
Abstract
Research shows that both cannabis use and emotional problems (anxiety and depression) tend to peak in emerging adulthood. There is a relative paucity of research examining the temporal associations between cannabis use and emotional problems among emerging adults. Accordingly, this multi-wave longitudinal study examined three competing models of temporal precedence: the vulnerability model (negative emotions precede cannabis use); the scar model (cannabis use precedes negative emotions), and the reciprocal model (bidirectional associations between cannabis use and negative emotions). A sample of 299 North American emerging adults (Mage = 23.69 years, 58% female) completed three waves of survey measures and cross-lagged panel models were run to evaluate how anxiety and depression were related to both cannabis use and related problems across the 1-month study period. Regarding anxiety symptoms, some support was found for the vulnerability model, in that anxiety preceded cannabis problems across some waves. No directional or reciprocal associations between anxiety and cannabis use were found. As for depression symptoms, there was support for reciprocal links between cannabis problems and depression across waves. However, consistent with the anxiety-related findings, no directional or reciprocal associations between depression and cannabis use were found. The scientific and practical implications of these findings are discussed.
Plain language summary
Research shows that both cannabis use and emotional problems (anxiety and depression) tend to peak in emerging adulthood. There is a relative paucity of research examining the temporal associations between cannabis use and emotional problems among emerging adults. Accordingly, this multi-wave longitudinal study examined three competing models of temporal precedence: the vulnerability model (negative emotions precede cannabis use); the scar model (cannabis use precedes negative emotions), and the reciprocal model (bidirectional associations between cannabis use and negative emotions). A sample of 299 North American emerging adults (Mage = 23.69 years, 58% female) completed three waves of survey measures and cross-lagged panel models were run to evaluate how anxiety and depression were related to both cannabis use and related problems across the 1-month study period. Regarding anxiety symptoms, some support was found for the vulnerability model, in that anxiety preceded cannabis problems across some waves. No directional or reciprocal associations between anxiety and cannabis use were found. As for depression symptoms, there was support for reciprocal links between cannabis problems and depression across waves. However, consistent with the anxiety-related findings, no directional or reciprocal associations between depression and cannabis use were found. The scientific and practical implications of these findings are discussed.
Emerging adulthood (ages 18–25) is a unique developmental period characterized by identity formation, rapid transition and stress, and increases in risky behaviors. National data from the US indicates that emerging adults have the highest rates of cannabis use across the lifespan (Center for Behavioral Health Statistics and Quality, 2018). Similarly, Canadian youth and emerging adults report high rates of cannabis use, with 20.6% of youth aged 15 to 19 and 29.7% of emerging adults aged 20 to 24 reporting cannabis use in the past year (Health Canada, 2018). The Canadian survey also revealed that 32.6% of youth age 15 to 19 and 27.4% of emerging adults age 20 to 24 who had used cannabis within the last 3 months reported daily or almost daily use (Health Canada, 2018). Research has shown that early and regular cannabis use during emerging adulthood is associated with a host of negative outcomes, including but not limited to poor educational outcomes, low income, increased welfare dependence, overall low relationship and life satisfaction (Fergusson & Boden, 2008), and increased risk for Cannabis Use Disorder (CUD) (American Psychiatric Association [APA], 2013; Han et al., 2018). These findings reinforce the notion that the heavy cannabis use has deleterious effects on well-being in emerging adulthood and beyond.
In addition to the increased rates of cannabis use, emerging adulthood is associated with increases in anxiety and mood disorder symptoms (Gustavson et al., 2018). It is possible that emerging adults with emotional vulnerabilities may turn to heavy cannabis use as a means to cope—especially in regions where cannabis use is now legal. Coping-related cannabis use in emerging adulthood may set the stage for problems with cannabis and mood later in adulthood (Bonar et al., 2017; Moitra et al., 2016). Therefore, emerging adulthood is an opportune time for examining the relationship between cannabis use and emotional concerns. The purpose of this multi-wave longitudinal study was to examine the temporal associations between cannabis behaviors (i.e., use and related problems) and emotional issues (i.e., anxiety and depression) in a large sample of North American emerging adults.
