
Abstract
This study investigated the influence of economic stressors on the relationship between healthcare adherence attitudes and intentions. The data were collected through two time points, three months apart, from 442 US workers recruited through Amazon’s Mechanical Turk. Multiple regression analysis was used to test the model with perceived income inadequacy and job insecurity as moderators of the adherence attitudes-intentions relationship. The model controlled for adherence intentions at Time 1 (T1), medical illness history, and medical illness recency. The results confirmed the healthcare adherence attitudes-intentions relationship, and supported the hypothesis that economic stressors were negatively correlated with healthcare adherence attitudes and intentions. Job insecurity moderated this relationship and perceived income inadequacy was negatively associated with healthcare intentions across time. The findings highlight the importance of considering economic stress as a social determinant in interventions aimed at improving adherence. Research is needed to understand the mechanisms underlying the relationship between economic stress and healthcare adherence.
Keywords
Healthcare adherence is the degree to which an individual’s behaviors align with the therapeutic recommendations established in collaboration with their healthcare provider. Adherence to treatment is crucial to the outcomes and efficacy of patient care, as well as maximizing patients’ health and quality of life. Non-adherence has been a continual problem for healthcare delivery and harms patients and the healthcare system alike by leading to poorer outcomes and increased costs (While, 2020). Specifically, there is an estimated annual cost of $528.4 billion (in 2016 US dollars) that can be attributed to morbidity and mortality from “nonoptimized medication therapy,” which includes medication nonadherence (Watanabe et al., 2018). Nonadherence rates are as high as 50% for hypertension treatment (Burnier & Egan, 2019), 35.9% for post-stroke medication (Zhang et al., 2019), and 34% for patients prescribed anticoagulants for atrial fibrillation (Ozaki et al., 2020). According to an overview of systematic reviews by Gast and Mathes (2019), nonadherence rates are associated with several patient characteristics including age (in a non-linear relationship), belonging to an ethnic minority, socioeconomic position, and depression. Therapy-related factors, gender, and disease duration have no consistent impact on adherence. These findings suggest that a complex interplay of socioeconomic and psychological factors may impact adherence.
The theoretical framework, the Theory of Planned Behavior (TPB), provides a comprehensive understanding of how individuals’ cognitions influence health-related behaviors like healthcare adherence. The TPB posits that attitudes, subjective norms, and perceived behavioral control shape individuals’ intentions to engage in a behavior, which in turn predicts actual behavior (Ajzen, 1985).
Attitudes and intentions are positively associated with adherence behavior in conditions like hypertension (Krousel-Wood et al., 2021) and medication following renal transplantation (Rebafka, 2016). Attitudes and intentions are not only related to behavior but also to each other; a 2015 meta-analysis utilized constructs from the TPB (attitudes, subjective norms, and perceived behavioral control) to account for 33% of variance in adherence intention and 9% of variance in adherence behavior (Rich et al., 2015). A 2016 meta-analysis showed that changes in adherence attitudes, among other cognitions, led to moderate changes in intentions and behavior (Sheeran et al., 2016). Attitudes and intentions thus represent useful subjective measures of healthcare adherence and, according to the TPB, these perceptions influence health behavior decisions (Glanz et al., 2008).
Using the behavior model set forth by the TPB, this study investigates the influence of economic stress on healthcare adherence behavior. Economic stress is a key social determinant of health. “Cost-related nonadherence” is considered one of the most common barriers to adherence for diseases like diabetes, cardiovascular disease, and hypertension, but relies on objective economic metrics like cost constraints (Van Alsten & Harris, 2020). Economic stress, alternatively, is a more subjective experience of lacking sufficient resources or threats to one’s economic resources (see Sinclair et al., 2024 for comprehensive review; Probst et al., 2018). While there has been much research on the causes and effects of cost-related nonadherence, there have been relatively fewer studies examining the effect of subjective economic stressors on the relationship between adherence attitudes and intentions. This study investigates two subjective measures of economic stress: perceived income inadequacy and job insecurity as these represent the two most heavily studied economic stress constructs (Sinclair et al., 2024).
