
Abstract
Elective surgical case cancellation is common and can have significant adverse effects by causing prolonged waiting times, harm to patients, and wasting of scarce resources in countries like Ethiopia. Cancellation of scheduled surgeries may lead to reduced occupation of operation theatres and may be recognized as a major cause of trauma to patients and their families. Reasons for elective surgery cancellation are complex and different from hospital to hospital. Many literatures agree with patient related, facility related, medical related and staff related others divide reason in to two avoidable and non-avoidable causes. The aim of this study was to assess prevalence of cancelation of elective surgery and associated factors in public teaching hospitals of Addis Ababa, Ethiopia, 2021. This was institutional-based cross-sectional study conducted in all operation theater specialties from February 1 to March 30, 2021 at Tikur Anbessa Specialized Hospital (TASH) and Yekatit 12 hospital. The study participants consisted of patients across all ages, included both genders and who were scheduled for elective surgery. Data was collected by using pretested structured questionnaires and an assigned operational theater staff was recording the cancelled cases in real time. Data was entered in to SPSS version 25 for analysis. Logistic regression models were used to identify predictors of cancellation of elective surgery. Statistical significance was determined using odds ratio with 95% confidence interval and the narratives were used to describe the quantitative findings. During data collection period, 924 elective surgeries were scheduled to be performed in all surgery departments at Tikur Anbessa Specialized Hospital and Yekatit 12 hospital, of which 225 (24.35%) were cancelled on the day of surgery. The average age of participants was 35.2 ± 19.17 (Standard Deviation) years the main reason for cancellation were shortage of time (26%) followed by facility related (23%), medical related (18%) and Covid-19 related problems (15%). This study found that the cancelation of elective surgical operations on the scheduled day of surgery was significant. Most of the reasons were due to avoidable causes. A team approach was employed to ensure the presence of policies and procedures for improving efficiency and scheduling realistic operation lists.
Introduction
Elective surgical case cancellation refers to any surgical case that is booked into the operation theatre list on the day prior to surgery, but is not operated upon as scheduled. Cancellation of elective operations is a parameter to assess quality of patient care and quality of the management system (Askari et al., 2020; El Bushra Ahmed Doumi & Mohamed, 2007). The reported incidence of cancellation in different hospitals ranges from 10% to 40%. There are many reasons of cancellation of elective surgical cases; and they differ from hospital to hospital (Cho et al., 2019; El Bushra Ahmed Doumi & Mohamed, 2007; El-Dawlatly et al., 2008). The cancellation of surgery is a significant drain on health resources therefore, major hospitals invest considerable resource in maintaining operating rooms (OR) (Karashi et al., 2018; Sultan et al., 2012). Higher rates of cancellation in academic institutions as well as the unpredictability of maximum care may lead to case cancellations (Schuster et al., 2011; Wong et al., 2018). Although, the OR accounts for more than 40% of the hospital’s revenue, it is also costly for the hospital to maintain the OR service (Health Association, 2005; Lankoande et al., 2016).
There are numerous reasons for cancellations of elective surgical cases which include patient-related factors such as inadequate preoperative preparation of the patient, changes in the patient’s medical condition prior to the surgical procedure or the patient refuses to continue with the surgery after procedural consent. Additionally, surgeon-related factors can influence cancellations through inadequate interpretations of indications, poor scheduling of procedures or unavailability of surgeons for the procedures. Facility related factors are emergency procedures which interfere with the regular operating schedule, lack of space and time to perform surgery or shortage of staff and materials necessary for the surgical procedure (Argo et al., 2009; Farasatkish et al., 2009; Karashi et al., 2018).
Unexpected operating room cancellations are traditionally divided into avoidable cancellations (e.g., scheduling errors, equipment shortages, and cancellation due to inadequate preoperative evaluation) and unavoidable cancellations (e.g., emergency case superseding the elective schedule, unexpected changes in the patient’s medical status, or patient nonappearance). And the most common factor which has led to cancellation is lack of OR time (Chalya et al., 2011; Dedecho et al., 2020).
Last minute cancellations result in inefficient use of resources, not in the interests of the patient or the hospital, and result in lost capacity and a substantial amount of work were done after admission of the patient still surgery with multidisciplinary team (Cho et al., 2019; Jamieson, 2008). A pre-surgical anesthetic evaluation to assess patient’s fitness for surgery is not usually performed before the operation unless requested by the senior surgery consultant a day before surgery (Desta et al., 2018; Kumar & Gandhi, 2012).
