
Abstract
Making contextual gender analysis helps to design strong evidence-based institutional strategies for reversing stereotypes that are embedded in the organizational culture. Hence, an institutional-based cross-sectional study was conducted on 401 participants to assess gender equality and workplace harassment among staff members of Haramaya University, College of Health and Medical Sciences, and Hiwot Fana Comprehensive Specialized Hospital, Eastern Ethiopia from November 1 to 30, 2021. Data were collected through a self-administered semi-structured questionnaire. We measured gender equality perception by indicators as a latent variable. To identify predictors of gender equality, a structural equation model fit and a coefficient of regression with 95% CI were used to report the association. Of the total participants, more than 85.5% were female, 36.7% had a bachelor’s degree, and about 56.6% were administrative staff. Only 0.5% had a managerial role. The perception of gender equality was predicted positively by political (β = .21, 95% CI: [0.10, 0.31]), institutional (β = .32, 95% CI: [0.09, 0.55]), and sociocultural (β = .18, 95% CI: [0.11, 0.26]) factors. The proportion of workplace harassment in one form of violence ranged from 15.2% to 39%. Preferring dialog to get a solution (9.7%) and the unavailability of a gender office at the hospital (7.5%) were the main reasons for not reporting acts of violence. The findings of this study fortify gender inequality in the health and medical institute of Haramaya university but these disparities were not reported by the participants. A decent workplace, free from harassment and discrimination, has to be set up by implementing the existing gender policies and by designing contextualized strategies.
Plain language summary
Gender refers to culturally specific arrangements and presumptions on the nature and character of men and women. These are manifested in several ideas and practices, which influence the identity, social opportunities, and life experiences of human actors. As a result, institutional cultures, mission statements, strategies, leadership styles, coordination, and staff profile are often gendered and dominated by patriarchal beliefs and attitudes to different degrees. Therefore, gender equity and equality can be ensured with the consideration of the gendered consequences of all actions, the gendered social relation, and power relations. Moreover, Gender-Based Violence is highly prevalent among health professionals, health sciences students, and patients. However, the health sector is lacking conceptual clarity and practical tools to address key challenges to gender mainstreaming. Therefore, this study aimed to assess gender equality and workplace harassment among staff members at health institutions in eastern Ethiopia. The result of this study showed the perception of gender equality was predicted by political, institutional, and sociocultural factors. The proportion of workplace harassment in one form of violence ranged from 15.2% to 39%. Preferring dialog to get a solution and the unavailability of a gender office at the hospital were the main reasons for not reporting acts of violence. The findings of this study fortify gender inequality in the health and medical institute of Haramaya university but these disparities were not reported by the participants. A decent workplace, free from harassment and discrimination, has to be set up by implementing the existing gender policies and by designing contextualized strategies. This survey was strong in presenting gendered analysis and gender-based violence in health and medical institutions in higher education sectors. However, the impacts of gender equality determinants could not be seen in this short study period.
Introduction
The Millenium Development Goal (MDG) 3 was dedicated to women’s equality and women empowerment in the year 2000 when the United Nations agencies in the presence of 189 countries drew the eight MDGs (Kabeer, 2005). Later, the Sustainable Development Goals (SDGs) were drafted, which had three major pillars: social development, economic development, and environmental protection (Franco et al., 2020). The document emphasized that one of the pillars, social development, cannot be realized without the equality and involvement of women (Bayeh, 2016). However, gender equality is disproportionate at all levels.
In line with the global health and workforce, strategies are identifying the critical importance of addressing the gender equality problems of the health workforce as key to achieving universal health coverage by 2030 and capitalizing on women’s economic empowerment and participation (Horton, 2015; Kim & Evans, 2015; C. Newman, 2014). Addressing gender and inequalities in the health system is indispensable not only for recognizing SDG 5 (gender equality) and SDG 3 (health and well-being) but also for understanding other SDGs, such as SDG 4 (quality education) and SDG 8 (decent work and inclusive economic growth) (Franco et al., 2020; Langer et al., 2015).
In Ethiopia, over the years, various policies, directives, and proclamations have been passed to narrow the gender gap (Baye, 2021). The progressive affirmative actions and policies have had significant contributions to closing gender parity in the number of girls that enter primary and secondary schools (Ministry of Education, 2015). Nonetheless, up the educational ladder, female representation has tended to be less and less. The number of Ethiopian female students that have been enrolled in higher education and especially in the Science, Technology, Engineering, and Math (STEM) field is small (Egne, 2014; Olkaba, 2019). Moreover, the dropout and dismissal rate is higher for women compared to their male counterparts. In addition to the field of study, the gender gap gets higher as the academic level increases. For example, the gap is 42% in the undergraduate program, while it is 84% in Ph.D., and post-collegiate states and the number of women that get access to become faculty is very low (Kassie, 2018).
Women’s participation in key decision-making positions in Ethiopian Higher Educational Institutions (HEIs) has also been minimal (Kvach et al., 2017). Although women’s representation in the lower pyramid of leadership positions has increased, their representation at the middle level is low and it is insignificant at the top levels (Kvach et al., 2015). In addition, gender disparity is observable in access to capacity-building opportunities and networking. This contributes considerably to the low representation of female staff in research and academic publications (Mengesha & Shaleka, 2018). For instance, only in 2006, that the first female author appeared in the Ethiopian Journal of Development Research (EJDR), a journal that had already been established in the 1970s; and still female authors appeared in less than 15% of the issues. Added to the capacity-building issues, low representation in publications plays a key role in constraining female faculty’s advancement on the academic ladder and gender disparity in leadership (Mengesha, 2017).
To rectify the gender disparity in leadership, the Ministry of Science and Higher Education (MoSHE), in collaboration with the government’s Education Sector Development Program, ESDP V (2015–2019/20), is implementing guidelines to improve female representation in leadership positions. The ESDPV’s target is for 50% of the top leadership positions to be filled by women, with at least one woman president in public universities. Although most presidents are male, the number of vice presidents has risen to 29, making up 16.27% of top leadership positions (Ministry of Education, 2015). Still, the implementation of the ESDPV guide on gender and leadership is not consistent across all HEIs, and neither is the enforcement mechanism in place. The guide itself has a limitation: it focuses only on representations, which does not necessarily result in attracting attention to address other gender concerns such as gender-based violence (GBV) in the HEIs, though various international gender-based agreements have been ratified and integrated into the health sector by the country. Some gender scholars have criticized the mere focus on representation on two grounds: (1) it ignores important differences between women and men as potential actors, and (2) it limits gender concerns to representation and undermines structural power relations. Gender refers to culturally specific arrangements and presumptions on the nature and character of men and women. These are manifested in several ideas and practices, which influence the identity, social opportunities, and life experiences of human actors. Due to this, gender and inequality cannot be addressed by just adding women to leadership positions.