Perceived income inadequacy (PII) is the perceived inability to afford wants and needs, rather than an objective measure of actual income and expenses (Sears, 2008). PII is an important factor in assessing one’s financial situation, especially because it can reflect the psychological context of individuals irrespective of their objective income. For example, PII variability explains discrepancies between levels of objective wealth and financial satisfaction; those with the most wealth reported the lowest levels of satisfaction (Sirgy, 2018). Job insecurity reflects perceptions about the uncertain future state of one’s job—hat one might be laid off or have their position change in undesirable ways. Job insecurity can influence an individual’s approach to financial decisions and has been shown to have an association with physical and psychological health (Shoss, 2017). Individuals who anticipate an imminent reduction in generative ability (demotion, unemployment, etc.) may experience depleted attentional resources that people could otherwise devote to attending to their treatment regimens (Hobfoll, 1989). Thus, individuals’ subjective experiences of economic stress are more proximal to adherence behaviors than are the objective resources.
There has been little research examining the effect of specific, subjective economic stressors. Behavioral economics research offers an explanation for the effect of economic stressors through scarcity theory, which suggests that when individuals experience scarcity or perceive limited resources their cognitive bandwidth becomes occupied with concerns related to those resources, resulting in a narrowing of attention and a focus on immediate needs (Meuris & Leana, 2015). We propose that individuals who are economically stressed may prioritize immediate financial concerns over preventive healthcare, medication adherence, or investing in healthier lifestyle choices.
This study addresses calls from previous researchers (Seabury et al., 2014) to examine economic factors affecting nonadherence. We propose the following hypothesized relationships: H1: Adherence attitudes at Time 1 (T1) are positively related to adherence intentions at Time 2 (T2). H2: Perceived income inadequacy at T1 is negatively related to adherence intentions at T2. H3: Job insecurity at T1 is negatively related to adherence intentions at T2. H4: Perceived income inadequacy at T1 moderates the relationship between adherence attitudes at T1 and adherence intentions at T2 such that greater perceived income inadequacy will weaken the relationship. H5: Job insecurity at T1 moderates the relationship between adherence attitudes at T1 and adherence intentions at T2 such that greater job insecurity will weaken the relationship.
See Figure 1 for Hypothesized Model.
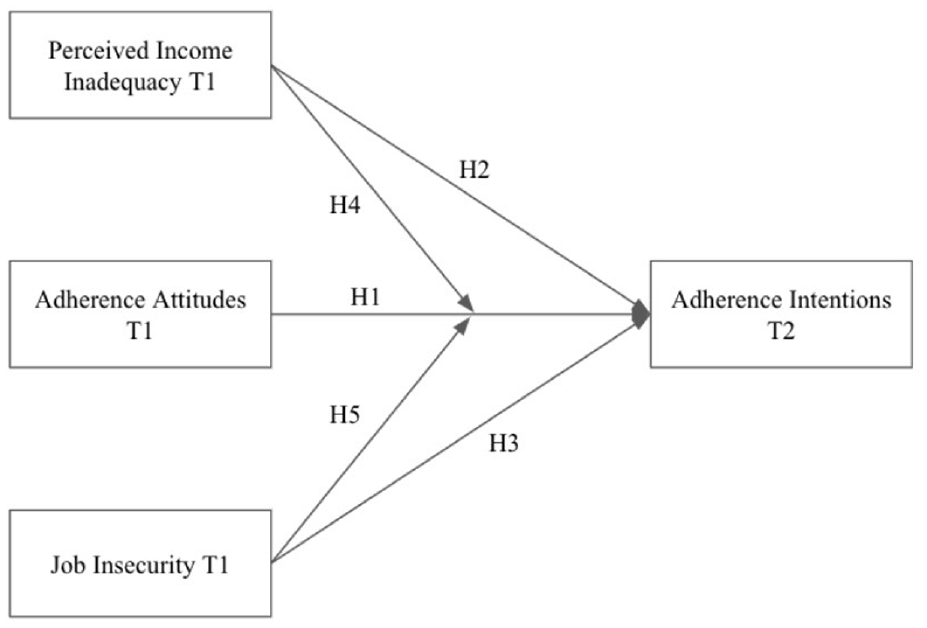
Hypothesized model.
Methods
Participants and Procedure
The present study used a prospective design that involved survey data collection at two time points through Amazon Mechanical Turk (MTurk). The surveys were administered during 2018, approximately 3 months apart and were approved by the university Internal Review Board. Collecting data at two timepoints reduced concerns about common method variance as this design allowed for temporal separation between the predictors and outcome variable. MTurk was chosen due to its diverse and representative sample of the general population (Buhrmester et al., 2015). Validity and reliability of data obtained through MTurk has been supported in prior work (Berinsky et al., 2012; Michel et al., 2018).