Cancellation of elective surgical procedure is a well-recognized problem in perioperative care and one of the nursing sensitive quality indicators in perioperative care. Cancellation of elective operation decrease the over-all efficiency of the operating rooms (ORs), reduces utilization of OR time and waste resources (Dexter et al., 2002; Wong et al., 2018). Unanticipated cancellation of planned operations results in distortion and alteration of surgical list, underutilization of man power wastage of scarce resource duplication of workload wastage of operating room time (Karashi et al., 2018; Kolawole & Bolaji, 2002; Robb et al., 2004; Zafar et al., 2007). Cancellation burden on patients and families are significance emotional trauma, anxiety, expend extra cost due to long hospital stay and poor satisfaction, disruption of daily life and interruption of patient hospital relationship (Cho et al., 2019; Kolawole & Bolaji, 2002; Miller, 2004; Ojo & Ihezue, 2008).
Continuous monitoring may be a tentative problem to encounter the solution. An efficient operating theater planning and scheduling provide efficient health care delivery system. University hospitals had significantly higher cancellation rates than did smaller hospitals, and among the services, general surgery services had the highest cancellation rate (Cardoen et al., 2010; Kaddoum et al., 2016). Previous studies conducted in low-income and developed countries have produced a strong body of evidence suggesting that the burden of these cancellations is excessively high in developing countries (Gajida et al., 2016).
Elective surgery would have an implication on patient satisfaction, staff morale and hospital patient relationships additionally, indirect way of assessing the quality of surgical services and care (Ogwal et al., 2020; Robb et al., 2004; Zafar et al., 2007). Elective surgeries have the advantage of advancing knowledge, planning and preparing for the possibility of complications, to achieve reduced morbidities and improved outcomes (Askari et al., 2020; Dexter et al., 2002; Rai & Pandit, 2003).
Globally, approximately 312.9 million operations are conducted every year between 10% and 40% of elective surgery were cancelled however, in low-income countries, cancellation rates are as high as 48.5%. While it may not be practically possible to have a zero percent cancellation rate in health facilities, especially due to unforeseen, unavoidable circumstances, an incidence rate of less than 10% may be permissible. In Ethiopia previous study reported from different university hospitals ranges b/n 8.9% and 33%. Elective surgery cancellation causes reduction in the efficiency of operating rooms and, consequently of hospitals. It is associated with wide-ranging clinical, psychological, and economic consequences to the patients, hospitals, and health care providers, although patients are the most affected (Fayed et al., 2016; Gajida et al., 2016; Hovlid et al., 2012; Weiser et al., 2016; Yohanes et al., 2020).
It is a well-known fact that if resources are not properly utilized, the general population suffers, this is especially true about the lower income groups, who depend more on public or government services for most of their healthcare needs. The cost of facilities and equipment that are underutilized adds to the cost of services, which is ultimately passed on to patients. Therefore, avoiding cancellation is an essential step to reducing these costs (Dedecho et al., 2020; Weinbroum et al., 2003).
Cancelation may cause patients and their families to experience emotional trauma, anxiety, expend extra costs during extended hospital stay, poor satisfaction with services, disrupt their daily lives and influence the patient-hospital relationship. These may worsen client conditions and also lead to morbidity as well as mortality. Cancellation of scheduled surgery creates an economic and psychological effect for patients and caregivers. It has long term negative emotional effects on the patient which includes anxiety and depression after hospital discharge (Mutwali et al., 2016).
Avoidable reasons for surgical cancellation may be due to inadequate preoperative preparation, difficulties with the operating schedule as well as cancelling surgery due to shortage of equipment and staff. Unavoidable reasons may include changes in the medical condition of the patient and emergency procedures that interfere with the elective operating schedule. Healthcare facilities have the goal of taking appropriate steps that will have an impact on the avoidable factors for cancelling elective cases in order to reduce the hospital’s costs, shorten the number of hospitalization days, enhance the utilization of the operating rooms, enable better distribution of the staff and increase the patient satisfaction level. In accordance with the hospital’s organization, internal work evaluation is conducted in order to improve efficiency, safety and quality of healthcare services. The rate of elective case cancellation on the day of surgery is an important health care quality indicator (Chalya et al., 2011; Solak et al., 2019).