Moreover, gender inequality influences workplace violence (C. J. Newman et al., 2011). Workplace violence generally refers to interpersonal aggression, sexual harassment, bullying, and other forms of discrimination and oppression (Van De Griend & Messias, 2014). Across the world, 35% of women fall victim to direct violence at the workplace, and of these between 40% and 50% are subjected to unwanted sexual advances, physical contact, or other forms of sexual harassment (Morris & Pillinger, 2016). It is also highly prevalent among health professionals, health sciences students, and patients (Ellsberg & Heise, 2005; García-Moreno et al., 2015; Parsons, 2020). Exposure to workplace GBV can affect women’s mental and physical health and work productivity in higher educational settings.
Developing countries where violence against health care professionals occurs commonly need more doctors as well. Doctors need to feel safe before they can effectively care for their patients. Thus, policies and implementable strategies are required to ensure a safe working environment to strengthen the services and prevent the loss of morale and emigration of trained healthcare personnel (Kumari et al., 2020). The assessment of risk factors, development and implementation of workplace violence programs, and addressing under-reporting of violent episodes have been suggested as some successful organizational mitigation strategies. Management of workplace violence might include the development of participative, gender-based, culture-based, non-discriminatory, and systematic strategies to deal with issues related to violence (Mayhew & Chappell, 2007). Effective gender mainstreaming and women empowerment activities could also boost addressing these issues in the health sector. However, the health sector is lacking conceptual clarity and practical tools to address key challenges to gender mainstreaming (Bergen et al., 2020; Jebessa et al., 2015; Melese, 2019).
Therefore, gender equality can be ensured with the consideration of the gendered consequences of all actions, the gendered social relation, and power relations (Dorfman et al., 2012). Besides, decision-makers need to understand the institutional gender dynamics and learn from previous efforts for addressing gender-specific needs (Kvach et al., 2015). Awareness of the structural dimensions of gender equality can also help challenge the gender stereotypes that are embedded in the institutional culture (Colbert, 2010; Yigeremu et al., 2021).
Institutions are a mirror image of society: social beliefs guide individuals’ and groups’ behavior, including who does what? Who gets what? how things have to be done, what is expected of them, and how to achieve certain things (Morrill, 2008). As a result, institutional cultures, mission statements, strategies, leadership styles, coordination, and staff profile are often gendered and dominated by patriarchal beliefs and attitudes to different degrees (Dorfman et al., 2012; Halford, 2018).
At the institutional level, Haramaya University (HU), and the College of Health and Medical Science (CHMS) have already taken steps to mainstream gender in their works. These include making the gender office be headed by academic female staff, involving her as a member of the academic committee, and implementing gender policy during staff recruitment and student department selection. Over fifty female and male faculty members participated in Gender-Responsive Pedagogy training (GRP). But, the college lacks enabling strategies to incorporate gender concerns into its work procedures, work ethics, and in its overall structure and system. This can make gender mainstreaming efforts less effective. This may be attributed to a lack of study considering the essential structural dimensions of gender equality within the institutions. Besides, the lack of enforcement mechanisms in place, the design, and implementation of activities have not been assessed from a gender perspective. Moreover, the effect of the efforts of gender equality so far has not been assessed.
Hence, the key signature of this study is to facilitate evidence-based interventions toward gender equality and women empowerment. Moreover, the result will create awareness and strengthen gender sensitivity in health and medical education in the country in general and CHMS in particular. Therefore, this study aimed to assess gender equality and workplace harassment among staff members at Haramaya University, College of Health and Medical Sciences, and Hiwot Fana Comprehensive Specialized Hospital, Eastern Ethiopia.
Literature Review
Gender in the Health and Medical Sector
The Concept of Gender and Sex
Gender refers to socially ascribed roles, responsibilities, behavior, performance, and ownership that are deemed to be appropriate for women, girls, men, and boys (Wood & Eagly, 2012). In medical sciences, the term gender is often interchangeably used with the terms sex (Verdonk et al., 2009). In social sciences, women studies literature, gender is different from sex which represents biological differences between men and women, that is, chromosomes, internal and external sex organs, and secondary sex characteristics as well as hormonal makeup (Muehlenhard & Peterson, 2011; Zieminska, 2018). The gender concept is also different in its features evolved from the nature-culture debate, with the belief that sex is unchangeable, where gender is constructed, and as such amenable to change (Bock, 1989; Cornwall & Lindisfarne, 2003). Some feminist scholars argue that biological explanations for differences between men and women are doubtful because biology has long been abused to legitimize the submission of women, for instance, because women were supposedly ruled by their bodily cycles (MacKinnon, 1983). Others argue that the concept of gender was not introduced to question biological differences as such, but rather to question biological explanations for the social difference (Guimond et al., 2007). However, the degree to which a health phenomenon is specifically social or biological cannot always be distinguished (Risberg et al., 2003). For instance, gender differences in responses to pain may be related to physiological mechanisms of the brain or psychosocial factors or both. As result, it has been suggested that all features of sex and gender be included in health and medicine to get a clear understanding of health determinants (Ostlin et al., 2006). Moreover, it has been identified that instance female and male health professionals do not necessarily have the same ideas about the characteristics of the ideal physician (Verdonk et al., 2009).
Gender Equality in the Health and Medical Sector
According to the ILO report, more than 234 million workers in the world are in the health and social care sectors (Kuhn et al., 2018). Of the global health and social care workers, about 70% are female (WHO, 2019) and deliver care to around 5 billion people (Langer et al., 2015). However, women’s contribution to the sector is undervalued and unrecognized as women are concentrated at a lower status, low paid, and unpaid roles (Langer et al., 2015; WHO, 2019).
The high representation of women in the health workforce is not reflected in the leadership potions. Women are underrepresented within top institutions, in global policy and governance forums, in thought leadership panels, and across decision-making structures in the public and private sectors (Dhatt et al., 2017).
The gender gaps are more visible in executive government positions (Morley, 2014), for instance, as of 2020, only 44 women worldwide were serving as Ministers of Health—less than half the number of women serving as Ministers of Children, Youth, and Family. Out of the 54 countries in Africa, only 13 countries have women health ministers. In addition, women’s representation at the biggest table of decisions, the World Health Assembly, declined from 31% (in 2017) to 23% (in 2020). The same is true in health-funding agencies (Finkel et al., 2023; Ijeoma, 2022; Milletler, 2020).
Globally, there has also been a systematic gendered occupational segregation; most physicians, dentists, and pharmacists are men while women are the vast majority of the nursing and midwifery (Bruce et al., 2015; Butkus et al., 2018; Risberg et al., 2003; Shin & Lee, 2020; Stephens et al., 2020; Theobald et al., 2004). The same is true in Ethiopia (Kibwana et al., 2016) where the female health workforce is dominant in the health extension work, which is mainly the program designed in a way to attract more women than men (Maes et al., 2015; Women, 2014).
