
Abstract
We assessed adherence to and predictors of two components of a telephone-supported self-care intervention for depression among primary care adults aged 40 and above with chronic physical illnesses and comorbid depressive symptoms. Participants received a “toolkit” containing six self-care tools. Trained lay self-care “coaches” negotiated a contact schedule of up to weekly contacts. Study outcomes were levels of completion of the self-care tool and the coach contacts at the 2-month follow-up. Coaches reported the number of completed contacts. In all, 57 of 63 participants completed the 2-month follow-up. Of these, 67% completed at least 1 tool; the mean number of coach contacts was 5.7 (SD = 2.4) of a possible 9 contacts (63% adherence). Higher disease comorbidity and lower initial depression severity independently predicted better tool adherence. Findings suggest that people with chronic physical illnesses can achieve acceptable levels of adherence to a depression self-care intervention similar to those reported for other populations.
Introduction
Depression has increased prevalence in persons with one or more chronic physical illness (Patten, 2005). Among people with depression, the presence of a chronic physical illness is associated with an increased duration of depressive episodes (Broemeling, Watson, & Prebtani, 2008; Kessler et al., 2003; Ostbye et al., 2005; Patten, 2005), greater functional disability and work absences (Stein, Cox, Afifi, Belik, & Sareen, 2006), functional decline (Schmitz, Wang, Malla, & Lesage, 2007; Stein et al., 2006; Stuck et al., 1999; Tinetti et al., 2011), increased use of health care services (Himelhoch, Weller, Wu, Anderson, & Cooper, 2004; Stein et al., 2006; Unützer et al., 1997), greater disease morbidity (Saz & Dewey, 2001; Wells & Burman, 1991), and mortality (Schulz, Drayer, & Rollman, 2002).
Low intensity psychosocial interventions, rather than medications, are recommended for adults with a non-severe depression and comorbid chronic physical illness (National Collaborating Center for Mental Health, 2009). However, access to publicly funded psychologists is scarce in many locations, and wait-lists are long (Lacoursière, 2011; Payne & Myhr, 2010). Individual supported (guided) self-care or computerized self-care treatments based on principles of cognitive-behavioral therapy (CBT) are recommended as a feasible alternative to traditional individual therapy (National Collaborating Center for Mental Health, 2009). Supported self-care interventions appear to be effective in treating depression (Gellatly et al., 2007), although most research has not been conducted in people with chronic physical illnesses. Less is known about the extent to which participants adhere to these largely self-administered treatments.
Better adherence to a range of treatments is associated with improved health outcomes (DiMatteo, Giordani, Lepper, & Croghan, 2002; Kazantzis, Deane, & Ronan, 2000). Adherence is defined as the degree to which a “person’s behavior—taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider” (Sabate, 2003). In a recent systematic review of adherence of supported self-care interventions for depression and anxiety (Simco, McCusker, & Sewitch, 2014), among 40 studies reviewed, 22 (55%) reported any measure of adherence: 18 reported the percentage of participants completing the entire self-care tool (M = 66%, SD = 17); 13 studies reported the amount of self-care tool completed by the average participant (M = 80%, SD = 11.6). Only four studies (18%) reported the frequency of contacts with the self-care guide/case manager. Notably, just one of these studies involved a population with chronic physical illness as defined in the present study. Although adherence to various medical and psychological interventions is often associated with participant characteristics—for example, illness severity, socioeconomic status, and social support (DiMatteo, 2004; DiMatteo, Haskard, & Williams, 2007)—only three studies evaluated the participant characteristics associated with better adherence. Information on predictors of adherence to self-care interventions may help to target people most likely to benefit from this type of intervention, as well as those who may require additional support.
We conducted a feasibility study of a telephone-supported depression self-care intervention among adults aged 40 and above with one or more of six high-impact chronic physical illnesses (McCusker et al., 2012). The intervention had two main components: a toolkit of paper and audiovisual tools, and weekly telephone support from a trained lay self-care coach. Specific objectives of the present study were (a) to assess patient adherence at 2 months to use of the self-care tools and coach contacts and (b) to determine predictors of adherence to these intervention components.
