
Abstract
The Malaysian healthcare system for individuals with Parkinson’s disease is still underdeveloped. Self-stigma has a significant influence on how successfully individuals with Parkinson’s disease handle their condition. Therefore, this study aimed to explore the association between self-stigma, basic and instrumental activities of daily living, and communication participation among individuals with Parkinson’s disease. In Study 1, 25 individuals with Parkinson’s disease from the Malaysian Parkinson’s Disease Association completed the Stigma Scale for Chronic Illness-8 Items, Katz Index of Independence in Activities of Daily Living, Lawton Instrumental Activities of Daily Living Scale, and Communicative Participation Item Bank. Survey responses were analyzed using descriptive statistics and correlation/regression. In Study 2, semi-structured interviews were conducted with nine individuals with Parkinson’s disease. Interview data were transcribed verbatim and analyzed using thematic analysis. Survey results indicated that a higher level of self-stigma was associated with lower levels of basic (r = −.47) and instrumental (r = −.21) activities of daily living and communication participation (r = −.41) among individuals with Parkinson’s disease. Furthermore, five main themes emerged from the in-person interviews: “challenges in performing activities of daily living due to Parkinson’s disease,” “speech and communication adaptations due to Parkinson’s disease,” “psychological responses toward one’s own Parkinson’s disease symptoms,” “self-stigmatization with impacts on self-concept,” and “perception formation of Parkinson’s disease resulting from self-stigmatization.” In conclusion, the self-stigma of individuals with Parkinson’s disease was considerably related to their activities of daily living and communication participation. Therefore, healthcare providers should address these factors collectively in their care of individuals with Parkinson’s disease. Moreover, health-related organizations and Parkinson’s disease associations must play a crucial role in educating and raising awareness of Parkinson’s disease in our society, considering that self-stigma is related to both how an individual perceives their condition and the public’s attitudes and perceptions toward it.
Introduction
The prevalence of Parkinson’s disease (PD) is continuing to rise along with an aging population (60 years and older) (Tysnes & Storstein, 2017), and the number of the aging population is estimated to reach 9.3 million in the year 2030 (Collier et al., 2017). This is a global issue, considering that Malaysia is moving toward becoming an aging country by 2030 (Ahmad et al., 2022). However, healthcare for individuals with PD (IwPD) is still underdeveloped in Malaysia. For instance, Malaysia currently has no prevalence of PD. IwPD often experience bradykinesia, rigidity, rest tremor, and difficulty with balance and speech (Kouli et al., 2018). Other than motor symptoms, non-motor symptoms related to PD have also been widely reported, including cognitive decline and mental health issues (Gupta & Shukla, 2021). Therefore, there is a growing need for healthcare providers to explore the nature of the symptoms of IwPD and how these symptoms affect the daily lives and communication participation of IwPD, and whether self-stigma is involved.
Ninety-two percent of individuals living with neurological disorders among the European population feel affected by stigma (European Federation of Neurological Associations [EFNA], 2020). In 1963, Goffman defined stigma as a mark of shame, disgrace, or disapproval, resulting in an individual being rejected, discriminated against, and excluded from participating in several different areas of society. Stigmatization toward an individual usually occurs when that individual exhibit behavior that differs negatively from the stereotypical behavior of a healthy individual, indicating a sign of impairment (Hanff et al., 2022). It is a multidimensional phenomenon and can be discussed through three aspects, which are: (1) public stigma (Vogel & Wade, 2022); (2) self-stigma (Gärtner et al., 2022); and (3) affiliate stigma (Zhang et al., 2018). The stigma surrounding PD is common (Ma et al., 2016). Numerous studies have explored public awareness and perception of PD (Alyamani et al., 2018; Youn et al., 2016). However, there are still a lack of studies that explore how IwPD perceive and internalize their condition, which is classified as self-stigma. Self-stigma is a process that starts when the individual is aware of others’ perceptions and stereotypes about their condition or the stigmatized group to which they belong. Then, they agree with the stereotypes and apply them to themselves (Sum et al., 2022). Typical PD symptoms may be considered stigmatizing (symbols of discrimination) and linked to a pejorative stereotype toward IwPD, since IwPD also encounter limitations in conducting their activities of daily living (ADLs) and communication (Hanff et al., 2022).
IwPD face difficulty performing their daily activities due to physical and psychological symptoms manifested by the disease. ADLs are the basic skills required to independently care for oneself, such as bathing, dressing, eating, using the toilet, transferring, and continence (Edemekong et al., 2022). Instrumental activities of daily living (IADLs) are those activities that require more advanced skills that allow an individual to live independently in a community, such as housekeeping, laundry, shopping, food preparation, using the telephone and transportation, handling finances, and taking medication (Edemekong et al., 2022). IwPD typically required assistance in carrying out basic daily activities, such as standing, and walking due to physical limitations caused by the disease (da Silva et al., 2020). It has been reported that individuals in the early stages of PD have greater difficulty performing IADLs due to impaired cognitive functioning and processing (Foster & Doty, 2021).
Cognitive deficits in IwPD are also closely related to their communication limitations (Rohl et al., 2022). It is reported that more than 90% of IwPD have speech and communication problems (Swales et al., 2021). IwPD frequently experience communication limitations due to changes in voice and articulation (e.g., weakness in voice, unintelligible production), body language and facial expressions (e.g., “mask face”), fatigue, self-image, communicative initiative, and familiarity with the conversation partner (Altaher et al., 2020). Moreover, they also face difficulties with both linguistic and pragmatic aspects of conversation, including problems with word-finding, the formulation of ideas, topic management, and turn-taking (Johansson et al., 2020).
Previous studies have reported that self-stigmatization negatively affects people with health issues, including IwPD, causing low self-esteem and self-efficacy, the avoidance of seeking for help (Wong et al., 2022), and decreases in social roles and network ties (Elliot et al., 2019). In the end, their health and well being suffered as a result of stigma (Fothergill-Misbah, 2023). According to Eccles et al. (2023), higher levels of felt stigma were linked to greater levels of distress among PD patients. Self-stigma, in particular, has a big impact on whether and how well PD sufferers handle their condition (Hanff et al., 2022). Their relationship could be explained by the mindsponge mechanism. The mind evaluates a choice via the mindsponge mechanism. An individual cannot regard a “’act” as a feasible and better alternative until two conditions are met. In the context of the IwPD, the first condition is the presence of information about societal attitudes, stereotypes, or personal experiences related to the stigmatized condition. The second condition is the filter’s choice to allow the information move in closer toward the mindset. Information must pass through the cost–benefit judgment gate in order to approach the thinking. If the relevant information (self-stigma) successfully infiltrate the mindset and becomes one of the mind’s core preferences, daily lives and communication participation will be affected (Nguyen et al., 2021).