Moreover, despite the high demand for healthcare services by women in Ethiopia, females’ representation as higher and middle-level professionals is low in the country (Kibwana et al., 2016). In addition, the minister of health in Ethiopia, Dr. Lia Tadesse in her speech mentioned that in spite of the increase of females in the health sectors, their representation in leadership positions is not to the desired level. Although the rate of women’s involvement in the healthcare leadership of the country is very slow at all levels, the impact of proven track records of performance in the health sector with the appointment of a female health minister is expected to increase female leadership in the sector.
Gender inequality in the health sector has implications for societal health (Javadi et al., 2016). For instance, women are a majority in the health work workforce but the hurdles to advancing to leadership positions affect their motivation and job satisfaction to provide proper healthcare services (C. Newman, 2014). Female leadership is imperative for sustainable development (Olonade et al., 2021). Evidence supports the link between female leadership and initiatives that improve women’s socioeconomic life (Javadi et al., 2016).
Factors Influencing Gender Equality in Health and Medical Sectors
Various factors are contributing to gender inequality in the health and medical sectors as identified from the literature. In the following sub-section, these factors are presented and discussed.
Women’s Employment Rights and Protection Legislation
Women’s employment rights in many countries are not protected by legislation governing critical areas such as equal pay for equal work, non-discrimination, and collective bargaining (Cantillon & Teasdale, 2021). According to World Economic Forum and Word Bank reports (2018), some countries still ban women from working night shifts and involving in certain jobs such as construction and agriculture. The reports also show that 104 economies have labor laws that limit the types of jobs women can assume, and when and where they are allowed to work. As a result, the employment choices of 2.7 billion women are affected. There are no laws to stop sexual harassment in the education sector in 123 countries, 45 countries lack domestic violence laws, and there is no workplace harassment legislation in 59 countries. Moreover, husbands have the legal right to prevent their wives from working in 18 countries and the right to prohibit them from registering a company in four countries (Iqbal, 2018). Most of these countries are located in Sub-Saharan Africa and the Middle East and North Africa (Kelly & Breslin, 2010).
Where legal instruments for promoting gender equality and protecting women workers’ rights exist (Goulovitch et al., 2020; Women, 2021) there is still a gap between the rights set out in national and international standards and their implementation in real situations. Although many countries have laws starting non-discrimination in employment based on gender, only 76 mandate equal remuneration for work of equal value, and 37 economies have no laws protecting pregnant workers from dismissal (ILO, 2012; Iqbal, 2018). In addition, most women across the world are unaware of the legal protection that can help them combat discrimination and fight for a fair balance of opportunity, treatment, pay, and equal representation in all areas of paid and unpaid employment and work-related decision-making. And these become the greatest challenge for women to exercise and fight for their rights (International Labour Organization, 2000).
Access of Girls to Education and Training for Formal Health Sector Jobs
Unequal access of girls to education in many low- and middle-income countries, particularly to secondary schooling, has limited women’s access to training for formal health sector jobs (Leach, 1998). Education can have a major impact on the lives of girls and women, boys and men. The social and economic benefits of education are well-known for a long; also, the advantages of education that girls and women can draw upon. Education is crucial in changing attitudes into accepting gender equality as a fundamental social value. It also ensures the ability to exercise rights. Education is vital for women’s empowerment as it enables them to involve in social, economic, and political domains (Sundaram et al., 2014).
However, gender gaps in access to quality education and performance mainly post-primary level still prevail in developing countries (Jannah, 2020). This constrains girls’ participation in key and growth-enhancing fields of education such as science, technology, engineering, and mathematics (Tinuke, 2012). Consequently, women’s representation workforce such as health sectors mainly middle and high-level professions become very low.
Following the pipeline theory, the under representation of women in higher education attainment such as health and medical college and the high and middle-level health professions make a significant contribution toward the huge gender gaps at top leadership positions (Al-Qahtani et al., 2020).
Women in the health sector as compared to men lack experience and access to a job opportunity that can lead them toward the senior leadership position. Moreover, in the workforce where women are not statistically disadvantaged in number such as in the health sector but seem systematically lower at the hierarchical level, it could be a result of lower starting positions for women than for men. The limitation with the lower starting points is that it takes longer to be in the higher ranks and is associated with a lower likelihood of advancing to the top leadership.
Gender Stereotypes and Occupational Segregation
Gender stereotypes and prevailing social norms create occupational segregation- sorting men and women into different kinds of jobs. Gendered occupational segregation is when there are women-dominant or men-dominant occupations that are based on gender norms. Studies show that the workforce in organizations and hierarchy is still segregated by gender, and reinforce gender inequality in status and pay (Breda et al., 2020).
When one gender dominates a job it creates “an archetype” of the worker in that profession and develops normative domination- then nurture characteristics needed to be successful in that profession. As a result, while an incompatibility between the gender stereotypes of an individual and the gendered occupational stereotypes of their profession is found, bias and employment discrimination can manifest (Breda et al., 2020). In the health sector, nursing is predominantly a women’s job with men accounting for only 10% of those entering the profession, whereas men hold the majority of jobs in surgical specialties (WHO, 2019).
Male Bias Systems and Work Conditions
Health systems and work conditions have been established to suit men’s life patterns and not women’s; for example, many health workers have no paid parental leave entitlement (WHO, 2019). This sector was developed based on bureaucracy and hierarchy, like that of a manufacturing plant, and change is not visible from where it was half a century ago (Oliveira et al., 2020). As a result, the preferred leadership styles especially in the medical sector are masculine such as competent, assertive, and decisive, whereas characteristics strongly associated with women such as modesty, cooperation, and emotiveness, are often seen as incompatible with strong leadership. The positive bias toward masculine attributes provides men opportunities for success, and the less favorable perceptions of feminine attributes may result in women being excluded from access to similar opportunities. For instance, professional hierarchies play a role in the appointment of health leaders in Kenya which is shaped by gender that medical doctors who are often male tend to be preferentially selected for leadership positions. In the study by Kvach et al. in Ethiopia, female respondents mentioned a lack of female role models such as female heads of departments as one of the key barriers (Kvach et al., 2017).
Lack of Political Will and Institutional Support
Political will is one of the key requirements to effectively mainstream gender in any program, project, curriculum, and research among others (Lombardo & Mergaert, 2013). Political commitment is not only indicated by a high level of support by the decision-makers but also by the allocation of financial resources and time to address gender inequality in the sector. According to the WHO, gender equality activities in the health sector are lacking the political will and lack of decision-makers in health systems to adopt the gender-transformative leadership and measures necessary to drive equality among people of different genders (WHO, 2019).
