
Abstract
The convergence of the high prevalence of HIV incidence among African American adolescent and adult women along with substance use and risky sexual behavior among university students necessitates the development of a HIV intervention specifically addressing culture, gender, and college factors for female African American university students. The woman-focused HIV intervention was chosen for adaptation because it has been shown to be efficacious with reducing risk for African American women who use alcohol and drugs, and has been successfully adapted 7 times. The target population was African American college women enrolled at a historically Black university who use alcohol and other drugs, and who engaged in risky sex behaviors. To understand and assess the needs of this population, we conducted four focus groups with African American college women, two in-depth interviews with faculty, and a combination of in-depth interviews and focus groups with student affairs and health staff that were analyzed using content analysis. From this analysis, several themes emerged that were used to adapt the intervention. Emerging themes included challenges related to identity and societal stereotypes, lack of knowledge about sexual health (i.e., negotiating safer sex) and the function of female and male anatomies, high incidents of pregnancy, negative consequences related to alcohol and marijuana use, and the need to incorporate testimonies from college students, media enhancements, and role-plays to convey intervention messages. After the preliminary adaptation, 11 college women reviewed the adapted intervention and provided positive feedback. Plans for future research are discussed.
Keywords
African American youth in the nation have been disproportionately affected by HIV/AIDS accounting for approximately 65% of all HIV infections diagnosed for ages 15 through 24 (Centers for Disease Control and Prevention [CDC], 2010a). Results from The Women’s HIV SeroIncidence Study (ISIS study) indicate the HIV incidence among African American adolescent and adult women from the northeast and southeast region of the United States (including Atlanta, Georgia; Raleigh-Durham, North Carolina; Washington, District of Columbia; Baltimore, Maryland; Newark, New Jersey; New York City, New York) ages 18 to 44 is 0.24% (Hodder et al., 2012). This incidence is 5 times higher than that estimated by CDC for African American women overall and is comparable with the estimated HIV incidence rates in some sub-Saharan African nations such as the Congo (0.28%; Hodder et al., 2012). Furthermore, in 2009, African American young women ages 15 to 24 had the highest rates of gonorrhea (rate of infection was 5,162.5 per 100,000) and the highest rates of Chlamydia infection with 1 out of 10 women in that age group (the rate of infection was 10,629.7 per 100,000; CDC, 2010b).
Specifically for African American college students, there is an increased risk of HIV infection among them as compared with their White peers (Bazargan, Kelly, Stein, Husaini, & Bazargan, 2000). Recent research indicates that HIV prevalence among North Carolina college students is on the rise on college campuses, especially historically Black colleges and universities (HBCUs; Hightow et al., 2005). In addition, research has shown that African American students (AAS) at HBCUs are more likely to have vaginal sex, have sexually transmitted infections (STIs), and have been pregnant or fathered a child, in comparison with their White counterparts at traditional White institutions (TWIs). Com-paratively, AAS are less likely to use alcohol before any sex act, more likely to have been tested for HIV, and generally speaking, take more protective sexual behaviors in some respects but practice riskier behaviors in other areas (Hou, 2009).
Furthermore findings indicate that there are six barriers to safer sex for AAS. Those barriers are negative views of condoms, trust, living in the moment, feelings of invincibility, lack of self-control, and peer pressure (Duncan et al., 2002). Whereas male and female AAS shared barriers to safer sex, African American college women (AACW) had additional barriers—under the influence of alcohol and other drugs (AODs), do not realize the consequences, and lack of self-respect. Researchers recommended assessing the AAS’ ability to problem solve (i.e., negotiation) and understand HIV transmission, alcohol and drug knowledge, and health beliefs (Duncan et al., 2002).
Results from The Historically Black College and University Campus Sexual Assault Study indicated that of the 3,952 AACW who participated, 14.2% reported experiencing either an attempted sexual assault or a completed one since they began college (Krebs, Lindquist, & Barrick, 2011). Three types of sexual assault were explored: “any sexual assault, forced sexual assault, and incapacitated sexual assault” (Krebs et al., 2011, pp. ES-3-ES-4). Findings indicated that numerous risk factors are differentially associated with the aforementioned types of sexual assault.