In fact, in a user-informed prioritization exercise for the purpose of developing a research agenda, IwPD identified self-stigma as one of their top research priorities (Schipper et al., 2014). In addition to enhancing other types of research in the field, qualitative research has sparked new theoretical insights, techniques, and research methods, as well as new approaches to how healthcare professionals might deliver their services in ways that are relevant to their communities. This can be achieved through an understanding of the lived experiences and perspectives of communities and the development of knowledge of how they function in everyday circumstances (Hersh et al., 2022).The Health and Discrimination framework states that multiple stigmas may arise when a person experiences stigma linked with a health condition and other perceived distinctions that may reinforce that stigma (Stangl et al., 2019). It is expected that IwPD will experience self-stigma when they are exposed to stigma in real-world settings.
Therefore, the aim of this study was to explore the association between self-stigma, activities of daily living, and communication participation among IwPD. It was hypothesized that IwPD who experienced more stigma would have lower levels of activities of daily living and communication participation. The outcomes of this study could have implications for society as a whole and for the design of tailored therapies for each person with PD, with the goal of enhancing the psychological health of IwPD and subsequently improving their quality of life.
Methods
Research Design
A mixed-methods explanatory sequential design was employed, in which a quantitative analysis of survey responses (Study 1) was followed by a qualitative evaluation of in-depth interviews (Study 2). In Study 1, a 32-item questionnaire was distributed to IwPD electronically through the Malaysian Parkinson Disease Association’s (MPDA) social media platforms (Facebook and WhatsApp). Survey responses were analyzed using descriptive statistics and bivariate or multivariate tests. In Study 2, IwPD who completed the online survey were invited for a semi-structured interview via teleconference. Interview data were transcribed verbatim and analyzed using thematic analysis.
Participants
Twenty-five IwPD were recruited for Study 1 via convenience and snowball sampling. Inclusion criteria included the ability to read English and use speech as a mode of communication. In Study 2, purposive sampling was used for an intended target of 14 IwPD; however, only nine were recruited for interviews. In study 2, participants used English or Bahasa Melayu as their primary language.
Instruments
Stigma Scale for Chronic Illness
The Stigma Scale for Chronic Illness (SSCI), which includes 24 items, measures enacted and individualized stigma for people across chronic illnesses, including PD (Rao et al., 2009). The SSCI-8 is a short version of the SSCI-24, which consists of three items of individualized stigma and five items of enacted stigma. Each item uses a 5-point Likert scale ranging from 1 (never) to 5 (always). The sum score range for the SSCI-8, accordingly, is 8 to 40, with higher scores indicating a greater perception of stigma. The SSCI-8 has a high internal consistency, with a Cronbach’s alpha of .89 and item-total correlations of .45 or higher (Molina et al., 2013).
Katz Index of Independence in Activities of Daily Living
The Katz Index of Independence in Activities of Daily Living (Katz ADLs) assesses a patient’s ability to perform basic activities in daily life independently. Patients rate their independence using yes = 1 and no = 0 in each of the six functions of bathing, dressing, toileting, transferring, continence, and feeding. A score of 6 indicates full function, 4 indicates moderate impairment, and 2 or less indicates severe functional impairment. The Katz ADLs has a high internal consistency, with a Cronbach’s alpha of .87 and item total correlations of .50 or higher (Ciesla et al., 1993).
Lawton Instrumental Activities of Daily Living Scale
The Lawton Instrumental Activities of Daily Living Scale (Lawton IADLs) is another measure of independent living skills (Graf, 2008). However, the skills measured in the Lawton IADLs are considered more complex than the basic daily living activities in the Katz ADLs. The Lawton IADLs assesses a patient’s functional independence in the areas of using the phone, shopping, food preparation, housekeeping, laundry, transportation, responsibility to own medicine, and handling finances. The sum score ranges from 0 (low function, dependent) to 8 (high function, independent). The Lawton IADLs is a reliable measure with a Cronbach’s alpha of .85 (Graf, 2008).
Communicative Participation Item Bank
The Communicative Participation Item Bank (CPIB) measures communicative participation for community-dwelling adults across a range of communication disorders and life situations, including PD (Baylor et al., 2011). The CPIB consists of 10 items, with each item using a 4-point Likert scale ranging from 0 (very much) to 3 (not at all). The sum score range is from 0 to 30, with high scores indicating that the patient experiences less interference in participation. The CPIB was validated using the modern measurement method of item response theory (IRT), with strong reliability and validity (information > 10) in the range of –3.0 to just above +2.0 logits (Baylor et al., 2011).
Data Collection
In Study 1, the participants were asked to complete a survey provided electronically via Google Forms. The survey, which included 32 items and was written in English, was comprised of demographic questions, as well as (1) the Stigma Scale for Chronic Illness-8 Items (SSCI-8); (2) the Katz Index of Independence in Activities of Daily Living (Katz ADLs); (3) the Lawton Instrumental Activities of Daily Living Scale (Lawton IADLs); and (4) the Communicative Participation Item Bank (CPIB). Prior to launching the survey, a pilot test (n = 6) was conducted to determine whether the survey length was appropriate and the questions were easy to comprehend. Following recommendations from the pilot test, a definition was added to three items of the Katz ADLs—(1) transferring: movement from one place to another; (2) continence: the ability to control movements of the bowels and bladder; and (3) feeding: the process of eating. The survey was posted on the MPDA’s social media platforms (Facebook and WhatsApp) from February 2021 to June 2021 during the COVID-19 movement restriction order.
The research team who were fluent in both English and Malay languages contacted the Study 1 participants via phone call and asked if they were willing to participate in a follow-up, semi-structured interview (Study 2). The interviews were conducted via teleconference (Google Meet) due to the COVID-19 pandemic lockdown in dual languages (English or Malay depends on participants’ familiarity). A set of interview questions were developed based on the key constructs included in the Study 1 survey. The study objectives were briefly explained to all of the participants prior to the interviews, and they were asked to share their perceptions living with PD, the challenges they experienced in daily life and communication due to their condition, how they overcame the challenges, and whether their experiences were related to self-stigmatization. Each interview was conducted in the preferred language of the participant. The duration of the interviews ranged from 30 to 45 min. All interviews were video-recorded and transcribed verbatim.
Data Analysis
For Study 1, the demographic characteristics of the participants and their responses on the survey items were summarized using descriptive statistics (i.e., mean and standard deviation) for continuous variables (e.g., scaled scores) and frequency and proportion for categorical variables. In addition, a bivariate correlation was computed (Pearson, Spearman, or point-biserial, depending on the nature of the distributions) between the demographic variables, self-stigma, limitation in daily living activities, and communicative participation. Lastly, ordinary least square (OLS) regression was conducted to evaluate the effects of self-stigma (independent variable) on basic and instrumental activities of daily living and communicative participation (dependent variables) while controlling for key demographic factors. The analyses were conducted using SAS 9.4.
