
Abstract
The goal of this study is to investigate physicians’ current knowledge, attitudes, and practice regarding colorectal cancer screening (CRC) screening, as well as to determine the barriers to undergoing screening. This was an online-based cross-sectional study that was conducted in the Jazan region of Saudi Arabia. Our targeted population was physicians at different levels. Data were analyzed and compared to determine the knowledge, attitude, and barriers toward the CRC screening. The study eventually included 323 participants, with a mean age of 32.66 (8.79) with the majority of them being residents (26.6%). Interns (25.1%), general practitioners (GP) (22.2%), specialists (15.2%), and consultants (11.2%) were the other levels of physicians. Many of the participants possessed a higher knowledge level. Physician and knowledge levels were not significantly different (p = .821). A statistical difference between the physician level and attitude score was not seen (p = .844), and all the physicians showed a positive attitude toward CRC screening. The most frequently stated patient-related and system-related hurdles were lack of knowledge about colorectal cancer and lack of knowledge about cancer screening guidelines, respectively. Physicians in the Jazan region are knowledgeable about CRC screening effectiveness and risk factors and have a positive attitude toward it. Obstacles, including a lack of understanding of colorectal cancer and the cancer screening recommendations, highlight the significance of raising cancer screening awareness among the public and implementing programs for doctors to update the integrated guidelines.
Plain language summary
Introduction
Colorectal cancer is the third most common cancer globally. Moreover, it is the fourth leading cause of death among all types of cancer (Ferlay et al., 2015). However, the incidence and mortality rates differ widely between countries, with more cases being reported from high-income countries (Arnold et al., 2017). The global burden of colon cancer is expected to increase, with current trends predicting that more than 2.2 million new cases will be diagnosed by 2030 (Arnold et al., 2017). Colorectal cancer is considered one of the most obvious markers of transition in cancer epidemiology, which replaces infection-related cancers in countries witnessing rapid changes in demographics and economic development (Bosetti et al., 2011). In 2015, the Saudi cancer registry stated that colon cancer was responsible for 12% of the total cancer incidence. When there were 1,465 new cases of colorectal cancer with male predominance. As shown by this report, colorectal cancer affected 55.9% of males and 44.1% of females, ranking as the major cause of male cancer and the third leading cause of female cancer (M. H. Mosli & Al-Ahwal, 2012). Since 2002, colorectal cancer incidence has steadily increased in Saudi Arabia, according to research done there (Ibrahim et al., 2008). In Saudi Arabia, the CRC survival rate is 44.6%, which is low compared to global CRC survival rates. When diagnosed at an early stage, the mortality rate of colorectal cancer significantly decreases (Al-Thafar et al., 2017). The WHO has reported that nearly 40% of cancers are preventable and 40% of cancer-related mortality can be avoided if diagnosed at an early stage (WHO, 2009). Several studies have reported a significant reduction in colorectal cancer mortality when screening programs are applied (Dominitz, 2006; Winar, 2007). Optimal recommendations for colorectal cancer screening include different modalities of screening commenced at the age of 50 years. These recommendations include an annual fecal occult blood test, colonoscopy every 10 years, flexible sigmoidoscopy every 5 years, and double-contrast enema every 5 years (Rex et al., 2009). Some patients are advised to undergo colorectal cancer screening earlier, such as those with a family history affecting first-degree relatives or those with a history of conditions that increase the likelihood of colorectal cancer, such as hereditary non-polyposis syndrome or Lynch syndrome. Screening can also detect premalignant lesions (Rex et al., 2009). However, in Saudi Arabia, on top of the absence of regular and well-organized screening programs, there is also a neglect of screening and early prevention culture (Alsanea et al., 2015). Patients will present at an early stage of the illness process if they are aware of the symptoms and signs of colorectal cancer. However, most CRC patients present at an advanced stage, making the chances of cure slim (Alsanea et al., 2015). Knowing the risk factors of colorectal cancer may also have a preventive role. For example, when people know that smoking, obesity, and an unhealthy diet can predispose them to colorectal cancer, they may adopt a healthier lifestyle or at least be triggered to undergo screening, especially when having symptoms suggestive of colorectal cancer (Wong et al., 2013). Therefore, this study aims to evaluate the level of knowledge, attitude, and practice toward colorectal cancer among physicians in the Jazan region. We have chosen the physician population as we believe they pose a great impact on educating people on how to minimize their risk and promoting screening programs.