Cannabis Use and Emotional Functioning
In the context of emotional difficulties among emerging adults, the rate of cannabis use as well as cannabis use problems are dimensions that have been examined in prior research (Brook et al., 2011; Georgiades & Boyle, 2007). A large prospective study of emerging adults found that frequent cannabis use, referring to use of cannabis every day or every few days, was associated with increased anxiety and depression (Hayatbakhsh et al., 2007), though there have been some inconsistent findings with regards to the relation between cannabis use and anxiety symptoms (Tournier et al., 2003). In a recent review of the effects of cannabis in people living with mental illness, Lowe et al. (2019) concluded that there are mixed results with regards to cannabis use and co-morbidity across anxiety disorders. However, there is increasing evidence that mental health difficulties are linked with cannabis use problems among emerging adults specifically. For instance, one study found that in a sample of emerging adults, elevated social anxiety was linked with increased risk for cannabis problems, with coping motives (but not cannabis use frequency) mediating this association (Buckner et al., 2007). Recent longitudinal research has shown that among emerging adults, changes in coping-motivated cannabis use are related to changes in the rate of cannabis use and cannabis use problems up to 12 months post-baseline (Moitra et al., 2021). In addition, a large self-report study of university students found that problematic cannabis use, as defined by scores in the severe range on the Cannabis Use Disorder Identification Test—Revised (CUDIT-R; Adamson et al., 2010), was positively related to anxiety symptoms, and this association was stronger among female students (Hellemans et al., 2019).
Regarding links with depression, a recent meta-analysis found that heavy cannabis use in adolescence increased risk for later depression as well as suicidal behavior in emerging adulthood (Gobbi et al., 2019). Other researchers found that emerging adults who used cannabis reported greater depressive symptoms and lower response to reward and fun seeking which may be indicative of increased apathy and lower mood (Wright et al., 2016). As with social anxiety, coping motives appear to influence the link between problematic cannabis use and depressive symptoms. For instance, recent research has found that among emerging adults, coping motives moderated the relationship between stress and depression, after controlling for anxiety (Glodosky & Cuttler, 2020). Other research by Moitra et al. (2015) found that, among emerging adults, using cannabis to cope was positively associated with DSM-5 cannabis use disorder, cannabis problem severity, depression and perceived stress.
Overall, there is a great deal of empirical support linking cannabis use to emotional problems, however presently very little is known about how these associations unfold as well as the directionality of these associations. In particular, there is minimal information regarding whether emotional difficulties (such as anxiety and depressive symptoms) lead to cannabis use as well as cannabis use problems or vice-versa. The directionality between emotional concerns as they relate to cannabis use and cannabis use problems in emerging adulthood has been largely understudied, despite knowing that emerging adulthood is a specific time period when the onset of cannabis use and emotional difficulties tend to occur (Kessler et al., 2005).
Potential Theoretical Models
Three theoretical models from the field of addictions can be used to clarify the temporal relationships between cannabis use and emotional difficulties among emerging adults: the vulnerability model, the scar/complication model and the reciprocal associations model. According to the vulnerability model (Khantzian, 1997), emotional problems emerge first and regular cannabis use is then used as a coping strategy. According to this model, people who use alcohol and/or drugs engage in this behavior because they are attempting to cope with strong negative emotions, such as anxiety or depression (Carrigan & Randall, 2003; Frone, 2016; McKernan et al., 2015; Weiss et al., 1992). For instance, one prospective study supporting the vulnerability model found that teen men with higher depressive symptoms at baseline subsequently used more cannabis later on, with the study having followed participants until they were within the 24- to 32-year-old age range (Wilkinson et al., 2016). Other longitudinal research has suggested that youth with more chronic or severe forms of depression during early adolescence are at elevated risk for the later development of a CUD (Rhew et al., 2017).
In contrast, the scar/complication model (Schuckit, 2006) posits that regular and heavy cannabis use precedes the development of emotional problems. A study sampling at-risk men from adolescence through to adulthood found support for the directional effect of cannabis use on the development of depressive symptoms but found limited evidence for the vulnerability model (Womack et al., 2016). Another study found significant associations between adolescent cannabis use and the later development of anxiety as well as depression, which was simultaneously paralleled by academic unpreparedness, delinquency, and poorer academic performance (D’Amico et al., 2016).