For Study 2, all raw data, such as audio recordings and interview transcripts, were coded with a unique identifier to represent each participant (e.g., participant code). Raw data were kept in a centralized repository (a secure network site with folders for each type of raw data) to perform an audit and to have a method of verifying the accuracy of data analysis and interpretations. One undergraduate speech-language pathology (SLP) student transcribed the audio recordings of the interviews and translated them into English languages. Another undergraduate SLP student reviewed each transcript’s accuracy for consistency of data (Chu et al., 2023). Verbatim transcriptions were analyzed using the six phases of the thematic analysis model (Braun & Clarke, 2006). The analysis proceeded in the following steps: (1) familiarizing with data through transcribing, reading, and re-reading, (2) generating condensed meaning units and codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing a report. Any content given by caregivers present during the interviews and/or information unrelated to the objectives of the study were excluded from the analysis.
Results
Study 1
Table 1 presents the demographic profile of the Study 1 participants (N = 25). Their mean age was 64.60 ± 9.09 years. Most of the participants were in the age range of 50 to 69 years old (n = 17) and the majority were diagnosed with PD between those ages (n = 17). Four participants were under 50 years old and four partcipants were over 70 years old at the time of onset. The race of the majority of the participants was Chinese (n = 12) and Malay (n = 8). The male to female ratio was 60:40 and most were married (n = 19). In addition, 21 participants were unemployed and about half earned less than 500 Malaysian Ringgit (RM) per month (about 106 United States Dollars as of November, 2022). The participants self-identified their stage of PD: six participants were in Stage 1 and had symptoms on only one side with a minimal disability; five participants were in Stage 2 and had symptoms on both sides but their balance was stable; nine participants who were in Stage 3 reported having a mild to moderate disability; two participants in Stage 4 reported having a severe disability but were capable of walking and standing unassisted; one participant in Stage 5 were confined to a bed or wheelchair unless assisted; and the remaining two participants were in unknown conditions.
Demographic Characteristics of Study 1 Participants (N = 25).

Table 2 shows the participants’ responses on the SSCI-8 items. The most frequently perceived stigmatization involved the feelings of being avoided, excluded, treated unkindly, and treated as if the illness was their fault. The overall prevalence of stigma was 96% in this sample when the cut-off score of 8 was considered. The distribution of the responses on the Katz ADLs items appears in Table 3. The vast majority (96%) of the participants were fully functional, indicating that they could manage basic activities independently. Table 4 presents the response distribution of the Lawton IADLs items. All participants were able to operate their phone and the majority were capable of handling finances (96%), housekeeping (88%), and laundry (80%). More than half of the participants were unable to shop for (44%) and prepare food (36%) on their own. The participants’ responses on the CPIB items are shown in Table 5. They experienced interference due to their condition particularly when talking with strangers, communicating while out in their community, during lengthy conversations about a topic of interest, and when attempting to persuade a friend or family member to see a different point of view.
Distribution of Responses on the Stigma Scale for Chronic Illness (N = 25).

Distribution of Responses on the Katz Index of Independence in Daily Living Activities (N = 25).

Distribution of Responses on the Lawton Instrumental Activities of Daily Living Scale (N = 25).

Distribution of Responses on the Communication Participant Item Bank (N = 25).

Table 6 presents the bivariate correlations among the study variables. The SSCI-8 score was strongly and negatively correlated with the Katz ADLs score (r = −.47, p < .05), suggesting that IwPD who have lower self-stigma would have greater ability and independence to conduct basic daily activities. The stigma score was also negatively related to the Lawton IADLs score; however, the correlation was in the small to moderate range and non-significant (r = −.21, p = .31). There was a strong, negative correlation between the stigma score and the CPIB score (r = −.41, p < .05), suggesting that IwPD who have greater self-stigma experience less interference in communication due to their condition.
Correlation Between Demographic Variables, Self-Stigma, Communicative Participation, and Daily Living Activities (N = 25).
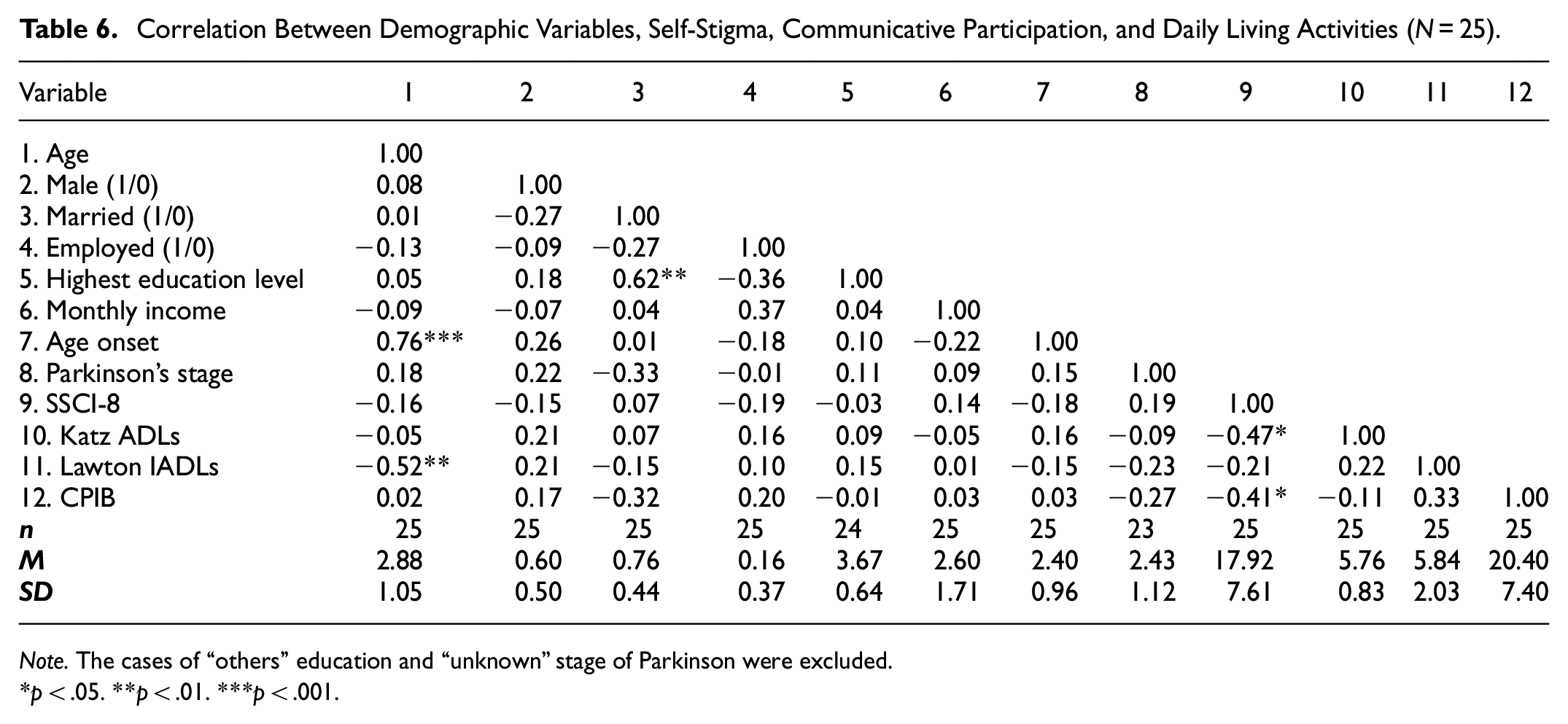
Note. The cases of “others” education and “unknown” stage of Parkinson were excluded.