Methods
Patients and Settings
This is an online-based cross-sectional study that was conducted in Jazan, Saudi Arabia in 2021. The directorate of health affairs of the Jazan region stratifies the 13 sub-regions of Jazan into six sectors: northern, southern, eastern, western, central, and major sectors. Subjects were recruited from the health care facilities of each determined subregion. After recruiting participants by simple random sampling, the questionnaire was sent through social networking applications to each registered email or phone number of participants (e.g., Telegram, WhatsApp, and phone SMS). The primary objective of this study was to investigate and assess knowledge, attitude, and practice toward CRC screening among physicians. Therefore, our targeted population was Jazan region physicians. The study was conducted following the approval of the Institutional Review Board, and participants were asked to agree to participate in the current study before completing the online questionnaire. We excluded respondents that did not agree to take part in this study.
Study Tool and Data Collection
A web-validated bilingual (Arabic and English) questionnaire was used to collect data (Althobaiti & Jradi, 2019). The questionnaire was transformed into an online format using Google forms. The questionnaire included five parts. The first part was to collect demographic information from the participants. The second part was on the knowledge of CRC screening method efficacy and risk factors of colorectal cancer. The third part was about questioning cancer screening beliefs and practices. The fourth part included questions on the attitude toward CRC cancer screening, and the fifth part will have questions on system-related and patient-related barriers to screening.
Demographic features of the physicians, such as gender, age, and level of experience, were collected. Questions about the effectiveness of various suggested cancer screening procedures were used to gage knowledge of colorectal cancer screening tests. In this part, seven screening techniques were provided, and the physicians were asked to say whether they were “very effective,”“somewhat effective,”“not effective,” or “did not know.” The second section contained questions regarding the risk factors for colorectal cancer. Questions on the risk factors for colorectal cancer were found in the second part. This was achieved by giving doctors a list of potential risk variables to pick from. The knowledge scale had a possible range of 0 to 21 points. The scores were converted to percentages, and the results were categorized into two levels of knowledge: high level of knowledge (cut-off value: 11; a score of 50% correct responses) and low level of knowledge (cut-off value: 11; a score of 50% correct responses). The knowledge score among this group of medical students had a median value of around 11, which served as the basis for the cut-off value.
Inquiries about their attitudes toward CRC screening and perceived barriers to patients undergoing CRC screening were also included in the questionnaire. The responses varied from “strongly agree” to “strongly disagree,” with a possible attitude score range of 0 to 10. Based on the mean attitude score of about 5 among the physicians included, the scores were transformed into percentages, and the resulting percentage scores were reported in terms of two categories: a good attitude (≥5) or a poor attitude (<5). Twelve statements were used to address the questions about patient and health system barriers, with seven of them addressing patient-related issues and five addressing health system issues. There were three possible answers: “major barrier,”“minor barrier,” or “not a barrier.”
Statistical Analysis
The data were entered into Microsoft Excel, which cleaned it all up for analysis. Variables were then imported into SPSS (Statistical Package for Social Sciences, version 26) for statistical analysis. Means and standard deviations were used to represent the qualitative data, while numbers and percentages were used to represent the quantitative data. Comparison tests, including the Chi-square test, and the one-way ANOVA, were used to assess the potential association between the different variables of this study. A p-value that is <.05 indicates a significant association.