Finally, the reciprocal associations model (Wardell & Read, 2013), proposes that regular cannabis use both impacts and is impacted by emotional problems. This theoretical model posits that there are bidirectional effects, such that cannabis use leads to increased anxiety and depressive symptoms, and conversely anxiety and depressive symptoms lead to worsening problem cannabis use. To date, however, research on the reciprocal associations model is limited, although there is some research that suggests there may be reciprocal associations over time with regards to cannabis use and psychological trauma. A recent study suggests the association between chronic cannabis use and post traumatic stress disorder may be reciprocal in that cannabis using-individuals who are exposed to traumatic events may learn to regulate post traumatic stress symptoms through the use of cannabis (Lee et al., 2018).
The Current Study
The current study addresses a critical gap in the research literature by testing temporal associations between two dimensions of cannabis-related behaviors (i.e., cannabis use and related problems) and emotional symptoms (i.e., anxiety and depression) among a sample of emerging adults. Importantly, this research makes use of a short-term longitudinal design to more precisely understand the nature of these relationships within a briefer window of time. This design represents a significant advancement in the field, where the majority of studies have relied on cross-sectional data, which fails to address temporal precedence, potentially overlooking meaningful short-term relationships between cannabis use and common correlates, such as anxiety and depression (Marshall et al., 2020). The aim of the current study was to test the three competing theories of directionality regarding anxiety and depression as they relate to cannabis use and cannabis use problems.
Materials and Methods
Participants and Procedure
Participants were emerging adults (N = 299) recruited through MTurk, an online marketplace whereby workers can complete surveys. Recent published studies show that survey data collected on MTurk are both reliable and valid (Shapiro et al., 2013), including data about addictive behaviors (Kim & Hodgins, 2017). Several safeguards were employed to increase the quality of our data, including embedding captchas throughout the survey to prevent bots, excluding participants with extremely fast completion times (<300 s), and only including participants who had previously completed at least 300 Human Intelligence Tasks (HITS) on MTurk with an approval rating no less than 95%. The only other inclusion criteria were that participants had to be English-speaking adults from North America ranging in age from 18 to 25.
On average, participants were 23.69 years old (SD = 1.77) and the sample consisted of 58% women. The majority of participants reported their race as being White (68%), with the remainder of participants reporting their race as Black (11%), Hispanic (8%), East Asian (7%), South Asian (2%), Aboriginal (1%), Middle Eastern (1%), and other (2%). An estimated 49% of participants reported currently being in either full- or part-time studies at a post-secondary institution. Regarding education level, most of the sample reported having at least some level of postsecondary schooling, either completed or in progress (83%). Finally, 53% of participants reported having a full-time job; 27% reported being employed part-time; and 20% reported being currently unemployed.
Ethics approval was obtained from a research ethics board before data collection commenced. At the beginning of the online study, participants were provided the option to indicate their informed consent before taking part in the research. A three-wave 4-week questionnaire administration schedule was used in accordance with previous short-term, multi-wave studies (Mackinnon & Sherry, 2012; Mushquash et al., 2013). Participants were asked to complete online questionnaires at baseline (Time 1), 2-week (Time 2), and 1-month (Time 3) time points. The timeframe of questionnaires at Time 1 was the past 30-days, whereas the timeframe for Time 2 and 3 were both the past 2-weeks, reflecting the period of time elapsed between surveys. Of the 299 participants who completed Time 1, 200 participants completed Time 2, and 100 participants completed Time 3. The final sample included all 299 participants, given that data loss was unsystematic (see Descriptive Statistics and Missing Data Analysis Section below).
Measures
Rutgers Marijuana Cannabis Problems Index
The Rutgers Marijuana Cannabis Problems Index (RMPI; V. Johnson & White, 1989) is adapted from the Rutgers Alcohol Problem Index (RAPI; White & Labouvie, 1989). Participants rate how often they have experienced various negative consequences during the last year as a result of using marijuana on a 5-point scale (1 = never to 5 = more than 10 times). Responses to items were dichotomized to reflect whether a given problem was endorsed or not and then summed (possible score: 0–23). The RMPI was administered at all three timepoints and was used as the primary measure of cannabis problems. Past research literature supports the use of the RMPI as a valid measure of marijuana-related problems (e.g., Simons et al., 1998; White et al., 2005). See Table 1 for the internal consistencies of the RMPI at all timepoints.
Means, Standard Deviations, and Alpha Reliabilities for Depression, Anxiety, Cannabis Use and Related Problems.

