in order to protect my family or friends from embarrassment,”“Being around people who don’t have a mental illness makes me feel out of place or inadequate,”“I avoid getting too close to people who don’t have a mental illness to avoid rejection.” Higher scores on the social withdrawal scale meant high social withdrawal behavior by participants. In this study, the internal consistency of the social withdrawal scale was good (α = .90).
Operationalization (Adaptation) of Instruments
(The instruments were used to assess the study variables in the following ways: (1) The morality/sin scale of the RBAMI was used to measure Religiocultural beliefs (RCB). (2) The blame/unfairness scale of the IEQ was used to measure the participants’ structural violence (SV) perspectives. (3) The Alienation scale of the ISMI was used to measure participants’ stigma perceptions appraisal (SPA). (4) The anticipated discrimination in interpersonal/professional relationships scale of the QUAD was used to measure the anticipated discrimination of participants, and (5) The Social withdrawal scale of the Internalized Stigma of Mental Illness Inventory (ISMI) was used to measure social withdrawal behavior of the participants. Areas of the scales that were not likely to suit the cultural context of the participants in Ghana were modified (reworded). For instance, “If a person I want to date or have an intimate relationship with knows I have a mental health problem, they will treat me unfairly” was reworded to read, “If a person I want to date or marry knows I have a mental health problem they will treat me unfairly.” The first author computed the mean responses in each instance (every subscale) and measured the internal consistency of all scales to ascertain the reliability of the scales across culturally distinct settings and populations. Any adapted scales were assessed by the first author’s committee of experts (already involved in research at the highest level) to ascertain their suitability in the Ghanaian context.
Data Analysis
Structural equation modeling
Data Preparation and Screening
To ensure the quality of data, the first author checked for completeness by randomly sampling from the data set to check for response sets against the scales for obvious patterns of responses. The first author also checked for missing values or pages and the consistency and accuracy of responses by conducting logical checks with the demographic data and range checks with the Likert response categories as provided in the questionnaire. Open-ended questions in the demographic data were categorized, and each was given an appropriate code before they were entered into SPSS for analysis. All missing values were given a code of −99 to account for them during analysis. One of the RAs entered data, after which the principal investigator validated and cleaned the data separately. This helped to reduce any errors. In this study, statistical analyses were done using two statistical packages: the Statistical Package for the Social Sciences (SPSS v.28.0, IBM Corp., 2021) for descriptive analysis, while inferential analyses related to the structural regression model were performed using Mplus 8.5 (Muthén & Muthén, 2020).
Confirmatory Factor Analysis and Model Estimation
Model estimation involves determining the value of the unknown parameters and the error associated with the estimated value using SEM software programs. Confirmatory factor analysis (CFA) can estimate latent variables (Byrne, 2013; Kline, 2015) based on correlated variations of a dataset in terms of associations (relationships) and can reduce data dimensions, standardize a scale with multiple indicators, and as well account for correlations inherent in a dataset (Byrne, 2013). Therefore, CFA techniques were used to analyze and determine the model structure of the hypothesized relationships between religiocultural beliefs, structural violence, stigma, stigma perceptions appraisal, anticipated discrimination, and social withdrawal. The CFA process was completed in two steps. Firstly, we focused on the measurement of the latent variables and their observed variables (indicators), and secondly, followed with an investigation of the structural model, which is essentially a set of regression hypotheses between the latent variables.
Determining Model Fit and Interpretation
In this study, model fit was determined using chi-square (χ2), Comparative Fit Index (CFI), Root Mean Square Error of Approximation (RMSEA), Standardized Root Mean Square Residual (SRMR), and Tucker–Lewis Index (TLI). Each modification was done stepwise (i.e., one modification at a time), guided by predicted post Hoc improvement indices in the Mplus output. Having achieved fit for the measurement model, the model was converted to include hypothesized pathways to measure the relationships between religiocultural beliefs, structural violence, stigma stress perception appraisal, anticipated discrimination, and social withdrawal.
Results
This study aimed to test a hypothesized Model of the Dynamic Stigma Model of Mental Illness (DYSMO) among 330 Outpatients in Ghana. Statistical analyses were done using two statistical packages (SPSS v.26.0 for descriptive analysis, while inferential analyses related to the structural regression model were performed using Mplus software.
