
Abstract
Depressive disorders are a worldwide leading cause of health-related burden, and a subgroup of depression patients fail to respond to available psychopharmacological treatments, a condition called Treatment Resistant Depression (TRD). While evidence suggests that both traditional and group (IPT-G) Interpersonal Psychotherapy interventions are efficient treatments for depression, few studies have evaluated the effect of IPT on TRD. Qualitatively analyze an IPT-G intervention conducted with TRD patients using a deductive, theory informed approach, to explore how TDR patients understand, contextualize and apply IPT’s problem-areas throughout the course of the treatment. 10 IPT-G sessions were analyzed using Framework Analysis. Sessions were video recorded and transcribed verbatim, and participants’ accounts were coded with predetermined, conceptually derived codes that were based on the three main problem areas identified in IPT. Following IPT’s main problem areas, three themes were generated: “Mechanisms of change—Improving communication”; “Acceptance of loss”; and “Finding new roles—depression, role transition, and reclaiming life conditions.” Our analysis suggests that patients with TRD can benefit from IPT-G. Depression is seen as a chronic condition that deeply affects the lives of patients, and IPT-G was seen as a way of promoting change and regaining control. However, we identified that patients to whom IPT-G did not achieve the same effect in terms of symptom reduction have greater difficulty in acquiring and generalizing new interpersonal skills, and often were immersed in severe family or marital interpersonal disputes.
Plain language summary
Six patients with treatment-resistant depression were enrolled in a 10-session Group Interpersonal Psychotherapy (IPT-G). After intervention, two participants did not show improvement in depressive symptomatology, while four did. Qualitative analysis showed that patients with intense, hard-to-solve interpersonal disputes were identified in the group that did not improve symptomatically, and reported having greater difficulties to engage with IPT-G techniques. Patients who improved progressively found more adaptive ways of dealing with interpersonal disputes, particularly through employing ITP strategies in communication. The findings suggest that solving difficulties in interpersonal relationships may be associated with improvement in depressive symptoms in patients with treatment-resistant depression, suggesting effective change mechanisms and intervention for this population.
Keywords
Introduction
Depressive disorders are a worldwide leading cause of health-related burden (Benson et al., 2021; Ferrari et al., 2013). While a common mental health disorder, depression deeply impacts the lives of those who suffer from it, posing big challenges not only to individuals, but to families and communities. While there is a wide range of available treatments, including antidepressants and psychosocial interventions, the mechanisms through which these interventions work are not always clear. Moreover, depression is a highly heterogeneous disorder (Goldberg, 2011), and not all patients respond the same to available interventions.
Among those who suffer from depressive disorders, we call attention to the subset of patients that fail to respond to at least two antidepressant drugs at adequate dosage and time-period, a condition called Treatment Resistant Depression (TRD). In this condition, other factors that may be involved in the maintenance of symptoms, such as psychosocial factors, are not addressed (Kennedy et al., 2016). Previous research has shown the benefits of using psychotherapy in managing TRD (van Bronswijk et al., 2019), which may highlight the importance of understanding mechanisms through which psychosocial interventions may benefit these individuals.
In the midst of available interventions, Interpersonal Psychotherapy (IPT) is recommended in several guidelines for the treatment of depression (e.g., Ijaz et al., 2018;), IPT considers that depression is often caused, or heavily influenced by interpersonal problems (Klerman et al., 1984). It was originally designed to be a time-limited individual intervention. However, in a global context in which resources are scarce and demands are high, IPT has been adapted to be implemented as a group intervention (IPT-G) (World Health Organization, 2016). Group therapy is based on the idea that many of the difficulties people face in their lives may be understood as a cohabitation problem and groups offer a unique opportunity to learn to discriminate between dysfunctional and adaptive interpersonal patterns (Rothberg, 2017; Stuart & Schultz, 2016; World Health Organization, 2016).