Note. CES-D = Center for Epidemiological Studies Depression Scale (Radloff, 1977); GAD = General Anxiety Disorder 7-item Scale (GAD-7; Spitzer et al., 2006); RMPI = Rutgers Marijuana Cannabis Problems Index (RMPI; V. Johnson & White, 1989); C-TLFB = Cannabis Timeline Follow Back (adjusted from Sobell & Sobell, 1992). C-TLFB were measured using self-report quantities; therefore, alpha reliabilities are not available.
Cannabis Use Timeline Follow-Back
The Cannabis Use Timeline Follow-Back (C-TLFB; Norberg et al., 2012) is adapted from the TLFB method by Sobell and Sobell (1992), which was initially created to evaluate alcohol consumption. In the current study, the C-TLFB was adapted to assess marijuana use within the past 30 days and was administered at all three time points. To quantify cannabis use intake, participants were asked to report on their use of “standard joints” which was defined as .25 g of cannabis per joint as outlined by Schaub et al. (2013). Daily estimates were summed to provide total marijuana use over the previous 30 days. Given that total marijuana use was represented as a single value, alpha reliabilities are therefore not available. Using the TLFB as a self-report method to obtain retrospective estimates of daily drug use over a specified interval is well established as a psychometrically sound way to measure a variety of addictive behaviors (see Robinson et al., 2014).
The Generalized Anxiety Disorder Scale
The Generalized Anxiety Disorder Scale (GAD-7; Spitzer et al., 2006) consists of seven items and measures the extent to which an individual has experienced general anxiety symptoms including worry within the last 2 weeks. Participants rate each item on a scale from 0 (not at all sure) to 3 (nearly every day). The GAD-7 was administered at all three time points. Total scores ranged from 0 to 21, with higher scores indicating more anxiety symptoms. The GAD-7 is commonly used as a measure for anxiety in general (Beard & Björgvinsson, 2014) as well as in anxiety disorder research (Dear et al., 2011). Past research has demonstrated that it is a reliable and valid measure of general anxiety disorder (GAD) symptoms in the general population (Hinz et al., 2017; Löwe et al., 2008). See Table 1 for the internal consistencies of the GAD-7 at all timepoints.
The Center for Epidemiological Studies Depression Scale
The Center for Epidemiological Studies Depression Scale (CES-D; Radloff, 1997) consists of 20 items and provided a measure of depressive symptoms during the past week. The CES-D was administered at all three time points. Participants indicated how often they had experienced symptoms of depression from 0 (rarely to none of the time) to 3 (most or all of the time). Total scores range from 0 to 60, with higher scores indicating more depressive symptoms. Past research has demonstrated that the CES-D has high internal consistency (α = .85–.90) and moderate test-retest reliability (r = .40; Radloff, 1997). See Table 1 for the internal consistencies of the CES-D at all timepoints.
Data Analysis Overview
All analyses were conducted with SPSS Version 26 and MPlus Version 8.0. Descriptive statistics for all measures were inspected and a missing data analysis was conducted to determine if there were any differences in baseline scores between individuals with complete data versus those with incomplete data across the time points. These initial preliminary analyses were followed by a series of cross-lagged panel models (CLPM), which were conducted to evaluate the temporal associations between cannabis use behaviors and depression/anxiety in our emerging adult sample. The first two CLPMs examined the associations between anxiety and both cannabis use (model 1) and related problems (model 2). The remaining two CLPMs examined the associations between depression and both cannabis use (model 3) and related problems (model 4).
Both gender (i.e., men and women) as well as student status (i.e., student or non-student) were included as covariates in the model given that the literature shows differences in cannabis use/problems and emotional problems between these groups. Some data suggest that female emerging adults are a group known to be at risk for comorbid cannabis-use disorder and clinical depression (Moitra et al., 2016). However, men tend to report using cannabis with greater frequency and in greater quantities as compared to women (Farmer et al., 2015; Foster et al., 2016). A recent study also found associations between cannabis use and depression among a large sample of students from 41 Canadian post-secondary institutions (Esmaeelzadeh et al., 2018), reflecting the unique vulnerability of the student population.
We assessed goodness of fit according to recommended guidelines (Hu & Bentler, 1999; Kline, 2016), where model fit is considered excellent if the following guidelines are met: non-significant χ2 (p > .05), comparative fit index [CFI] ≥ 0.95, root-mean-square error of approximation [RMSEA] ≤ 0.06, and standardized root mean square residual [SRMR] ≤ 0.08. If fit of an initial model was poor, we inspected the modification indices for theoretically permissible paths to add to the model that would result in improved fit. Fit was considered substantially improved if the CFI value increased by 0.01 or more (Cheung & Rensvold, 2002). Full information maximum likelihood estimation was used for all CLPMs.