Hispanic ethnicity, opinion of school, fraternity party attendance, intimate partner violence, and having been a victim of forced sexual assault before entering college were associated with experiencing physically forced (but not incapacitated) sexual assault since entering college. Depression, getting drunk, and having been a victim of incapacitated sexual assault before college were associated with experiencing incapacitated (but not physically forced) sexual assault since entering college. Some risk factors, such as sorority membership, sexual activity, posttraumatic stress disorder, and accepting a drink from a stranger, were risk factors for experiencing both forced and incapacitated sexual assault since entering college. (Krebs et al., 2011, pp. ES-3-ES-4)
Some college students experience considerable peer pressure to use alcohol, drugs, and cigarettes, particularly when trying to adjust to making friends and adapting to college life. Consuming alcohol among college-aged students and on university campuses is more pervasive and destructive than is apparent. Research indicates that four out of five university students consume alcohol. In particular, alcohol consumption is associated with other health-risk behaviors, including high-risk sexual behavior, smoking, and physical violence (CDC, 2011). With regard to AOD use, AAS on HBCUs have been found to have more AOD-related problems associated with marijuana and alcohol use compared with alcohol use only (Rhodes, Peters, Perrino, & Bryant, 2008). In addition, substance abuse was among the potential factors that were associated with HIV infection (p < .05; Hodder et al., 2012). AOD abuse and HIV prevention interventions for college students should be tailored based on gender, age, and ethnicity (Randolph, Torres, Gore-Felton, Lloyd, & McGarvey, 2009).
To address the needs of at-risk female college students who use AOD at HBCUs, a HIV prevention intervention specifically focusing on culture, gender, and college factors is needed. A search of the literature indicates that there is no HIV prevention intervention tailored for AACW at HBCUs who use AOD. There have been a series of HIV interventions that have been found to be evidence-based interventions (EBIs). For behavioral prevention efforts to be considered an EBI, it must provide scientific evidence of efficacy for decreasing HIV risk (Lyles et al., 2007). Although EBIs have been shown to be efficacious with specific populations, researchers should adapt EBIs for different cultures for the EBI to be tailored to the nuances of that particular population or culture (McKleroy et al., 2006).
EBI Selected for Adaptation
A women-focused HIV prevention intervention called the Women’s CoOp was developed by Wechsberg (1998) that addresses cultural, contextual, and gender issues (Wechsberg et al., 2003) had excellent outcome (Wechsberg, Lam, Zule, &Bobashev, 2004). The CDC found this HIV intervention to provide best evidence with African American crack using women in North Carolina (Lyles et al., 2007). This intervention’s foundation is based on empowerment and feminist theories that encourage women to understand the risks associated with AOD use, how AOD abuse can affect personal power and subject women to risky sexual behavior (Wechsberg, 1998). Further adaptations of the intervention have addressed victimization, communication, and sexual negotiation (Wechsberg, Browne, Middlesteadt Ellerson, & Zule, 2010). The core elements of this women-focused intervention include (a) educational cue cards that address risk-reduction information, (b) peer interventionist who had gone through extensive training, (c) behavioral skills training, (d) role-plays of how to negotiate for safer sex and how to communicate, (e) individualized action plans to address risk behavior and goals, and (f) HIV testing and referral to necessary agencies (Wechsberg et al., 2011).
Results from numerous adaptations suggest that the intervention can be effectively translated and adapted for use with additional groups of vulnerable women (Wechsberg et al., 2010). The focus of this article is to present the formative phase of the adaption process where we explored the lives of AACW, their challenges, substance use, and risky behavior so to adapt the intervention for young AACW at HBCUs, who are at high risk for HIV infection and AOD abuse, and intimate partner violence (i.e., date rape).
Method
Procedure
Methods to adapt evidence-based HIV intervention have been duly noted in the literature (e.g., McKleroy et al., 2006; Wainberg et al., 2007; Wechsberg et al., 2010; Wingood & DiClemente, 2008). McKleroy et al. (2006), Wainberg et al. (2007), Wingood and DiClemente (2008), and Wechsberg et al. (2010) report similar adaptation processes of evidence-based HIV interventions. An overview of these adaption processes includes (a) assessing the needs of the target population who is at risk of HIV through focus groups and interviewers with key stakeholders in the community; (b) choosing an appropriate HIV intervention; (c) eliciting the opinions of the target population and key stakeholders on the intervention; (d) using the knowledge gained from the focus groups and interviews that adapt the intervention while keeping with the fidelity of the core elements and characteristics of the original intervention; (e) having members of the target population, key stakeholders, and experts in HIV interventions give feedback on the adapted intervention; and (f) training staff to implement the intervention so that the efficacy of the intervention can be determined. With the exception of training the staff, implementing the intervention to determine its efficacy, we completed the aforementioned process.
