
Abstract
Men who have sex with men (MSM) across South Africa face significant health disparities rooted in stigmatization due to their sexual orientation, which negatively affects their health. Toward curbing sexually transmitted diseases and ensuring equitable distribution of access to health services for MSM, this study developed a framework capable of providing equal health for MSM in South Africa. The study aims to develop a framework that promote equitable health among MSM in South Africa. This study adopted a qualitative method with in-depth consented interviews targeted at MSM in Umlazi township, South Africa. A total of 25 MSM were interviewed, and their responses were analyzed using Nvivo 11, supported by content analysis. The Equitable Health Access Framework (EHAF) was developed using the study findings, guided by the WHO framework for social health determinants, and underpinned by the systems theory. The framework was structured around three factors: input, processes and output. The key finding depicted that the implementation and collaboration of the input and process will result in an output of equitable health access for MSM. Based on the study findings, the processes and key factors to be considered are sensitization training, community engagement and support, MSM empowerment program, and health promotion. At the same time, the input are finance, human resources, infrastructure, medical equipment and consumables. The “framework” could guide policymakers and health professionals by providing structured processes and key elements to ensure better health space and equal healthcare delivery to MSM in the research setting and similar settings in developing countries.
Plain language summary
The focus of this study is on South Africa, men who have sex with men who are often seen to suffer with health problems because of their sexual orientation. And in order to help them in dealing with their health issues researcher talked to 25 MSM in Umlazi and learnt about their personal stories. And it was the result of their feedback that help in developing the study framework which is called the Equitable Health Access Framework (EHAF). The framework describes mechanisms that can be used to grant MSM population platform to better access healthcare with the interventions like health education, trainings and community support. It’s expected that with this framework different policy makers, health care workers and program implementers will be able to use the mechanism to better support MSM in accessing health services withouth any fear, stigma or discimination.
Introduction
Global health disparities among sexual minorities such as men who have sex with men (MSM) exemplify major problems in achieving egalitarian access to health systems and optimal health indicators on the global scale (Richardson & Monro, 2017). These disparities are outcomes of the widespread discrimination, stigma, and social exclusion, leading to the lack of healthcare access and hence the amplification of human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), sexually transmitted illnesses, mental health issues, and drug addiction within the sexual minority groups (Beyrer et al., 2013). While South Africa’s constitution forbids any discrimination on the basis of sexual orientation, MSM regardless confront a negative social attitude and a lot of difficulties in accessing healthcare services because of structural and institutional barriers. South Africa has one of the highest HIV infection rates in the world, with MSM being a larger group (Beyrer et al., 2013). The sexual minorities experience many health problems that the healthcare system of the country sometimes fails to address in a timely manner. This suggests that precise frameworks and policies should be crafted and implemented for ensuring equal access to healthcare and dealing with health gaps among the South African MSM individual as well as their counterparts in other parts of the globe.
Health, often referred to as wealth, has been a significant concern for the governments of most developing nations (Semyonov et al., 2013). According to Sustainable Development Goals 3 and 5 (SDG), all ages and members of a nation should have equitable access to health regardless of their sexual orientation. Unfortunately, Müller et al. (2018) submitted that the sexual orientation of men who have sex with men (MSM) are often marginalized from the entire population impacting their access to health services. Tapp and Hudson (2020) reported that the segregation of this population from health access is one of the factors responsible for the high transfer of sexually transmitted diseases among MSM. A meta-analysis found that MSM in developing countries, especially in Africa, are nearly four times more likely to be infected with the human immunodeficiency virus (HIV) than the general population due to underlying factors affecting their wellbeing (Hessou et al., 2019). There is also a high rate of unprotected sexual intercourse among MSM in South Africa, which harms their total wellbeing (Stannah et al., 2019). Yuan et al. (2019) classified MSM as a high-risk population regarding HIV prevalence due to an increase in the transmission of HIV among this target population. The United Nations (UN) pronounced that MSM are 24 times more likely to get HIV than the general population (UNAIDS, 2018). The review of literature conducted in metro cities within Africa indicated a high prevalence of HIV among MSM in three cities, with the highest being Durban (48.2%), Johannesburg (26.8%) and Cape Town (22.3%; Cloete et al., 2014). Thus, it can be implied that MSM often face numerous health challenges.
The health challenges affecting MSM are attributed to the discrimination they face due to their sexual orientation, which further hinders them from accessing quality healthcare services (Müller et al., 2018). Likewise, Albert Ikhile and Mavhandu-Mudzui (2023) affirmed that the discrimination faced by MSM leads to social stigma, limiting their access to quality health amenities. This discrimination is also experienced in the form of harsh treatment or rejection at the workplace compared to their heterosexual counterparts (DeSouza et al., 2017). Aside from abusive treatment, A. M. Anderson et al. (2015) stated that MSM are confronted with constant violence and discrimination at their place of work. This violence affects their social relationships and creates a social stigma, preventing them from sharing their sexual orientation with others. Due to this discrimination and social stigma, MSM individuals often experience depression, suicidal thoughts and substance abuse (Kunzweiler et al., 2018). According to Henny et al. (2018), social stigma and discrimination toward MSM worsened during the 19th century. During this century, MSM had no right under the law, as the act of homosexuality was seen as forbidden or taboo. South Africa became the first country in Africa to accept the identity of MSM (Scheibe et al., 2017). Despite the South African government accepting the sexual orientation of MSM within the country, they are still confronted with a lack of equitable access to health (Scheibe et al., 2017).