Results
Descriptive Statistics and Missing Data Analysis
Potential baseline differences between those with incomplete data (coded as 0; n = 199) and complete data (coded as 1; n = 100) were examined using a series of t-tests. There were no significant baseline group differences in anxiety [t(297) = 1.47, p = .14], depression [t(297) = 1.79, p = .07], cannabis use problems [t(297) = 1.05, p = .29], and the rate of cannabis use itself [t(297) = 1.29, p = .19]. These results provided support for the data being missing at random. The means in Table 1 suggest that the sample as a whole exceeds the cut-off of 16 for depression. Similarly, mean scores exceed the GAD-7 cut-off of five for mild anxiety.
Cross-Lagged Panel Models
Model 1: Anxiety and Cannabis Use
A model with all autoregressive and cross-lagged paths provided excellent fit to the data (χ2(4) = 6.84, p = .144, CFI = 0.992; RMSEA = 0.049 (95% CI [0.000, 0.109]); SRMR = 0.015). This model also included gender and student status as time invariant covariates (i.e., their effects on anxiety and cannabis use were controlled for at all time points). As seen in Figure 1, all autoregressive paths were statistically significant, suggesting stability in anxiety and cannabis use over the study period. None of the cross-lagged paths were significant, suggesting no directional or reciprocal associations between anxiety and cannabis use in our sample.
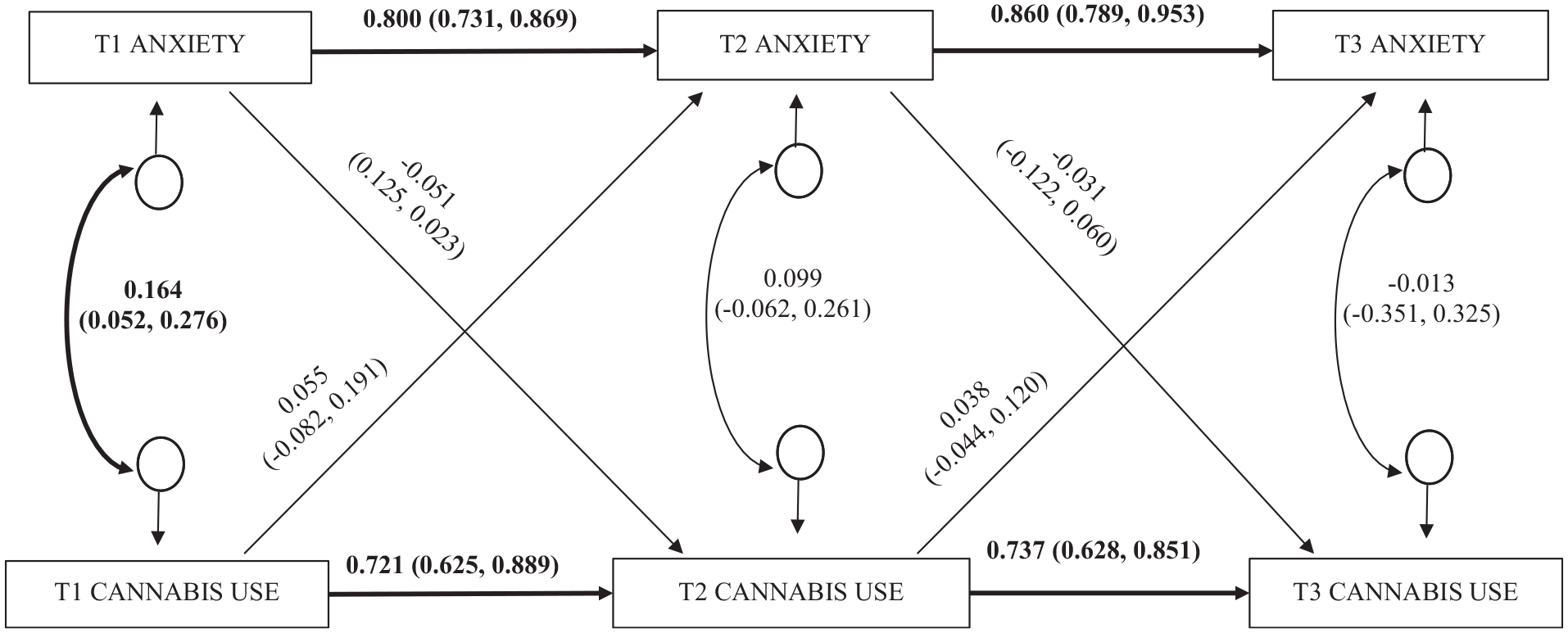
A three timepoint cross-lagged panel model examining the temporal relation between anxiety and cannabis use.