While evidence suggests that both traditional (Cuijpers et al., 2011, 2016; Markowitz & Weissman, 2012; Souza & Fleck, 2013; Stuart, 2006; Weissman, 2020) and group IPT (Levkovitz et al., 2000; MacKenzie & Grabovac, 2001; Rothberg, 2017; Stuart & Schultz, 2016; Weissman, 2020; Wilfley, 2000) are efficient treatments for depression. To this moment, few studies have evaluated the effect of IPT on TRD. The available results tend to focus on individual ITP, showing improvements in depressive symptomatology using combined IPT and pharmacotherapy (Souza et al., 2016). However, evidence of using group IPT in this clinical populations is even more scarce: to this date, we found no trials aiming to evaluate IPT-G on TRD.
In this direction, qualitative studies may aid the understanding of how interventions work, and how change is promoted through them (Grote et al., 2021). Specifically in IPT, they can help practitioners and researchers to understand IPT problem-areas’ (Grief and Loss, Interpersonal Disputes, and Role Transitions) fit to the lived experience of patients, but also to understands how they interact with overall engagement with change mechanisms proposed by IPT.
In the present study, we aimed to contribute to this discussion by qualitatively analyzing an IPT-G intervention conducted with TRD patients. Using a deductive, theory-informed approach, guided by a pragmatist approach, 10 group therapy sessions were analyzed in order to explore how TRD patients understand, contextualize and apply IPT’s problem-areas throughout the course of the treatment. Moreover, we aimed to identify differences between patients who benefited from IPT and faced a reduction of symptoms after treatment and those who did not.
Study Design and Sampling
We selected seven patients (five women and two men) identified as having TRD. At the time, they were enrolled in a tertiary health service specializing in the treatment of depression in Hospital de Clínicas de Porto Alegre—Brazil, coordinated by the last author. They were already users of the service and thus sampled by accordance to the desired patient profile, and were offered the IPT-G treatment. In this study, were eligible patients between 18 and 65 years of age diagnosed with Major Depression Episode that failed at least two treatment courses with antidepressants, with proper dose and time considering the current episode. Overall inclusion and exclusion criteria for eligibility are described in Appendix A.
Participants attended 10 IPT-G sessions in addition to receiving treatment as usual (antidepressant medication). Sessions were conducted at Hospital de Clínicas de Porto Alegre (HCPA) by the first (psychologist and PhD candidate) and last author (psychiatrist). Both therapists have had formal training and are IPT-G certified. Previously to the group, each participant completed an individual interview to perform the Interpersonal Inventory and Interpersonal Formulation. Afterwards, 10 weekly in person sessions were conducted with all participants. Each couple of sessions had a pre-stablished goal, in order to address the three main problem areas within IPT and train related abilities, such as communication and problem-solving techniques (for further information on each session structure, refer to Appendix B). Sessions were 75 min each. The study intervention was conducted from January 8, 2020 through March 18, 2020. All sessions were video recorded and transcribed verbatim. All patients completed rating scales for depression (BDI-II; Gomes-Oliveira et al., 2012) and anxiety (BAI; Gorenstein & Andrade, 1996) at baseline and after the intervention. Symptomatic improvement in scales (see Table 1) was used to define whether participants benefited from the treatment. Study data were collected and managed using REDCap electronic data capture tools hosted at HCPA (Harris et al., 2009).
Results Pre- and Post-Intervention.

Data Analysis
Sessions were analyzed using Framework Analysis (FA) (Ritchie et al., 1994). A deductive theory-informed codebook was created based on IPT main problem-areas (Markowitz & Weissman, 2012; Mutamba et al., 2018; Stuart, 2006; Weissman, 2020). In this sense, participants’ accounts were coded with predetermined, conceptually derived codes that were based on the three main problem areas identified in IPT. The code “Interpersonal Dispute” was used when participants discussed disputes, arguments, and disagreements with close or significant others as well as the participant’s response to these situations. “Role Transitions” was used when discussions centered on life changes, such as loss of health, and its psychological, social, or interpersonal consequences. Lastly, “Grief” was used for situations related to death of people with a significant role in participants’ lives. Additionally, each problem area was sub-divided into positive and negative valence statements, understanding that positive changes in how participants dealt with these areas could indicate a response to treatment.