Results
Baseline Characteristics of Health Care Providers Included in the Sample
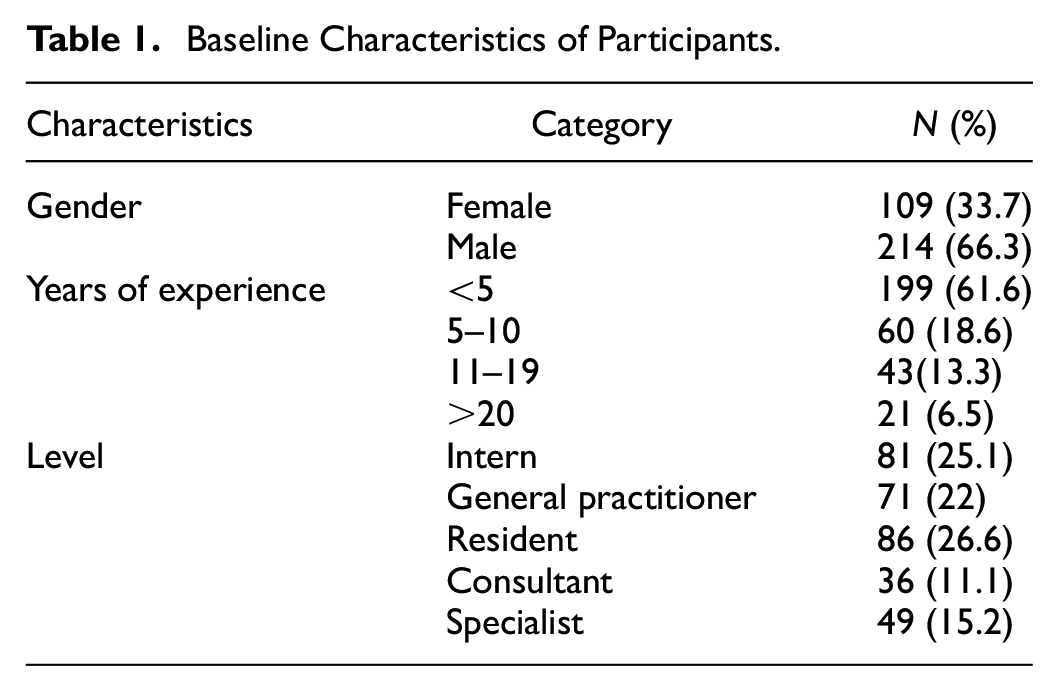
A total of 323 participants were included in this study, with a mean age of 32.66 (±8.79). Most of the participants were male (66.3%), and 33.7% were female. The physicians were mostly residents (26.6%), 22% were general practitioners, 15.2 were specialists, and the remaining participants were consultants (11.1%) in the sample. Only 6.5% of the physician had more than 20 years of experience, while the majority had less than 5 years. The detailed characteristics of the 323 participants are presented in Table 1.
Baseline Characteristics of Participants.
Knowledge Regarding the Effectiveness of CRC Screening Modalities
More than half of the physicians recorded pap smear (51.7%), mammography (57.6%), flexible sigmoidoscopy (62.5%), and colonoscopy (78%) as very effective screening modalities. The majority of physicians (78%) regarded colonoscopy as an effective tool for CRC screening, with only 2.5% stating that it was ineffective. According to about 45.2% of them, the fecal occult blood test is also a very efficient technique. About 36.5% of the physicians in this study believed that the double-contrast barium enema screening technique was somewhat useful, 16.4% said it was ineffective, and 7.1% were unaware of the procedure. According to the findings in Table 2, colonoscopy is a very successful method for CRC screening. There was no significant difference observed in the effectiveness of screening modalities reported among the different physicians (all p-values >.05).
Reported Knowledge Regarding the Effectiveness of CRC Screening Modalities and Risk Factors for CRC.

Of the 323 physicians, most indicated that family history and polyps as the major risk factors following inflammatory bowel disease influenced CRC risk classification. All of the general practitioners (GPs) cited family history and polyps as risk factors, while 98.8% of interns, 93.0% of residents, 89.8% of specialists, and 88.90% of consultants did the same. The other major risk factor identified was IBD. More than 70% of consultants, GPs, interns, and residents claimed that advanced age, smoking, and diet as risk factors. A comparatively lesser proportion of specialists than other levels of participants mentioned smoking (63.3%), diet (61.2%), advanced age (65.3%), or inflammatory bowel disease (71.4%) as risk factors. Specialists claimed a family history of CR and polyps (89.8%) is the major risk factor compared to other factors. Knowledge of risk factors did not differ by physician level (p = .999). With regard to the effectiveness of CRC screening techniques and risk factors, 8% of the physicians in this sample had knowledge scores that were below average, while 92% of the physicians had knowledge scores that were above average. In terms of knowledge level, there was no significant difference between the physicians (p = .821). The detailed statistics are presented in Tables 2 and 3. The knowledge level of physicians was compared across different demographical factors. It has been observed that higher age groups and more experienced physicians had higher knowledge levels (Table 4 and Figure 1).