Increasing patient satisfaction through efficient practice is an appropriate objective of a healthcare system. A high cancellation rate for elective surgical procedures makes it difficult to accomplish this (Dexter et al., 2002; Solak et al., 2019). Cancellation reduces operating room efficiency and increases treatment costs. Cancellation of operations in hospitals is a significant problem with far reaching consequences. Cancellation of an elective surgery increases the patient’s stay in the hospital and associated inconvenience (Dexter et al., 2002; González-Arévalo et al., 2009; Shiferaw, 2016).
Methods and Materials
Study Design, Setting, and Period
This study was conducted in Addis Ababa, the capital city of Ethiopia. The city has a subtropical highland climate. Addis Ababa city currently has a population of 4.8 million people in the urban area and 2.7 million people in its city area and all ethnic groups of the country are represented in this capital with the biggest groups being the Amhara, Oromo, Gurage, Tigray and Gamo.
Languages spoken include; Amharic, Afan Oromo, Gurage, Gamo, Tigrinya and Silte. The religion with the most devotees in the city is Orthodox followed by Muslims, protestant and catholic (55).
In this city, there are 14 public hospitals, 34 private hospitals, 86 health centers and various NGOs and health institutions. Out of 14 public hospitals three of them are public teaching hospitals these are Tikur Anbesa Specialized Hospital, St. Paul’s Hospital Millennium Medical college, and Yekatit 12 medical college. From these three public teaching hospitals we selected the two hospitals by using simple random sampling technique. These hospitals are relatively equipped and serve as almost the whole population of the city as well as receive patients from other regions for a sub specialty area.
These hospitals are tertiary referral hospitals which perform activities in a sub specialist level TASH have 850 beds and 9 OR and Yekatit 12 hospital medical college have 5 OR suite. They are also a teaching hospital for the Medical College and it gives service to the patients under different clinical disciplines which include orthopedics, general surgery, obstetrics, gynecology, pediatrics, cardiothoracic, urology, neurosurgery and ENT surgery and also internal medicine. The data obtain from these two hospitals until the required number of patients fulfill in all selected specialty, to assess the cancellation rate and factors of cancellation among elective scheduled surgery in 2021.
Study Participants
All patients, of all ages, both genders, who were scheduled for elective surgical operations from all surgical specialties at TASH and Yekatit hospitals all major OR table during the study period were included.
Sample Size and Sampling Technique
The sample size was calculated by manually taking the population proportion of 21.41% from a systematic review and meta-analysis study done at Gonder University, Ethiopia (21). The sample size was calculated by using the following formula.

p = incidence of day of surgery cancelation; d = margin of error …0.05; z = 95% Confidence interval: Zα/2 = 1.96; and n = 1.96 × 1.96 × 0.2141 (1−0.2141)/0.05 × 0.05 = 259
From the above initial population calculated sample size, N or total number population is <10,000 population that needs adjustment using final correction formula.

where ni = calculated sample size; N = total target population of the study area; nf = final sample size; nf = 259/(1 + (259/950)) = 204; and n = 204, considering 10% non-responders sample size were = 225.
Distribution of study subject for each hospital was TASH (136) and Yekatit 12 hospital (89).
We used the random sampling techniques and includes two public teaching hospitals of Addis Ababa (TASH) and Yekatit 12 medical college). All patients scheduled for elective surgical procedures during the study period were included in the study, and those listed for elective surgery but done before the day of schedule as an emergency, patients scheduled in a minor operating room for minor surgery, which does not have preoperative assessment sheet were excluded.
Before conducting the interview, we were obtained the consent from all study participants and by using non probability, purposive sampling technique interview the participant until the required sample size. Data collectors was recruited based on reviewing their experience on data collection and OR training was a selection criterion, the recruitment was done by the OR directorate collaborate with the principal investigation.
Data Analysis
Data were checked for consistency of information, code and cleanness and manually edited and entered into the computer using Epi Info version 3.5.4 for further editing. Edited data was exported to the SPSS version 24 statistical software for analysis. Descriptive and basic analytical statistics were used to summarize the data and present in the form of proportion frequency, table, bar graph, pie chart, mean, standard deviation and bivariate.