Resistance to Gender Equality Initiatives
Gender equality initiatives or activities likely trigger resistance or opposition and result in the ineffective implementation of gender mainstreaming (Lombardo & Mergaert, 2013). Resistance is often aimed at maintaining the status quo and opposing gender equality activities that require a change in the norms, practices, and assumptions concerning the relationship between women and men that work at the level of individuals and institutional actors. Gender issues may cause resistance which is due to political-ideological connotations of gender matters (Verdonk et al., 2005). As cited in Verdonk et al. (2009), identified resistance to gender issues by medical students ranging from denying to dismay. Denial exists when those believe that they haven’t experienced gender inequality, and if do not notice gender inequality, it must not exist. For example, in the study by Kvach et al., most of the female medical faculty in Ethiopia mentioned that they did not feel that their gender had been a disadvantage or an advantage to their careers. Gender issues may also be reduced within the hierarchical scale of worthwhile knowledge. Individuals also distanced themselves from dealing with gender issues when problems are blamed on an unchangeable factor. Dismay occurs when confusion is overwhelming and no solutions are seen (Kvach et al., 2017). However, a study in Sweden’s medical school shows that integrating gender in the medical curricula was found to be more interesting for female students than male students as it met the needs of the former than the latter, implying the gendered nature of medical sector (Hamberg & Johansson, 2006). Another study in the same medical school found that more female physicians found gender important in their profession than male physicians (Risberg et al., 2003).
At an institutional level, traditional health and medical school perceive health as the absence of disease- form a resistance to change norms which result in gender inequality in the sector (Verdonk et al., 2009). Institutional norms that focus on preserving boundaries and maintaining traditional beliefs of reductionism and objectivity constrain the implementation of gender equality activities. Yet, the belief that medical knowledge is neutral and objective does not hamper the uptake of (biomedical) sex difference, rather these issues indeed risk being cut loose from their gendered roots.
Work-Family Conflict
In most societies across the world, domestic roles are reserved for women regardless of their responsibilities in the public arena (Lyu et al., 2019). As a result, the disproportionate responsibility of women’s domestic chores and care roles is a potential reason for the delay in their career advancement and under-representation in leadership. Studies from the developed country show that women physicians have more family workload, reported higher work-family conflicts, higher incidence of burnout and emotional exhaustion, and demonstrated a negative association of parenthood with career routes (Baptiste et al., 2017; Dyrbye et al., 2011). Evidence also shows that some women self-select themselves out of leadership positions due to work-family conflict and adversely affect their career advancement by prioritizing domestic care roles over career roles when the two are in conflict and difficult for them to balance, mainly to meet gender role expectations (Couzy, 2012).
Gender Discrimination, Biases, and Sexual Harassment
Gender discrimination is when individuals are treated differently or less favorably because of their sex, or gender identity (Carr et al., 2000; Parsons, 2020). Not all of the discriminations are intentional or explicit. Gender discrimination is often systemic, unintentional, and subtle (Togioka et al., 2021). Policy and practices such as job requirements that mention nothing about gender may end up denying a job opportunity, paying less, and firing as a result of systemic discrimination (C. Newman et al., 2017).
Sexual harassment includes generalized sexist remarks, behaviors to coercive sexual advances, unconscious patronization, and subtle ambiguity to obvious sexual threats (Parsons, 2020). Literature from developed countries such as the US shows that female physicians encounter more gender discrimination and sexual harassment than female physicians in the community (Butkus et al., 2018). Female physicians, even those in positions of authority in medical schools, perceive a considerably more hostile environment than their male colleagues, and gender discrimination and sexual harassment contribute substantially to these perceptions. Studies also show that females are more likely than males to avoid surgical careers based on the belief that surgical personalities and the persistence of old boys’ mentality (Bruce et al., 2015). According to WHO report, female health workers face a burden of bias, discrimination, sexual harassment, and violence not faced by their male counterparts, and often not recorded or addressed (Hingle et al., 2018).
A report from India stated about 50% (49.5%) of respondents had experienced GBV in their workplace where 47.3% faced emotional violence and 14.8% faced sexual violence (Kaphle et al., 2015). An institutional-based cross-sectional survey conducted on female staff from public and private universities in Nigeria showed the prevalence of workplace incivility, bullying, and sexual harassment (SH) was 63.8%, 53.5%, and 40.5% (Agbaje et al., 2021). In addition, 39% of health workers had experienced some form of workplace violence in Rwanda.
Stalking is the most prevalent form of abuse at work. It poses risks to the physical safety of workers, co-workers, and customers/clients can lead to property damage, and can negatively affect productivity and morale. In addition, employers could be held liable if an employee uses work time and resources to engage in stalking. Stalking often indicates an increased risk of fatality for those who experience it. According to a 2015 survey by the Centers for Disease Control and Prevention, nearly one in six women (19.1 million) and one in 17 men (6.4 million) in the U.S. were survivors of stalking at some point in their lifetime. In one study, the majority of the women (74.2%) reported that the stalking partner had interfered with their employment more than one-half (58.7%) experienced work disruption or a diminished ability to obtain or maintain employment (Morris & Pillinger, 2016).
Lack of Data and Research to Highlight Gender Gaps
According to the WHO, the lack of data and research is constraining to highlight gender gaps in critical areas and driving accountability and policy change. Lack of evidence also triggers gender blindness and creates a situation where the differences in needs and interests between men/boys and women/girls are overlooked in the health and medical sectors. Clinical research often excludes female patients due to reproductive health and associated costs, and this results in a lack of female knowledge (Clark et al., 2002). It has also been argued that medical curricula and research have not been transformed based on gender research, research on women’s health issues, and the growing numbers of female students in medical school (Verdonk et al., 2009).
As result, gender differences are concealed and a male norm is apparent in the sector. Lack of recognition of gender differences in medical and health research and curriculum can lead to the absence of a strategic focus and resources dedicated to addressing the gender imbalance in the sector (Ann Keogh Hoss et al., 2011).
Moreover, to date, violence against women and girls (VAWG) studies in Ethiopia are limited in number and scope, and most existing VAWG studies have been conducted at the subnational/regional or community levels. There have been very few national and/or population-based prevalence studies on VAWG in Ethiopia. The 2016 Ethiopia Demographic and Health Survey (EDHS) was the first national population-based study that included a focus on VAWG, particularly women’s experiences with domestic violence since the age of 15. Prior to the 2016 EDHS, comprehensive data on VAWG in Ethiopia was not available (Handebo et al., 2021). Internal policy dialogs, the strengthening of national capacities, and statistical systems for data collection and reporting would lead to more gender-responsive programing and resource allocation (Dayanandan, 2014).
Methods
Study Area and Period
The study was conducted in CHMS and HFCSH of HU from November 1 to 30, 2021. Both the college and its teaching hospital- Hiwot Fana Comprehensive Specialized Hospital which is the biggest referral hospital in the eastern region of Ethiopia, are in Harar town, about 23 km from the main campus. The college was established in 1996 under the long-term plan of the government and mandate given to Higher Education Institutions to train competent health professionals. The total number of academic staff is 414 (69 are female), with no female associate and professor academic rank. There is also 1,074 administrative staff. The hospital has 568 (308 female) healthcare professionals and 452 administrative staff. The CHMS trains health professionals at both graduate and undergraduate levels. Currently, it is running 26 MSC, 20 undergraduate, 10 specializations in medicine, and 4 PhD programs. The total student population in the college is 2,716 (858 females) (Haramaya University Webpage, 2022).