The survey was available to English-speaking, US-based MTurk members. To focus on job insecurity, we excluded 288 participants who were not employed outside of MTurk. Participants were compensated with $4 for completing each survey, which took approximately 30 min. Attention checks were included to assess the participants’ attentiveness and were worded as instructed response items, such as “Please respond ‘neutral’ to this question.” Participants who incorrectly responded to attention checks were excluded from the analysis.
Measures
All measures used a five-point response scale from (1) “strongly disagree” to (5) “strongly agree” unless noted otherwise.
Perceived Income Inadequacy
Perceived income inadequacy (PII) was measured with a 10-item scale based on Sears (2008). A sample item included, “I can pay my bills on time.” The Cronbach’s alpha for this measure was .91 at Time 1. All items were reverse-coded such that respondents with higher scores were considered to have higher PII.
Job Insecurity
Job insecurity was measured using a 10-item scale from Probst (2003). A sample item included, “My job will be there as long as I want it.” The Cronbach’s alpha for the job insecurity measure was .92 at Time 1. Items were reverse-coded when appropriate, and respondents with higher scores were considered to experience greater levels of job insecurity.
Adherence Attitudes
Adherence attitudes were measured with a 12-item Theory of Planned Behavior (TPB) questionnaire (Ajzen, 2013). Cronbach’s alpha for this measure was .79 at Time 1. This measure included three subscales: attitudes, subjective norms, and perceived behavioral control, which work together as direct determinants of behavior intention under the TPB (Conner & Armitage, 1998). Sample items for each subscale included, “I trust my doctor’s recommendations for my care,”“If I had a serious medical condition, my family/friends would help me follow treatment instructions,” and “When I have a medical condition I usually know what I need to do to get it treated,” respectively. Items were reverse-coded when appropriate, and respondents with higher scores were considered to have more positive attitudes toward healthcare adherence.
Adherence Intentions
Adherence intentions were measured using a 10-item scale developed from relevant literature (Martin et al., 2005). This measure assessed participants’ stated intention of engaging in health behaviors, and asked participants to rate whether they would perform each item. A sample item included, “Attend recommended follow-up appointments.” Each item was scored on a six-point scale from (1) “Definitely would not do this” to (6) “Definitely would do this.” The Cronbach’s alpha for this measure was .90 at Time 1 and .90 at Time 2. Items were reverse-coded when appropriate, and respondents with higher scores were considered to have greater intent to adhere to health-promoting behaviors.
Medical Illness Experience
We used two items to control participants’ medical illness experiences. The first item assessed medical history by asking “Have you ever had a serious medical illness or condition (i.e., one that required repeated visits to a doctor)?” The response scale was (a) “No, never,” (b) “Yes, one,” and (c) “Yes, more than one.” The second item inquired about the recency of a medical illness or condition (“How long has it been since your last serious illness/condition?”). Respondents answered on a scale with (a) “I have never had one”, (b) “Over 5 years”, (c) “1-5 years”, and (d) “I currently have one.”
Results
A total of 677 employed participants completed the first wave of the survey, passed all attention checks, and were then invited to complete the second wave. Of these participants, 442 (65% response rate) successfully completed both waves of the survey including all attention checks. Participants were primarily US-based, with an average age of 36.43 years (SD = 10.03) and a slight majority being male (55.66%). Participants identified themselves predominantly as White (79.81%), followed by Black and African American (7.36%), Hispanic/Latino (6.18%), and Asian (5.46%). The majority of participants had a bachelor’s degree or higher (50.90%). For marital status, 47.51% of participants were single and never married, 41.40% were married, and 11.09% were divorced/separated. Over half of the participants (60.18%) reported not having any financially dependent children. Of the 39.82% of participants who reported having financial dependents, the average was two financial dependents.
Nearly half of the participants (45.70%) reported having one serious medical illness or condition that required repeated visits to a doctor, and 28.73% reported having more than one. Only 25.57% of the participants reported no previous history with a serious medical illness or condition. Regarding the recency of the medical illness or condition, 19.00% of participants indicated that they were currently experiencing the illness or condition at the time of completing the survey. Another 37.10% of participants reported experiencing the illness or condition in the past 5 years, and 19.68% reported their experience was more than 5 years prior to the survey. Again, nearly 25% of participants never having a serious medical illness or condition in the past.