Method
The study was an open, uncontrolled trial, conducted during 2010-2011.
Recruitment/Inclusion Criteria
Recruitment methods have been described previously (McCusker, et al., 2012). Participants were recruited through family physicians’ offices within a manageable travel distance from the study site. Participants were eligible if they were aged 40 or more, diagnosed with one or more of six targeted high-impact chronic physical illnesses (arthritis, hypertension, diabetes, heart disease, chronic obstructive pulmonary disease, and asthma; Broemeling et al., 2008) at least 6 months prior to recruitment, and had at least mild depressive symptoms (Patient Health Questionnaire–9 [PHQ-9] score ≥ 5; Simco, 2012; Spitzer, Kroenke, & Williams, 1999). Patients were excluded if they were suicidal, were receiving counseling or help at least once a month for a mental health problem from any health professional other than their family doctor, were unable to read in either English or French, were more than mildly cognitively impaired (Blessed Orientation Memory and Concentration Test score of 10), or had a physical impairment that would prevent the patient from participating in a self-care intervention (e.g., visual impairment). Short initial screening forms were distributed to patients by their family doctors or office staff to ascertain age, presence of a chronic illness, and possible depression assessed by the PHQ-2 (Kroenke, Spitzer, & Williams, 2003). Initially eligible participants were then contacted by the study research assistant by telephone to confirm study eligibility and invite them to provide written consent. Family doctors of participating patients were instructed to continue with usual care.
Intervention
A multi-disciplinary team of investigators designed and conducted the intervention, which comprised two components: providing patients a toolkit of self-care tools and telephone-based coaching. The tools were classified into three categories: (a) informational tools that provided information on causes, symptoms, and available treatments for depression (e.g., information brochure); (b) cognitive-behavioral tools that included exercises for behavioral activation, cognitive restructuring, problem solving, and/or mood monitoring (e.g., mood-monitoring logbook); and (c) combined tools that included both informational and cognitive-behavioral elements (e.g., comprehensive antidepressant skills workbook).
Six tools comprised the toolkit and were available in English or French. They included (a) an information brochure describing causes, symptoms, and treatments for depression (informational tool); (b) a DVD film titled “Finding a way out of depression” using patient and health care professional testimonials to describe causes, symptoms, and treatments for depression (informational tool; Maher, 2001); (c) a mood-monitoring logbook providing instructions and charts for daily mood monitoring (cognitive-behavioral tool); (d) an antidepressant skills workbook describing causes and symptoms of depression, providing techniques, exercises, and worksheets for behavioral activation, recognition of depressive thoughts, and problem solving (informational/cognitive-behavioral; Bilsker & Paterson, 2010); (e) an action plan in booklet form, based on material in the antidepressant skills workbook, to encourage behavioral activation in five general areas related to self-care for depressive symptoms and chronic illness, including goal-setting techniques and action plan charts (cognitive-behavioral tool; Bilsker & Paterson, 2010); and (f) Internet tools for English-speaking participants, specifically a website, e-couch (developed by the Australian National University), to permit creation of a confidential account, completion of an extensive interactive informational component on symptoms and causes of depression, and access to modules on interpersonal therapy, physical activity, CBT, and problem solving. Worksheets were provided and stored online (informational/cognitive-behavioral; Australian National University, 2009). An informational French-language site was provided as an alternative, as e-couch was only available in English (Briffault et al., 2010).
The role of the coach was to support the participants in using the self-care tools by encouraging them to try different tools and facilitating their practical application. Coaches were instructed to not engage in active therapy (e.g., making personal/behavior change recommendations, linking behavior with mood changes, etc.). Two lay coaches (A and B) were trained using a standardized training manual and supervised by the study psychiatrist (author MGC) and psychologist (author KLL). The coaches offered weekly telephone contacts with each participant for the first 3 months and once per month for the second 3 months. Schedules for each subsequent contact were re-confirmed at the end of each call. For each scheduled contact, a window period of 5 days was designated during which the coach could make a limited number (3 to 5) of attempts to reach the participant. If unsuccessful, that week’s contact was skipped, and the following week’s contact was resumed at the regular time negotiated by the coach and the participant. We audio-recorded all the contacts and randomly reviewed a sample to assess the fidelity of the intervention and to provide feedback to the coaches.