The final codebook was used to code the full dataset using NVivo version 16 (QSR International, 2002). Two researchers (MIPM and AV, both female and with a background in psychotherapy) coded the data in Portuguese. Researchers coded independently two sessions. Inter-rater reliability (IRR) of 0.87 (Cohen’s Kappa) among the coders was considered an indication of reasonable agreement (McHugh, 2012). After adequate IRR was established, sessions were single coded by one researcher.
Since the unit of analysis was an IPT-G course of treatment, data saturation was not a criterion for data collection or analysis. Instead, we understood the dataset as a closed unit. All transcripts were then checked by a senior researcher with extensive experience in IPT. Since response to treatment was of interest in the analysis, code queries were executed on NVivo stratified by response to treatment.
In addition to this stratification, the biopsychosocial/cultural/spiritual model played a significant role in theme generation. Drawing on IPT’s Interpersonal Formulation, the participants’ accounts were understood in relation to the multiple biological, psychosocial, cultural and spiritual processes that occurred in their lives. Thus, we understand that our work draws on representations of reality that are mediated by material and cultural aspects, which is aligned with a critical realist ontological perspective (Pilgrim & Rogers, 2002). As researchers, we understand that our clinical work has strong implications on the research findings here presented. Thus, our results are heavily influenced by clinical expertise, which guided the generation of the research question and further data analysis and reporting.
All stages of analysis and reporting were executed according to Consolidated Criteria for Reporting Qualitative Research (COREQ) (Appendix C) (Tong et al., 2007). In preparing the manuscript for publication, the original quotes were translated into English.
Ethics
This study was approved by the HCPA Ethics Committee (CAAE: 94975918000005327). All participants provided written consent to participate in the study before starting the IPT-G sessions. In the consent process, they were informed of the goals and objectives of the study, as well as consented to both use of scales and recording of each session. They were given the option to withdraw consent at any part of the study and were also informed that consent withdraw would not affect access to any services and/or future treatments in the Hospital. To ensure protection of confidentiality and anonymization of the data, all identifiable details given by participants during their interviews were omitted from transcripts.
Results
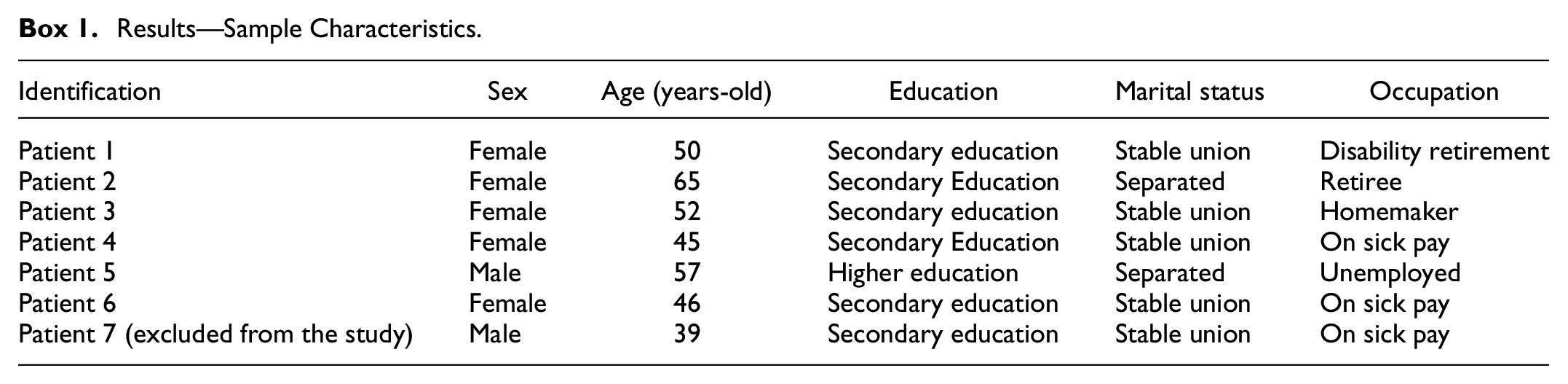
Six participants had full data available—five females and one male (Box 1). One participant (male) did not complete the IPT-G treatment and was excluded in the analysis. Anxiety (BAI) and depression (BDI-II) symptomatology scores are presented in Table 1. Prior to intervention, participants had a mean score of 32.66 on the BDI-II. For those who completed intervention, the mean score dropped to 21.16. In Table 1, we present individual results in regards to depression and anxiety for all participants who completed the intervention. Two of these participants (1 and 3, both female and with baseline severe depression) did now show improvement in depressive symptomatology, while four did.