Association Between Knowledge of the Effectiveness of CRC Screening and Risk Factors Between the Physician Levels.

Knowledge Level Among Different Demographic Variables.

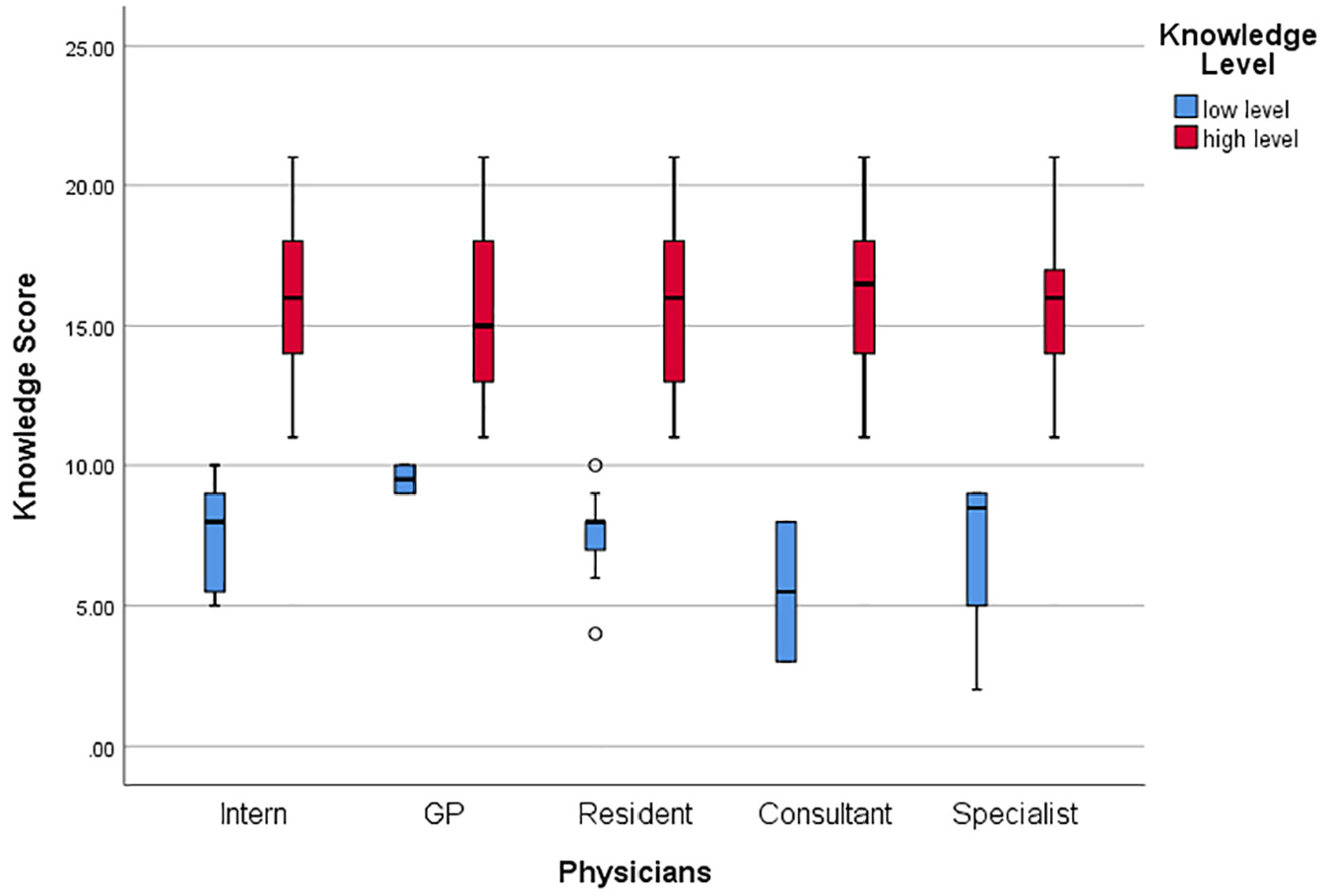
Knowledge score level among the physicians.