Müller et al. (2018) attributed the poor access to health of MSM in South Africa to the concept of indigenous psychology. This psychology is concerned about what a particular environment and culture perceive as the truth and ideal behavior of human nature. This implies that indigenous psychology determines human nature’s accepted and rejected sexual relationships. Duby et al. (2018) found that, in some parts of South Africa, indigenous people still perceive the sexual relationship of MSM as perverted and a sign of mental problems. Scheibe et al. (2017) maintain that the negative perception and discrimination of MSM hinder their access to better healthcare services, despite government recognition and support. Under the Constitution of South Africa, access to better and quality healthcare is the right of all citizens, regardless of their sexual orientation (Albertyn, 2019). Despite the South African government policy ensuring equal health care for its citizens, it was discovered that some minorities (MSM) still face challenges in accessing quality health (Albertyn, 2019).
Research that focuses on MSM challenges and some recommendation on our to support this target population has grown rapid since 2020 (A. I. Ikhile, 2024). Thus, this study aims to develop a framework for ensuring equitable health for men who have sex with men in South Africa, while the World Health Organization (WHO) developed a similar framework for the social determinants of health based on an individual’s characteristics, features, or identity, containing 12 components that they believe are sufficient for determining an individual’s health condition (Kunzweiler et al., 2018). These components include early childhood development, employment and working conditions, education and literacy, physical environments, social supports, coping skills, healthy behaviors, health services, biology, genetic endowment, gender and culture. However, as evidenced by past literature, these components exclude the sexual orientation of MSM as a factor crucial for ensuring equal health distribution. The gap in the existing study further motivated this study to develop a framework for accessing equal health of MSM.
Also, majority of studies in Africa, including South Africa, such as those conducted by Huebner et al. (2012), Kunzweiler et al. (2018) and Jobson et al. (2018) have focused on the HIV risk among MSM, abuse of MSM and factors that shape heterosexual fathers’ relationship with their gay sons. It was discovered that there is still a gap in studies concerning challenges confronting MSM individuals. A. M. Anderson et al. (2015) and Gyamerah et al. (2020) evaluated the stigma facing MSM and their physical and mental health challenges. Unfortunately, it was discovered that there are still more gaps in the literature regarding the establishment of a framework for health equality for MSM. Thus, this study aimed to develop a framework for health equality for MSM.
Method
Study Site
The study was conducted in Umlazi, a township in KwaZulu-Natal, South Africa. This township is located in the southwest of Durban in the eThekwini district and is one of the largest townships in South Africa. The researcher’s rationale for choosing this study site is based on the township’s population size, estimated at ≥500,000. As per the South African national HIV prevalence, incidence and behavior survey, the KwaZulu-Natal province has the highest HIV prevalence in South Africa—with 27.6% of men and women aged between 15 and 49-years being HIV positive (Human Sciences Research Council [HSRC], 2017).
Study Design
The researcher conducted this study and adopted the qualitative research approach. A qualitative research method was selected for this research to explore the views and perceptions of MSM in Umlazi in detail since it gives the possibility of getting in-depth knowledge about the social dynamics, lived experiences and the multifaceted nature of challenges and obstacles which the MSM community faces. While quantitative methods provide insight into data, the qualitative research method can bring in more depth and rich context to the topic at hand (Tracy, 2019).
Guided by Rashid et al. (2019) and Mayan (2016), the researcher collected data in a narrative format through one-on-one in-depth interviews (Rashid et al., 2019). The narrative structure is developed from interviewing the study participants and creating a detailed note of the response and behavior of the study participants in their natural habitat. Mayan (2016) proclaimed that the naturalistic paradigm controls qualitative research because it stipulates that the individual, not the researcher, constructs reality. Under the qualitative research approach, the validity of the matter being investigated is not a fixed entity; rather, it depends on the research participants’ beliefs (Turner et al., 2017).
Study Instrument
An in-depth interview was used as the data collection tool facilitated by the researcher. A structured open-ended question was designed on the idea that fits into the literature review and meets the study’s set objective. As guided by Eppich et al. (2019) the researcher pre-tested the interview questions with study partners before embarking on and validating the chosen question meeting the study objectives. At the beginning of each interview, the researcher allows the participants to read through the consent form and sign it before embarking on the interview. Also, the participant was required to fill out a demographic data form before the start of the interview. Each interview took one and a half hours to 2 hours, though some participants exceeded 2 hours due to their long, shared experiences. The questionnaire covers participants’ community experiences regarding their health and social economic within their society.
Sampling and Target Population
This study adopted a non-probability sampling method involving selecting samples based on the researcher’s subjective judgment instead of random selection. Tuli (2010) affirmed that non-probability sampling is widely used for qualitative studies. Therefore, this study adopted the snowball non-probability sampling technique in order to effectively reach MSM through already existing network and trusted connections within the community (Parker et al., 2019).
The study’s target population are MSMs over the age of 18 residing in Umlazi. The respondents were selected because they are capable of providing a answers to the research problem questions. The researcher collaborated with Anova Health Institute in Durban, a non-governmental organization that services the health needs of MSM in Umlazi township. Anova Health Institute already has a good network of MSM in Umlazi. Due to this benefit, it was easier for the researcher to select MSM who participated in this research.