Model 2: Anxiety and Cannabis Problems
A model with all autoregressive and cross-lagged paths provided excellent fit to the data (χ2(4) = 4.926, p = .295, CFI = 0.997; RMSEA = 0.028 (95% CI [0.000, 0.095]); SRMR = 0.021). This model also included gender and student status as time invariant covariates. As seen in Figure 2, all autoregressive paths were statistically significant, suggesting stability in anxiety and cannabis use problems over the study period. The cross-lagged path from Time 1 anxiety to Time 2 cannabis problems was also significant. No other cross-lagged paths were supported by the data. This provides some support for the vulnerability model given that anxious symptoms preceded cannabis use problems.

A three timepoint cross-lagged panel model examining the temporal relation between anxiety and cannabis problems.
Model 3: Depression and Cannabis Use
An initial model with all autoregressive and cross-lagged paths provided suboptimal fit to the data (χ2(4) = 14.652, p = .005, CFI = 0.971; RMSEA = 0.094 (95% CI [0.046, 0.148]); SRMR = 0.021). This model also included gender and student status as time invariant covariates. The modification indices suggested including covariance between the error terms for Time 1 and Time 3 depression. Adding this covariance improved model fit appreciably (χ2(3) = 1.342, p = .719, CFI = 1.000; RMSEA = 0.000 (95% CI [0.000, 0.071]); SRMR = 0.007); and therefore, this model was retained. Figure 3 illustrates that all autoregressive paths were statistically significant, suggesting stability in depression and cannabis use over the three time points. None of the cross-lagged paths were significant, suggesting no directional or reciprocal associations between depression and cannabis use in our sample.

A three timepoint cross-lagged panel model examining the temporal relation between depression and cannabis use.
Model 4: Depression and Cannabis Problems
An initial model with all autoregressive and cross-lagged paths provided excellent fit to the data (χ2(4) = 7.812, p = .098, CFI = 0.988; RMSEA = 0.056 (95% CI [0.000, 0.115]); SRMR = 0.025). This model also included gender and student status as time invariant covariates. Figure 4 illustrates that all autoregressive paths were significant, again suggesting consistency in depression and cannabis problems across the study period. Half of the cross-lagged paths were significant: Time 1 depression to Time 2 cannabis problems, and in conjunction Time 1 cannabis problems to Time 2 depression. This finding provides support for the reciprocal model given the bidirectional association between depression and cannabis problems.

A three timepoint cross-lagged panel model examining the temporal relation between depression and cannabis problems.
Discussion
The purpose of the current study was to extend what is known thus far about the directionality of anxiety and depression in terms of their link to cannabis use as well as cannabis problems within a sample of emerging adults. The CLPM analyses revealed that whereas there were no directional or reciprocal associations for cannabis use and its link with anxiety and depression, there were links between cannabis problems and emotional problems. As mentioned previously, these findings align with much of the existing literature in that they demonstrate that cannabis use problems rather than cannabis use are more influential with regards to emotional functioning within this age group. These research findings suggest the focus should perhaps be less on the rate of cannabis use and instead attention should be on the ways in which it causes impairments and challenges in functioning and daily life, in keeping with the clinical importance attached to impairment and life impact.