Participant Characteristics
Means, standard deviations, skewness, and kurtosis values were calculated to determine the general characteristics of the study participants. Descriptive statistics of variables are presented in Tables 1 and 2.
Sociodemographic Characteristics of Study Participants.

Descriptive Statistics of Observed Variables.

Note. RBAMI = religious beliefs about mental illness; IEQ = injustice experience questionnaire; ISMI = internalized stigma of mental illness scale; QUAD = questionnaire on anticipated discrimination.
In this study, all participants (n = 330, 100%) reported their demographic characteristics, with most being Christian (270, 81.8%) and with a mean age of 37.11 years (SD = 10.9). Most participants were male (n = 185, 56.1%). Regarding marital status, most participants were unmarried (n = 244, 74%). In terms of living situation, most (276, n = 83.6%) lived with someone (i.e., friends, family, or partner). About 154 (46.7%) were employed in either government, self, or private employment, while 132 (40%) were unemployed. All participants had some form of formal education, with about 266 (80.6%) having secondary or tertiary educational backgrounds. Out of the 196 (59.4%) who expressed knowledge of their illness, most had schizophrenia (91, 46.4%), followed by substance use disorder (57, 29.1%), mood disorders, that is, depression, and bipolar (43, 22%). The rest of the diagnoses included post-traumatic stress disorder (3, 1.5%), Epilepsy (1, 0.5%), and dementia (1, 0.5%). Most participants, 138 (70.4%), who expressed knowledge of their illness agreed with their current diagnosis. The average treatment duration of participants’ illness was 6.94 years (SD = 3.0). Details of the participant demographic characteristics are reported in Table 1.
Descriptive Statistics of Observed Variables
Means, standard deviations, skewness, and kurtosis values were calculated to determine the general characteristics of the variables and to assist in assessing the assumptions of the structural regression model for possible redress should there be any form of unfavorable skewness or kurtosis, as skewness may affect regression coefficients associated with the model (Malehi et al., 2015). Descriptive statistics of the variables are presented in Table 2 below.
Assessing Assumptions of the Structural Regression Model
The output from the descriptive statistical analysis was used to assess if data was normally distributed by assessing skewness (the degree to which a variable distribution was asymmetrical (i.e., Sk > 0 if positively skewed, and Sk < 0 if negatively skewed) and kurtosis (measure of the peakedness of the distribution). Establishing normality helped to ascertain whether the sample recruited for the study represented the outpatients being studied. In the event of data skewness or kurtosis, the first author fixed it by performing a square root transformation of the data (this helped to reduce skewness to acceptable levels). The investigator also determined if there was any form of multicollinearity between the variables by performing a correlation analysis. Before the initial correlational analysis, we proposed removing all items that (1) had coefficients above .8. (2) items that had coefficients below .3 will also be removed. (3) items that correlated strongly with other items that belonged to different instruments or scales would be removed. We took this decision because we believe multicollinearity could affect the precision of the estimated regression coefficients and the model fit. After performing correlational analysis on all items, the following items were removed before performing CFA: ISMI2, ISMI3, ISMI4, and ISMI24 were removed due to high correlations with their items. However, RBM1, RBM2, RBM7, RBM9, IEQ11, IEQ12, QUAD13, and QUAD14 were removed due to low correlation with own items. Again, IEQ9 and QUAD9, which had high correlations with the ISMI items, were removed. See Table 3 for a detailed correlation matrix of items used in the initial CFA of the DYSMO.
Correlation Matrix of Observed Variables Used in the Model.

All missing values were assigned a value of −99 and were handled within the analysis model using Full Information Maximum Likelihood (FIML) as a default in Mplus. Since this was the first time most of the instruments were used among a culturally different sample, EFA was performed to ascertain the factor structure of these instruments. The EFA revealed that most of the instruments retained their original structure. Therefore, they were used in their original form in the CFA of the DYSMO. See Table 3 below for details.
Testing the Psychometric Properties of the Original Hypothesized (Measurement) Model
To test the hypothesized model, a confirmatory factor analysis (CFA) was performed on the first model, which had five latent variables (RCB, SV, SPA, AD, and SW) that contained 19 indicators in total, with subsequent model modification to assess the best fit.