Study Design and Population
An institutional-based cross-sectional study was employed, using a quantitative method. The population for this study was permanent academics, health professionals, administrative, and supportive staff of CHMS and HFCSH at Haramaya University. Individuals available at the time of the data collection were included while those with mental illness and communication problems were excluded.
Sample Size Determination and Sampling Technique
A single population proportion formula was used: since there was no data on the distribution of resources by gender in a similar context. Hence, p = 50%, with a precision of 5% on either side of the proportion and a 95% confidence level, design effect of 2, and 10% of the non-response rate will be considered
This final sample size was proportionally allotted to the different categories, and a simple random sampling technique was employed to select the study subjects.
Data Collection Instruments and Procedure
A semi-structured questionnaire that consisted of items on socio-demographic variables (age, gender, income, profession, academic rank, etc.), access to college resources, institutional factors, and sexual harassment events was developed. It was first developed in English, then translated into the local languages. Six experienced and first-degree-holder health professionals were recruited as data collectors while two trained second-degree holders were appointed as supervisors. Then, data collection was undertaken through a self-administered semi-structured questionnaire to participants following the receipt of informed consent reaching their working places by data collectors.
Study Variables
Gender equality is the dependent variable, whereas, socio-demographic, institutional, political, knowledge/skill, and workplace harassment are the independent variables.
Operational Definitions
Gender Inequality
gender gaps in representation at different levels, access to resources and opportunities, and availability and use of gender mainstreaming resources within the CHMS/HFCSH.
Gender Representation
gender gaps in participation at different levels of leadership positions, academic ranks, and health professions within CHMS/HFCSH. It also refers to the number of males and females based on fields of study, performance, and attrition rate.
Access to Resources and Opportunities
gender gaps in access to resources such as housing, office spaces, and laboratories. It also refers to gender gaps in access to opportunities for personal development such as further education and training including participation in conferences and meetings.
Gender Mainstreaming
all activities, initiatives, and projects within CHMS/HFCSH toward ensuring gender equality and empowering women.
Political Factors
the absence of women’s employment rights and protection legislation and the lack of commitment to ensure gender equality and empower women.
Institutional Factors
occupational segregation, resistance to gender equality initiatives, and male bias systems and work conditions.
Socio-cultural Factors
gender stereotypes, gender discrimination, biased sexual harassment, access of girls to education and training for formal health sector jobs, and work-family conflict.
Knowledge Gaps
lack of data and research to highlight gender gaps, lack of awareness, and skill to mainstream gender in the health and medical sectors.
Violence Against Women
any act of gender-based violence that results in, or is likely to result in, physical, sexual, or psychological harm or suffering to women, including threats of such acts, coercion, or arbitrary deprivation of liberty, whether occurring in public or private life.
Gender-based Violence in the Workplace
a serious violation of human rights and an attack on the dignity and physical and psychological integrity.
Perception; is how something is regarded, understood, or interpreted.
Data Processing and Analysis
Data were coded and entered into SPSS Version 26 for analysis. Then, they were cleaned and checked for completeness with simple frequencies and cross-tabulation. The completed data were analyzed using SPSS. A descriptive analysis was conducted and data were presented using percentages (frequency distribution), tables, and figures. A narrative description of the key variables’ was included. Documents of the college were reviewed to evaluate the staffing profile.
The main enquire of the survey was perception toward gender equality, which was measured as a latent variable. Four latent variables (political, institutional, knowledge and skill, and sociocultural factor (s) were considered as predictors for the outcome variable. Prior to fitting the structural equation model (SEM), a confirmatory factor analysis (CFA) was conducted to test the model fit of the gender equality score and other latent variables scores.
Individual SEM models are described using path diagrams. Path diagrams are used in SEM’s GUI, known as the SEM Builder as the input to describe the model to be fit. SEM diagram is composed of the following:
Coefficients for the fitted model were reported using a standardized value in standard deviation units, along with estimated error variances as the fraction of the variance that is unexplained. The variances of the latent variables are standardized to 1, and obviously, being a normalization, there is no corresponding standard error.
Indicators used to evaluate the SEM fit were the Sartorra- Bentler Chi-squared test of fit (p > .05), Comparative Fit Index (CFI ≥ 0.90), Tucker-Lewis Index (TLI ≥ 0.90), Root Mean Square Error of Approximation (RMSEA ≤ 0.08), Standardized Root Mean Square Residual (SRMR ≤ 0.08) and the coefficient of determination (R2). Satorra–Bentler scaled X2 test was reported using a test for “model versus saturated”; a non-significant result implies that the model does fit well. The null hypothesis of the test is that the fitted covariance matrix and mean vector of the observed variables are equal to the matrix and vector observed in the population.
Results
Sociodemographic Characteristics of Staff
In this study, out of the assumed 422, 401 respondents participated, with a response rate of 95%.
Of the whole participants 343 (85.5%) were females, 147 (36.7%) were first-degree holders, 239 (59.6%) were administrative staff and Only 2 (0.5%) had a managerial role (Table 1).
Sociodemographic Characteristics of staff Health Institutions of Haramaya University, Eastern Ethiopia, 2021.
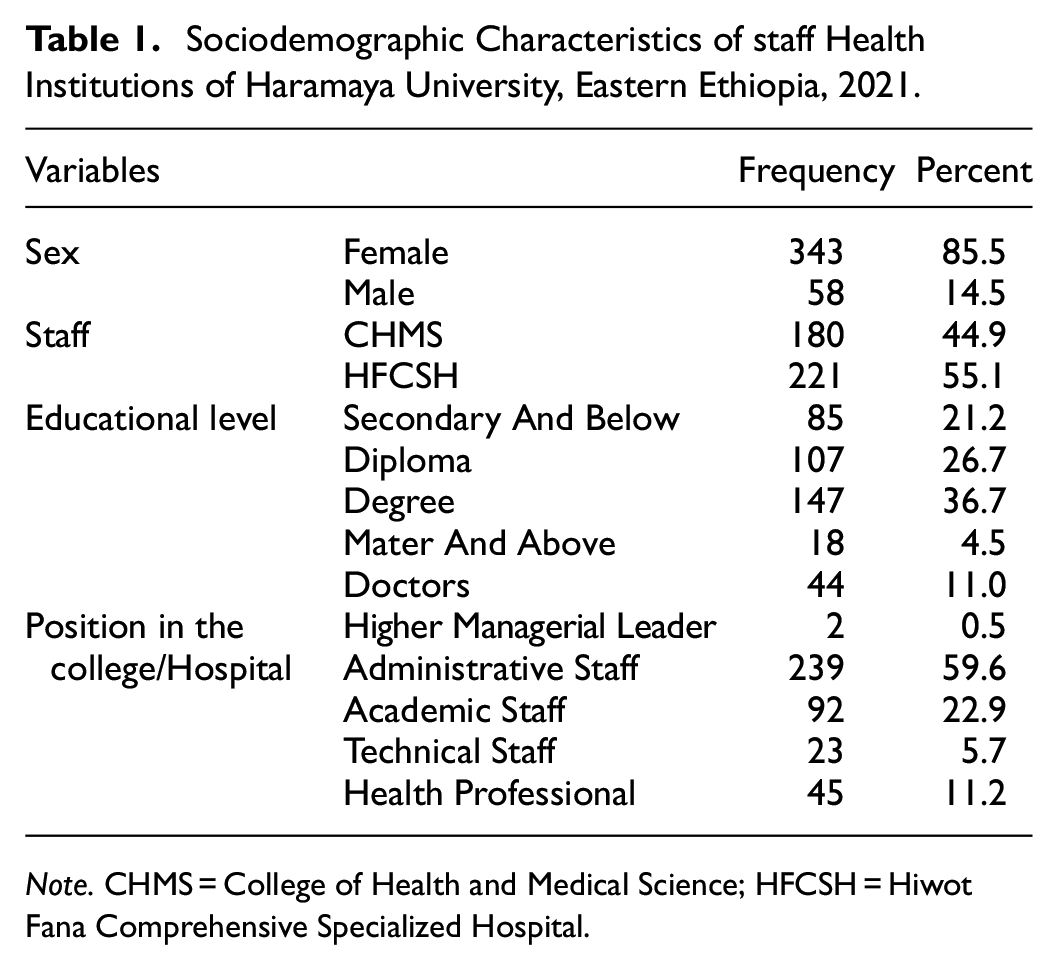
Note. CHMS = College of Health and Medical Science; HFCSH = Hiwot Fana Comprehensive Specialized Hospital.