Cancer Screening Beliefs, Practices, and Attitudes Toward CRC Screening Among Physicians
There was no significant difference observed in cancer screening beliefs and practices among physicians (all p-values >.05; Table 5). Interestingly, it has been found that all the physicians included in the study had good attitude scores (8.63 ± 0.93) and there was no statistical difference observed between the different physicians in terms of attitude scores (p = .844; Table 6 and Figure 2).
Physician’s Cancer Screening Beliefs and Practices.

Attitude of Different Levels of Physicians Toward CRC Cancer Screening.


Attitude scores among the physicians.
Perceived Patient and System Barriers to CRC Screening
The physicians reported patient-related and system-related barriers to CRC screening. Among the reported patient-related major barriers were patients’ lack of knowledge about screening programs (67.8%), procrastinating the procedure (61.6%), being asymptomatic (58.8%), feeling embarrassed or anxious (58.5%), a fear of discovering cancer (57%), the perception that CRC is not a major health threat (36.8%), and believing that screening is ineffective (34.4%). Lack of knowledge about screening recommendations or guidelines (67.2%), lack of healthcare professionals to provide follow-up with invasive screening (60.1%), and the high cost of screening modalities (49.8%), were the three main health system-related barriers to CRC screening (Table 7 and Figure 3).
Perceived Patient and System Barriers to CRC Screening Among Physicians.

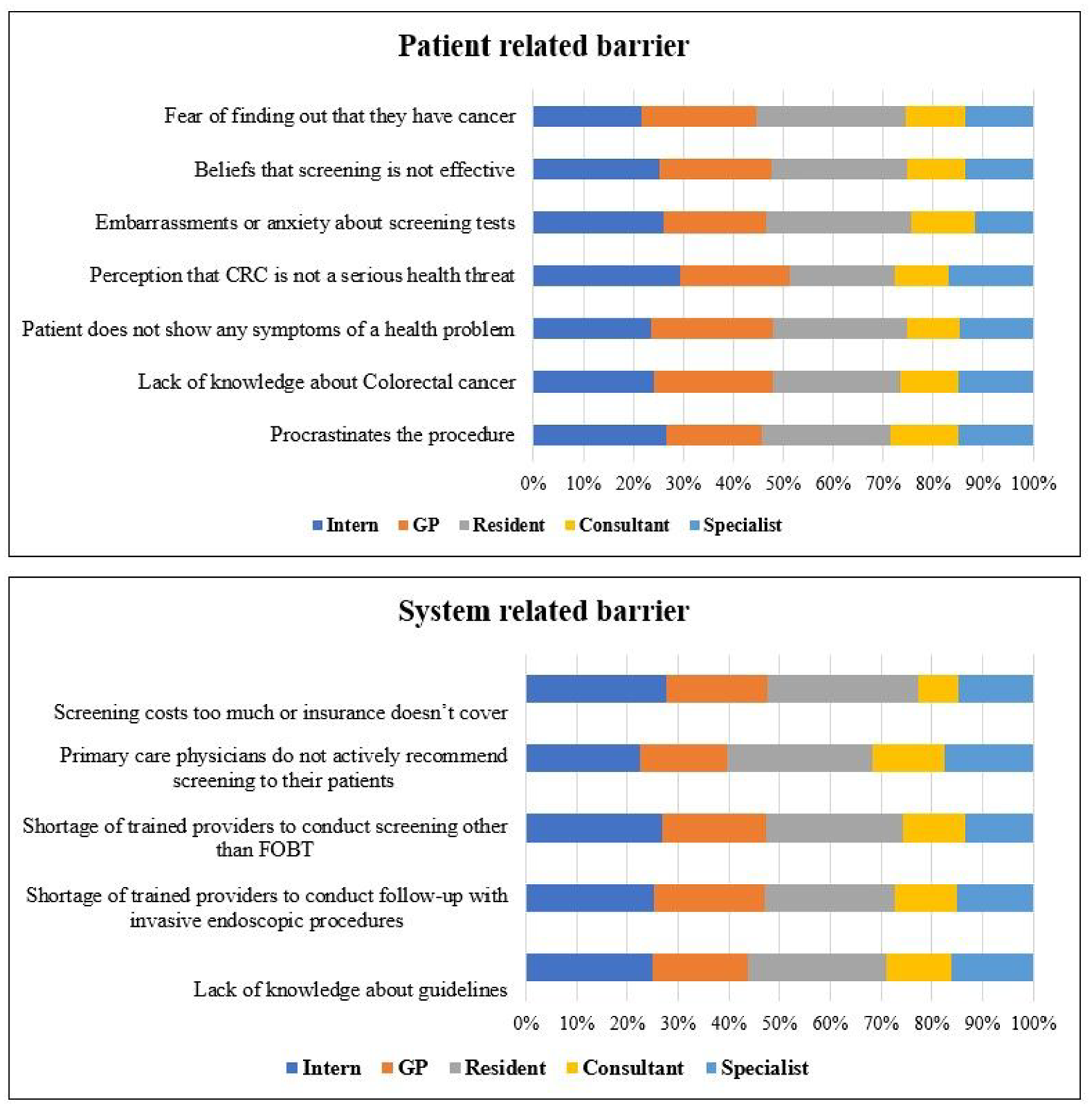
Patient-related and system-related barriers.
Discussion
Since colorectal cancer is a significant cause of cancer morbidity and mortality worldwide, it has been the focus of many studies around the globe. Colorectal cancer screening programs have a direct impact on improving survival rates; thus, many studies have been done to evaluate physicians’ knowledge, attitudes about, and practices surrounding colorectal cancer screening. In the Middle