The means, standard deviations, and correlations among the variables were reported in Table 1. In accordance with the hypothesis, adherence attitudes at Time 1 (T1) and adherence intentions at Time 2 (T2) were positively and significantly correlated (r = .58, p < .001). Both economic stressors at T1—perceived income inadequacy and job insecurity—were negatively associated with adherence attitudes at T1 (r = −.29, p < .001; r = −.36, p < .001, respectively) and adherence intentions at T2 (r = −.30, p < .001; r = -.24, p < .001, respectively). Perceived income inadequacy was positively related to medical illness history (r = .17, p < .001) and medical illness recency (r = .16, p < .001) such that participants facing greater economic stress reported more serious medical illness experiences.
Means, Standard Deviations, and Correlations With Confidence Intervals.

Note. M and SD are used to represent mean and standard deviation, respectively.
indicates p < .05. ** indicates p < .01.
Analyses were conducted using R version 4.3.1. Hierarchical moderation analysis was used to test our hypothesized model using the lm() function. The predictor variables (i.e., adherence attitudes at T1, perceived income inadequacy, job insecurity) and control variables (i.e., adherence intentions at T1, medical illness history, medical illness recency) were centered and standardized prior to analysis per best practices (Dawson, 2013). In order to standardize the data and facilitate meaningful comparisons, we applied the scale() function from the R statistical software package. This function performs two key transformations: centering the data by subtracting the mean of each column and scaling it by dividing each value by the standard deviation of its column. This process ensures that each variable is centered around zero with a standard deviation of one, mitigating the influence of varying scales and facilitating the robustness of our analyses.
Control variables (healthcare adherence at T1, medical illness history, and medical illness recency) were entered in step one. The main effects of adherence attitudes, perceived income inadequacy, and job insecurity at T1 were added in step two. Interaction terms were included in step three for the moderation hypotheses. For significant interaction terms, the simslopes() was used to calculate simple slopes and plotted with interact_plot().The hierarchical regression results are presented in Table 2.
Hierarchical Regression Results.

Note. Standardized coefficients are reported.
p < .05. **p < .01. ***p < .001. †p < .10.
The results indicated that H1 was supported. Adherence attitudes at T1 were positively associated with adherence intentions at T2 (β = .08, p = .009) even when controlling for perceived income inadequacy, job insecurity, medical illness, and adherence intentions at T1. H2 was also supported as perceived income inadequacy at T1 was negatively related to adherence intentions at T2 (β = −.08, p = .001). Job insecurity at T1 was not significantly related to adherence intentions at T2 (β = .04, p = .160), thus H3 was not supported. H4 was not supported as the interaction term for perceived income inadequacy was not significant (β = .03, p = .191). Lastly, job insecurity was a significant moderator (β = −.06, p = .027) of the adherence attitudes at T1—adherence intentions at T2 relationship, supporting H5. Because the interaction term was significant, we conducted simple slopes analysis for job insecurity as a moderator as shown in Figure 2. At low levels of job insecurity, the slope was significant and positive (β = .13, p < .001); however, at high levels of job insecurity, the slope was not significant (β = .02, p = .640).

Moderating effects of job insecurity.
Discussion
The purpose of this study was to investigate the relationship of economic stress with healthcare adherence attitudes and intentions. Findings confirm the established relationship between adherence attitudes and intentions, consistent with previous literature (Rich et al., 2015; Sheeran et al., 2016) and our hypothesis (H1). The direct relationship between healthcare adherence attitudes and intentions (H1) was supported even when controlling for subjective economic stress (e.g., perceived income inadequacy, job insecurity) and healthcare adherence intentions at T1. H2 was also supported, as perceived income inadequacy at T1 was negatively related to adherence intentions at T2, but job insecurity at T1 was not significantly related to adherence intentions at T2 (H3). Notably, job insecurity had a moderating effect (H5) such that the relationship between healthcare adherence attitudes and intentions was significant and positive for those with low job insecurity but non-significant for those with high job insecurity.
The effect of perceived income inadequacy on adherence intentions is of particular importance. The relationship was negative, indicating that participants who experienced greater inadequacy (i.e., those who consider income to not be sufficient to meet their wants and needs) reported lower intentions to adhere to health behaviors. These findings suggest individuals’ perceptions of limited resources relative to wants and needs may restrict them from having the bandwidth (financially, emotionally, etc.) to properly adhere to health guidance. This result affirms findings from previous research (Sirgy, 2018) and the TPB model. It highlights the importance of taking into account perceptions of income inadequacy in healthcare decision making and demonstrates that studying objective income alone is insufficient for understanding how one’s economic situation affects healthcare decision making. Clinically, communication that emphasizes joint decision making and patient-centered processes might help clinicians address specific barriers patients are experiencing related to income inadequacy.