Results—Sample Characteristics.
Individual results for all participants who completed the intervention. We here present pre- and post-intervention scores for both depression (BDI-II: Beck’s Depression Inventory—Second Edition) and anxiety (BAI: Beck’s Anxiety Inventory) symptoms. Additionally, clinical significance of each score and variation is also presented in the “comments” column.
In our qualitative analysis, we generated four themes (and one subtheme) that represented the overarching narrative across all respondents. They were: “Mechanisms of change—Improving communication,”“Acceptance of loss,” and “Finding new roles—depression, role transition and reclaiming life conditions.” Each theme highlights one of IPT’s main problem areas: interpersonal disputes, grief, and role transition (respectively). The generated themes, however, aimed to represent the representations, dilemmas, and other significant aspects of each problem area for the included participants. Thus, they highlight aspects considered more relevant to our participants, as well as the temporal aspect of the group intervention—when relevant, descriptions also aim to show how the problem areas’ conceptualization changed during the intervention, as well as how the techniques were employed by participants throughout the 10 weeks. For this, participant’s quotations in each theme also indicate the session in which it was provided.
Theme 1: Mechanisms of Change—Improving Communication
Across all respondents, interpersonal disputes were the central focus of accounts. Family and marital disputes were mentioned as causes of isolation, strain, irritation, and violence: There are certain things that just drive me mad. I feel like disappearing, being by myself. Leaving home. I’m not the same person anymore and this bothers them too. I got to the point of having a friend of mine telling me that I should occupy my mind, that I had nothing to do. (patient 4, session 8)
When facing these situations, patients would often express lack of control: “(I had) Such rage that if I grabbed her by the neck, I think I would tear her in half” (patient 2, session 4). Disputes were usually related to lack of dialogue, distrust, and isolation.
However, over the treatment, participants reported adopting adaptative attitudes to deal with conflicts. Communication strategies were the most common strategies mentioned: by using assertive forms of communication, patients perceived they could achieve better outcomes regarding disputes: “I didn’t like what you did, if you’re my friend and want to keep me as a friend, don’t do that to me again, because it made me very sad.” (patient 4, session 9).
In addition to improving communication, participants also reported engaging in evaluation processes aimed at avoiding confrontation, strain, and losses resulting from arguments with lack of control.