Results
Socio-Demographic Characteristics
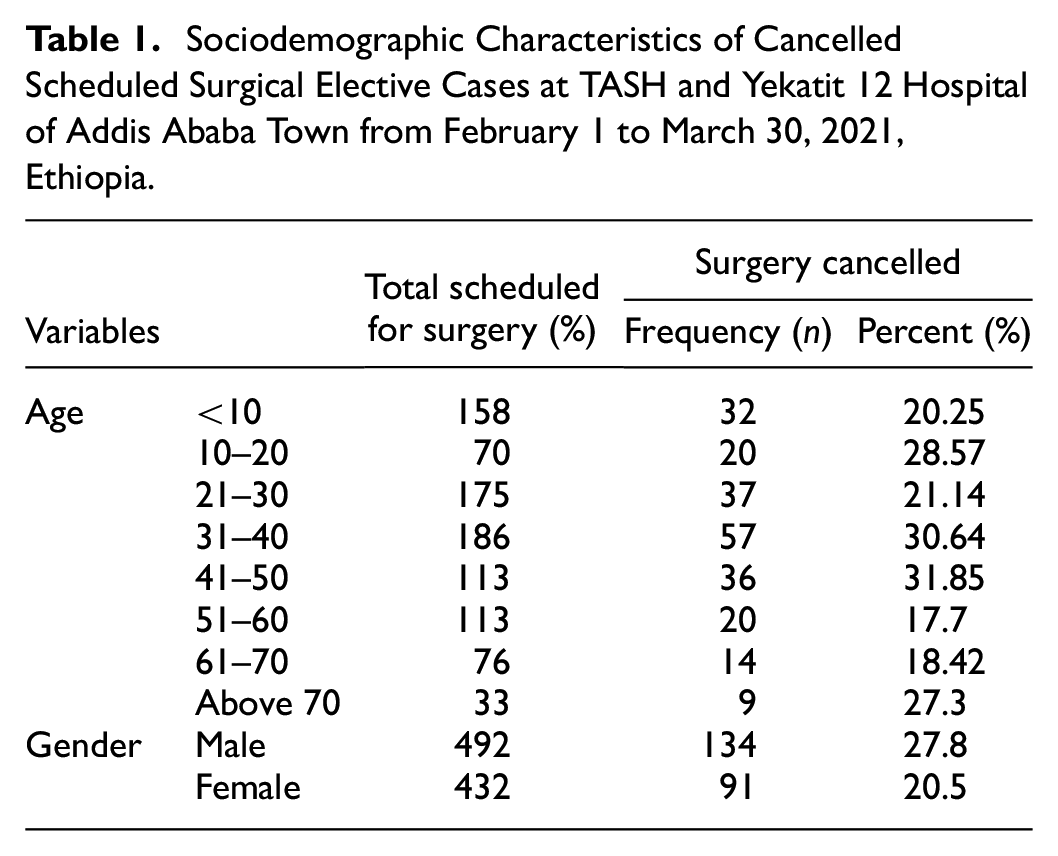
A total of 924 elective surgical cases were scheduled for operation during the study period. The mean age of the participant was 35.2 ± 19.17 (SD) years and most of the participants were in the age group of 31 to 40 years. From the study 699 patients were operated on the intended day of surgery and 225 patients were cancelled. Male gender comprises of 134 in number and 91 for females. Male have a high rate of cancellation than female (Table 1). Regarding the hospital CR TASH was 459 patient plans for surgery of which 136 (29.63) cancelled and Yekatit hospital was also 465 patients plan for surgery out of which 89 (19.14%) cancelled (Table 1).
Sociodemographic Characteristics of Cancelled Scheduled Surgical Elective Cases at TASH and Yekatit 12 Hospital of Addis Ababa Town from February 1 to March 30, 2021, Ethiopia.
Distribution of Cancelled Scheduled Elective Surgery
General surgery and orthopedics had the highest number of cancellation (45 and 36 respectively) whereas vascular and maxillofacial surgery had the least number of cancellations (7 and 2) respectively. Pattern of cancellations of every surgical specialty (Figure 1).