p < .05. **p < .01. ***p < .001.
The results of OLS regression further confirmed the relationship of the variables. As shown in Table 7, the effects of self-stigma on daily basic activities (b = –0.06, p < .05, partial η2 = 0.28) and instrumental activities (b = –0.36, p < .10, partial η2 = 0.22) were considerably large and significant, even when the key demographic variables were controlled. The effect of self-stigma on communicative participation was in the small to medium range and not significant (b = –0.07, p = .25, partial η2 = 0.10).
OLS Regression Results (N = 25).

Note. The cases of “others” education and “unknown” stage of Parkinson were excluded.
DV = dependent variable; ES = effect size (partial η 2).
Study 2
Table 8 presents the profiles of the participants (N = 9) who were interviewed. Each participant was given a numeric identification (PD 1–9) to maintain confidentiality. Half of the participants were female (PD 1–4) and the others were male (PD 5–9). Their mean age was 65.22 ± 8.03. Four participants were in the age range of 70 to 79, three were in the age range of 60 to 69, one participant was in the 40 to 49 age group, and one participant ranged in age from 50 to 59. Eight out of the nine participants were married. The racial composition of the participants included seven Chinese, one Malay, and one who identified as “other.” For all of the participants, the range in years since receiving the diagnosis of PD was from 3 to 20 years. Table 8 also includes each participant’s self-identified stage of Parkinson’s disease, which were obtained from their responses in the questionnaire used for Study 1.
Profile of Study 2 Participants.

PD = participants with Parkinson Disease; SRS = self-report symptoms.
Table 9 presents the summary of thematic analysis collected from the semi-structured interviews. Five main themes and 18 subthemes emerged from the interviews: “challenges in performing ADLs due to PD,” “speech and communication adaptations due to PD,” “psychological responses toward one’s own Parkinson’s disease symptoms,” “self-stigmatization with impacts on self-concept” and “perception formation of Parkinson’s disease resulting from self-stigmatization.” The verbatim reporting of participants that were made in their native colloquial English are quoted directly rather than being edited into more formal language. However, Malay translations are reported in Standard English.
Summary of Thematic Analysis From Semi-Structured Interviews.

Theme 1: “I Can’t Wear My Pants”: Challenges in Performing ADLs due to PD
All of the participants commented on the physical symptoms they experienced due to PD, such as loss of balance, weakness on one side of the body, and tremors. Most of the participants were mobile and half were independent in performing their daily activities. However, there were times when they felt a lack of energy and fatigue, required a longer time to do things, and assistance from family members. Seven participants shared their experiences on how they coped with the limitations they encountered. Four of them (PD 6, PD 1, PD 2, and PD 4) required a longer time to complete simple daily tasks, such as dressing. PD 6 reported: “Most of the time I can do by my own, but some takes times to do,” and PD 1 stated: “I cannot wear my panty…because you need to wear panty, but my hand no energy. How to wear? So you need to have more than half an hour in the toilet.”
In some cases, such as the one for PD 4, the ability to perform simple tasks independently was possible; however, if in a rush, she required help from her sister. According to PD 4: “If I’m not in a rush, I can manage all that myself. If I’m in hurry, like late or something, then I need help.” PD 2 also reported on the same challenge by stating: “Like me, because of Parkinson, so I walk slower.”
Three participants (PD 1, PD 3, and PD 9) reported requiring assistance from family members, such as their spouses and children, to perform their daily activities, including dressing, walking, and driving, due to their condition. One participant (PD 3) said: “My husband also always leads me if I walk, hold my hand, or push my wheelchair.”
Theme 2: “I Need to Speak Louder”: Speech and Communication Adaptations due to PD
Based on the impact of PD on speech, the participants’ communication breakdowns were mostly due to reduced speech intelligibility as a result of speaking in a soft tone. They acknowledged their condition caused their communication partners, which included their children, spouses, and close contacts, to be unable to hear their speech and understand the words they were saying. The participants reported feeling frustrated when communication breakdowns occurred between them and their loved ones due to the limitations they were experiencing. PD 3, PD 6, PD 5, and PD 4 reported they realized they needed to speak louder to emphasize certain words, especially when communication partners said they were unable to hear them. PD 6 stated: “Definitely, because that I realized that I must speak louder when want to emphasize the words more. Even my wife cannot understand me.” PD 3 reported: “They said I’m speaking in the very soft tone, in the very low tone. Sometimes my husband cannot hear me. Sometimes my children also will ask, ‘What do you say?’”
In order to improve their speech, three participants (PD 2, PD 5, and PD 4) reported they practiced vocal exercises that they had learned from speech therapists. Due to the realization that their speech had declined over time, they were currently undergoing speech intervention sessions with clinical students from a university on a weekly basis. For them, the exercises helped them improve their oral muscles and speech quality. PD 2 reported: “I’m out of tune. I’m become monotone. Even speaking now isn’t it one tone only, so need exercise.” PD 5 expressed: “When I learned exercise my face, my tongue. In fact, that way more help with the move and effect how you do the sound.”
The participants did not just experience difficulty in communication due to the way they sounded. They also experienced difficulties participating in long conversations or group conversations. Three participants (PD 1, PD 7, and PD 3) reported the need to use alternative ways to successfully participate in conversations with friends and relatives. One of them, PD 7 said he made things short and fast in conversation, since his PD condition limited his ability to sit and focus for a long time. PD 1 and PD 7 reported they raised their hands when they wanted to state their thoughts in a group conversation, since they could not verbally interfere. PD 1 mentioned: “So I just, hands up my hand and say stop…Say I have my opinion. I need to talk now.” PD 7 stated: “I need to make it short. I see people, so I have to make it fast.”