Overview of procedure
The woman-focused HIV intervention was selected because of its efficacy with African American women who use AOD and who are at risk for contracting HIV (e.g., Jones et al., in press; Wechsberg et al., 2004). The research team assessed the needs of AACW at a HBCU in the South by interviewing key stakeholders (i.e., faculty and administrators) and conducting focus groups with AACW. After analyzing the interview, focus group, and questionnaire data, the research team took the original intervention and using the results they adapted as well as added elements to the intervention for AACW who use AOD and who are at risk for contracting HIV. Once the adaptation was complete, AACW were recruited and offered feedback about the newly adapted intervention.
Eligibility and Human Subjects Approval
To be eligible for the study, female students had to be ages 18 to 24 years who self-identified as African American women, were undergraduates enrolled at a HBCU, were involved in heterosexual sexual relationships (defined as having had a minimum of two dating or sexual encounters with men during the past 12 months), and who had used alcohol or other drugs within the past 12 months. Professionals who provide direct services or teach AACW were eligible to participate in the university professional in-depth interviews. The present study protocol and materials were approved by a university’s Institution Review Board.
Sample and Recruitment
The sample included 28 AACW (4 focus groups), 11 university professionals who provided direct services or teach the students, and 11 AACW who reviewed the intervention once it was adapted. Participants were recruited from a HBCU in the southeast by posting flyers in residence halls, cafeterias, the student union, and academic buildings; by contacting student organizations and university departments; and by snowball sampling procedures.
Participants were scheduled for preset focus group discussions. Key areas addressed in the focus groups with AACW included self-esteem, academic, and social stressors; coping mechanisms; knowledge of HIV/STI and pregnancy risk; condom efficacy; AOD abuse; relationships with men; intimate partner violence; concerns about risks of HIV; and treatment options. Following these discussions, participants attending the African American women’s focus groups were asked to complete a brief questionnaire packet that included 3 of the 10 sections of the Revised Risk Behavior Assessment (RRBA)—alcohol use, drug use, and sexual practices (RRBA has good psychometrics. Cronbach’s alphas of .71 and .91 have been reported; Jones et al., in press). The questionnaire also included other topics such as strength of religious faith with the Santa Clara Strength of Religious Faith Questionnaire (SCSRFQ; research indicates that the SCSRFQ possesses a high level of internal consistency, with Cronbach’s alpha scores ranging between .94 and .97 and split-half reliability correlations ranging between .90 and .96. Validity was also strong. For more information, please see Plante, 2010). The focus groups and questionnaire took approximately 2 hr. Student participants were given a US$30 gift card to a local store as an incentive for participation.
The university faculty and staff focus groups focused on recruitment and retention, concerns about rape, pregnancy, STIs, HIV, and intervention implementation. The faculty and staff interviews took about an hour. No incentives were given for faculty or staff participation.
All focus groups and interviews were recorded, and two members of the research team took notes. The focus groups and interviews were transcribed verbatim, and each transcript was checked for accuracy. Transcripts were entered into ATLAS.ti, a qualitative analysis and research software, for organization and coding of data. Through content analysis, each transcript was coded and themes emerged. Themes that were common across all groups were used in the process of adaptation. Responses from the brief questionnaire were entered into SPSS to determine descriptive statistics of the participants.
Results
The results include demographic information on the AACW participants (see Table 1); emerging themes from focus groups with the women, staff, and faculty; descriptive information about sexual risk behavior (see Table 2); descriptive information on alcohol and drug use and behaviors (see Table 3); results from the subscales of the SCSRFQ (see Table 4); and finally, a description of the adaptations and additions to the interventions (see Table 5).
AACW Descriptive Statistics (N = 28)

Self-Reported Sexual Attitudes and Behaviors Within the Past 12 Months

Note: Sex can refer to vaginal, oral, and/or anal.
Self-Reported Alcohol and Drug Use and Behaviors

Note: AACW = African American college women. AACW refers to participants in this study.
Examples given: codeine, Tylenol with codeine, OxyContin, hydrocodone, Vicodin, Percocet, and Percodan.
AACW’s Scores on Their Strength of Religious Faith

Note: AACW = African American college women. AACW refers to participants in the study.