Covariances between the five latent variables ranged from −0.02 to 0.63, indicating that they were all separate and independent constructs.
The standardized factor loadings of the original model include RCB by RBM1 (0.732), RBM2 (0.786), RBM3 (0.824), RBM4 (0.818), RBM5 (0.825), RBM6 (0.812), and RBM8 (0.617). SV by IEQ7 (0.838), IEQ8 (0.739), IEQ10 (0.669). SPA by ISMI1 (0.650), ISMI5 (0.906), and ISMI6 (0.735). AD by QUAD10 (0.684), QUAD11 (0.759), and QUAD12 (0.685). SW by ISMI19 (0.774), ISMI20 (0.768), ISMI21 (0.814), ISMI22 (0.851), and ISMI23 (0.643). All standardized factor loadings were statistically significant (different from 0.00) at p = .000. Results of the original model include: (χ2/df = 926.621 (220)), p ≤ .000; RMSEA = 0.099 (90% CI: [0.092, 0.105]; CFI = 0.838; SRMSR = 0.074; TLI = 0.814). The fit indices of the original model show that none of the statistics for the model provided sufficient indices for a well-fit model, indicating that model fit was not achieved (see Table 4 below). Therefore, a revision was made to improve and get a better fit.
Summary of the Model Fitness Indices of the Original Hypothesized Model and Modifications.

Note. p ≤ .05; χ2 values are based on Maximum likelihood in Mplus.
Modifying the Hypothesized Model
The RBM8 indicator was removed from the RCB factor to modify the model. Deleting led to significant improvement in fit indices, with the Chi-Square value dropping (from 926.621 to 810.917). Despite improvement in fit indices, the model fit was not satisfactory. A second modification was therefore conducted by correlating the residuals of IEQ8 with IEQ7. This modification also reduced the χ2 value marginally and improved the CFI (from 0.838 to 0.858). A third model modification was performed by removing ISMI23 from the SW variable. The ensuing fit indices showed further improvement in model fitness (i.e., χ2 = 692.421, CFI = 0.868) yet warranted additional modification. A fourth modification was done by allowing the ISMI20 and ISMI19 residuals to correlate. This modification improved the indices further (χ2 = 540.685, CFI = 0.885). Despite achieving a satisfactory SRMR of 0.064, there was a need for further modification to achieve an improved fit. A fifth modification allowed the residuals of ISMI21 and ISMI20 to correlate with a resultant CFI = 0.890.
Final Fit Indices, Factor Structure, and Standardized Parameter Estimates of the Measurement Model
With a CFI = 0.90 (when rounded), one could argue that, at this point, the model fits the data. Despite this significant improvement in the model indices, a sixth modification was performed by correlating residuals of RBM5 with RBM6. The standardized factor loadings of the final measurement model were significant at p ≤ .000 and ranged from moderate to high. These include: RCB by RBM3 (0.87), RBM4 (0.88), RBM5 (0.75), and RBM6 (0.73). SV by IEQ7 (0.65), IEQ8 (0.58), and IEQ10 (0.81). SPA by ISMI1 (0.65), ISMI5 (0.91), and ISMI6 (0.73). AD by QUAD10 (0.68), QUAD11 (0.77), and QUAD12 (0.68). SW by ISMI19 (0.73), ISMI20 (0.67), ISMI21 (0.82), and ISMI22 (0.89). The final model had five latent variables with 17 indicators in total. Covariances between the latent variables ranged from 0.06 to 0.65, indicating that all five latent variables (i.e., RCB, SV, SPA, AD, and SW) were all separate and independent constructs.
While some standard factor covariances were significant (SV with RCB = 0.46, p ≤ .000; SPA with RCB = 0.14, p ≤ .025; SPA with SV = 0.61, p ≤ .000; SW with SPA = 0.21, p ≤ .001; AD with SV = 0.16, p ≤ .041; AD with SPA = 0.37, p ≤ .000; AD with SW = 0.65, p ≤ .000), others such as (SW with RCB = 0.08, p ≤ .211; SW with SV = 0.11, p ≤ .111; AD with RCB = 0.06, p ≤ .397) were not significant (see Figure 3 below for details).