East, the topic of CRC screening was the focus of interest for different studies. Therefore, in the present cross-sectional study, we assessed knowledge, attitude, and practice regarding CRC screening among physicians. Therefore, our targeted population was Jazan region physicians in Saudi Arabia. The results of this survey demonstrate that the majority of physicians in the Jazan region, practicing at various levels, have sufficient knowledge of CRC screening method effectiveness and risk factors related to CRC, as well as favorable attitudes and opinions regarding the obstacles to CRC screening. The resident was found to have a low degree of knowledge compared to others, whereas consultants and GPs were found to have a better level of expertise. The most frequently reported patient-related barriers were not knowing about CRC (67.8%) and procrastinating the procedure (61.6%), while the most common health system-related barriers were not knowing about screening recommendation guidelines (67.2%).
No prior research has looked into the perceived competency of the five levels of physicians included in the present research, despite the fact that colorectal cancer screening knowledge and practices have been investigated in a number of publications. Regarding CRC, a number of studies have been carried out in Saudi Arabia, and each of them came to the same conclusion and emphasized the value of screening (Aljebreen, 2007; Almurshed, 2009; Demyati, 2014; M. H. Mosli & Al-Ahwal, 2012). Previous research has indicated that physicians’ awareness of colorectal cancer screening is satisfactory, which is in line with our study findings (Demyati, 2014). About 56.2% of the 130 physicians did not use CRC screening, although 94.6% thought CRC screening was effective. When compared to other physicians, board-certified physicians had higher knowledge scores and used CRC screening more frequently. As per that study, physicians who reported performing CRC screening performed better on the knowledge test than those who did not.