Intervention Core Areas Adapted From Women’s CoOp Intervention or Added to Address Needs of AACW
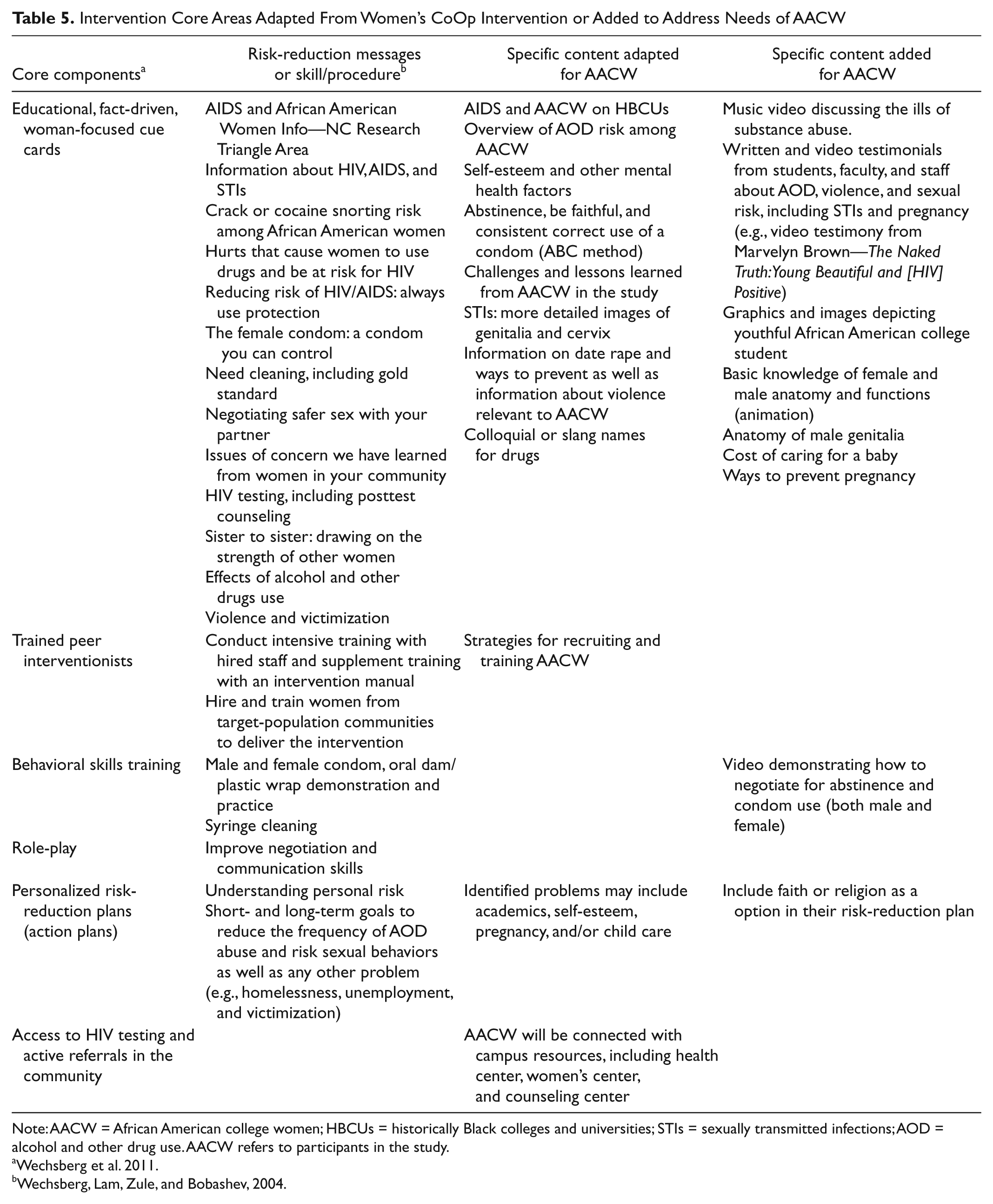
Note: AACW = African American college women; HBCUs = historically Black colleges and universities; STIs = sexually transmitted infections; AOD = alcohol and other drug use. AACW refers to participants in the study.
Several themes emerged that were helpful in the adaptation process. Those themes are (a) AACW are challenged with issues around self-esteem and self-image, (b) a need for understanding the anatomy and function of both the female and the male body, (c) a need for testimonies and media enhancements to the intervention featuring African Americans who are of college age, (d) the impact of AOD use on campus, (e) sexual risk-taking behavior, and (f) reactions to the adapted intervention. The preceding thematic categories are supported by the direct quotes of the participants. Not all the quotes associated with the theme are listed. The quotes that were chosen best illuminate the theme.
Challenges of AACW
Of the many challenges mentioned in the study—finances, pressure to succeed, mate selection and choice, substance abuse, sexual health, and coming to college with psychological issues, including childhood sexual abuse—the most common challenge that emerged was issues related to identity, self-esteem, societal stereotypes, and standards—both positive and negative.