Ethical Issues
Written informed consent was received from all participants. Participants who became severely depressed after enrollment (PHQ-9 score of 20 or higher) were not withdrawn from the study but referred to their family doctor for follow-up. Participants who disclosed suicidal plans after enrollment were withdrawn from the study and referred for appropriate follow-up. The study protocol and consent procedures were approved by the St. Mary’s Hospital Research Ethics Committee.
Potential Predictor Variables
Sociodemographics
Questions were adapted from Statistics Canada’s (2004) Canadian Community Health Survey Cycle 3.1: Educational attainment was a binary variable indicating having obtained at least a bachelor’s degree. Total household income in the previous year, before taxes, in Canadian dollars was classified as 0—no income; 1—less than $30,000; 2—$30,000 to $60,000; and 3—more than $60,000 (Statistics Canada, 2004). Marital status was classified as married/cohabiting versus other.
Physical health
Comorbidity was measured using the self-reported Charlson Comorbidity Index (CCI). For the analysis, scores ≥3 were combined as the same category (Deyo, Cherkin, & Ciol, 1992; Katz, Chang, Sangha, Fossel, & Bates, 1996). Physical health status and functioning were measured by the 12-Item Short-Form (SF-12) Physical Component Summary score (Ware, Kosinski, & Keller, 1996).
Mental health
Depression severity and possible depression diagnoses (major, minor) were assessed with the PHQ-9 (Spitzer, Williams, & Kroenke, 2010). Two anxiety disorders (panic, other) were assessed using the Primary Care Evaluation of Mental Disorders diagnostic tool (Spitzer et al., 2010). Cognitive impairment was measured using the short Blessed Orientation–Memory–Concentration score (Katzman et al., 1983). Mental health status and functioning were measured by the SF-12 Mental Component Summary (Ware et al., 1996).
Health behavior
Physical activity was measured using Godin’s Leisure-Time Exercise Questionnaire (Godin & Shepard, 1997). Social network was assessed using Lubben’s Social Network Scale (Lubben et al., 2006). Activation was calculated using the Patient Activation Measure (Hibbard, Stockard, Mahoney, & Tusler, 2004). Adherence to medical recommendations was determined by the General Adherence Scale (Hays, 1994).
Adherence Outcomes
Self-care tool adherence
Self-reported tool adherence was assessed in a telephone interview by a research assistant, 2 months after the baseline interview. Completion of each tool was recorded on a Likert-type scale 0—none, 1—very little, 2—less than half, 3—more than half, 4—most, 5—all. Adherence to the mood-monitoring notebook was assessed as total number of days during the previous 2 months using a similar Likert-type scale.
A three-level composite ordinal outcome was created prior to data analysis to describe overall tool adherence. The rationale behind the measure was that “high adherence” would constitute significant use of both informational and cognitive-behavioral tool content. Participants with high adherence therefore completed either most to all (i.e., scores of 4 or 5 on the Likert-type scale) of either a combined informational/cognitive-behavioral tool (the workbook or e-couch) or most to all (i.e., scores of 4 or 5 on the Likert-type scale) of both an informational tool (information brochure or film) and a cognitive-behavioral tool (action plan or mood monitoring). Participants with moderate adherence completed most to all (i.e., scores of 4 or 5 on the Likert-type scale) of either an informational or cognitive-behavioral tool. Patients with low adherence completed less than most to all (i.e., scores of 0 to 3 on the Likert-type scale) of all tools.