Distribution of cancelled scheduled elective surgical cases in each department/specialty at TASH and Yekatit 12 hospitals of Addis Ababa town from February 1 to March 30, 2021, Ethiopia.
Reason for Cancelled Scheduled Elective Surgery
The most common causes for cancellations were time related factor (overbooked list) (45%), around 26.22% of the cancellations were due to prolonged previous case, over scheduling and late skin incision time at the day of planned operation (Table 2).
Reason for Cancelled Scheduled Elective Surgical Cases at TASH and Yekatit 12 Hospital of Addis Ababa Town from February 1 to March 30, 2021, Ethiopia.

Frequency of Elective Surgery Cancelation
Frequency of elective surgery cancelation were 72% of the patient cancelled for first time and the rest 28% cancelled two and above times (Figure 2).

Shows number of cancelation experience of participant in TASH and Yekatit hospital of Addis Ababa, from February 1 to March 30, 2021, Ethiopia.
Facility Related Reason for Scheduled Elective Surgery Cancelation
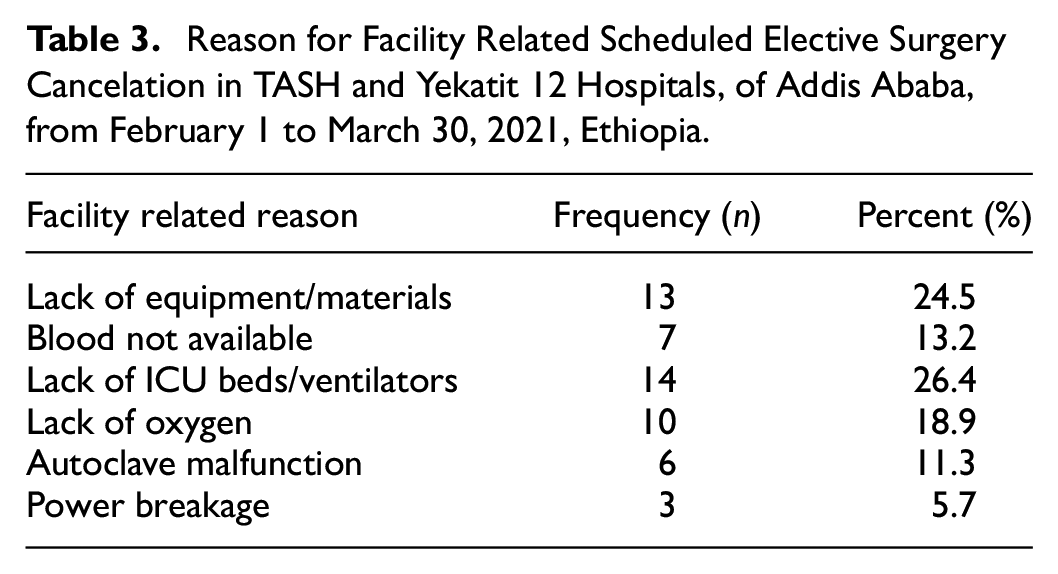
The second causes of cancellations were due to facility related or management related such as lack of ICU beds with mechanical ventilator, around 23.56%, in this category, lack of necessary equipment and devices it accounts 25% and lack of oxygen 19% reason of cancellation had shown in (Table 3).
Reason for Facility Related Scheduled Elective Surgery Cancelation in TASH and Yekatit 12 Hospitals, of Addis Ababa, from February 1 to March 30, 2021, Ethiopia.
Other Causes of Cancellation for Scheduled Elective Surgery
Other causes of cancellation in our study were uncontrolled medical illness 41 (18.22%) out of which the most common disease were hypertension and upper respiratory infection and the next cause of cancelation was COVID 19 related reason accounts 34 (15.11%) in this category common reasons are positive COVID 19 result and result was not reach or not available during the time of surgery.
Patient related reasons contributed 16 (7.1%) in this category patient on medication is common. Lack of important investigation 13 (5.4%) lack of electrolyte and echocardiogram investigation were the most common problems. Staff related reasons 8 (3.6%) only surgeon and anesthesia staff participate in cancelation of patients and unexpected emergency 1 (0.45%) due to difficult intubation (Table 4)
Reasons for Cancelled Elective Surgical Cases in Tikur Anbesa Specialized Hospital (TASH) and Yekatit 12 Hospital of Addis Ababa, from February 1 to March 30, 2021, Ethiopia.