Different sampling selection criteria were used to determine a better fit to participate in the study. The sampling selection criteria are listed below:
Participants must identify as MSM and voluntarily show interest in participating in the study.
Participants must not be under 18 years of age at the time of the study.
Participants must be residents of Umlazi at the time of the study and be willing to participate.
By adopting these criteria, 30 MSM were pre-selected and registered through the health organization to participate in the face-to-face interviews. Still, only 25 were finally interviewed, as the others did not attend the interviews as planned due to COVID-19-related issues.
Participants’ Informed Consent
This study used a qualitative methodology based on the research questions and aims (Eppich et al., 2019). The data collection phases relied on volunteer participants, and those who took part in the qualitative study gave their informed consent by signing an informed consent after the researcher duly explained the content of the informed consent form giving the participants a complete understanding of the study processes and options to take part voluntarily. All participants fully understood and signed the shared consent forms to participate voluntarily in this study.
However, the information from the interview was recorded, and confidentiality was maintained by using pseudonyms as necessary. Additionally, the qualitative data-maintained confidentiality by omitting names and making them optional. Additionally, the collected data were handled with optimum strictness to prevent loss of confidentiality and will be deleted after being used for this study.
Theoretical Framework
The theoretical methodology of this study builds into the World Health Organization’s framework for Social Determinant of health determinant grounded in System Theory. The Social Determinant of Health Framework of the World Health Organization (WHO) clearly demonstrates how individuals’ health outcomes are influenced by social, economic, and environmental factors and thus underpins the role of addressing social inequalities to achieve health equity (WHO, 2012).
The objective is to investigate how social, cultural, and systemic factors related to MSM in South Africa and the rest of the African countries influence the level of healthcare access and the health outcomes using theoretical frameworks. The developed EHAF starts from the conclusions of all these trends, suggesting a structured approach as the way to overcome the multifaceted barriers and disparities that the MSM face in accessing healthcare services. The framework believes in instruments like sensitization training, community mobilization and support, vulnerable population empowerment, and health promotion to foster consensus between policy makers, healthcare providers, and MSM communities to tailor their healthcare delivery systems to the specific needs of this population. Taking into account the type of finance, human resources, infrastructure, and medical equipment the EHFA intends to promote the availability and development of policies that guarantees access to health care services for men that have sex with men. Subsequently, the proposed framework which envisions ensuring a favorable healthcare environment to MSM in South Africa and other African countries by way of respecting their rights, addressing their health needs, and finally is built on promotion of their general health and wellness.
Ethical Clearance and Confidentiality
The Research Ethics Committee from the University of South Africa under the Department of Health Studies granted the study’s ethical clearance with an ethical approval letter (REC-012714-039) after the submission of approval signed letter from Anova Health Institute as the key collaborator in the research study. As part of the research protocols, the researcher thoroughly explained the study’s aim, nature and potential benefit to the participants, giving them a choice to participate voluntarily in the study. In ensuring the confidentiality of the participants, the researcher used pseudonyms to represent the participants’ names. The ethical challenges related to the researching of MSM in South Africa was tackled through informing the participants about the study and receiving their consent for participation, maintaining anonymity and confidentiality in the data collection and reporting process, training researchers on cultural sensitivity and establishing trust and rapport with the MSM community to address the stigma and discrimination concerns (Pietilä et al., 2020).
Research Limitation
Limited generalizability of findings is one of the key research limitations identified in establishing an equitable health access framework for MSM in South Africa. This can be traced to the conduction of research in a location that does not capture or represent experiences of other MSM across other regions. The researcher also noted that some key factors like stigma-related concerns, social desirability bias and non-sampling techniques might affect respondents’ willingness and freedom to disclose sensitive information. It is then recommended for future research studies that diverse sampling be used that will cover larger and diverse locations.
Result and Discussion
This section presents the result and discussion of findings from the responses acquired from the participants (MSM). It commenced with a demographic description of the participants interviewed in the study. The results are presented based on the theme that was developed during the research data analysis, supported by participants’ verbatim statements to substantiate the findings. The findings are discussed as per the reviewed literature.
Demographic Data
The demographic data of the MSM that were examined in this study include participant age, educational level and sexual orientation.
Age
There are 25 participants in this study, and as per the study selection criteria, all selected participants are ≥18 years old. The median age is 27 years old, the youngest participant is 21 years old, and the oldest is 55 years old. The most represented participants are those ≥36 years old (but only nine out of the 25 are ≥36 years). The age group selected in this research is aligned with other published past research focusing on MSM (Wilson et al., 2020). Data obtained on age group variance provides an insight into the diversified MSM population with respect to the repercussions of health access and outcomes. The age distribution can assist to generate the health interventions and the health services that are specific to the addressed the health risks and the needs of different age groups among the MSM whose goal is to achieve better health equity and outcomes across the MSM aged.