Coach contacts
Coaches recorded weekly contacts in the coach log book. The number of coach contacts completed at 2 months was categorized prior to data analysis to create an ordinal outcome indicating progressive adherence to the coach contacts schedule. Categories were high (7-9), medium (4-6), and low (0-3) adherence.
Because coach characteristics may have affected participants’ willingness to receive weekly phone contacts, we analyzed a series of dichotomous “yes” or “no” questions evaluating the coaching intervention as (a) too often, (b) too long, (c) about the right amount, (d) helpful, (e) intrusive, (f) supportive, and (g) bothersome. In addition, participants were asked, “Was (coach) helpful in” (a) introducing you to the tools, (b) helping you select the tools, (c) helping you set goals, or (d) helping you select community resources.
Statistical Analysis
To assess the impact of patient characteristics on tool and coach adherence, we used ordered logistic regression with a three-level outcome for each kind of adherence corresponding to increasing degrees of adherence; we tested for proportionality of odds ratio for both outcomes (Hosmer & Lemeshow, 2000). All patient variables were pre-screened by fitting univariate ordinal logistic regressions (Hosmer & Lemeshow, 2000); only variables with a p value of .25 or less were retained for use in multivariate model building.
The model for each outcome was constructed by stepwise selection with backward elimination (Hosmer & Lemeshow, 2000). The proportional odds assumptions were tested in the final models using the likelihood ratio test and also the Brant test (Long & Freese, 2005; Wolfe & Gould, 1998). Multiple imputation was used to handle missing predictors (Graham & Schafer, 1999; Rubin, 1976; Schafer & Graham, 2002; Schlomer, Bauman, & Card, 2010).
All analyses were conducted using Stata 11 (StataCorp, 2009).
Results
The recruitment flowchart is shown in Figure 1. A total of 254 patients completed the initial screening questionnaire, of whom 165 (65%) completed the telephone screening. Of the 165 who completed the second screening questionnaire, 98 were eligible and provided verbal consent. Of the 63 fully consenting participants, 57 (90%) responded to the 2-month questionnaire. Participant characteristics indicate an older, mostly female, and sicker sample—as the physical and mental health status scores were below age-adjusted Canadian national averages, and comorbidity scores were high (Table 1; Hopman et al., 2000).

Study sample flow diagram.
Participant Characteristics (n = 57).

Note. Income: 0 = no income; 1 = less than $30,000; 2 = $30,000$60,000; 3 = more than $60,000; Charlson Comorbidity Index categorized as 0, 1, 2, 3 (3+).
Imputed data variable.
Imputation for less than 5% of the sample.
Imputation for 14% to 33% of the sample.
Self-reported completion rates of each tool are shown in Table 2. Viewing the DVD film had the highest completion (51%) and the Internet tool the lowest (3.5%; Table 2). Sixty-seven percent (38) of the participants completed all of at least one tool; 21 of those 38 participants completed all of 1 or more behavioral tools (mood-monitoring logbook, action plan, workbook, e-couch). Of the remaining 19, 17 started but did not complete any tool, and 2 did not start any tool. Tool adherence was classified as high for 42% of the participants and low for 23%. Mean (SD) coach contacts completed was 5.7 (2.4) out of a maximum possible of 9 (63.3%). Adherence to coach contacts was classified as high for 42% and low for 18% of the participants. The correlation between the ordinal self-care tool adherence variable and total number of completed coach contacts was r = .36.
Measures of Adherence to Self-Care Tools and Coach Intervention Components (n = 57).

Following univariate screening, four variables were included in the stepwise selection procedure for prediction of the ordinal tool adherence outcome: sex, social networks, comorbidity, and depression severity. Table 3 presents cumulative odds ratios representing the odds of being in a higher adherence category compared with a lower category. Statistically significant predictors of higher adherence in the multivariate model were higher comorbidity and lower severity of depression symptoms. A 1-point increase in comorbidity score (capped at ≥3) was associated with a 1.67-fold increase in the odds of higher adherence. A 1-point increase in depression severity score was associated with an 11% decrease in the odds of higher adherence.