Because if I start lashing out at them and they at me, it won’t work. It won’t work, right? I don’t like this type of thing. And regarding relationships with people like that, it’s ok. Back when I worked in a factory, I used to be the boss. I had good relations with people. (patient 6, session 5)
As part of the IPT-G process, participants were able to reflect and ponder on protective and positive factors within interpersonal relationships. Among those, they mentioned choosing relationships that promote well-being, as well as reframing potential interpersonal dispute situations, such as coping well with divorce or separation, and owning up to their mistakes as an expression of emotional maturity. As a consequence of improving communication, accessing support and care, in spite of the fear of stigma, was also reported by the participants throughout the intervention: For the first time I was able to open up to my family, tell them what I’m going through, let them know how I feel and for the first time I heard from them that they love me and that I can count on them, and then this gave me strength to come again. (patient 4, session 2)
Subtheme: It Feels Like a Dead End—Difficulty in Engaging in IPT-G Techniques
While interpersonal conflict set the tone to most participants’ accounts, the subgroup of participants who did not benefit from reduced depressive symptoms by the end of treatment exhibited a different pattern of engagement with communication strategies co-constructed by the group throughout the treatment. Conflicting relationships and frequent arguments, particularly within the nuclear family, were often described, but participants who were less benefited by IPT seemed to be less willing to deal with conflicts in a resolutive fashion: I face a lot of conflict with my husband, with my family, I argue, I don’t want them to think I’m weak, because I’m not gonna be weak. I won’t let anyone tell me what to do, but I’m holding up, I know I’m holding up. (patient 3, session 4)
This was evident when, even when taking part in a brainstorming session to find possible solutions to problems, patients would say that the only possible solution for their problems would be death. Overall, they seemed to be unable to perceive alternative resolutions: I think that my best decision would be death. Because I think that the one thing I can do is take my own life and then it will be over. (patient 1, session 7) You know that I feel just like you do, for me it seems that death is the best thing. (patient 3, session 7)
This was often expressed by dismissal of proposed strategies and an overall pattern of diminished generalization of IPT skills and concepts. In the treatment, some participants had difficulty in meaningfully engaging in alternative strategies aimed at interpersonal relationships, both proposed by the group and the facilitators, struggled to develop and apply coping and communication skills to interpersonal disputes. Additionally, their family environment would constantly reinforce a negative assessment of these patients, which was echoed by them as a way of confirming the negative character of their personalities and actions: Then, as soon as I got back, he said: “See how bad you are? Look, poor little dog had an accident to show you that you’re bad”. (…) I know I’m really feisty, that I’m annoying. I know I’m bad, that it’s hard. (patient 3, session 7)
Theme 2: Acceptance of Loss
Along with interpersonal problems, patients’ narratives reported grief experienced in its negative valence. The sense of life losing its meaning following the death of a loved one is a manifestation of that: “When my mother passed, in 2014, I went with her.” (patient 5, session 2).
When faced with death, participants expressed a hard time overcoming grief. Difficulties in communicating distress and feelings triggered by loss were a common theme, but also feelings of loneliness.
Today for me it is very hard to accept the loss caused by death when someone dies. I don’t know why, I almost cry myself to death. I almost lose it every time a friend, a relative dies, God forbid. (patient 4, session 8)
Overall, coping strategies mentioned were aimed at diminishing negative feelings. Accepting and understanding loss was pictured as a difficult path, and participants relied on factors such as spirituality as a way to accept finitude. Additionally, caring for loved ones before their deaths was also related to an increased capacity to cope with loss. However, death was something of difficult assimilation, and making sense of it took years: I think what helped me accept it was, like, being my daughter’s mother. (…) And now I have a grandson, she got pregnant; then with this grandson it’s easier to accept. I lost her, but I’ll get a grandson. (patient 1, session 8)
Theme 3: Finding New Roles—Depression, Role Transition, and Reclaiming Life Conditions
All patients reported experiences of loss due to depression and viewed it as a chronic condition. Depression was described as “something close to being in hell,” something capable of transforming the way participants perceived themselves and their lives: Before I was somebody who… It is not that I don’t like people, but it’s just that I think that each person is so bad that I think that when depression is really strong, it is the same as being in hell. (…) I keep wondering: Am I to blame? It doesn’t heal, it won’t get better, and I’ll die. (patient 3, session 2)
Depression was, then, viewed by participants as an impeditive to agency and control of their own lives. This was due to feelings of persistent emotional pain, but also stress and a marked decrease in quality of life. This feeling of loss was normally accompanied by a sense of guilt about being depressed: “Today I blame myself when I get depressed, because it’s my fault, I am guilty of this, and I’m guilty of that and I argue all the time.” (patient 3, session 3).
The loss related to not being able to work and generate income associated with depression was also brought up as a negative experience connected to this role transition: “I was used to working, I have always worked in my life, always, always, always. And now I feel kind of useless. (…) We end up feeling like a dead weight.” (patient 6, session 3).