Colonoscopy was rated as the most efficient cancer screening tool by more than 70% of the consultants, GPs, interns, residents, and specialists, with flexible sigmoidoscopy coming in second. Less than half of the participating doctors thought that the fecal occult blood test was not very useful, which is similar to research done on Riyadh-based doctors by M. Mosli et al. (2017). For asymptomatic, average-risk patients, primary care physicians now most frequently prescribe colonoscopy (95%), followed by a fecal occult blood test (80%; Klabunde et al., 2003; Scheid et al., 2013; Shin et al., 2017). The majority of primary healthcare doctors do not advocate all of the tests included in the national recommendations (Scheid et al., 2013).
Many of the respondents in this survey claimed that the primary risk factor for CRC is a family history of CR or polyps. Major physicians at all levels in this research were aware of the risk factors for CRC, and more than 88% could pinpoint a family history or polyp as a risk factor. In contrast, according to the Survey of Health Care Providers Working in Primary Care Settings, only 25.9% of Health Care Professionals (HCP) were able to correctly identify family history (genetics) as a risk factor. Additionally, more than 70% of the physicians in the various groups who were included in this investigation correctly identified inflammatory bowel disease as a risk factor for CRC. Furthermore, a considerable proportion of physician stated that smoking, getting older and, diet are risk factors for CRC. Nevertheless, a substantial portion of the consultants indicated that CRC development is related to a lack of regular exercise. Although epidemiological data repeatedly reveals that physical activity lowers the incidence of colorectal cancer (Amersi et al., 2005; Baena & Salinas, 2015; Giacosa et al., 1999; Haggar & Boushey, 2009). In our study, over 40% of interns, GPs, residents, and specialists underestimated the connection between physical inactivity and colorectal cancer.
Patients’ fear of finding out they have cancer, a lack of information on CRC screening tests, a shortage of skilled staff to do screening procedures, and a lack of protocol on CRC screening were the most reported barriers to CRC screening (Omran et al., 2015). According to a study conducted in Oman in 2016 (Muliira et al., 2016), the key barriers reported by the participants were a lack of hospital guidelines, a shortage of skilled HCPs, a scarcity of CRC screening services, and timely CRC screening appointments. The reported patient-related barriers were fear of cancer diagnosis, feeling that screening is ineffective, and anxiety over screening tests. The lack of understanding of colorectal cancer standard guidelines, in general, has been noted to be a major health system-related barrier that prevents the recommendation of specific types of CRC screening tests or procedures or any screening at all. The lack of integrated and updated guidelines in the health care system is the major barrier in the current study that is in line with other literature (Althobaiti & Jradi, 2019; Chen et al., 2014; Omran et al., 2015; Qumseya et al., 2014). The low incidence of screening has been attributed to behavioral patterns and educational limitations (Scheid et al., 2013). The findings indicate a need for interventions to enhance patient awareness, HCP’s CRC screening practices, and strategies to ameliorate patient and system barriers to CRC screening.
In Qatar, A cross-sectional survey was distributed to internal physicians in the period 2018 to 2019. According to the study, internal physicians had a good attitude regarding CRC screening, but their knowledge of relevant guidelines for screening and practice was suboptimal (Mahmoud et al., 2020). A descriptive study was conducted in a university hospital in Turkey in 2019 (Soylar et al., 2020). A total of 475 health care providers participated in this study, including 84 medical doctors. The study showed an overall positive attitude toward all kinds of cancer screening. In Saudi Arabia, a study was conducted among family physicians in the national guard hospital in 2014. The study showed that the overall attitude toward CRC screening was positive. Male physicians generally had more positive attitudes than female physicians (Demyati, 2014). In general, physicians have a positive attitude toward CRC screening, as reflected by the attitude score.
Study Limitations
The present study is the first to document physicians’ perspectives on the hurdles of CRC screening and their understanding of screening practices in the Jazan region. However, it is important to acknowledge several limitations that should be considered when interpreting the results. First, the cross-sectional design limits the ability to establish causal relationships between physician knowledge, attitudes, and practices related to CRC screening. Since data were collected at a single point in time, it is not possible to assess changes in these variables over time or determine how certain factors might influence future screening behaviors. This design inherently limits the conclusions that can be drawn about the long-term effects of interventions to improve CRC screening practices.