They expect so little from you. Society . . . and you can kind of see it on campus. Like the way women dress. If you were to see a woman scantily dressed it shows me that her self-esteem is low or that she doesn’t see the value in herself that she doesn’t have to dress that way. I guess the pressures of being thought of as being very promiscuous and the other stereotypes of Black women gets into their psyche. It comes out in out how they dress, how they act, how they interact with men.
Substance use. That is part of it. It seems like it is external gratification. Whether it is sex or alcohol. If I don’t feel good about myself inside I get use to relying on these external factors to make yourself feel good and you forget how to do it yourself.
Much of BET and MTV and pop culture are busy defining what it means to be a Black woman and I think that is counter to what it has been historically. I think that is challenging for the sistas.
Sexuality 101: Sexual Health Including Knowledge of Anatomy Function
Lack of knowledge is a consistent theme that emerged with all participants in the study. Most AACW are unknowledgeable about sexual health (i.e., negotiate safer sex) and the function of their anatomy or the anatomy of their male counterparts. Furthermore, Table 2 describes the self-reported sexual risk behavior of the AACW.
They don’t know or they don’t want to feel like . . . I guess women feel like if they are too aware about certain things like sex that men are going to think that they are promiscuous or that they have an STI or STD.
I think it is [because of lack of self-worth and feelings of invincibility] because [they] are coming in for the same thing (i.e., STIs) and not being able to negotiate safer sex. [Their rationale is] “if we haven’t been using condoms and he is going to expect that, how do I now bring it up?” So we end up going through a long list of things they can say and there is even a pamphlet “how to get your partner to use a condom” but sometimes it’s hard to negotiate yeah I want to use a condom, but the girl across the street will have sex with him without a condom but I want him so I will just not use a condom. Some of that thinking, well I want to keep him and he looks clean, he looks good, and I haven’t gotten anything so far and he tells me I’m the only one so there you go. It breaks your heart.
Uhm, there’s a lack of awareness. I think when they think about, uhm, contraception they focus on pills—so pregnancy prevention—more so than anything else. Uh, in my . . . class right now we’re talking about AIDS. And I show them a video. And so they’re very unaware that African American women have the highest rates of HIV/AIDS; very unaware, they were very alarmed and very upset by that . . . Uh, just lack of awareness about their body. Uh, sexual health—just knowing the different anatomy, anatomical structures and functions, I found that they, they’re not as aware of that. Uhm, don’t know what they . . . they know what the ovaries are, don’t know where they are, not sure the function of fallopian tubes and things like ectopic pregnancies and how Chlamydia and gonorrhea contribute to infertility, those kind of things. They don’t, they don’t make the connection.
It is an area that is totally new for them. They have never been educated. It’s like you ask them where did you get your education or from whom did you get your education about sex from? They will not say anything or say my brother or my cousin. If you are lucky maybe mom or dad.
Pregnancy on Campus
Students, professors, and staff reported that pregnancy was common and attributed it to a lack of education, being in the moment, wanting to love and be loved, and trying to secure a relationship with their boyfriend. They believe that showing the reality of the costs and the responsibilities having a baby would help reduce pregnancy as well as making it personal by including stories of students’ pregnancy journeys.
Something in the water . . . For a minute, I was like really scared to mess with anybody on this campus. They’ve got supersperm over here.
Show them their responsibility . . . like on a chart . . . how much you’ve gotta pay for it. Having a baby is a responsibility and it costs money. And if you think about it, your parents are most likely going to raise that child . . . not yourself. So, I just think if you put like a chart explaining to someone how much it goes for like a job. How much you paying for school. How much you paying for rent. How much you paying for these bills, then think about it.
But I’ve had . . . a number of young women who come in here, and, uh, I would probably say easily 95% of the time, even higher than that, you know, that didn’t plan this pregnancy, got pregnant, and now, you know, have to decide to leave the university. And unfortunately, a lot of times the game plan is “I’m gonna have this baby, then come right back.”
I have to realize even though they are older they are still not connecting their actions with the result of pregnancy. They are not thinking I can become pregnant. They might get on birth control and stop taking it and don’t use condoms and I say so you are trying to get pregnant and they say, “No I am not trying to get pregnant!” But you are not using birth control and you’re not using condoms and you still see that surprise which I am surprised to see in college women. I am surprised to see that kind of naivety among college women because I think that you know. Then we have some that are not protecting themselves but have not gotten pregnant so they think they have a fertility issue, and I find that surprising when you are 20, 19, or 20.