Theme 3: “Parkinson Has Many Stages”: Psychological Responses Towards One’s Own Parkinson’s Disease Symptoms
All of the participants understood the degenerative nature of PD and acknowledged that there were stages in the disease, which were presented by changes in motor symptoms manifested by the disease. Most of them were aware of the current physical limitations they were experiencing. PD 2 and PD 8, who self-reported themselves in stage 1, the “honeymoon stage,” had experienced few changes in their movement, such as loss of balance. Nevertheless, their symptoms did not interfere with their daily activities and communication, as indicated by PD 8: “Can still in stage 1, but I just be more careful on my movement, because there’s will be tripping, fall. Yeah, that’s why that calls honeymoon stage.” PD 2 reported: “Mine is still early stage. Parkinson has many stages. Mine was only the early stage. Still, I’m progressed slowly deteriorating, but I’m still okay.”
The PD 3, PD 4, and PD 1, who self-reported themselves at stages 3, 5, and 6, respectively, had experienced more severe physical symptoms, including cramped legs, weakness in one side, and the inability to move. Their limitations affected their ability to do even simple tasks in daily life, such as walking and moving objects. PD 1 reported: “Because now my, more serious is now my leg is cramped, and cannot walk.” PD 4 stated: “It’s the truth, every bowl that I carry in the house, I broken them.” PD 3 also reported: “I cannot sweep anymore because I’m not balanced. I have to sit down to do a lot of things to be more stable.”
After being diagnosed, the participants reported seeing their condition gradually decline over time. PD 9 said his condition became worse after 2 years of receiving a diagnosis. In his early years, the symptoms were not severe, similar to the current condition reported by PD 8, who had only been diagnosed for 1 year and had not experienced many symptoms. One of the participants, PD 7 reported he had lost the ability to control his balance, and PD 2 reported she slowly lost her tone in speech and became monotone. According to PD 7: “But then slowly I realize that I’m starting to lose my ability to balance properly. My leg feel a bit tired, my left side feel weak, and all that thing, and realize that something is not right.”
Some participants reported that their declining physical condition made them less independent and they required assistance from others with performing daily activities. PD 3 reported: “Over the years, I gradually decline and I need more help in my daily life. Like I need to sit down to bathe.” PD 9 said: “My daughter drive me. I don’t drive already. I cannot afford to.”
The participants also expressed concerns about the later symptoms they may have. Two of the participants (PD 2 and PD 5) met other IwPD through group therapy and their involvement in the PD support group in their state. Based on these experiences, they were exposed to the later symptoms of PD and became concerned. PD 2, who met another IwPD in a late stage of the disease via group intervention, became traumatized and decided to stop treatment: Actually, in general hospital previously, they also did, did like group therapy. In there, I encounter Parkinson patient at late stage. It was very traumatic experience for me. So, so scary. Scary of the late symptom. Then, I don’t go anymore. It, it traumatizing. (PD 2)
Four participants (PD 7, PD 5, PD 1, and PD 8) recognized that medication improved their PD condition. Before taking medication, they felt tired and required more effort to perform simple tasks, such as taking a bath. However, after taking prescribed medication, they became more independent with physical activity and communication. PD 7 stated: “I do everything by myself. Again, the medication helps me. Before medication, it that I have more effort to put in, to take my bath, put on my clothes and all that.” PD 8 reported: “But I spot drastic improvement with and without Madopar, your communication, your movement. That help. Madopar really helps a lot.”
Four participants (PD 6, PD 1, PD 8, and PD 7) shared their experiences with accepting their condition. They reported it took them a while to accept their PD condition and adjust to their situation. PD 1 shared that she was now able to explain her condition to strangers compared to earlier years: “Now it’s okay. I can, I’ll told her that I have this disease and I ain’t got no choice to move like that.” These participants were also involved in a support group through MPDA, which allowed them to stay connected with other IwPD and to slowly learn to adjust to their changing environment and condition. For one Malay participant (PD 8), the acceptance of his condition was attributed to his religious beliefs: And furthermore, to me, we as Muslim, this thing come from Tuhan (God). So, you already in a good health, so be grateful la. Then whatever comes to you now, just take it step by step. This thing have its own reason; we don’t know (PD 8).
Theme 4: “You Tend to be a Bit Withdrawn”: Self-Stigmatization With Impacts on Self-Concept
All of the participants reported experiencing changes in their social lives due to their PD condition. Two participants (PD 7 and PD 4) expressed they were socially withdrawn. When their condition was not optimal, they did not go out into the community to engage in activities, such as participating in shopping tasks or buying food from stalls. They based this decision on their feeling weak, experiencing difficulties with walking, and being at high risk of being pushed by others, especially in the crowd. According to PD 7: “You tend to be a bit withdrawn and because of your condition making you weaker. And when you want to walk or so, you have a problem. You don’t want to do anything.”
PD 2, PD 7, and PD 1 also did not want to engage with other people and minimized their interactions, especially with people outside their close circle. These three participants participated in online activities with the MPDA, which one of the participants (PD 2) reported she enjoyed, doing, since they only needed to show their face and not many interactions were required. In addition, all three participants mentioned that other people in the MPDA tended to not divulge whether they had the disease. According to PD 2: “Online group? Yeah okay, because, we, we didn’t see each other, only face one. So I’m okay, I like it.” PD 3 stated: “I don’t want to let people know that I have PD. I want to pretend that I am normal.”
Five participants (PD 1, PD 2, PD 3, PD 5, PD 6) expressed the loss of their social roles as individuals, committee members, parents, and employees. Two participants, PD 3 and PD 6 reported that their physical limitations restricted them from doing their hobbies. For instance, PD 6 reported he used to enjoy reading books, but now that his hands shake consistently, he has trouble flipping the pages, so he has stopped reading books: “I used to read a lot. But reading is difficult for me now, not because of my eyesight or anything, but because one of my hand shakes. So, it’s difficult to turn the page.”
PD 3 reported she felt she no longer belonged to the community, as people started to look at her differently: I can feel that some of them feel they want to look away, you know. They don’t want to look at you, and some of them actually come forward to help you: “May I help you?,” which is very very great. Some of them maybe think that we are, we are the aliens you know. We don’t belong to a community. (PD 3)
PD 6 also reported a similar experience: “But I am too old for them to think I’m dangerous. Well, because you look out of place. So you feel uncomfortable.”