For anxiety symptoms, the current findings suggest support for the vulnerability model given that Time 1 anxiety prospectively predicted Time 2 cannabis use problems. This is not surprising given that as noted previously, research has provided support for the vulnerability model hypothesis in that mental health concerns have been linked to experiencing subsequent problems with cannabis use (Rhew et al., 2017; Wilkinson et al., 2016). For example, experimental research has found that individuals with social anxiety disorder are more likely to crave cannabis during social interactions, a response that supports a coping mechanism (Buckner et al., 2016). Regarding depressive symptoms, the present findings revealed that there is a bidirectional relationship between depression and cannabis problems, which is consistent with the general coping motives literature, where emotional problems tend to be more strongly linked with cannabis problems rather than cannabis use. This statement is made with the caveat that the general coping motives literature does not usually differentiate between coping with depression and coping with anxiety; therefore, it is important to consider differential motives for coping with anxiety versus depressive symptoms (Grant et al., 2009). Using cannabis to cope with symptoms of depression may influence the degree to which emerging adults are prone to experiencing both depression and problems related to their use of cannabis use. Researchers continue to show that using cannabis to cope with negative affect is related to higher levels of depression and that it is ultimately maladaptive as it exacerbates the same problems that coping-motivated cannabis users are trying to alleviate (Glodosky & Cuttler, 2020).
Implications of the Current Research and Future Directions
It is well established that emerging adults are among those most at-risk for experiencing both emotional concerns and harmful effects of cannabis use (Center for Behavioral Health Statistics and Quality, 2018; Fergusson & Boden, 2008; Health Canada, 2018; Kessler et al., 2005). To date, however, the directionality of these effects has thus far remained largely unexplored. Using CLPM, the current study provides important insight into the temporal relationships between cannabis use and mental health problems among emerging adults, although the shorter duration of the measurement intervals does not allow for assessment of causal relationships (for related discussion, see Kearney, 2017).
In addition, the current study did not explore mechanisms that link emotional concerns and cannabis outcomes. To expand upon this research, it may be useful to also assess cannabis use motives along with other risk and protective factors that contribute to the experience of depressive symptoms and cannabis related problems among emerging adults. For instance, it may be pertinent to also assess relevant ecological factors including socioeconomic status, and level of social or familial support (see R. M. Johnson & Guttmannova, 2019) as well as individual factors such as the occurrence of trauma or emotion regulation vulnerabilities such as a ruminative response style. Unfortunately, we were not able to model the complex associations between such factors in our study because these measures were not included in data collection. Additionally, it would be useful for future research to also assess polysubstance use in order to get a sense of whether use of other substances may be driving or intensifying the current findings. Bearing this in mind, frequent cannabis use is associated with increased anxiety and depression in emerging adults regardless of whether other illicit drugs have been used (Hayatbakhsh et al., 2007). Although the shorter time frame of the current study allowed for more precise and in depth understanding of the cannabis use-emotional concerns relationship, future research should involve longer windows of time to better assess causality over the course of critical developmental periods (e.g., adolescence to emerging adulthood). This research will provide important information to assist with prevention efforts designed to minimize the harmful effects of cannabis use during adolescence and throughout their later years. Finally, our sample was primarily comprised of participants who self-identified as White and many reported either being in or having finished postsecondary education. It will be essential for future work to recruit more diverse samples to examine potential differences based on important sociodemographic characteristics.
One overarching implication of this research was to identify the ways in which it may be most beneficial to intervene with regards to addressing cannabis use problems and issues related to emotional functioning among emerging adults. The current results suggest it would be valuable to design interventions that acknowledge the effects of anxiety on the subsequent development of cannabis use problems, as well as the bidirectional influence between depressive symptoms and issues related to cannabis use. The present research highlights that for this age group in particular, it is likely less effective to target services toward addressing the rate of cannabis use itself. Rather, results suggest that efforts should be focused on ameliorating the impact of cannabis use problems and issues related to emotional health and well-being. A one-size-fits-all approach to intervention designed to address the needs of emerging adults is simply inadequate. Few substance use services have been developed to address the specific needs of emerging adults despite this population reporting high comorbidity rates between substance use and mental health conditions as well as unique challenges posed by the transition to adulthood itself (Bergman et al., 2016; Sheidow et al., 2012). Results from this research emphasize that there is both merit and much to be gained with regards to exploring the risk factors associated with emerging adults’ use of cannabis in the interests of developing and implementing more effective and age-appropriate treatment interventions.
Footnotes
Author Note
This research was conducted while Dr. Matthew Keough was at the University of Manitoba. He is now at York University and may be contacted at
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge University of Manitoba start-up funding in support of this research.
Ethics Approval
Ethics approval (study number HS22657) was obtained from the University of Manitoba Psychology/Sociology Research Ethics Board.
Consent to Participate
Informed consent (via online questionnaire administration) was obtained from all individual participants included in the research study.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.