Physical Violence Against Women
The response about physical violence (i.e., sexual and domestic violence) was presented differently between students and faculty/staff. The staff and faculty were aware of rape and physical violence, because they had heard personal reports of incidents from students. The students had a more distant response and stated that they heard about AACW being raped but did not know anyone personally. Both groups discussed that AACW do not talk about being raped because people may not believe them, feeling that it was their fault, or they are apprehensive about reporting the incident or getting blamed. Some students expressed that some students were influenced by alcohol and regretted having sex. Both students and administrators mentioned that domestic violence occurs and sometimes women fight back.
I have heard of a few women getting raped on campus at campus [apartments] . . . I don’t know any of them. I feel sorry that they feel like it is their fault or that they can’t talk to anyone about it. That is the worse thing that can happen . . . someone just taking something from you and you can’t do anything about it, so I feel like I wish they would just get the strength to tell someone about it.
I think a lot of times date rape on campus is more like the girl slept with him last night and now she regrets it so she’s saying he raped her . . . and she used alcohol as an excuse. “I was drunken and he raped me.” But really she just gave it up. She was into it and in the morning she was like, “Why did I do that?”
I talk to one, and I remember her story and she told me that she went to a party with friends. They all left her, she’d come around a guy who basically said he knew the way back to the school. He took her out to some housing development that wasn’t completed yet and it was dirt dark outside there, and next thing you know, he parked his car with her side of the door facing the tree. So she couldn’t open it up, and she couldn’t get out. So she said the next 35 min were fighting, literally fighting with him for her life. And she said she got out of the car and he screamed, yelled, and cursed at her, threw her bag, and she had no idea where she was. She was standing in the middle of a housing development in pitch black dark at 2:00 or 3:00 in the morning, not knowing which way to go; couldn’t even figure out how to get out of the housing development to begin with . . . And, uh, you know what, if this is where he went, he probably did this before! And it probably worked before, and you know he didn’t change the plan. He went someplace where he thought he could isolate somebody. So our young women in here are often times they are very trusting . . . Uh, I can’t even tell you the women I talk to who—you know—still take drinks from people, and they don’t have any idea who it is. And here it comes, straight to them. They’re underage to begin with, and they’re drinking something somebody put in their hand, who is probably waiting to see whether or not, who’s gonna, what’s gonna happen to them when they start drinking. You know, there are predators out there.
Impact of Alcohol and Substance Abuse
With regard to AODs, all participants noted that marijuana and alcohol were widely used on campus. Other drugs mentioned were crack, pills like ecstasy, and “Superman”—”it’s like speed,” said one student. Administrators and faculty noted that AOD use was often linked with violence, sexual risk, or poor judgment. Table 3 describes the AOD behaviors reported by the participants.
I am probably sure they are using other things, but the two worst things on this campus are alcohol and weed.
I think marijuana is probably pretty significant. I mean, I think students are choosing to do, you know, smoke marijuana, or however they ingest it, uhm, quite regularly, on a pretty regular basis. And so they then behave as, you know, in the moment of having gotten high or whatever, and so . . . Uhm, from that perspective I think there’s a lot of substance abuse. And there is some alcohol, and it does get kinda tangled up in there. We’ve had a couple of parties where there’ve been people who have been just sloppy, sloppy drunk, drinking 15 and 20 shots and this or that, and so. Uhm, yeah, alcohol is, is probably not—percentage-wise—as high as weed is, but it’s there! It’s high, and they do it together often times they’re drinking and smoking simultaneously.
Um certainly alcohol, but marijuana is a bigger issue . . . This is something that my research is looking at. If we spend all of our time focuses on alcohol education which is what most sexual violence education does and then that’s not as big of an issue on HBCUs, what are the implications? So marijuana is a big issue on this campus. I haven’t encountered a lot of other things like opioids and meth, that I know of. But I certainly talking to a lot of women who have been high when things have happened like sexual assault or physical altercation.
What I do know about Black students and substance abuse is that they smoke weed and drink Hennessey. They aren’t out there into that wild stuff . . . I think it lowers inhibitions and it puts them in situations where they are more likely to engage in unprotected.
Importance of Spirituality to AACW
Participants—students, faculty, and staff—discussed the spirituality of AACW. One student said that AACW look to their faith and church
to be uplifted [and a place] to put your burdens on the altar or just get your problems off your chest. I guess church is not a way of escaping reality, but a way to know that it will get better. Some way, there is a silver lining somewhere.