Some participants also reported that having PD caused them to lose their role as a parent as they struggled to adjust to their condition. PD 1, a mother to three teenagers, felt she had neglected her duties as a parent after receiving a PD diagnosis. She also felt she had burdened her eldest son by having him take on the parenting role: The second and third (her children). They didn’t know much what happened to me. I think my condition affecting them really much, because he need to take care of his brother. Take care of his brother and then affecting his curriculum- (PD 1)
Although some participants were diagnosed with PD before retirement, most reported they were diagnosed after retiring. The participants who were still employees felt that their efficiency and competency in performing their work tasks had declined, and they could not continue carrying on their duties. They were slow at their jobs and struggled with tasks that required high cognitive abilities. PD 5 reported: I have first at work and I started to get affected by Parkinson’s. I did not know anything. I used to do my job and didn’t think. I didn’t realize I have slow motion talk, and I was do my job very slow. (PD 5)
The participants were also aware of the stigma they received from the community due to the symptoms manifested by PD in both physical and communication aspects. Most of the stigma they experienced came from strangers who were not aware of the disease. Two participants (PD 1 and PD 6) shared about situations when their body or hand kept shaking and people started to look at them. PD 6 said: “Know my right hand shakes, for instance. So everybody look at my right hand and see wonder what’s wrong with him.” PD 1 reported: “My hand is shaking, shaking all day, so the other peoples look at me as strangers, as aliens.” The participants reported that when people looked at them, the participants perceived the public’s stares as a negative stigma. PD 5 reported that when he struggled with words and could only stay still and stare, people looked “funny” at him: “They look you funny because sometimes when you talk, you suddenly freeze. And you look, empty stare, staring like nobody.”
Theme 5: “You Feel Emotionally Upset Before People Can React”: Perception Formation of Parkinson’s Disease Resulting From Self-Stigmatization
All of the participants were aware that their condition caused others to see and treat them differently. The actions and perceptions of others toward them emotionally affected the participants. However, the participants tried to avoid the stigma. Several participants (PD 2, PD 3, PD 4, and PD 8) reported that they tended to avoid self-sympathizing behaviors due to their PD condition. Therefore, they avoided revealing their condition to other people and behaved like a normal person and as a part of the community. PD 2 reported: “Yes. I mean, when you tell people that you have Parkinson’s, you yourself, uh, feel emotionally upset before people can react, even. So, I normally don’t reveal to people lah. I don’t expose that also, except in certain groups.”
PD 4 shared that she tends to make jokes about her condition to avoid having others treat and look at her differently. “I mean if I feel limited and I see people who are healthy and strong, and I say ‘Aiyo, I’m malu aih (shameful), you are too strong and I can’t. I make a joke a bit,”
Lastly, more than half of the participants (PD 5, PD 1, PD 9, PD 7, and PD 3) were involved in a support group or PD association in their area to interact with other IwPD. Their interactions with other IwPD made them feel like they were not alone, since everyone experienced the same condition and symptoms, such as dirtying the floor while eating. In addition, their involvement in these groups made them happy and excited, and they felt like they had friends and someone who understood them better than their family members. PD 5 expressed: “You can get, like, be playful, cause nobody gonna look strange. Yes, like I have a little heaven.” PD 9 stated: “You know ah, that’s my family also unhappy with how I eat. Because ah, with PD, we normally dirty the floor. When I was eating with him, I got friend.”
Discussion
This study explored the relationship between self-stigma, activities of daily living, and communication participation among IwPD. The results revealed a high prevalence of self-stigma among IwPD. Our study found that self-stigma had a negative correlation with activities of daily living and communication participation. The strong correlation between self-stigma and communication participation is an indication that people who face more interference with communication tend to have higher self-stigma. Regarding activities of daily living, the results showed a strong correlation between self-stigma and ADLs and a weak correlation with IADLs. In study 2, the descriptive experiences of participants regarding their limitations due to PD in their daily lives and communication participation were obtained. Based on the participants’ responses, five themes and eighteen subthemes were identified related for Study 2: “challenges in performing ADLs due to PD,” “speech and communication adaptations due to PD,” “psychological responses toward one’s own Parkinson’s disease symptoms,” “self-stigmatization with impacts on self-concept,” and “perception formation of Parkinson’s disease resulting from self-stigmatization.” Based on these themes, it can be concluded that the IwPD in this study faced difficulties with daily living activities and communication participation due to their condition, which led to self-stigmatization. However, several strategies were used by these IwPD to cope with their limitations and minimize the self-stigma they were experiencing.
Psychological Responses Towards One’s Own Parkinson’s Disease Symptoms
All of the participants shared their self-perceptions of PD and their current condition. Several participants reported only feeling minor changes during the early stages of the disease, such as feeling unbalanced at times. According to Gazibara et al. (2017), after a 2-year follow-up with IwPD, not many differences were reported in gross motor skills; therefore, the authors suggested a longer-term follow-up of the disability. In our study, the participants who were in later stages of the disease or who had been diagnosed for more than 5 years reported experiencing more severe symptoms, such as being unable to walk and dress. The participants acknowledged that medication helped alleviate their tremors and fatigue (Bhidayasiri & Tarsy, 2012) especially during the later stages of the disease, when the dose of the medication was higher (Gazibara et al., 2017).
Furthermore, the participants were aware of the stages of PD and the degenerative nature of the disease, which caused several of them to feel apprehensive about the later stages of PD. After observing IwPD in the later stages of the disease during face-to-face therapy, one of the participants felt traumatized and switched to online therapy. Considering these concerns, the intervention provided by healthcare professionals should also address an IwPD’s psychosocial and emotional condition, especially with regard to coping with their overall life (e.g., social life, daily activities) after receiving a diagnosis of PD. Younger IwPD with an early onset of the disease also struggle to cope with readjusting to new social, familial, and professional roles, and the prevalence of self-stigma in this age group is higher. Self-stigma also tends to decrease in IwPD, as the disease progresses, the ability to accept the illness over time may be helpful, in addition to receiving the right patient education (Lin et al., 2022).
Self-stigma
Chronic neuropsychiatric disease patients are more prone to experience stigma throughout their lives (da Silva et al., 2020). Based on our results, IwPD experienced self-stigmatization due to their illness and the prevalence was high. This finding is consistent with previous research that has demonstrated the existence of internalized stigma in progressive neurological disorders, including PD (EFNA, 2020; Hou et al., 2021). Corrigan et al. (2009) described a three “A”s process that IwPD need to apply to experience self-stigma: aware, agree, and apply. The majority of our participants reported they were being avoided, excluded from activities, treated unkindly, and blamed for their illness. This indicated that they were aware of others’ attitudes and stereotypes toward their condition and how PD affected their daily activities and communication. Based on their agreement with these stereotypes, they experienced psychosocial effects, such as reduced self-esteem, social isolation, and depression, which occur after an IwPD applies these stereotypes to themselves (Elliot et al., 2019).