Second, while we employed a simple random sampling method to recruit physicians across Jazan, the online data collection method may introduce selection bias. Specifically, only those who agreed to participate in the study were included, which could lead to self-selection bias. It is possible that those who chose to participate were more motivated or had higher baseline knowledge about CRC screening, potentially skewing the results and making it difficult to generalize findings to the entire population of physicians in the region.
In terms of reliability, the use of a self-reported online questionnaire may introduce response bias. Participants may overestimate their knowledge or underreport certain barriers due to social desirability bias. The knowledge and attitude scores were derived from participants’ subjective responses, which can lead to variability in how individuals interpret and respond to the questions. While the questionnaire was adapted from validated tools, the subjective nature of some items could affect the consistency of responses across participants.
Another limitation is the potential for measurement error in assessing physicians’ knowledge. Although the knowledge scale was based on correct responses to factual questions, ambiguity in how some questions were understood could lead to misclassification of knowledge levels. Additionally, the cut-off value for distinguishing high and low knowledge levels, based on the median score, may not capture subtle variations in knowledge across the sample.
Lastly, while this study provides valuable insights into the Jazan region, external validity may be influenced by contextual factors such as differences in patient populations or regional implementation challenges. These factors could affect knowledge, attitudes, and practices related to CRC screening. To enhance generalizability, future studies should aim for broader representation across diverse regions and healthcare systems. Despite its limitations, the current study’s findings highlight the need for initiatives to raise public awareness of CRC screening and for clinicians to improve their knowledge about screening standards.
Implications for Practice, Public Health Education, Policy, and Research
Raising public awareness about CRC and the importance of regular screening is critical for promoting disease prevention and control. This is particularly pressing in the Middle East, where cancer mortality is projected to rise substantially in the coming years. While CRC screening has already been shown to reduce mortality rates globally, the burden of CRC remains high as it continues to be the third most common cancer worldwide. Public health education campaigns tailored to local populations can serve as a critical intervention, as awareness has been repeatedly shown to influence preventive behaviors. Therefore, community-focused efforts to educate the public about CRC risk factors, screening modalities, and the benefits of early detection should be prioritized.
In practice, this highlights the need for improved physician education and training, particularly for trainee physicians. Ensuring that these physicians are well-versed in CRC screening protocols and the proper use of diagnostic tools can significantly enhance screening uptake. There is a pressing need for physicians to be regularly updated on CRC screening guidelines and protocols, with continuing medical education programs focusing on improving physician knowledge and addressing any gaps in understanding. Adequate training is crucial for ensuring that physicians not only understand the risk factors and screening options but also feel confident in recommending and performing appropriate screening procedures. This will be vital to reducing the burden of CRC in regions like Jazan and beyond.
From a policy standpoint, the need for standardized national screening programs cannot be overstated. In the current study, both patient-related and system-related barriers to CRC screening were highlighted, with the most common health system barriers being a lack of awareness about screening guidelines and the limited availability of trained healthcare professionals. To address these issues, policymakers must focus on expanding access to affordable CRC screening services and ensuring that healthcare professionals are adequately trained and supported to perform these procedures. There is also a need for integrated, up-to-date screening guidelines within healthcare systems, as identified in both this study and the existing literature. Policymakers should prioritize funding for training and infrastructure development to build capacity for CRC screening, particularly in underserved areas.
In terms of research, further investigation into the effectiveness of interventions aimed at enhancing both physician knowledge and public awareness is warranted. Longitudinal studies could provide valuable insights into how improvements in physician training and public education impact CRC screening rates and patient outcomes. Additionally, future research should explore the specific barriers to CRC screening in various populations, with a focus on tailoring interventions to address cultural, socio-economic, and systemic challenges. Exploring the impact of policy changes and public health initiatives on screening uptake would also be valuable for informing future healthcare strategies.
Conclusion
Physicians in the Jazan region are knowledgeable about CRC screening effectiveness and risk factors and have a favorable attitude toward it. Obstacles, including a lack of understanding of colorectal cancer and the cancer screening recommendations, highlight the significance of raising cancer screening awareness among the public and implementing programs for doctors to update the integrated guidelines.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.