Factors Association with Cancelled Scheduled Surgical Elective Cases
We perform bivariate analysis of gender, department and age group of which male patient OR (odds ratio) 1.403 CI [1.034, 1.904], p (.03). Department of ENT surgery with the OR 0.356 CI [0.181, 0.697], p (.003) and Endourology surgery were OR 0.297 CI [0.138, 0.642], p (.002). From the age group 31 to 40 years OR 1.740 CI [1.058, 2.862], p (.029) and 41 to 50 years OR 1.841 CI [1.058, 3.204] p (.031) were significant but in multivariate analysis only male patient OR 0.623 CI [0.441, 0.879] p (0.03) were significant (Table 5).
Bivariate and Multivariate Analysis of Gender, Department and Age at TASH and Yekatit 12 Hospital of Addis Ababa from February 1 to March 30, 2021, Ethiopia.

Statistically significant.
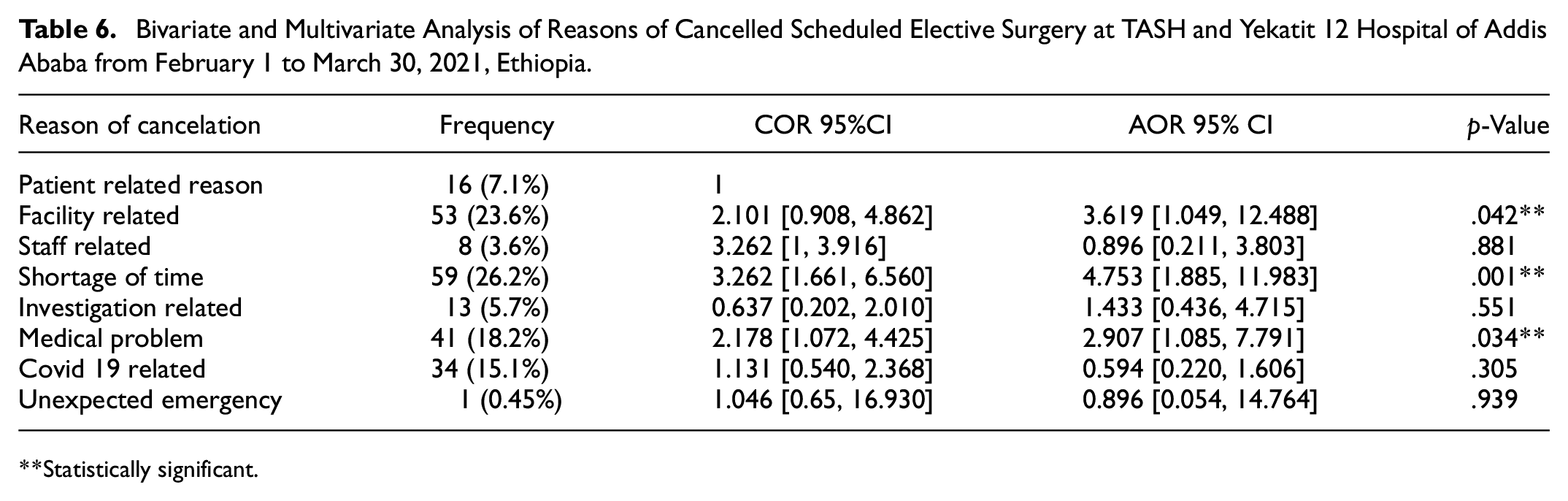
In bivariate analysis for the reason of cancelation on facility related the OR shows 2.101 CI [0.908, 4.862] p (.02), shortage of time OR 3.262 CI [1.661, 6.560] and p (.03) and medical reason OR 2.178 CI [1.072, 4.425] and p (.017) were statistically significant (Table 6).
Bivariate and Multivariate Analysis of Reasons of Cancelled Scheduled Elective Surgery at TASH and Yekatit 12 Hospital of Addis Ababa from February 1 to March 30, 2021, Ethiopia.
Statistically significant.
Also, in multivariate analysis facility related reason OR 3.619 CI [1.049, 12.488], p (.042), shortage of time OR 4.753 CI [1.885, 11.983], p (.001) and medical reason OR 2.907 CI [1.085, 7.791], p (.034) were statistically significant but staff related, Covid 19 related, investigation and unexpected emergency were not significant (Table 6).