Although, generally speaking, their religion and spirituality is very important to them, they sometimes found a disconnection between their faith and their actions. One female administrator said,
I think that there are a fair number of women who experience conflict because of what they are trying to do to keep their man. It could even be part of the sex life. Something that is contrary to their values, but it is something that the male wants or that they perceive that the male wants and they are trying to keep the male. I have had two or three firsthand experiences with women courting with those kind of experiences.
Results from the Santa Clara Strength of Religious Faith questionnaire (SCSRFQ) indicate that AACW reported that their relationship with God is important and that religious faith is important to them (see Table 4).
Intervention Enhancements: Testimonials, Skits, and Role-Plays
All participants mentioned that personal stories, skits, or role-plays would be helpful in educating AACW about substance abuse, sexual risk, and violence. Students emphasized that the intervention should have images, music, and people that are relevant to their culture. Being able to relate to the information presented was very important to the students.
I like your suggestion about having someone talk [in the intervention] because just from talking to some of my peers, particularly younger peers, I’ve learned that a lot of people think that [HIV] is farther away than it is. Everything that we talked about tonight [in the focus group] is farther away than it really is; if you could find someone who is comfortable enough to say, “Hey I am a student at [an HBCU]; I am a junior education major and this is my story. That would really help someone because I know a lot of females that are really naive about the things [i.e., HIV, impact of drugs and alcohol, pregnancy and rape] we talked about.”
[I think that students will] like skits too because they can reenact it in their minds.
I would say make it personal. Like the story/series that the editor did in the campus newspaper [where she talked about her experience getting pregnant and having a baby in college.] I think that really went a long way to start the conversation. Not hiding these women. That is going to be hard because some people are going to say well that is encouraging it that is promoting it. Well to be pregnant and to have unprotected sex, just to talk about it in a real way . . . this is what the life of a pregnant student or a single parent on campus looks like and its hard. But then also having women have real conversations about how they do creative sexually responsible things. Having them role-play flirting and talking about condoms or how I don’t really want to have sex tonight but I think you’re really cool and I hope we can go out again and having the confidence to say that too.
Feedback on the Intervention
A total of 11 AACW had an opportunity to observe the adapted intervention—The Aziza College Women CoOp. (Aziza has Swahili and Arabic origins, and means powerful, beloved, gorgeous, and valuable; Parents Connect, 2012). Each woman reflected on the various aspects of the intervention and was pleased with the final product as they believe that the intervention reflected the needs of AACW. They felt connected with the intervention in many areas (i.e., name of intervention; images of college-aged African American women of various shapes, shades, and styles; relevant case studies; media elements, including music video; interview with Marvelyn Brown; condom negotiation video; etc.). Participants wanted the information presented in a concise manner with bold colors and with diverse images of young college-aged African American women.
Love the name of the CoOp. It is a great name because so many women do feel powerless, not valued and unattractive . . . Like the name because it comes from our roots. [AACW] will relate. Important to know about what . . . Need to know about what pleases you. A lot of women just have sex and don’t come out with anything—no sexual pleasure/orgasm. They go into sex to please the man. It goes back to self-worth. Why are you doing it if you are not being pleased. Women competing to keep a man is important bullet. Because it is important that women know about their bodies. If they know about their bodies then they would know about the implications of risky sex. They don’t teach what they need to in sex education. You need to know this stuff so you know what you are getting yourself into. The slides on “Do you know your body,” they are good. Physical props of the female anatomy are important to have because women don’t examine themselves. Love that [you used] pictures are of real people. Attractive. Like the case study [about Jamila, her multiple sex partners and her chances for pregnancy and/or STIs/HIV] . . . It’s realistic. About the music video about the ills of substance abuse: The video is not corny. When main stream America tries to send a message through hip-hip it can come off strange. This is really organic. It sends a message without trying.
Adaptations and Additions of the Women’s CoOp Intervention for AACW
Based on the analysis of the data, various additions and adaptations were made to the intervention. Table 5 lists the core components to the original Women’s CoOp intervention as well as the adaptations and additions to address the needs of AACW.