Educational Level
The level of educational attainment is one of the biodata items collected from the study participants. Past research showed low educational attainment in 2018. A total of 59% of South African citizens aged 25–64 attained an upper secondary certificate as their highest qualification (OECD, 2016). As per this research, the researcher considered the different educational attainments of each participant in this study. The researcher’s reason for collecting the educational attainment data is to compare and contrast the education level to other study variables and then analyze their impacts on MSM health. In this study, all the study participants attained some level of education. The most educated had obtained a master’s degree (8%), while 28% of the participants achieved a bachelor’s degree. A total of 20% of the participants attained a diploma, while 44% of the study participants, the most represented, matriculated from high schools. This finding shows more educated participants, contrary to the cited study above.
The implication of these findings illustrates that among MSM there is a multi-faceted educational attainment framework, and this may have implications on how health access, healthcare utilization and health outcomes are affected within communities of MSM. Learning these dynamics, among other things, should assist in the development of specific interventions and policies addressing health disparities as well as in promoting equitable healthcare access across the various level of education enjoyed by MSM.
Sexual Orientation
Sexual identity is the personality an individual identifies with without shame or regret (Lady & Burnham, 2019). In this study, MSM participants identify themselves into four categorized sexual identities as defined below:
In the provision of inclusive and culturally competent health care services for MSM, it is crucial to know the respective sexual identity of MSM individuals. This would help to address MSM individual needs based on their unique identity as their habit and behavioral patterns differs (Tasker & Wren, 2002). Each sexual identity has unique experiences and challenges they faced, and these attributes cannot be taken for granted if we need to create a better access to health services for each group that will in turn achieve a better health for all.
Framework Development
The framework for health equality was developed based on the health inequalities confronting MSM to improve their social health determinants. The framework was structured around three factors: input, processes and output. The information used in developing the framework was guided by the themes emanating from the interview findings, and the output was synthesized from the literature and subthemes of the interview.
Table 1 presents the themes and the subthemes that were extracted from the interview.
Theme Table.

Table 1 summarizes the themes extracted from the MSM interview within the study area. The interview was centered on the major factors that hinder or challenge MSM from accessing adequate health care. The major challenge was labeled as the superordinate column, as shown in Table 1. In contrast, the column labeled as theme and subtheme contains the specific challenges (superordinate theme) that hinder access to equal health. The themes were merged using the WHO Commission on Social Determinants of Health framework and the WHO Sustainable Development Goals as a global guide. On the national level, this study used the South African National Strategic Plan on HIV, STIs and TB (2017–2022).
Input
During the interview processes, the feedback from the respondents showed key challenges and conditions they faced in the community support in determining the inputs. These inputs are categorized as gaps in socioeconomic factors determining the health of MSM in their communities. Figure 1 below shows the inputs needed to develop the social health determinants model among MSM individuals, and each input is explained in detail below.
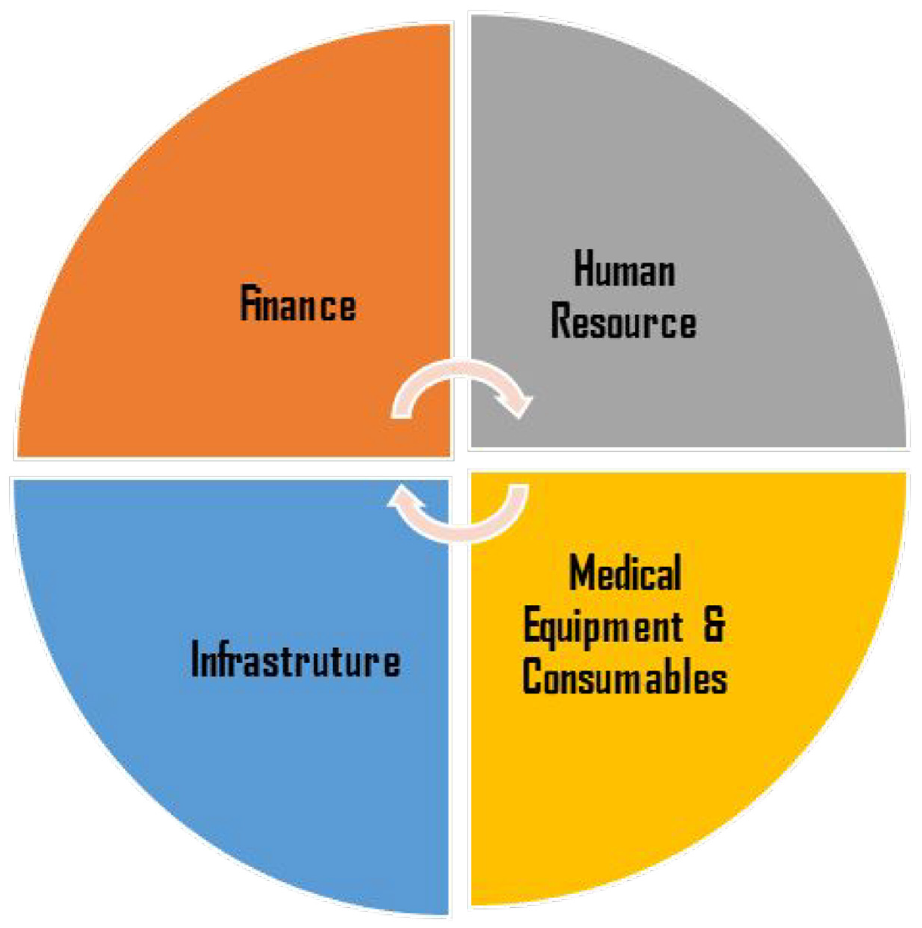
The inputs required for the MSM social determinant of health model. (I. A. Ikhile & Mavhandu-Mudzusi, 2024).