Gender Equality Measurement
Contextualized gender equality was evaluated by considering 12 points (Table 2). Most of the respondents replied with either neutral or beyond neutral scores with a mean of 3.27 ± 0.918 (SD) of gender equality (Table 3).
Gender Equality Measurement in Health and Medical Institutions of Haramaya University, Eastern Ethiopia, 2021.

Score of Construct Variables Using Mean and Standard Deviation.

Note. PF = political factors; IF = institutional factors; KS = knowledge and skill factors; SCF = sociocultural factors.
Predictor of Perception Toward Gender Equality
Table 4 shows the scores of the predictors of perception toward gender equality from a multivariable structural equation model. The model was adjusted for sex, educational level, and profession. In the multivariable regression model, political factors, institutional, and sociocultural factors (Supplemental Table) independently predicted gender equality while knowledge and skill were not.
Multivariate Analysis for the Perception of Gender Equality.

Controlled variables; sex, educational level, and profession.
since there is no indirect relationship between variables, the total effect is equal to a direct effect of four latent variables.
P-value with < 0.05 > 0.01 ** < 0.001 > 0.0001.
The perception of gender equality increased by 0.21 (standardized β = .21, 95% CI: [0.10, 0.31]) as the political factors score increased by one. An increase in one institutional score increased the perception of gender equality by 0.32 (standardized β = 0.32, 95% CI: [0.09, 0.55]). Similarly, the increment in sociocultural factors scores resulted in the increment of perception toward gender equality by 0.18 (standardized β = .18, 95% CI: [0.11, 0.26]) (Table 4). Figure 1 shows the SEM for the perception of gender equality according to a theoretical model. Model fit for the SEM was adequate according to the Mplus fit statistics (RMSEA = 0.089, CFI = 0.771, TLI = 0.754, CD = 0.999).
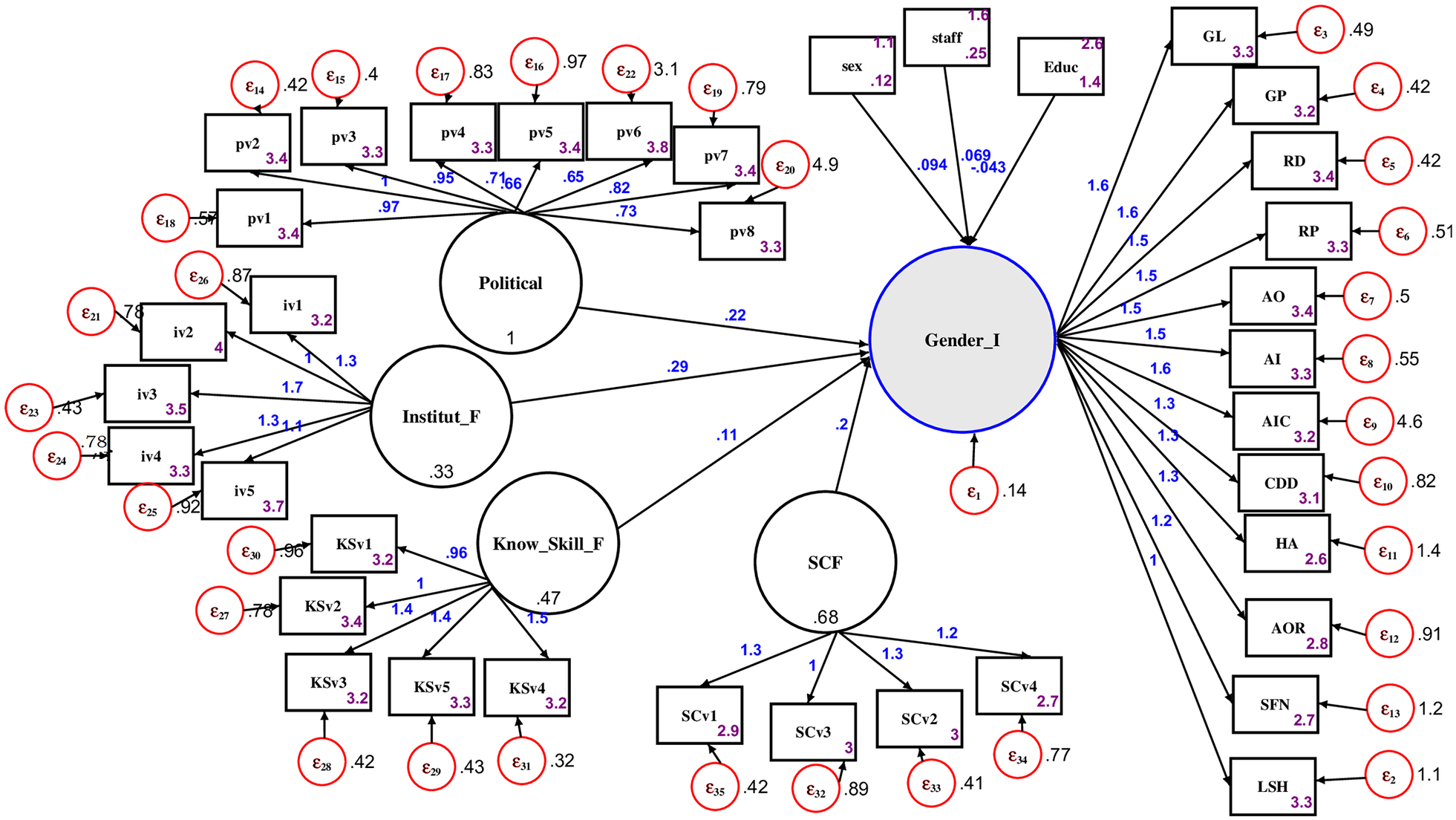
The relationship between the perception of gender equality and independent predictors according to structural equation model at Haramaya University, Eastern Ethiopia, 2021.