Results of the Ordinal Logistic Regression Model for Self-Care Tool Adherence (n = 57).
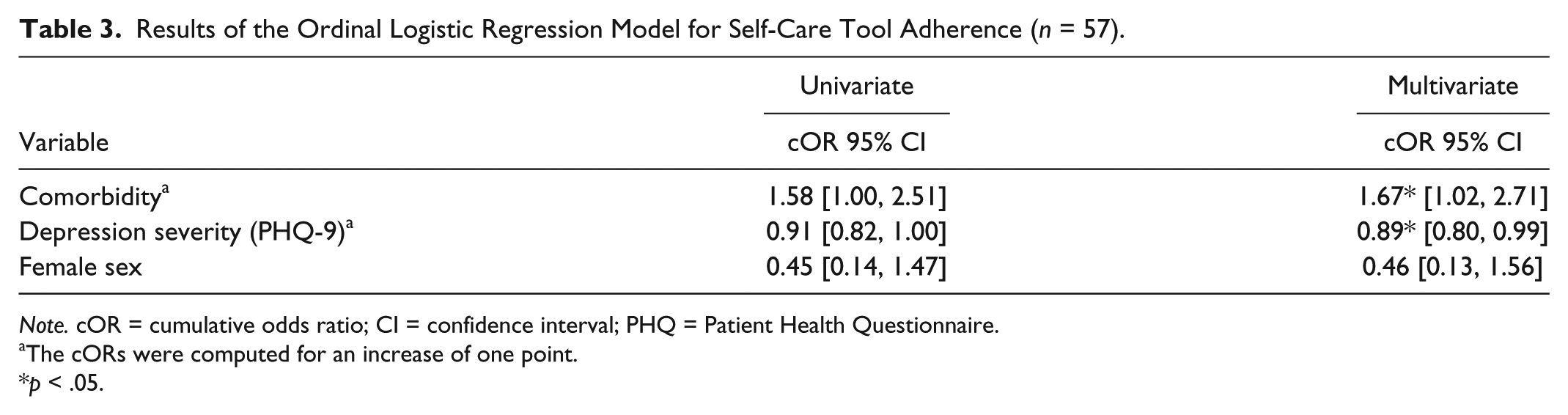
Note. cOR = cumulative odds ratio; CI = confidence interval; PHQ = Patient Health Questionnaire.
The cORs were computed for an increase of one point.
p < .05.
Five variables (comorbidity, minor and major depression diagnosis, assigned coach, and physical activity) were included in the stepwise selection for prediction of the ordinal coach adherence outcome: Assigned coach, minor and major depression diagnosis, and physical activity were included in the final model, presented in Table 4. Only assigned coach was a statistically significant predictor in the multivariate model: Participants assigned coach B had 4.5-fold increase in odds of higher adherence (p = .001). Means (SDs) of completed coach contacts for Coaches A and B were 5.1 (2.5) n = 32, and 6.5 (2.2) n = 25, respectively.
Ordinal Logistic Regression for Self-Care Coach Contact Adherence (n = 57).

Note. Physical activity: Godin’s Leisure-Time Exercise score. cOR = cumulative odds ratio; CI = confidence interval; PHQ = Patient Health Questionnaire.
PHQ-9.
The cOR was computed for an increase of one point.
p < .05.
Although evaluations of patient perceptions of the two coaches revealed no significant differences, trends suggested that Coach B was perceived to be more helpful with introducing the tools (100% vs. 93%), helping participants set goals (87% vs. 68%), and referring participants to community resources (68% vs. 36%) compared with Coach A. However, Coach B was also rated as more intrusive (20% vs. 11.5%) and bothersome (20% vs. 3.6%) than Coach A. The audiotaped recordings provided complementary information, indicating that although both coaches adhered to the coaching guidelines, Coach B was generally more enthusiastic than Coach A and gave liberal praise to the participants.