Finance
The study findings show that health for MSM could not be enhanced without proper financial resources. A valuable financial resource would guarantee better health for MSM without any sense of inequalities, as shown in Figure 1. To ensure equitable distribution of health for MSM, the recommended model in this study calls for creating a form of financial resources capable of providing a sustainable, inclusive society for MSM with better access to quality health services. The eThekwini Metropolitan Municipality has been allocated a budget as part of its mandate to meet the National Strategic Plan for HIV, STIs and TB from 2017 to 2021 (Municipality,e, 2020). As part of the district health plan, the lesbian, gay, bisexual, trans and gender-diverse intersex, queer/ questioning (LGBTIQ) organizations in the district with the mandate of creating an inclusive environment for MSM should be financially supported. This funding will help support different programs that focus on the wellbeing of MSM in the district, such as health promotion, health workers’ sensitization training and empowerment, HIV counseling and testing, community awareness, and engagements, as per some of the feedback gotten from the participants: “We have gone through much abuse from our community, and we need the government to support us with safe space facilities like Men’s wellness centers with a focus on MSM health care services.” Msizi (32 years—Gay) “LGBTIQ non-governmental organizations in our community support us so well, but due to lack of funding from the Government, they can’t implement programs that will benefit MSM. The Government need to provide them with stable funding.” Linda (24 years—Gay)
Adequate allocated funding will support MSM-targeted programs to create an enabling environment for MSM in the districts and grant better access to health services. Another critical input is human resources.
Human Resources in Community Health Facilities
One of the key findings that emerge from the study is the shortage of human resources that support MSM health structures in the community. Healthcare workers are critical to the issues of MSM social determinants of health as they play an essential role in contributing to MSM health by providing quality services. Maphumulo and Bhengu (2019, p. 3) affirmed the shortage of healthcare workers in South Africa as a challenge to quality improvement in the health sector.
“I used private paid Doctors whenever I needed to consult for any health issues because I had lost hope in the local Clinic due to their poor services and unprofessional attitude. When you visit the local Clinic, you will find the staff roaming all about, and people will be in a long queue not being attended to on time. There is a lack of professionalism in the clinic staff, and they don’t even keep confidentiality.” Funani (42 years—Bisexual) “Our local Clinic only has 3 Nurses without doctors that service thousands of people. They are always overworked and place their frustrated anger on their clients. The government must employ more Nurses and Doctors in the local Clinics.” Nkosiyabo (28 years—Gay) “The second hindrance to using public health services is the long queues and lack of medical equipment. After being in the queue for hours, you would be referred to another clinic or hospital because they don’t have the equipment to render the services. Sometimes the Nurses will tell you that they cannot attend to your situation, but you have to see a Doctor for the situation. We lack untrained clinicians in our clinics that can attend to MSM issues, so in that regard, why should I waste my time going to a place where I won’t get the help that I need.” Gatsha (24 years—Homosexual)
During the interview process, the respondents listed the following adverse effects of the shortage of healthcare workers:
Long queues—Clinic wait times always limit MSM in accessing good health care. Long lines may dissuade sexual orientation-related healthcare patients. Healthcare environments may stigmatize, discriminate and judge MSM patients, raising privacy and confidentiality problems. Long wait periods may increase these fears, deterring people from getting treatment. Creating open, welcoming healthcare facilities that promote anonymity, shorten wait times and provide MSM-specific treatments should solve this problem.
Poor quality care services—Clinics with low-quality treatment might limit MSM health services. These people may need sexual health exams and HIV-prevention programs. However, if clinics lack MSM-related training, understanding, or sensitivity, treatment may be inadequate. MSM may feel suspicion, discomfort and unwillingness to seek treatment. Healthcare practitioners need comprehensive MSM health, cultural competence and LGBTQ+ inclusion training to increase access. Trust and fair access to high-quality healthcare for MSM persons depend on clinics providing safe environments free from prejudice and judgment.
Decreased efficiency and effectiveness of healthcare workers—Clinic staff efficiency and efficacy may limit MSM access to health treatments. Healthcare practitioners may not be able to give appropriate treatment or services if they lack MSM-specific expertise, training, or understanding. Misdiagnosis, insufficient treatment and lack of referrals to professional services might ensue. Healthcare staff that are biased toward MSM patients might create a hostile atmosphere that deters them from getting therapy. To solve this problem, healthcare practitioner education, cultural competence training and a supportive, diverse work environment are needed. Improved healthcare staff education and skills may improve efficiency and effectiveness, enhancing MSM access to health treatments.
On the other hand, the clinical healthcare workers themselves experience so much dissatisfaction, lack of motivation and burnout that it affects the services they render, resulting in the abovementioned points. In light of this shortage, no dedicated clinicians attend to the specific health needs of MSM. All these factors prevent MSM from accessing quality health services. The district municipality’s recruitment and allocation of more healthcare workers, such as doctors, nurses, psychologists, health promoters, peer educators and counselors, to the local clinics are crucial in alleviating the human resource shortages.
Infrastructure
Infrastructure in this study refers to the basic construction and maintenance structures required for an inclusive environment for MSM that translate into improving their health.