Workplace Harassment
In this study, the proportion of workplace harassment in one form of violence ranged from 15.2% to 39%. In addition, 33% of participants responded having the habit of reporting the incident(s). The reasons forwarded for not reporting were seeking a solution by dialog (n = 26, 9.7%), lack of gender office at the hospital setup (n = 19, 7.5%), fear (n = 16, 6%), privacy (n = 15, 5.6%), and considering the experience as simple occasions (n = 13, 4.9%) (Table 5).
Workplace Sexual Harassment Incidences in Health and Medical Institutions of Haramaya University, Eastern Ethiopia, 2021.

Discussion
In this study, political, institutional, and sociocultural factors independently predicted gender equality while knowledge and skill were not. Around one-third of the respondents experience one form of violence. Preference for dialog and the absence of a gender office in the hospital setup were the main cited reasons for not reporting harassment experiences.
Gender Equality
Gender equality means the state or condition that affords women and men equal enjoyment of human rights, socially valued goods, opportunities, and resources (Cruz & Klinger, 2016). Hence, in this study, the perception of gender equality was measured by considering gender distribution in representation at different levels of leadership, access to resources and opportunities (educational and training), availability and use of gender mainstreaming resources, and other related issues within the institutions (Table 2). On the five-point Linkert scale, most of the participants responded with neutral equality, with a mean of 3.27 ± 0.918 (SD) for a total of twelve enquires. However, the document reviews in the college showed unequal academic representation (17%) and a gap in the professional distribution of departments. Likewise, findings from other research universities in Ethiopia; Addis Ababa University (15.35%), Arbaminch University (15.42%), Jimma University (16.72%), and University of Gondar (17.94%); showed female academic staff accounted for below one-fifth of faculty members (Alemayehu, 2021; Gobaw, 2017; O’Keeffe, 2017; Yigeremu et al., 2021) and international higher academic institutions further witnessed analogous inequality (Mama, 2006; Morley, 2014).
However, the respondents in this study did not report these disparities. These overlooked replies may further implicate gaps in women networking for information sharing, support, and mentorship among themselves (Sisay et al., 2021). Besides, respondents may not understand gender equality from a different perspective. They might perceive equality by looking at a mere number of female staff (higher lower-level) and some academically advanced female healthcare providers (doctors, specialists) compared with previous trends in Ethiopia. In addition, the medical staff has also reflected resistance to gender issues by ranging from denying to dismay. Denial exists when those believe that they haven’t experienced gender inequality, and if do not notice gender inequality, it must not exist. This was also mentioned by most of the female medical faculty in Ethiopia that they did not feel that their gender had been a disadvantage or an advantage to their careers. Gender issues may also be reduced within the hierarchical scale of worthwhile knowledge. Individuals also distanced themselves from dealing with gender issues when problems are blamed on an unchangeable factor. Dismay occurs when confusion is overwhelming and no solutions are seen (Kvach et al., 2017) which might contribute to careless responses. Hence, though gender equality measurement varies at an individual and societal level (García-González et al., 2019; Tsegay, 2017), individuals are expected to understand the problem up to the level and must be committed to playing the role to come up with a tangible change in society (Tsegay, 2017).
In the present study, the multivariable regression model of SED, political, institutional, and sociocultural factors independently predicted the perception of gender equality. Similar relations have been reported from gender studies in higher education institutions in Ethiopia (Ademe & Singh, 2015). Another finding also revealed that women’s empowerment is highly affected by personal, institutional, and social factors (Singh, 2019). Besides, the implementation of gender policy in the government system showed to improve women’s political participation (Abdul Jabbar et al., 2015; Bussmann, 2010; Mlambo & Kapingura, 2019; Robinson & Gottlieb, 2021). This shows political will is one of the key requirements to effectively mainstream gender in any program, project, curriculum, and research, among others (Lombardo & Mergaert, 2013). Political commitment is not only indicated by a high level of support by the decision-makers but also by the allocation of financial resources and time to address gender equality in the sector (Stratigaki, 2005). Accordingly, women’s meaningful involvement in the processes will create a more legitimate representation of socio-economic and health concerns (González, 2018; Meagher et al., 2021; Moyo & Dhliwayo, 2019).
It has also been reported that socio-cultural factors have a lot of influence on women’s participation in decision-making. Women usually consult their male relatives since they feel that leadership is supposed to be for only men. Some community cultures completely prohibit women from participating in public matters; as a result, women’s access to information is limited (Hafkin, 2017; Mungiria, 2013; Sey & Hafkin, 2019). Besides, in most societies across the world, domestic roles are reserved for women, regardless of their responsibilities in the public arena. As a result, the disproportionate responsibility of women’s domestic chores and care roles are potential reasons for the delay in their career advancement and under-representation in leadership (Bahiru & Mengistu, 2018; Lyu et al., 2019). These expected triple roles (family, career, and community) would result in higher work-family conflicts, higher incidence of burnout and emotional exhaustion, and a negative association of parenthood with career routes (Baptiste et al., 2017; Dyrbye et al., 2011; Lyu et al., 2019). Evidence also showed that some women resign themselves from leadership positions due to work-family conflict (Tomer et al., 2015).
In this study, knowledge and skill were not a predictor of gender equality. This might reflect that other factors may strongly influence implementations of gender equality at the grass root level. Though understanding gender equality is a transformative process to develop skills and changes in attitudes and behaviors, it is a continuous and long-term process that requires the political will and commitment of all parties to create inclusive societies that recognize the need to promote gender equality.
It seems that without a change in attitude which is highly interfered with local sociocultural factors (Yeba & Meno, 2015), knowledge may not guarantee the implementation of gender equality (Kirima, 2019). Culture is part of the fabric of every society. It shapes “the way things are done” and our understanding of why this should be so. The cultural values of a particular area are described as a major constraint on efforts for gender equality, and therefore action is considered to be difficult for practical reasons. A balanced assessment of the potential for gender equality initiatives requires consultations with a range of actors, including those working for equality to bring behavioral change (Schalkwyk, 2021).