Factor structure of the final DYSMO with standardized loadings.
The resulting final (sixth) model fit indices were as follows: (χ2/df = 335.403 (105)) p = .000; RMSEA = 0.080 (90% CI: [0.072, 0.092]; CFI = 0.921; SRMSR = 0.059; TLI = 0.897). At this point, all the fit indices had met the standard thresholds for a good model fit. Therefore, no further modifications were made (see Table 4 below for details). The model fit indices of the original and revised models of the DYSMO are also presented in Table 4 below.
The Full Structural Regression Model and Mediation Analyses
The current study examined the relationships between religiocultural beliefs (perceptions), structural violence perspectives, stigma perceptions appraisal, and related outcomes of anticipated discrimination and social withdrawal among people with mental illness in two public Mental Health Hospitals in Ghana.
Having established the psychometric properties and model fit for the measurement part of the DYSMO, a mediation analysis was performed to test hypothesized relationships of the latent constructs (i.e., between the predictors; RCB, SV, and outcomes AD and SW through SPA) of the full structural model using the Maximum Likelihood default and bootstrap (10,000) resampling technique to correct for possible bias and to calculate the confidence intervals of all coefficients, including mediated/indirect effects. Fit indices of the full model indicated that the data fits the model. The standardized values of the full model include the following: (χ2/df = 335.403 (105)), p ≤ .000; RMSEA = 0.08 (90% CI: [0.072, 0.092]; CFI = 0.921; SRMSR = 0.059; TLI = 0.897).
While some of the standardized regression coefficients of the DYSMO were significant, others were not. The significant coefficients include: structural violence (SV) versus religiocultural beliefs (RCB) = 0.463, p ≤ .000; stigma perception appraisal (SPA) versus SV = 0.698, p ≤ .000; SPA versus RCB = −0.185, p ≤ .042; anticipated discrimination (AD) versus SPA = 0.448, p ≤ .000; and social withdrawal (SW) versus AD = 0.661, p ≤ .000. The following coefficients were, however, not significant: AD versus SV = −0.147, p = −.147; AD versus RCB = 0.064, p = 0.494; SW versus SPA = −0.047 p = .710; SW versus SV = 0.016, p = .904; SW versus RCB = 0.039, p = .619 (see Figures 4 and 5 below for details).

The standardized full structural model with all regression paths (significant and non-significant).

The standardized full structural model with only significant regression paths.
Analysis of the path from RCB to AD and RCB to SW indicated that the total effects for the two paths were not significant at (.058, 95% CI = [−0.080, 0.195], p = .411). and (.078, 95% CI = [−0.045, 0.197], p = .205) respectively, as all the confidence intervals included 0.0 within the range of (−2.5% to 2.5% at the 95% CI). In another vein, analysis of the path from SV to AD and SV to SW indicated nonsignificant total effects at (.166, 95% CI = [−0.058, 0.346], p = .107), and (.093, 95% CI = [−0.099, 0.267], p = .317) respectfully. Meanwhile, the total indirect effect from RCB to AD, SV to AD, and SV to SW were significant at (.145, 95% CI = [0.050, 0.293], p = .022), (.313, 95% CI = [0.130, 0.559], p = .004), and (.207, 95% CI = [0.079, 0.420], p = .019) respectively. The total indirect effects of RCB to AD, RCB to SW, and SV to SW were not significant. Details of all the paths, including the specific effects, are presented in Table 5 below).
A Summary of the Mediation Analysis of the DYSMO.

Note. *Denotes significance at p ≤ .05.
Discussion
The current study sought to test a model that examined whether religiocultural beliefs (perceptions), structural violence perspectives, predicted stigma perceptions appraisal, and related outcomes of anticipated discrimination and social withdrawal among PWMI in two public Mental Health Hospitals in Ghana.
A final model with five latent variables and 17 indicators (was more parsimonious and fit the data better than the preceding models. All standardized coefficients of the final model were generally good, as all factor loadings were significant at p ≤ .05). While some standard factor covariances including (SV with RCB; SPA with RCB; SPA with SV; SW with SPA; AD with SV; AD with SPA; and AD with SW), were significant, others such as (SW with RCB; SW with SV; and AD with RCB) were not significant.