Also of note is the moderation effect of job insecurity. The moderation results suggest that the significant relationship between healthcare adherence attitudes and intentions only exists for participants with low job insecurity. In essence, this means that adherence attitudes are only positively related to intentions for those who feel that their job is secure. The inverse is also true, as participants with higher levels of job insecurity had no significant relationship between adherence attitudes and intentions. For workers with insecure jobs, their adherence attitudes did not matter and had no influence on their adherence intentions. Job insecurity is known to have detrimental effects on job performance, physical health, and mental health (Sinclair et al., 2024). Our findings suggest that the stress associated with high levels of job insecurity leads individuals to deprioritize concerns about long-term outcomes in healthcare outcomes and treatment adherence.
Also of clinical significance is that participants facing greater economic stress reported more serious medical illness experiences. The likely bidirectional relationship of these factors and the rising costs of healthcare and missed wages due to chronic illness (Chronic Disease Fact Sheet [CDC], 2022) will only worsen over time and continue to compound with an aging population. Thus, future research cannot ignore the impact of economic stability, one of the key social determinants of health amplifying morbidity and mortality rates and healthcare policy makers focus on solutions that mitigate the impact of economic instability.
Our findings suggest that economic stress has negative impacts on healthcare adherence, but further research is needed to understand these relationships fully. Results of this study offer several important implications for researchers and policymakers alike. Understanding the role of economic stress, particularly job insecurity, on the adherence attitudes-intentions relationship (H1) is important for evaluating research and interventions on healthcare adherence. As a moderator, participants’ job insecurity may affect the efficacy of interventions targeting healthcare adherence attitudes and intentions if not accounted for. For those with job insecurity, positive attitudes toward adherence may not matter if the stress of the situation impedes adherence intentions and actions. Future research should examine attitudes and intentions specifically in people with these and other economic stressors to determine how these attitudes are then incorporated into decision-making. For patients with job insecurity or other financial strain, it may be imperative to focus first on identifying and removing economic barriers to healthcare to help facilitate patient’s access to resources and ability to adhere. A stepped intervention focused on barriers at different levels, starting with resources and then moving on to knowledge and attitudes, may be more impactful.
Some limitations to this study should be considered when interpreting the results. The data were self-reported and may have been subject to response biases; however, self-report is the most appropriate method for assessing subjective constructs such as attitudes, intentions, and perceptions. Future researchers should consider utilizing objective metrics to ascertain the impact of these perceptions on actual health outcomes and should investigate the effects of additional variables like health insurance coverage, health status, substance use, and education. Furthermore, it is important to acknowledge the potential biases inherent in using MTurk as a platform for data collection. While MTurk provides access to a diverse pool of participants, including those with varied socioeconomic backgrounds and employment statuses, it is worth noting that MTurk workers may not fully represent the general population. In this study, specifically surveying MTurk workers may introduce biases related to their demographic characteristics, internet literacy, and employment status. However, utilizing MTurk workers who are also employed outside of the platform may offer a more diverse and representative sample, potentially mitigating biases associated with a solely MTurk-based sample. Future research should aim to replicate findings using more diverse samples and consider alternative recruitment strategies to enhance generalizability.
Conclusion
In summary, healthcare providers and policymakers should consider the impact of economic stress on adherence behaviors when designing interventions to improve healthcare outcomes. Further research is needed to explore the mechanisms through which economic stress impacts healthcare adherence and to identify effective interventions that can address this issue. Our results contribute to the literature on healthcare adherence by showing how economic stress may be influencing adherence attitudes and intentions and reinforce the significance of economic factors in health behavior, consistent with previous studies (Van Alsten & Harris, 2020).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received private funding through a donation to Clemson: Sinclair, R.R., & Jones, K.O. (2017) Improving patient communication for the 21st Century: Revising the Patient Needs Assessment Protocol. Private Donor. IRB 2017-247, Institution: Clemson University, Title: Improving Patient Communication for the 21st Century: Revising the Patient Needs Assessment Protocol (PNAP)
The institution number is 2017002063
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.