Hence, gender empowering policies (Bayeh, 2016; Lewis et al., 2014) have to bring out the oppressed and marginalized groups, women, out of domination (Arora-Jonsson et al., 2019; Choudhry et al., 2019). The implementation Ethiopia Policies of Gender Equality (Bekana, 2020) at an institutional and national level has paramount significance to tackle culturally flawed concepts of gender, workplace discrimination, and impediments to education (Abate & Woldie, 2022; Wright, 2020). In addition, awareness programs relating to gender equality, women’s education, and greater inclusion of women in society and the labor market can potentially foster more favorable attitudes toward equality (Van der Vleuten et al., 2020; Beckert, 2019; Nasr & Hammoudeh, 2019).
Workplace Harassment
An international labor organization (ILO) stated in the convention and recommendation that everyone has the right to a working life free from workplace violence and that member states should adopt appropriate measures of prevention (Nyberg et al., 2021). However, violence has been reported in all sectors, particularly in female-dominated sectors such as health and social services (C. J. Newman et al., 2011).
In this study, the proportion of workplace harassment in one form of violence ranged from 15.2% (unsafe workplace) to 39% (workplace bullying). Similar findings were reported from studies conducted in public health facilities of Ethiopia which the prevalence of workplace violence was 43.1% in the southern region (Weldehawaryat et al., 2020) and 26.7% in the northwest region (Tiruneh et al., 2016). But a greater percentage of violence was reported from 64.0% in the eastern part (Legesse et al., 2022) and 58.2% northwest region of the country (Yenealem et al., 2019). Another systemic meta-analysis reported a national pooled prevalence of 46.93% (Kassa & Abajobir, 2020) and 49% (Worke et al., 2020) among female university staff. These differences are attributed to sociocultural variations among regions of Ethiopia in how treating women in society. Moreover, the 2016 Ethiopian Demographic Health Survey also found that as many as 1 out of 4 or 26% of women aged 15 to 49 experienced physical and/or sexual violence by an intimate partner or non-partner in their lifetime (Handebo et al., 2021).
Studies from Nigeria further showed, the prevalence of workplace incivility, bullying, and sexual harassment (SH) have been reported at 63.8%, 53.5%, and 40.5%, respectively (Parkes et al., 2017). Besides, in Rwanda’s health sector, 39% of health workers had experienced some form of workplace violence (C. J. Newman et al., 2011). Another study has found that GBV exists in most public workplaces in the Edo state of Nigeria and that at least one in every three women in the state public sector claimed to have been harassed sexually, physically beaten, and/or otherwise abused in their workplace (Ajayi, 2021). This supports the findings of the ILO working paper (Cruz & Klinger, 2016).
Moreover, in the present study, one-third of the participants have a habit of reporting the GBV experience(s). And the reasons for not reporting the experiences were privacy, fear, absence of gender office at the hospital, considering the harassment as a simple occasion, and preferring to find a solution with dialog. Similarly, findings from the 2016 EDHS revealed only 23% of women who experienced physical and/or sexual violence sought help, whereas 66% of women never sought help and never told anyone about the violence (Handebo et al., 2021). A similar tendency of under-reporting due to social stigma, economic conditions, and illiteracy has been reported elsewhere (Kaphle et al., 2015).
Exposure to workplace GBV can affect women’s mental and physical health and work productivity (Parkes et al., 2017). Accordingly, a reduction or elimination of this violence, and the health problems it creates, requires concerted and integrated proactive strategies, together with rigorous evaluation of preventive measures (Mayhew & Chappell, 2007) to reduce employers’ economic losses associated with employees’ experience with GBV (Women, 2015).
Ethiopia has laws (Proclamation No 1156/2019) (Teshome, 2020) incorporating sexual harassment and sexual violence consequences that guarantee equal rights and prohibit most forms of GBV. The government as a whole, as well as its institutions, should work harder to enhance gender equality and thereby prevent violence against women (VAW) and specifically achieve SDG5 of eliminating VAW by 2030 (Kassa & Abajobir, 2020). For this identifying the risk factors of violence at community and institution-based levels is useful. Key elements of successful interventions have been proposed as participatory group learning, engaging male partners, engaging the community, and utilizing existing platforms (Cruz & Klinger, 2016; Keith et al., 2023).
Conclusion and Recommendation
The findings of this study showed the challenge of achieving gender equality in the health and medical institute of Haramaya university. But, these disparities were not reported by the participants. Political, institutional, and sociocultural factors independently predicted the perception of gender equality while knowledge and skills were not. This might reflect that though understanding gender equality is a transformative process to develop skills and changes in attitudes and behaviors, it is a continuous and long-term process requiring the political will, and institutional commitment of all parties to create inclusive societies that recognize the need to promote gender equality.
The experiences of workplace harassment in one form were reported/witnessed by 39% of the participants. The main reasons for a decreased habit of reporting GBV were preferring dialog to get a solution and the unavailability of a gender office at the hospital. Therefore, strategies and interventions that alleviate the socio-cultural, political, and institutional barriers should be designed. Moreover, a decent workplace free from harassment and indiscrimination has to be addressed by strengthening and establishing gender offices in the hospital to increase the scope of the services. Further research considering an in-depth assessment of the impacts of each factor and how the different forms of workplace violence may affect the employees’ health has to be conducted.
Strength and Limitation
A gendered analysis of health and medical university systems at higher educational institutions gives insight into the existing situation and helps map solutions to transform the organizations in general, Haramaya University in particular. Our survey is the prime research of its kind in the eastern part of Ethiopia. However, the impacts of gender equality determinants could not be seen in the short study period.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241298396 – Supplemental material for Assessment of Gender Equality and Workplace Harassment in Health Institutions of Haramaya University, Eastern Ethiopia: A Time to Question our Perception
Supplemental material, sj-docx-1-sgo-10.1177_21582440241298396 for Assessment of Gender Equality and Workplace Harassment in Health Institutions of Haramaya University, Eastern Ethiopia: A Time to Question our Perception by Mulu Berhanu Hundera, Yadeta Dessie, Herma Majoor and Tigist Gashaw in SAGE Open
Footnotes
Acknowledgements
We would like to thank CHMS’s and HFCSH’s staff members for their cooperation during data collection.
Authors’ Contribution
All authors made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis, and interpretation. All took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, and agreed on the journal to which the article has been submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research received financial support for data collection from the Elizabeth Strouven Foundation in Maastricht.
Ethical Considerations
Before data collection, ethical clearance was obtained from the Institutional Health Research Ethics Review Committee of Haramaya University, College of Health and Medical Sciences (Ref. No. IHRERC/178/2021). The objectives and purposes of the study, as well as risks and benefits, were explained to the heads of the institutions and the study participants, and then informed, voluntary, written, and signed consent was obtained from the participants. Throughout the study period, the confidentiality of the data was strictly kept, and the data were not used for another purpose. Besides, COVID-19 protective mechanisms were maximized during the data collection, by keeping social distance and providing preventive materials such as face masks and sanitizer. Finally, based on the gap identified, impacting interventions such as dialogues, seminars, and drafting of gender policies were undertaken, along with the sustainable designation of strategies.
Data Availability Statement
All relevant data that support the findings of this study are included in the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.