The relatively high loadings on the latent variables could be attributed to (1) The fact that items with low correlation coefficients were removed before conducting CFA. (2) Several modifications were made to achieve model fit. (3) The fact that most items were operationalized by rewording them to suit the cultural perspectives of the participants could have influenced responses and subsequent indicator loading problems on latent variables. (4) It is noteworthy that some indicators had negatively worded items. Even though these items were reversed coded, it is possible that the negative wording influenced participant responses during data collection. Being the first model of its kind that studied whether religiocultural beliefs and structural violence perspectives predict stigma perceptions and appraisal, future research may consider replicating the study among different samples of outpatients with mental illness.
Even though Hu and Bentler (1999) suggested a cut-off RMSEA value of <0.05 for a good fit, Browne and Cudeck (1993) and Jöreskog and Sörbom (1993) argue that an RMSEA value up to 0.08 suggests an acceptable model–data fit. Again, some authorities have recommended that to obtain a reasonably well-fit model, the CFI and TLI must be ≥0.90 to demonstrate reasonable fitness (Maydeu-Olivares & García-Forero, 2010; Sun et al., 2012; Zhao et al., 2014). Based on these assertions, one can conclude that the DYSMO fits the data to acceptable levels as the standardized values of the full model include RMSEA = 0.08 (90% CI: [0.072, 0.092]; CFI = 0.92; SRMSR = 0.059; TLI = 0.90).
Having achieved an acceptable model fit for the measurement model, a full structural model analysis was performed in Mplus to test hypothesized relationships between religiocultural beliefs (RCB), structural violence (SV), stigma perceptions appraisal (SPA), and related outcomes of anticipated discrimination (AD), and social withdrawal (SW) among PWMI in Ghana.
Standardized regression coefficients of the structural model were generally significant. These include: (structural violence (SV) versus religiocultural beliefs (RCB); stigma perception appraisal (SPA) versus SV; SPA versus RCB; anticipated discrimination (AD) versus SPA; and social withdrawal (SW) versus AD). The following coefficients were, however, not significant: AD versus SV; AD versus RCB; SW versus SPA; SW versus SV; SW versus RCB).
Again, path analysis of the structural model from RCB to AD and RCB to SW indicated that the total effects for the two paths were not significant, as all the confidence intervals included 0.0 within the range of (−2.5% to 2.5% at the 95% CI). In another vein, analysis of the path from SV to AD and SV to SW indicated nonsignificant total effects. Meanwhile, the total indirect effects from RCB to AD, SV to AD, and SV to SW were significant, while the total indirect effects of RCB to AD, RCB to SW, and SV to SW were not significant. Out of the eight hypothesized relationships, only three (i.e., H4b: Stigma perception appraisal is positively related to social withdrawal behavior among PWMI; H5: Religiocultural beliefs are positively related to anticipated discrimination among PWMI, and H6: Structural violence is positively related to social withdrawal behavior of PWMI, were not significant.
Cultural and religious beliefs influence how mental illness is appraised, recognized, and managed (American Psychiatric Association [APA], 2013). The APA believes that the cultural undertones present a framework for assessing information concerning cultural attributes of an individual’s mental illness and how it relates to a person’s social, cultural, and historical context.
Ghana’s traditional, religious, and cultural practices influence the sociopolitical, educational, legal, and health systems (Gyamfi et al., 2018; Gyamfi, Martin-Yeboah, et al., 2024). These factors intersect to impact individuals’ development and belief systems throughout life. No wonder the understanding and interpretations attached to mental illness vary from culture to culture. It should be noted, therefore, that how one interprets their culture might also influence their appraisal and response to stigma cues. While admitting that some positive religiocultural beliefs, such as praying for the sick person, and giving support among others, tend to lessen the obvious presence of stigma and subsequently reduce the stigma perceptions and appraisal among PWMI, the fact remains that existing religiocultural factors (positive or negative) influence and strengthens structural violence against individuals with mental illness. It is also worth noting that once PWMI normalize their societal religious and cultural belief systems (Vygotsky, 1978; 1987 [1934]), they no longer feel directly affected by these belief systems (negative or positive) and, therefore, may be unlikely to perceive and appropriately appraise the obvious impact of religiocultural beliefs on their stigma perceptions. No wonder that among our Ghanaian participants, religiocultural beliefs were negatively associated with the stigma stress perceptions and appraisal of PWMI. This finding, though significant, considering the role cultural and religious contexts play in the treatment of mental health problems in Ghana and the fact that there is no known study concerning religiocultural beliefs and stigma perception appraisal among PWMI, there would be the need for further research in this area in future studies.