The participants in our study expressed their struggles with self-stigmatization as a result of the impact of the disease on their mental and emotional health. Based on the analyses of the results in our study, the participants tended to avoid engaging in self-pity and interacted with other IwPD. The methods they used to keep themselves from engaging in self-pity included not telling people about their illness (Elliot et al., 2019), seeing themselves as normal, and making jokes. According to Nilsson et al. (2020), IwPD present a variety of copying styles toward PD, such as “social support,” “optimistic,” and one of the most stable styles: “humor.” Considering that having an illness that reduces independence and has negative impacts on self-identity contributes greatly to low self-esteem and efficiency in IwPD, maintaining a positive self-concept, such as not revealing their illness and treating themselves as normal, is an inner response to maintaining their self-worth (Corrigan et al., 2009). Support-seeking behavior was also one of the distinct coping patterns identified in the IwPD in our study. Most of the participants were actively involved in support teams and PD associations, such as MPDA. They reported that because of their involvement in these groups, they felt more accepted and supported, since they were all in “the same boat.” Previous research has also indicated that a positive group identity is likely to help IwPD overcome self-stigma (Lee et al., 2018).
The difficulties IwPD faced due to their tremors, fatigue, and rigidity significantly impacted their lives, especially their social lives. Several participants reported they socially withdrew and did not want to interact with other people due to their disease. For instance, one of the participants reported he avoided interacting with other people because he had trouble moving and sitting for a long time. This finding is in line with two qualitative studies that found IwPD avoided socializing and reduced their participation in conversations with caregivers and community members (Swales et al., 2021).
Several participants also chose to not let other people know about the disease. This is considered a stigma reaction, which is highly related to their decreases in self-esteem and efficiency (Elliot et al., 2019). Moreover, their limitations due to having PD caused them to lose their social roles as individuals, parents, committee members, and employees (EFNA, 2020; Jonasson et al., 2020). They were also aware that others looked at them differently and perceived them as aliens or dangerous people. This may be closely related to the limited knowledge and awareness of PD in Malaysian society, and IwPD are aware of that (Alyamani et al., 2018). Therefore, actions are needed to increase the public’s education about and exposure to PD in Malaysian society, as this would lead to improvements in both public and individual attitudes toward PD. Lastly, it would also be advantageous to raise self-awareness about the symptoms of PD and encourage IwPD to seek help (Nizam & Nen, 2022).
Association Between Self-Stigma and Activities of Daily Living
The results of our study showed that the majority of IwPD participants were fully functional and performed their ADLs independently. Regarding their performance of IADLs, which are more complex and demanding activities, the participants in our study were fairly independent. Nevertheless, although some participants were still able to manage their finances and housekeeping, more than half reported they could not do errands or prepare their food. Previous studies have also found that performing IADLs resulted in poorer motor performance in IwPD due to overloads in cognitive functioning and processing, including in IwPD in the early stages of the disease (Foster & Doty, 2021).
In these factors, we also need to consider the gender and cultural division of household work among the participants, which, in Asian culture, favors women over men (Boo, 2020). The majority of our participants were male and married, and all were from different cultural backgrounds. Therefore, this could possibly be one of the factors that influenced the results of the participants’ independence in performing IADLs, since they may not have been responsible for doing the tasks either before or after being diagnosed with PD.
One of the aims in this study was to identify the relationship between self-perceived stigma and activities of daily living. We found that there was a negative correlation between self-perceived stigma and activities of daily living, indicating that IwPD who have higher self-stigma tend to have lower functionality or independence in conducting ADLs and IADLs (da Silva et al., 2020). However, self-perceived stigma was more strongly correlated with ADLs than IADLs in spite of the fact that IADLs were reported to be more challenging for the participants. This outcome may be relatable to a study that found IwPD reported their gross motor abilities were more significantly affected than fine motor abilities, and that not much changed in their IADLs across a 2-year period (Gazibara et al., 2017), suggesting that physical limitations, which involve gross motor skills, were more noticeable. Moreover, difficulties with performing ADLs may be more apparent to others than challenges with IADLs, affecting self-image and self-esteem (Angulo et al., 2019) and triggering higher self-stigma in IwPD.
Based on our analysis of the qualitative data, the independence of the IwPD in our study was dependent upon their prescribed medication. They reported they faced difficulties from time to time, which may be attributed to the “on-off” phenomenon caused by the effects of medications, such as Madopar and Levodopa. During the “on” period, the medication was working and the symptoms were under control, while during the “off” period, the medication was wearing off, and their symptoms became more apparent (McNamara & Lakhan, 2020). The physical limitations reported by the participants included handshaking, loss of balance, and fatigue, which are those commonly reported by IwPD (Abasi et al., 2020; Jonasson et al., 2020). Therefore, the IwPD required alternative ways to perform their ADLs, even simple tasks like walking and dressing. Several participants reported they required more time, whereas others required assistance from family members and relatives to complete the activities. For IwPD, the reduction of independence and shift in roles and family dynamics as a result of having PD lead to reductions in self-esteem, loss of identity, and they perceive themselves as a burden (Angulo et al., 2019; Elliot et al., 2019). According to Tan et al. (2019), self-stigma among PD patients is also linked to a significant caregiver burden.
Association Between Self-Stigma and Communication
The results of Study 1 indicated that IwPD encountered the most interference when communicating with strangers and community members, during lengthy conversations, and when trying to persuade a friend or family member to see a different point of view. According to the findings of a study by Johansson et al. (2020), even close-contact caregivers tended to misunderstand IwPD due to difficulties with hearing them as a result of the IwPD’s changes in voice and the IwPD’s challenges with word-finding difficulties, fatigue, and changes in body language (e.g., facial expression) during conversation. Other studies have also reported familiar findings related to language aspects of communication in IwPD, such as difficulties with word-finding and topic management. However, voice quality issues are the most highly reported, with more than 80% of IwPD saying their soft voice and unclear speech lead to communication breakdowns (Altaher et al., 2020; Swales et al., 2021). Considering that communicative interactions with those close to them are challenging, communicating with strangers is even more difficult for IwPD. Moreover, since public awareness and knowledge toward PD are still low (Alyamani et al., 2018; Youn et al., 2016), others may not know how to react toward IwPD during communicative interactions and unconsciously trigger stigmatization toward the population. Although speech characteristics in PD were not addressed in our quantitative study, they were mentioned in our qualitative study.