As the treatment unfolded, however, participants seemed to start acknowledging the need to play an active role when facing limitations imposed by their depression and other chronic diseases and to adapt to their new role. Patient 1, for instance, decided to start working: I told myself “I’m going to work”. It didn’t pay off, right? It didn’t pay off at all, but I showed up. I was happy for showing up. (…) I told myself: “Oh, well, I’m able to do that”. I have never done anything in my life, right? I have done plenty of dishes. Now I have to wait for my prescription glasses, I’ve just had my glasses made. I didn’t want to accept that I had to wear glasses, I didn’t want to accept it and now I had them made. Now I’m gonna have to wear them, right? (patient 1, session 8)
Reclaiming life and agency was a theme discussed by participants. To participants, the group also had a positive impact on recognizing their capacity to cope with depression: It is quite a different thing to listen to other people talking about their issues, compare them with yours in your head, and reach other conclusions, like, ‘gee, wait a minute, if she managed to solve her problems like that, why can’t I do the same?’. For me it was super nice, it still is. Here I share. It is different from mulling over your problems, or at best discussing them with your therapist in front of you. (patient 5, session 10)
At the same time, they emphasized they still need to face the sense of depression and pessimism that follows depressive episodes: In fact, I did improve, but in the past I didn’t think I could do it. You don’t see any future ahead, you remain in a negative mood and then when you’re fine, deep down you know you’re not… Then, when you feel bad, you think: “Will I get out of this? I think I won’t be able to do it”. And then, all of a sudden, things clear up, and you think life is very good. With depression, life is no good. (patient 3, session 9)
Discussion
The present study sought to analyze qualitatively IPT-G sessions delivered to Brazilian adults identified as having TRD. As means to analysis, we formulated an analytical plan based on IPT principles and stratified accounts by response treatment, which guided coding and construction of themes. Overall, as part of a structured intervention, participants made relevant progress in the way they dealt with interpersonal disputes, role transitions, grief, and loss. This improvement was both qualitative, per reported accounts, and in regards to overall depressive symptomatology.
Qualitatively, participants highlighted the relevance of the group modality, and the importance of sharing their experiences with people facing a similar situation and listening to other people’s experiences. This is consistent with previous literature that suggests the IPT’s ability to activate change mechanisms by enhancing social support, decreasing interpersonal stress, and improving interpersonal skills (Lipsitz & Markowitz, 2013). This may also be due to the fact that Brazilian culture is historically group oriented. In collectivist societies, such as Brazil, group therapies can present great value, especially since they leverage the sense of solidarity (Ortega & Wenceslau, 2020).
When looking specifically into the accounts of patients who did not exhibit a reduction in their depressive symptoms, we identified that it was harder for these patients to use the tools provided by IPT-G to deal with the problem area of interpersonal disputes. On the other hand, patients who improved progressively found more adaptive ways of dealing with interpersonal disputes, particularly through communication strategies, thus corroborating the IPT proposition that solving difficulties in interpersonal relationships through the use of better communication skills is associated with improvement in depressive symptoms (Cuijpers et al., 2011; Kennedy et al., 2016; Markowitz & Weissman, 2012; Souza & Fleck, 2013).
Moreover, we identified that interpersonal dispute was the focus area in which patients who did not improve—they reported intense disputes, especially within their nuclear family (mostly with spouses). These patients struggled to generalize skills to their environment, and a hypothesis to explain why these participants did not show improvement may be related to the context in which their disputes took place. In the renegotiation stage, therapists try to modify negative interaction patterns and increase mutual support, aiming at changing the interpersonal context of depression (Barbato & D’Avanzo, 2008). When the situation is irreversible and intolerable, dissolution may be the best alternative. For patients suffering from severe resistant depression, dissolution may be a harder option due to patients’ own symptomatology, which could be a hypothesis to explain the modest improvement in symptoms and the less favorable outcome of IPT-G among these patients.
Overall, our findings support that improving the quality of interpersonal relationships is essential for the improvement of depressive symptomatology (Cuijpers et al., 2011; Kennedy, et al., 2016; Markowitz & Weissman, 2012; Rahioui et al., 2015). Overall, IPT-G seemed to provide tools to participants to manage interpersonal disputes, but also role changes and grief and loss. Reported improvements may suggest that IPT-G potential is not limited to mild to moderately depressed patients (Levkovitz et al., 2000; MacKenzie & Grabovac, 2001; Mutamba et al., 2018; Rothberg, 2017; Stuart & Schultz, 2016; World Health Organization, 2016). However, a close evaluation of biopsychosocial profiles among patients may be in order to further clarify which patients actually benefit from this type of intervention.