Some contemporary research, including (Gyamfi et al., 2018; Mjøsund et al., 2015; Tawiah et al., 2015), have cited spiritual, supernatural, and cultural (traditional) beliefs as key contributors to perceived origins and treatment protocols of mental illness in certain jurisdictions. Despite strong attributions of supernatural and traditional bases of mental illness, researchers have also alluded to the role of biopsychosocial causal domains of mental illness (Lin, 2013; Shrivastava et al., 2011; Tawiah et al., 2015). In Ghana, a mix of beliefs about mental illness also exist (Gyamfi et al., 2018; Tawiah et al., 2015). All of which could impact stigma stress perception appraisal.
In the current study, Hypotheses (H1: Religiocultural beliefs about PWMI have a significant relationship with societal structural violence against PWMI, H2: Religiocultural beliefs have a relationship with stigma perception appraisal of PWMI and H3: Structural violence is positively related to stigma perception appraisal of PWMI were all supported.
In the study, RCB marginally and negatively correlated with SPA. Several factors could have accounted for this outcome among the participants. (1) Some people see mental illness as a blessing and spiritual connection with God (Choudhry & Bokharey, 2013; Mjøsund et al., 2015). (2) Increased knowledge and acceptance of Biopsychosocial etiology/contemporary Biomedical and genetic treatment courses. (3) Individual cultural and religious differences influence how PWMI experience, perceive or appraise stigma stress. Proponents of the identity threat models of stigma (Major & O’Brien, 2005; Rüsch, Corrigan, Powell, et al., 2009; Rüsch, Corrigan, Wassel et al., 2009) have posited that perceived public discriminatory attitudes and personal factors influence the extent to which PWMI perceive and appraise stigma as stressful, regardless of existing diagnosis or symptoms. The extant literature has also corroborated and established that no two stigmatized persons experience, perceive, or appraise stigma the same way due to existing individual and cultural differences (Bracke et al., 2019; Gopalkrishnan, 2018; Mannarini & Rossi, 2018). (4) Available personal resources. Persons who believe they have enough resources to deal with life’s challenges may likely cope better and effectively deal with any forms of discrimination that come their way. However, the lack of certain resources, including social networks, family and close friends, knowledge, health, energy, and financial resources, or a threat to self-esteem and well-being may potentiate perceived stigma stress appraisal in the individual (Lazarus & Folkman, 1984; Major & O’Brien, 2005). (5) Some PWMI believe and uphold the traditional/religious-oriented therapeutic procedures that include praying and fasting (Breland-Noble et al., 2015; Choudhry et al., 2016), spiritual exorcism and deliverance from “witchcraft” and “evil spirits” (Hailemariam, 2015; Liu et al., 2015) and the administration of herbal concoction to PWMI (Choudhry et al., 2016) as a form of spiritual/social support (Wesselmann et al., 2015) and coping for the individual (Chronister et al., 2015; Wesselmann et al., 2015). Persons who hold their belief systems dear may normalize these practices and, therefore, are more likely to be less affected negatively. Pastwa-Wojciechowska et al. (2021) have asserted that religious and spiritual issues can promote and damage mental health perceptions. This has implications for our findings. Christians often incorporate spiritual and theological concepts into their understanding and meaning-making of mental illness (Lehmann et al., 2021; Pastwa-Wojciechowska et al., 2021).