Discussion
Cancellation of elective surgery is a worldwide problem though booking elective surgery is considered a contract between the patient and the healthcare institution and also determines the day of service. Elective surgical operations require a multidisciplinary approach between surgical team, hospital staff and hospital administration. Case cancellations on the day of surgery lead to underuse of OTãs, increases waiting period for the patients, frustration and mental stress to the patients and their families, and increases cost and wastage of hospital consumables (El-Dawlatly et al., 2008; Lankoande et al., 2016; Ojo & Ihezue, 2008; Zafar et al., 2007). Therefore, any cancellation of the booking, without prior notice or arrangement from either the patient or the healthcare provider, has far-reaching implications for both (Perroca et al., 2007).
There is no consensus on the maximum acceptable case cancellation rate for efficient operating theatres, but rates under 5% are generally recommended (Ogwal et al., 2020). Elective surgical case cancellation in developing country ranges from 10% to 40% (Chalya et al., 2011). In our study, the rate of cancellation of elective surgical procedures was 24.35%, indicates preoperative system was inefficient which is higher than study done in USA 4.4 % (Kaddoum et al., 2016), UK 10% (Wong et al., 2018), Bahrain 7.3% (Yu et al., 2017), Korea 8% (Cho et al., 2019) and Nigeria 20.2% (Fatungase et al., 2016) and similar with studies done in Ghana 25% (Anarfi et al., 2020) and Jimma university teaching hospital (23%) (Haile & Desalegn, 2015) and lower than study conducted in India 27.3% (Nanjappa et al., 2014), Uganda 28% (Ogwal et al., 2020), Asella 32% (Dedecho et al., 2020), and Hawassa 31.6% (Desta et al., 2018). This discrepancy might be due to the fact that in sociodemographic characteristics, sample size, study area, methodological difference, inappropriate scheduling and poor communication among stakeholders.
From 924 scheduled cases 492 (53.24%) male and 432 (46.75%) were female, of which 225 were cancelled of this male and female were 59.6% and 40.4% respectively. This result is similar with the study done in Hawassa university hospital, were (56.8%) male and (43.2%) female. In our study Male have a high rate of cancellation than female.
The mean age of the scheduled elective surgical cases was 35.2 ± 19.17 (SD), with minimum value 15 days and maximum 86 years old. Between 31 and 40 years old age group were the highest scheduled and canceled 198 (20.1%) and 56 (25.2%) respectively and 21 to 30 years old group were second highest 37 (16.6%) canceled groups and less frequent cancellation were over the age of 70 (4%).
Most common reasons for cancellation were shortage of time and management related 59 (26.22%) and 53 (23.56%) respectively. Shortage of time in our study were the most common avoidable factor which are prolonged first case 45%, over /improper/ scheduling 35%, late start skin incision 16% and poor integration or communication among staffs. This result is similar to other studies done in Bahrain, the most common causes for cancellation were 110 (26.1%) long list (Karashi et al., 2018), in Bosnia and Herzegovina lack of time to perform surgery were 33.51% (Lankoande et al., 2016) and in Jimma cancellation due to in-appropriate scheduling were (33.5%) (Haile & Desalegn, 2015), but study higher when compared to our result which is done in India cancellation due to list over run were (73%) (Nanjappa et al., 2014). This is due to over booked and not know exact time of the procedure, majority of the surgery starts after 2:30 am and extended time of break between surgeries. In addition, in proper anesthesia setup and unavailability of experienced surgeons on time. Patients who cancelled by shortage of time were 4.7 times more likely canceled than patients who canceled by patient related reason 95%CI [1.885, 11.983].
The second most reasons in our study were management /facility/ related reasons which accounts 53 (23.56%) these are lack of ICU beds with mechanical ventilator 14 (26.92%), lack of instrument and medical device 13 (25%) and lack of oxygen 10 (19.23%) similar study done in American University of Beirut, (19.9 %) (Kaddoum et al., 2016), in Saudi Arabia 20.3% (Askari et al., 2020) in Nigeria, 27.6% (Fatungase et al., 2016) in Jimma, (21.87%) (Haile & Desalegn, 2015) in Hawassa, 21.2% (Desta et al., 2018),but study higher when compared to our result were 53% in Bahrain (Karashi et al., 2018) and 67.83% in Uganda (Ogwal et al., 2020) were due to facility related factors. The cause of facility related problem was insufficient organization among hospital stakeholders and gap in utilization of scarce resources and long process while in purchase. Patients who cancelled by facility related reason was 3.6 times more likely to be cancelled when compared to patient related cancelation 95%CI [1.049, 12.488].