Another objective of our study was to identify the relationship between self-stigma and communication participation among IwPD. Our results showed a significant relationship between self-perceived stigma and communication participation in the PD population. This finding indicates that IwPD who face more interference in communication due to their limitations tend to have greater levels of self-stigmatization. These results correlate with the studies reviewed by Maffoni et al. (2017), which found that IwPD experience stigma related to their communication problems and to impairments in their oral functioning (e.g., dysarthria) and body language (e.g., facial masking). The changes in their condition cause IwPD to experience negative emotional reactions, such as frustration and shame (Angulo et al., 2019). As a result, instances of reduced socializing and social withdrawal increase for IwPD (Altaher et al., 2020; Elliot et al., 2019; Johansson et al., 2020; Swales et al., 2021), triggering their self-stigmatization behavior.
Through semi-structured interviews with the participants, we found that the majority of the participants reported that their communication breakdowns were primarily caused by poor vocal quality. This finding was supported by Swales et al. (2021), who reported that 85% of IwPD reported their voices were perceived as soft and not clear. The participants described being neglected by family members during conversations, and their communication partners misunderstood their words and were unable to hear them. Therefore, the IwPD realized they needed to speak louder and emphasize certain important words in conversation. Most of the participants actively participated in MPDA’s online activities and teletherapy conducted by the speech department at the Universiti Kebangsaan Malaysia (UKM). Therefore, they performed their assigned vocal exercises to improve their speech. Several participants also reported having difficulty participating in lengthy and group conversations. Several studies have also described the language aspects that affect IwPD, including difficulties with production, pausing, following group conversations, and topic management (Smith & Caplan, 2018; Swales et al., 2021). As a result, several IwPD in our study found alternative ways to minimize communication breakdowns, by making conversations short and raising their hands to participate. Since speech and communication are essential aspects of one’s daily lives, their challenges in these areas caused IwPD to experience negative emotional reactions, such as social withdrawal, reduced self-esteem, and less life satisfaction (Chu & Tan, 2019; Swales et al., 2021). However, due to the COVID-19 pandemic lockdown, the IwPD had fewer opportunities to engage in social communication with others.
Mechanism Interplay Between Self-Stigma, Levels of Activities of Daily Living and Communication Participation
According to the mindsponge information processing mechanism (Vuong & Napier, 2015), two key elements in an individual’s psychological process are perceived information accessibility and trust. This mechanism illustrates how the mind receives and filters information, accepts or rejects values, and evolves in the process. Despite the intricate and dynamic nature of the mind’s information processing, it can be summarized into five main principles that shed light on the complex relationship between self-stigma, levels of activities of daily living and communication participation.
First, the theory proposes that subjective information particles, representing societal attitudes or personal experiences related to the stigmatized condition, must be present in the mind for processing. This internalization forms the foundation for subsequent cognitive processes and influences how IwPD perceive themselves in relation to societal norms. The information processing mechanism, characterized by multiple filtering processes and cost-benefit judgments, is influenced by a trust evaluator, reflecting the IwPD’s perception of the reliability of societal attitudes. IwPD with self-stigma may engage in a multi-filtering process, evaluating the trustworthiness of societal attitudes and making subjective cost-benefit judgments. Due to the perceived high costs of engaging in daily living or communication participation (due to potential judgment or discrimination), they more likely to avoid such activities.
This evaluative process is closely linked to the third principle, emphasizing the dependency of the multi-filtering process on the value system shaped by the mindset, specifically a set of core values. If the core values include self-acceptance and resilience, IwPD may be better equipped to challenge and overcome self-stigmatizing beliefs. Consequently, the outcomes of conscious and subconscious mental processes, including thoughts, feelings, and behaviors, are significantly influenced by these core values. For individuals experiencing self-stigma, the interplay between the value system and processing mechanisms can perpetuate negative self-perceptions.
Finally, the theory highlights that information particles related to stigmatized conditions from the objective world (environment) need to be within perceivable range to be absorbed into the subjective world (mind), emphasizing the dynamic interaction between internal and external factors in shaping mental processes. Overall, the mindsponge theory offerss a comprehensive framework for understanding the intricate connections between self-stigma, levels of activities of daily living and communication participation (Vuong, 2023).
By integrating the patient’s perspective and experiences, healthcare professionals can gain a better understanding of the impact of societal attitudes on self-stigma, thus influencing the overall well-being of IwPD. Incorporating a humanistic approach in healthcare, centered on empathy, understanding, and respect for the individual’s values, has the potential to alleviate self-stigma.
Limitations
Due to the movement restriction order and complete lockdown imposed in response to the COVID-19 pandemic, our team could not recruit PD participants face-to-face. Therefore, this may have affected our recruitment rate. Although our team recognized that collecting the Katz ADL and Lawton IADL online rather than in person might yield different results, due to the COVID-19 lockdown, this was the only way we could run the study. Future studies should examine whether there are any differences between in-person versus online data collection methods. Additionally, the MPDA secretary reported to our team that the majority of their PD members were exhausted and suffering from “survey fatigue” during this time period as a result of the association’s numerous requests for subject recruitment for other studies besides ours. This could possibly be another reason why our response rate was low. Furthermore, due to financial constraints on our part, participation in this study was entirely voluntary, with no compensation provided in exchange for participation. This may have also contributed to our low recruitment for Study 2, in which we only interviewed nine subjects (36%) to obtain more in-depth information regarding their experiences with PD and its impacts on their ADLs and communication participation.
In our study, we employed a combination of convenience and snowball sampling due to the challenges associated with accessing and identifying potential participants from the target population of IwPD. This approach is commonly used in research involving marginalized or stigmatized groups where conventional sampling methods may not be effective. However, we acknowledge that convenience and snowball sampling can introduce bias into the sample, as participants are not randomly selected from the population. Additionally, the small size of our sample limits our ability to generalize our findings to the target population.
Conclusion
This study demonstrated that PD-related limitations elicited self-stigma in IwPD and had a considerable negative impact on their overall well-being. More consideration should be given to self-stigma in clinical practice, since it is reversible. In order to effectively manage IwPD, healthcare providers must address the self-stigmatization factors that are triggered among IwPD due to their condition, with particular focus on the individual who is newly diagnosed with PD. Moreover, health-related organizations and PD associations must play a crucial role in educating and raising awareness of PD in our society, considering that self-stigma is related to both how an individual perceives their condition and the public’s attitudes and perceptions toward it.
Footnotes
Acknowledgements
The authors thank all participants who involved in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by the Universiti Kebangsaan Malaysia Prime Impact Fund (DIP-2022-008) and UKM (DPK-2021-010).
Ethical Approval
This research is partly supported by the Universiti Kebangsaan Malaysia (DPK-2021-010) and Sumitomo Foundation (208490, NN-2021-009). All participants completed a consent form and their responses were handled anonymously and de-identified prior to analyses.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.