In their recent study, Lehmann et al. (2021) investigated cultural and theological appropriate pathways toward hospitality in the church in terms of potential resources (such as beliefs, perspectives, and practices) within churches as well as the facilitators or barriers towards PWMI. They observed that their Christian participants recognized the PWMI in their church and acted lovingly towards the sick members by showing compassion, accepting them, and including them in church activities. The fact that the church members showed respect and were nonjudgmental towards the PWMI in the church made them feel a strong sense of belonging in the social setting. In the end, Lehmann and colleagues asserted that the joy associated with the hospitality in some Christian organizations in relation to the support the church gives to members who are sick from mental health problems plays a key role in helping them to normalize the negative perceptions about their illness and to cope with the stigma associated with “being sick from mental health problems.”
Notwithstanding the marginal and inverse direct effect of RCB on SPA, it is apparent that RCB indirectly influences SPA through the mediation effect of SV (which is the aggregation of social injustices and the harms that society inflicts on PWMI).
Our findings also revealed that SPA positively relates to the anticipation of discrimination among PWMI. We found no direct relationship between SW and SPA per our hypothesis (stigma perception appraisal is positively related to social withdrawal behavior among PWMI). It, however, became apparent that AD mediates the effect of SPA on SW as an outcome. This was proven by a significant specific indirect effect from SV to SW. Even though a prediction of a positive direct relationship between SV and AD was not supported, the fact that the indirect effect of SV on AD was significant indicates that structural violence remotely relates to the anticipation of discrimination through the mediation effect of stigma perception appraisal. In other words, heightened levels of stigma stress perception led to increased anxiety and sensitivity to discrimination behaviors from the public.
Structural violence constitutes a psychological form of violence associated with indirect acts from society that constrain and undermine the human rights of certain groups of persons that society regards as different (Gyamfi, 2022, 2024). Structural violence constitutes an injustice within social arrangements that systematically brings subordinate and disadvantaged groups of persons into maltreatment, further placing them in danger of various forms of suffering (Benson, 2008). It must be noted that there is no identifiable perpetrator in structural violence, unlike physical violence, making it difficult to tackle as the source is not readily known. There is no human face seen trying to directly cause harm, and the violence perpetrated is incorporated into existing social structures, a source of “unequal power” that gives rise to inequities such as found in resource allocation against PWMI and mental health care institutions in Ghana and elsewhere (Leatherman, 2011).
Structural violence is characterized by inequality and perceived discriminatory attitudes from society. Perceived discrimination is often associated with stress and anxiety (Cuevas et al., 2021). Stigma stress perception appraisal results from sustained anxiety and self-stigma that leads to continued anticipation of discrimination (Hansson et al., 2014) and subsequently to negative outcomes of social withdrawal, which in a way, acts as both a reaction to negative societal attitudes and as a coping mechanism to reducing further stigmatization (Corrigan & Rao, 2012; Holubova et al., 2016; Tam, 2019). As posited by the stress and coping model (Lazarus & Folkman, 1984), once an individual perceives that their coping resources are unable to stand against the potential harms caused by public stigmatizing attitudes and behaviors (stigma stress appraisal), they may experience negative outcomes that worsen their symptoms and ultimately affect their self-esteem, education, job search, starting or keeping close relationships and overall wellbeing. Therefore, enacting policies that have the potential to reduce exposure to societal discrimination could reduce stigma and its sequels for improved social integration and mental health at the communal and individual levels.
Implications of the Study
The study found that structural violence empowers existing social influences (including religiocultural belief systems) against stigmatized persons in legitimizing and justifying inequalities in the social order. This finding is significant for social and advocacy policy development to lessen social stigma, especially among religion- and culture-oriented societies. Culture greatly influences public perceptions about mental illness and associated stigma among members of society (Choudhry et al., 2016; Mannarini & Rossi, 2018). Cultural influences legitimizing social inequity constitute cultural violence (Galtung, 1990). Cultural violence toward PWMI may be due to deeply entrenched historical and religious antecedents inherited from the Dark Ages. In this demonological era, mental illness was believed to be caused by evil spirits. To this end, “cultural intervention,” an equally opposing strategy aimed at questioning and taking steps to deal with stigma and associated inequalities, should be implemented.
Caregivers, including the patient’s family, ought to be aware of existing negative cultural practices and how they likely impact the therapeutic pathway of their clients so that they can put appropriate remedial measures in place. Having realized that religious and spiritual issues can promote and damage perceptions about mental health, it is imperative that mental health practitioners gain increased awareness and knowledge of the role religious and cultural beliefs play in the treatment and recovery process of PWMI. Experts have observed that the faith of the individual and their involvement in religious practices are a source of hope and strength in fighting against the illness, giving meaning to the illness and, ultimately, leading to better outcomes of treatment (Dyga & Stupak, 2018; Lehmann et al., 2021).