In our study the third causes of cancellation were medical reasons 41 (18.46%) of which the most common were 34.14% hypertension,24.39% Upper Respiratory tract infection,12.9% acute febrile illness and heart problem similar study done in Ghana komfo anokye teaching hospital were 15.5% due to medical problem (Al Khawalde et al., 2015) and in Ethiopia Asella hospital 25% cancelation were medical related (Dedecho et al., 2020) in Bahrain most common medical reason were hypertension and upper respiratory tract infection (Karashi et al., 2018).
Study done in Nigeria, hypertension and diabetes, recent onset of respiratory tract infections, and acute onset of cardiovascular disorders was commonest reasons (Fatungase et al., 2016). Studies higher than to our result was 67.7% in England St Albans city hospital and 32.6% in American university of Beirut cancelation were medical related reason (Anarfi et al., 2020; Kaddoum et al., 2016). Other study done in Saudi Arabia 9.45% due to Medical related reason which is low (Dhafar et al., 2015). This problem raises from inadequate preoperative evaluation after admission and poor follow up procedure for those who have medical problem. patients who have medical reasons was 2.9 times more likely cancelled than patients who have had patient related cancelation reason 95%CI [1.085, 7.791].
Conclusion
The results of our study are in line with the results obtained in literature sources. Based on the results of our study, we concluded that the percentage of elective cases cancelled on the day of surgery would be high however; more than 60 % of observed cancellation was being potentially prevented Which means appropriate steps could contribute to lowering the presence of cancelled elective surgery.
The most common causes of elective surgery cancelations are shortage of time, facility related, Improper scheduling, lack of ICU beds, COVID 19 related problem, acute and chronic medical illness, unavailability of operating room equipment and lack of important investigations. Effort should be made to prevent elective surgery cancelation by careful planning and organizing of works in a sustainable way.
In general surgeons took longer than estimated time to finish the procedure since the facility is teaching center however, limit the number of teaching resident’s or student and arrange time which is not interfere the operation room efficiency. Share works with responsible and accountable ways for the better outcome of patients and increase operating room efficiency and improve communication among multidisciplinary team. Performed the necessary investigation prior to schedule if the patient with medical problem was detected and appropriate measure would be taken and communicate with concerned staff. Reduce time gap between cases, ensure realistic schedule of patient list and communicate with concerned body before posted.
Footnotes
Acknowledgements
Our deepest gratitude goes to Addis Ababa University, School of Nursing and Midwifery for giving this chance and approval of the study too. Data collectors and respondents were highly acknowledged for investing their precious time for collecting data and providing the necessary information
Abbreviations
IRB: Institutional review board; NHS: National Health System; Oby/Gyn: obstetrics and gynecology; OR: operation room; OT: operating theater; PRE-OP: preoperative care; SPHMMC: St. Paul’s Hospital Millennium Medical College; SPSS: Statistical Package for the Social Science; TASH: Tikur Anbesa Specialized Hospital
Author Contributions
TE, YA, DG, FA was involved in the design of the study, data analysis, and interpretation of the findings, report writing and manuscript preparation of this study. FA, TE, DG and YA was involved in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas by revising, editing, and supervising up to final manuscript preparation
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
Prior to the commencement of data collection, ethical clearance and approval was obtained from the Institutional Review Board (IRB) of the College of Health Sciences of Addis Ababa University. Official letter was obtained from School of Nursing and Midwifery, Department of Nursing (Reference number: CHS/NSG/00/80). The study participants were informed about their rights to refuse, to join, ask any question or withdraw at any time during the data collection process without any fear. After explaining the purpose and possible benefit of the study, oral and written informed consent was obtained from each patient before starting the interview. The information of participants was kept confidential.
Data Availability Statement
The data used during the current study are available from the corresponding author upon reasonable request.