Study Limitations
First, this study relies on a qualitative approach to evaluate treatment response; it does not propose to generalize findings to all patients with depression. It is necessary to underscore that these results represent the experiences of a group of patients with TRD coming from a specialized tertiary health service in Brazil. Moreover, patients were mostly elderly, married women, which may represent only a subsection of TRD patients. Additionally, our sample was relatively small, and only one intervention group was evaluated. In this sense, qualitative analysis was limited to sessions transcriptions, and we chose to conduct a deductive analysis that was not blinded regarding outcomes. While this provided a naturalistic view of the psychotherapy process, this hindered our ability to assess data saturation. In this sense, we suggest further studies to include qualitative interviews of participants, in order to provide more information on their views and perceptions of both the process and outcomes in IPT-G. Nonetheless, the results do generate hypotheses that can guide future studies on IPT-G principles and their effectiveness.
Conclusion
To our knowledge, this is the first qualitative analysis of IPT-G for TRD. Our analysis suggests that patients with TRD can benefit from IPT-G, an effect perceived both in symptomatic improvements pre- and post-intervention and qualitative accounts. These patients see depression as a chronic condition that deeply affects their lives, and IPT-G was seen as a way of promoting change and regaining control. However, we identified that patients to whom IPT-G did not achieve the same effect in terms of symptom reduction have greater difficulty in acquiring and generalizing new interpersonal skills, and often were immersed in severe family or marital interpersonal disputes. This study adds to the understanding of IPT mechanisms of change and how treatment components could be adapted to better respond to a population’s needs ad experiences (Stuart & Robertson, 2012; Stuart & Schultz, 2016).
Footnotes
Appendix A: Inclusion and Exclusion Criteria
Inclusion criteria:
Exclusion Criteria:
Appendix B: IPT-G Structure
The IPT-G structured used in this study included:
Prior to group sessions, all participants underwent an individual interview with the first author. In this moment, participants completed the Interpersonal Inventory and Interpersonal Formulation. Both instruments are based on the biopsychosocial/cultural/spiritual model. They are part of IPT’s formulation assessments and are an extended psychosocial assessment. They aim to help the therapist understand the sources of social support, nature of confiding relationships, romantic attachments, interpersonal communication style, and relationship difficulties that may be a cause or consequence of the depressive episode. In this session, participants also completed the anxiety and depression questionnaires.
After inclusion the intervention, Sessions 1 and 2 focused on the presentation of members. This moment was important to promote the construction of group cohesion and establishment of group support.
These sessions focused on role transition. To this, participants were invited to create an individual timeline. This timeline was used the present the concept of role transition. Using this timeline, participants were asked to indicate pivotal moments of role transition and relate these moments to their current depressive episode.
These sessions focused on strategies and techniques aimed at communication and problem-solving. Participants engaged in brainstorming possible solutions to interpersonal problems presented by members of the group. They were also presented with additional strategies and techniques that could help them communicate their needs, as well as engaged in group problem-solving.
This session focused on grief. ITP’s conceptualization of grief only involves the actual death of people to which participants had significant interpersonal relationships. In this session, participants engaged in reflections regarding grief, loss, and acceptance.
This session focused on closure. Participants were invited to reflect upon the group trajectory and summarizing what they had lean from IPT-G.
After completing the 10 IPT-G sessions, participants were once again invited to complete anxiety and depression symptomatology questionnaires. At this stage, participants who did not exhibit symptomatic improvement or presented additional need were also referred to other services to continue psychosocial treatment.
Appendix C: Consolidated Criteria for Reporting Qualitative Research (COREQ)
See Table C1.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001 and by FIPE – Hospital de Clínicas de Porto Alegre (HCPA) - Registration number 2018-0547.
Data Availability Statement
Research data are available with the corresponding author.