Effective measures may safeguard the therapeutic process for the utmost outcomes towards patient recovery and stigma reduction in society, a perspective from which social responsibility, local and global advocacy, and action toward stigma mechanisms should be assessed and addressed. Structural violence is a product of social and institutional stigma that fuels marginalizing policies of private and governmental institutions that intentionally restrict and hinder the opportunities of people with mental illness (Corrigan, 2004). The outcome of such societal restrictions is the bedrock upon which perceived self and public stigma appraisal thrive among PWMI.
According to Corrigan, “The stigma of mental illness is first, foremost, and only an issue of social injustice. As such, it needs to be understood in the same light as the other forms of prejudice and discrimination that have hounded the modern world: racism, sexism, and ageism, to name a few. As a social injustice, mental illness stigma is largely the responsibility of the societies that created it. Hence, it is up to the people and institutions that populate these societies to recognize the harm caused by stigma and embrace their duty to erase it” (Corrigan, 2005, p. 315). Though largely invisible, the consequence of structural violence embodies long-standing social inequality and psychological pain, otherwise known as social suffering.
That said, the concept of structural violence and its relationship with religiocultural beliefs and stigma perception appraisal among persons with mental illness, as established by this current study, should be of concern to all.
Strengths and Limitations of the Study
This was a seminal work that examined the influence of religiocultural and structural violence perspectives on the stigma perception and subsequent appraisal among individuals with mental illness. The fact that the study was able to ascertain relationships between structural violence, religiocultural beliefs, and stigma perception appraisal is a refreshing and significant contribution to stigma literature and theory. Also, the fact that the data fit the model is an achievement that prepares the ground for future longitudinal and multinational studies in multiple sites. Even though cross-sectional studies are useful for planning, monitoring, and evaluating issues of public health importance, because the research team recruited available outpatients using convenience sampling techniques, these participants likely possessed characteristics that were inherently different from the entire population of outpatients. This could affect the generalizability of the research findings across all outpatients diagnosed with a mental illness. Also, the results may have differed if the sample included a combination of young people (below 18 years) and adults and equal sex distribution among the participants. The fact that some of the instruments in this study were adapted to suit the cultural context of the study population has the potential to undermine the validity and reliability of the study findings. Even though most of the hypotheses were supported, it must be noted that this study was exploratory work that would require further investigation from multiple settings and in different populations of PWMI to validate the DYSMO in the future.
Conclusion
Findings from this study will contribute to global literature on stigma and how people perceive and appraise it vis-à-vis existing public attitudes and behaviors. The model fit indices of the study suggest an acceptable model that fits the data. The study has the potential to ignite national and perhaps global discourses on capacity building through community and institutional engagement to inform and create unique advocacy platforms to begin questioning the status quo while finding innovative ways to address cultural and religious-specific stigma-related behaviors in society. Making such novel ideas available forms the foundation of substantive evidence for future health debates and reference, healthcare policy review, and the conduct of further longitudinal and interventional studies in stigma research to help reduce the ongoing social harms that PWMI face daily.
Footnotes
Acknowledgements
The authors would like to thank all participants.
Authors’ Contributions
SG is the project lead and was involved in the project conceptualization, design, and overall responsibility for the project implementation, data collection and analysis, manuscript writing, and publication. CF was involved in advisory group meetings, project review, implementation, analysis validation, and manuscript review. While RB was involved in advisory group meetings, analysis validation, and manuscript review. IL was also involved in advisory group meetings, analysis validation, and manuscript review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The study was approved by the Western University Research Ethics Board (#115773), Ankaful Hospital (#197487), and Pantang Hospital (#102018). Before participating in the study, the researchers obtained written informed consent from each participant. All methods relating to the study were carried out in accordance with the REB guidelines and regulations.
Data Availability Statement
Datasets generated and/or analyzed during the current study are not publicly available due to participant privacy but are available from the corresponding author upon reasonable request.