Discussion
Using an open, uncontrolled intervention study design, we investigated adherence to a telephone-supported self-care depression intervention in persons aged 40 and above recruited from primary care practices with depressive symptoms and comorbid chronic physical illnesses. Overall, 67% of the participants reported completion of at least one tool, and mean completion of coach contacts was 63%. Lower initial depression scores and higher comorbidity scores were predictors of better self-care tool adherence. Patient characteristics did not predict adherence to coach calls. Moreover, as the number of coach calls differed between the two coaches, coaching style may be important in mediating patient use of the support component of the intervention.
Sixty-seven percent of the participants completed at least one entire tool in the toolkit, which was similar to the mean completion of 66% found in our systematic review of self-care interventions for depression or anxiety (Simco, et al., 2014) and somewhat higher than the median percent completion of 56 reported in a systematic review of 36 studies of computerized CBT interventions (Waller & Gilbody, 2009). We cannot compare the low completion rate of our computerized CBT tool directly to the results of the latter study, because we presented participants with multiple tools, and they could select the tool(s) that most appealed to them. Completion of individual tools ranged from a high of 51% for the DVD film and a low of 3.5% for the Internet tool, suggesting low acceptability to the latter in this population.
The composite tool adherence outcome suggests that, globally, the self-care intervention was acceptable, with 77% of the participants included in the moderate-to-high adherence categories. Two predictors of better tool adherence (greater physical comorbidity and lower depression severity) also predicted better adherence to other types of medical treatment according to published meta-analyses (DiMatteo et al., 2002; DiMatteo et al., 2007; DiMatteo, Lepper, & Croghan, 2000). Greater physical comorbidity may increase motivation to engage in self-care. However, greater severity of depressive symptoms is associated with lower motivation.
To our knowledge, no previous study has reported data on adherence to the self-care coach component of self-care interventions. Eighty-two percent of the participants completed a third or more of possible coach contacts; 42% completed two thirds to all of possible contacts, indicating the acceptability of the coaching intervention was limited and coach-dependent. Importantly, however, there was only a modest correlation between tool adherence and the number of coach calls, and no differences in tool adherence between the two coaches. Our data on patient perceptions of the coaches suggest that differences in coaching style may have affected the relationship developed between the coach and the patient (Dobkin, Sita, & Sewitch, 2006; Sewitch et al., 2004). Further research is needed on the characteristics of coaches that improve intervention adherence. Notably, we have reported from this same study that adherence to the behavioral tools—but not the number of coach calls—was associated with better clinical outcomes (McCusker, et al., 2012). Further research is also needed on whether the provision of coach support increases adherence to and outcomes of self-care interventions for depression, and on the optimal number of coach contacts needed.
Limitations
Self-reported adherence was assessed retrospectively and was subject to recall and social desirability biases, which likely overestimated tool adherence. However, self-report is unavoidable when using non-electronic self-care tools. For tools requiring mood or activity logging, reporting the number of entries made might have improved accuracy. We did not collect data on why participants chose to use or not use a given tool. Small sample size and the resulting low statistical power limited the number of variables that could be entered into the prediction models (Hosmer & Lemeshow, 2000). The highly selected patient sample may also limit the generalizability of our findings.
Implications
Our findings on adherence to both the self-care tool and coach components of our intervention are promising for the use of this intervention in the targeted population. Further research on depression self-care interventions is required to confirm our findings in larger patient samples of adults with depressive symptoms and chronic physical illnesses. We recommend that adherence to both the self-care coach and self-care tool components be reported in future studies. Additional areas for future research include examining the contributions of the two intervention components to patient outcomes and the characteristics of coaches associated with better intervention adherence and outcomes. We have an ongoing randomized trial that aims to compare a supported versus an unsupported depression self-care intervention (McCusker, 2012).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the Fonds de la Recherche du Québec–Santé (FRQS) [Grant 16384], May 2009 to April 2013. Erin Strumpf was supported by a Chercheur Boursier Junior 1 from the FRQS and the Ministère de la Santé et des Services sociaux du Québec. Maida Sewitch was supported by a Chercheur Boursier Junior 1 from the FRQS.