Discussion
The knowledge that we have gained from the focus groups with AACW and in-depth interviews with faculty and staff has guided our adaption process. Much of what we have found has been supported in the existing literature. In our study, we found that 71.4% of AACW participants did not use condoms for every sex act. Predictors of HBCU students’ willingness to practice safer sex or their intent to practice safer sex was associated with their academic classification (upper class students were more willing to practice safer sex than underclass students), knowledge of HIV/AIDS, students’ willingness to associate with a HIV infected person, interest in HIV/AIDS education, understanding HIV risk behavior, and knowledge of HIV transmission modes (Mongkuo, Mushi, & Thomas, 2010). AACW in this study disclosed that one of the reasons that they did not insist on condom use is because they were in monogamous relationships. This finding is consistent with Duncan et al.’s (2002) research on barriers to HIV prevention. Duncan and his associates found that female participants in their study believed that they could trust that the man that they are having sex with would not give them a STI or HIV because they were in a monogamous relationship. Furthermore, their female participants defined their relationship as monogamous after 1 month or 12 sexual encounters. This relationship status was assumed by the AACW without the benefit of a discussion with their male partners. If monogamy is only assumed by AACW, it leaves them vulnerable to disease, pregnancy, and emotional hurt. The lack of communication exhibited by some AACW who do not discuss relationship status can put some young African American women at greater risk for pregnancy, contracting HIV, and other sexually transmitted diseases.
In the present study, alcohol and weed were reported to be the drugs of choice for some AACW on this particular HBCU. As a group, participants reported that they use alcohol, prescription pain relievers without a prescription, and marijuana the most. A total of 47% of participants had unprotected sex while under the influence of AOD. Intoxication is considered to be a barrier for safer sex among AACW (Duncan et al., 2002). Greater risk-taking behavior (i.e., having sex without a condom) may occur while intoxicated. In Duncan et al.’s (2002) research, intoxication was among the most significant barriers for AACW. This significant barrier may affect AACW more because women are more often the victims of sexual abuse when they are drunk or high (Duncan et al., 2002).
Research indicates that the students who attend HBCUs are positively impacted because they foster a nurturing and assistive environment where character development and religious expression are emphasized (Kapner, 2008). The scores from the SCSRFQ indicated that religious faith is an important aspect of AACW’s lives. Undergraduate students who regularly attend a religious service and who are highly religious are less likely to participate in selected sexual risk-taking behaviors (Campbell, 2008). Furthermore, results indicated that as levels of spiritual orientation decreased (e.g., very, moderate, a little bit, undecided, not at all), the occurrences of participation in selected sexual risk-taking behaviors increased (Campbell, 2008). To personalize the intervention, we propose for AACW to be given opportunities to create action plans for reducing risks with an option to incorporate their faith into their plans as some felt their relationship with God was extremely important to them and that faith often impacted their decision making. Resources for support will also include churches and faith-based college groups as AACW enjoy being around others who share their faith. Although it may be difficult to generalize, researchers believe that religious activity may be a key reason AAS consume less alcohol compared with other students (Brown, Parks, Zimmerman, & Phillips, 2001).
The proposed intervention—the Aziza College Women’s CoOp—has been adapted to address the cultural, gender, and college issues specific to AACW. Educational cue cards, films, and role-play activities educate women about HIV and other STIs and how they are transmitted, sexual risk behaviors, knowledge of the function of female and male sexual anatomy, how to reduce one’s AOD intake and abuse, and how to avoid violent relationships. The Aziza College Women’s CoOp is also designed to empower women to protect themselves by watching films that demonstrate how to negotiating for safer sex and practicing how to properly use the male and female condom. Using narrative communication such as role-plays and narrative films that were incorporated in this intervention have been shown to be a tool for health behavior change (Hinyard & Kreuter, 2007). Woman-focused interventions utilize interventionists as peers. AACW participants indicated that they wanted to hear from their peers with regard to intervention messages. Although more research needs to be conducted on the effectiveness of peer-led HIV interventions, however, the Joint United Nations Programme on HIV/AIDS (UNAIDS, 1999) reported that
peer education programs using experimental or quasi-experimental designs, with outcome indicators such as reduction of HIV-related risk behaviour and/or STI/HIV incidence, shows that peer education (in combination with other prevention strategies) is very effective in several populations and geographical areas. (p. 33)
Because of the high incidence of HIV infection among African American women and impact that AOD use has on HIV infection, a HIV prevention intervention, which addresses their specific needs as it relates to culture, gender, and the college experience, is needed. Now that we have adapted a woman-focused intervention for AACW at HBCUs, the next step is to conduct a feasibility study of the newly adapted intervention that will include adapting the woman-focused questionnaire and training staff to implement the intervention, and the efficacy of the intervention can be determined. It is our hope that the Aziza College Women’s CoOp will empower AACW who use AOD to reduce their sexual risk and improve their overall sexual health and help them make smarter choices about their AOD use.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research is supported by the University of North Carolina Center for AIDS Research (UNC CFAR P30 AI50410). The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the views of the UNC Center for AIDS Research.