“Why will I use a Clinic where I am not welcome as a gay man? I need a place where I will be respected for who I am. We need a safe space to accommodate us and serve our health needs. We have problems and always need someone to talk to, so a mental health facility with recreation equipment won’t be a bad idea.” Solomon (32 years—Gay)
Examples of infrastructure are MSM-friendly health centers, mental health facilities, and men’s empowerment centers. Such infrastructure is essential input required to contribute to MSM’s safe and inclusive society. MSM need safe spaces that provide privacy and confidentiality to receive quality and focused health services. Through the model, the researcher recommends constructing MSM facilities or embedded facilities within the current local health facilities across the district to promote quality care for MSM. This would create better access to quality health services and inclusive society that improves MSM health in the district.
Medical Equipment and Consumables
Medical equipment and consumables in this study refer to equipment used in the consulting rooms to address MSM’s health needs (patient monitor, anal, pelvic muscle probes, anoscopy, proctoscopy, anesthesia machines, surgical tables, stretcher bed and defibrillators). Consumables such as surgical gloves, condoms, lubes, dental dams, PrEP and PEP are essential. All these material goods are needed to improve MSM’s health. One of the critical challenges faced by MSM is the lack of medical equipment and consumables in health facilities.
“Accessing health services has never been a problem for me, but the lack of basic equipment in our Clinics makes me very angry. I went to the Clinic and was told that the blood pressure machine was faulty so they couldn’t attend to me. How on earth can a Clinic have only one blood pressure machine? What is our Government doing and not equipping our Clinic with basic equipment.” Phila (20 years—Gay) “I was told about PrEP by a friend, and I went to my Local Clinic with joy to enquire about it. I was surprised that the Nurse I spoke to does not even have any idea about PrEP and asked if I was raped or had a condom burst for her to prescribe PEP. We need PrEP, Condoms, and Lubes in our local Clinics.” Mpilo (19 years—Gay)
The researcher recommends the support of the eThekwini Metropolitan Municipality to provide these commodity goods and basic equipment in all local clinics across the district. These will improve access and quality health services for MSM in the district.
The Process Used in Developing the Framework
Marmot et al. (2012) submitted that the process involves the activities and steps undertaken to achieve an output. Therefore, this section’s focus is on activities that guarantee the transformation of the input of the social health determinants model to generate the needed output. The process includes sensitization training, community role players engagement and support, MSM empowerment programs, policies integration and inclusion, and health promotion. Figure 2 (I. A. Ikhile & Mavhandu-Mudzusi, 2024) depicts the different processes identified in this study that contribute to supporting MSM in realizing good health.

Process of the model (I. A. Ikhile & Mavhandu-Mudzusi, 2024).
Sensitization Training
Sensitization training roll-out for health care workers, government departments and community leaders on issues regarding MSM health and psychosocial wellbeing is essential in creating better access to health services for MSM. MSM’s key challenge is accessing quality health services, as most healthcare workers lack knowledge and understanding of MSM health needs and psychology. The sensitization training would capacitate healthcare workers to address MSM clinical and psychosocial health aspects. These will assist in creating better access to quality health services.
“Our Nurses need to be sensitized as unprofessionalism, and lack of confidentiality is high on the list because of the attitude of health care workers. I can give an experience of a friend that went to a local clinic when he realized he had an anal ulcer as he did not have the fund to consult with a private Doctor. When he got to the Clinic, the nurse attending to him called another Nurse, and the other Nurse also called another, and they were busy making fun of him after he told them how he got the infection. That attitude is very unprofessional, and client confidentiality should always be respected. Most of those Nurses supposed never to be a Nurse because they are not compassionate but rather insulting and unprofessional. Those experiences push people away from using public facilities. Rather, they will live with their sickness at home rather than to pass through such insult.” Bhekizizwe (20 years—Gay) “The traditional leaders like the king of Zulu land and some of the political leaderships that made abusive comments against MSM all lack wisdom and are ignorant. I feel they all need to be sensitized and given lessons that being gay is never a choice.” Bonginkosi (45 years—Bisexual)
Kapanda et al. (2019, p. 6) affirm in their study that sensitization training improves the attitude of healthcare workers toward MSM, thereby creating better access to quality health services free from stigma and discrimination. In creating an inclusive society for MSM, it is required to extend the sensitization training to key government departments such as the South Africa Police Service, Department of Home Affairs, Department of Health, Department of Correctional Services, Department of Education and Department of Justice. Sensitizing all the key staff in these departments would empower the staff on MSM-related issues, reduce stigma and discrimination and create an inclusive society for MSM.
Engagement and Support of Community Role Players
MSM lack community role players that support and advocate for the needs of MSM in the community. These role players are well-respected community institutions that will help and enlighten the community about issues relating to MSM, creating an inclusive society for all. As identified by the study participants, the role players are their family members, religious and traditional leaders, media houses and government parastatals. The involvement and support of all the mentioned structures will create an enabling environment for MSM, decreasing one key challenge MSM face in the community: stigma and discrimination that translate to violence and abuse directed at their sexual orientation.
“A member of the community physically molested me, and for months I felt ashamed to speak out until a support group in my community supported me. We need all the support required from the community to stop abuse directed at our sexual orientation.” Bhekizizwe (20 years—Gay)
The finding implication shows the importance of the community role players as a crucial community driven initiative in achievement of better health for MSM individuals in the community. The community role players will foster love and trust, reduce stigma and discrimination and advocate for MSM health rights without any prejudice. Through all these mentioned support healthcare policies and actions can be changed to better meet the unique needs of these groups, leading to better health results and equality (A. I. Ikhile, 2024).
Health Promotion
Health promotion is a critical initiative that has existed for years and is stated in the WHO Ottawa Charter for Health Promotion (Thompson et al., 2018:4). The aim is to enable people to increase control over and improve their health. MSM need to increase their effort in taking good care of themselves and their health, as they are solely responsible for themselves. This can be done by a balanced behavioral change directed to healthy sexual behavior without any risk factors. The community role players that include parastatals like the eThekwini Municipality also significantly promote MSM health in their communities.
“The support group started by Anova Health Institute in my Community has been my anchor. They taught me great lessons that boosted my self-confidence and the Process of taking good care of my health. They organized good training that promoted healthy living among MSM.” Bhekumbuso (38 years—Homosexual)
The allocation of funds to district LGBTI organizations will promote MSM health through different platforms such as outreach, workshops, seminars and IEC materials distribution. All these recommended initiatives will support and improve MSM’s health status.
MSM Empowerment Programming
Apart from the different interventional programs that focus on MSM health needs, it is also crucial to have empowerment programs directed at MSM. Such empowerment programs will focus on sexual behavioral change that promotes HIV prevention and protection messages. Moreover, they will reduce HIV infection among MSM and encourage the use of condoms with lubes and treatment as prevention (TasP), such as pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP). All these will improve sexual behavior among MSM, which translates to good health. Pérez et al. (2018, p. 5) affirmed in their study the need for empowerment programs that focus on HIV prevention among MSM.
“Due to our sexual orientation, employers sometimes discriminate against us and do not offer us jobs. We will need to be self-employed if we can get empowered by the Government or NGOs in the community. We need soft skills training to help us start our businesses.” Thabo (21 years—Gay)
Another recommended key empowerment area for MSM is a skills program that focuses on career growth, encouraging soft skills such as self-motivation, leadership, responsibility, problem-solving, time management, negotiation and conflict resolution. Acquiring such soft skills will support MSM in their careers and create an avenue to access better jobs. Unemployment is high among MSM, as discovered by the study participants; therefore, encouraging and empowering MSM to be entrepreneurs by starting their businesses is needed. This will help satisfy their financial needs and promote better mental health, diminishing stress and depression caused by lack of money.
Policies, Integration and Inclusion
One of the critical challenges identified in this study is stigma and discrimination against MSM sexual orientation in their communities. The community is significant for improving MSM’s health status because most MSM are marginalized from the wider society, which prevents their access to adequate health. The marginalization originates from the decriminalization of MSM sexual activities in the townships. This study discovered that MSM are sometimes excluded from community leadership roles and rites because of their sexual preference.
“Cultural beliefs and rites have always stood as a challenge to gay men, last year, my father passed away, and as a first male child, I was expected to perform certain rituals. But because I am gay, I was refused the right to do that because they said I am not a man and I don’t have the right to perform the rituals. The said culture did not welcome me; instead, they chose my younger brother to perform the rites, which is very wrong as they discriminated against my sexuality. It was painful because I was depressed for months due to that incident; I consulted a psychologist to return to myself.” Thabo (21 years—Gay)
The lack of political role models further increases the marginalization confronting MSM in their community. It was also discovered that MSM often feel neglected within their community. McKay (2016, p. 5) stressed the need to include them in global policies about their health as they are mostly marginalized. The feeling of neglect often leads to mental health problems that cause stress and depression among MSM. The researcher recommends the intervention of all key players, such as community role players and community-based organizations like LGBTI organizations, in developing and integrating policies that will protect the rights of MSM and uphold an inclusive society for all.
Output
This study describes output as the expected benefit or output achieved from combining the necessary input. Thus, the social health determinants model’s output could be described as adopting the model input with the established process. Ravitz et al. (2019, p. 8) described output as the tangible products that a system provides. This model’s output is anticipated to enhance MSM health by improving access to quality health services in Durban in the KwaZulu-Natal province. It is predicted that if finance, human resources, infrastructure, medical equipment and consumables are effectively combined with the input as indicated by the proposed model in conjunction with the stipulated process, this will result in the output, improving MSM’s health. The process includes sensitization training, community role players engagement and support, MSM empowerment programs, policies integration and inclusion, and health promotion. The expected output from implementing these processes would significantly improve MSM’s overarching health in Durban. Figure 3 (I. A. Ikhile & Mavhandu-Mudzusi, 2024) provides a visual illustration of the recommended framework for ensuring equitable health for MSM within the South African context and being influenced by the global context. The figure illustrates the different aspects of the model and how they are expected to work, including the model structure’s relationship.

Framework for ensuring equitable health for MSM (I. A. Ikhile & Mavhandu-Mudzusi, 2024).
Framework Summary
The EHAF model is a holistic approach framework which is designed to solve the specific needs and challenges experienced by MSM in South Africa in regards better access to health services. The framework is structured around three main components: Input and process which specifies difference actions to take in reaching the third main component which is the output, improve better access to health services and enhancing overall health of MSM.
The framework assumes that if all the input, namely finance, human resources, infrastructure and medical equipment and consumables, are combined with the process, MSM health will improve. The framework comprises an input, which entails finance, human resources, infrastructure, medical equipment and consumables. The process consists of sensitization training, community role players engagement and support, MSM empowerment programs, policies integration and inclusion, and health promotion. The anticipated framework output is to enhance MSM health and improve access to health services in African countries. Figure 3 shows the relationship between the elements of the models using interconnected arrows. The model recommends that all the inputs be made available for the adequate performance of MSM social health determinants within South Africa. The processes should also be used as a transformation tool for the inputs to provide the anticipated output.
Conclusion and Recommendations
Access to quality health should not be a privilege to a certain few, as everyone is equal before the law. Therefore, no matter their sexuality, every person should be given equal access to health. Unfortunately, this is not the case with MSM in most developing countries, regardless of government support. Despite the support of the South African government for MSM, it was discovered that they are still segregated from access to quality health. Toward ensuring equal health for MSM in Africa, focusing on South Africa, this study develops a framework that guarantees equal access to health for MSM. The framework was underpinned by the WHO Social Health Determinants Framework, supporting the equitable distribution of health to minorities in a community and backed up by systems theory. System theory is a transdisciplinary framework that examines the interconnectedness, interactions, and behavior of complex systems (Popa et al., 2015). According to systems theory, a model contains independent and interconnected elements, therefore the model was developed using the following interlinked elements: input, process and output (Popa et al., 2015). It was discovered that equal access to health would be achieved in the presence of the following variables: finance, human resource, infrastructure, medical equipment and consumables.
The variables would also be supported by specific processes and institutions, such as sensitization training, community role players’ engagement and support, MSM empowerment programs, policies integration and inclusion, and health promotion. It was discovered that the absence of effective processes and institutions is responsible for the violence confronting MSM, which includes verbal abuse, emotional abuse and physical abuse. This study revealed that MSM within the study area suffer mostly from physical abuse among all forms of abuse. The violence suffered by MSM affects their health (physical and mental). This study proposed that the government of South Africa should provide legal support focused on protecting their civic rights. Aside from the violence confronting MSM due to weak legal resources, it was established that MSM are faced with poor financial support. Poor financial support is responsible for risky sexual behavior among young men. MSM’s financial constraints are attributed to the social exclusion of MSM in their communities, which further leads to poor quality of life. This study calls for the financial empowerment of MSM, especially those within the townships. It is anticipated that the financial empowerment of MSM will reduce their risky sexual behavior and contribute immensely to their health.
The study recommends that all health facility clinicians receive further psychological and medical training to improve their knowledge in addressing the health issues of MSM. The sensitization training’s roll-out will empower health workers to provide quality health services to MSM without homophobic attitudes. It also recommends that LGBTI organizations in Durban be supported financially in fulfilling their aim of creating an enabling environment for MSM. As such organizations implement focused programs that strengthen an inclusive and enabling environment for MSM, it is highly recommended that the government fund these programs to support MSM against stigma, discrimination and any homophobic factors that might affect their health. This EHAF will serve as a comprehensive guide for policymakers in the implementation and development of quality healthcare policies and practices that address MSM needs in the provision of equitable health services access.
The study contributes to literature and practice as it developed a framework for improving MSM’s health. Aside from contributing to existing knowledge, this study provides policymakers and healthcare professionals with data to ensure a better health space and equal healthcare delivery to MSM. The model developed in this study contributes to creating a standard procedure for monitoring and evaluating the challenges confronting MSM in their communities. The research findings will also motivate other researchers to adopt a qualitative approach to their work. The input, process and institutions that form the backbone of the model developed for this study can be adapted as a standard of best practice in addressing MSM health issues. This study contributed to the existing body of knowledge as it provided the inputs, processes and institutions capable of ensuring equal health of MSM.
Footnotes
Acknowledgements
I am very grateful to those who helped complete this study. First, I want to thank the University of South Africa for its invaluable resources and consistent support for our work. I am grateful to the Men who have sex with men (MSM) in Umlazi township, South Africa, for sharing their significant thoughts, which built the Equitable Health Access Framework. I also appreciate my university mentors Prof Mavhandu-Mudzusi for her guidance and mentorship, colleagues, family, and friends for their constant support. Lastly, I thank the academic and healthcare community for their commitment to reducing health inequalities in disadvantaged communities and promoting equitable healthcare access.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This research study’s ethical approval was granted by the Department of Health Studies ethical committee at the University of South Africa with the approval number REC-012714-039 (NHERC) following ethical guidelines throughout. All studies involving humans, especially MSM in Umlazi township, South Africa, followed the University of South Africa’s Institutional Review Board’s norms and procedures. All participants gave informed permission, assuring they knew the study’s goal, their rights, and their replies’ confidentiality. No research outcomes revealed participant identities. The research also sought to minimize participant injury and maximize their benefits.
Data Availability Statement
The data collected and processed for this research project are secret and include sensitive information on MSM in Umlazi township, South Africa. These data will not be released to safeguard participant privacy and comply with ethical norms and consent agreements. Researchers and institutions interested in accessing or collaborating on data analysis should contact the principal investigator, who will review such requests on a case-by-case basis, taking ethical and data protection into account. The main goal is to advance research and knowledge while protecting study participants’ privacy.