
Abstract
The quality of life of children with leukemia can be affected by their parents’ emotional stress. We examined the effects of social care collaboration on the psychological states of parents of children with leukemia. This was a prospective, single-center, randomized study. The parents of children diagnosed with leukemia between January 1 and December 31, 2021, were divided randomly into experimental and control groups, in which the health education model and psychological counselling by medical social workers paired with online health education by nurses were used, respectively. Questionnaire surveys were used to evaluate their psychological state. Data were analyzed using t-test and linear regressions. Varying degrees of anxiety and depression were present in 94% of the participants. Anxiety and depression scores were significantly different between the groups, as indicated by the SAS (p = .002), SDS (p = .016), and SCL-90 (p = .015) scales. Income level was related to the degree of anxiety (p = .047). Although anxiety and depression scores of both groups declined with time, the trend showed no significant difference (anxiety: p = .957; depression: p = .776). Social care collaboration was beneficial in relieving negative emotions in parents of children with leukemia.
Plain language summary
Purpose: Examined the effects of social care cooperation on the psychological states of parents of children with leukemia. Methods: This was a prospective, single-center, randomized, controlled, and operationally feasible study. A case-control study design was used to randomly assign participants into observation and experimental groups. The control group used the traditional nursing health education model according to the standard of nursing work. In the experimental group, online psychological counselling with the participation of medical social workers, based on the traditional nursing health education model. Conclusion: Social care collaboration was beneficial in relieving negative emotions in parents of children with leukemia. Implication: This study mainly focuses on the status and improvement methods of the caregivers’ psychological symptoms at the early stage of the disease. This study lays a foundation for the psychological care of parents of children with whole-cycle leukemia in the future. Limitations: The number of participants that could be enrolled during the observation period was limited. Moreover, this study mainly focuses on the status and improvement methods of the caregivers’ psychological symptoms at the early stage of the disease. Thus, it lacks long-term attention and intervention for parents with psychological problems.
Introduction
Leukemia is the most common malignant hematological disease in children (Teachey & O’Connor, 2020), with its diagnosis and treatment protocols being complex and highly specialized. In the early stages of the disease, the parents of children with leukemia often lack knowledge and experience in caring for them. Parents may experience serious anxiety regarding their own ability to cope with stressful events, their ability to change roles in caring for their child, the impact of their child’s illness on the quality of life of the family, and the effectiveness of early treatment, particularly in the first few months of acute leukemia diagnosis in children (Irwanto et al., 2020). The outward expression of stressful emotions by the parents of children with acute leukemia can exacerbate the child’s tendency to communicate negatively. This impacts the child’s ability to express their feelings and physical discomfort, ultimately affecting their quality of life. Studies have shown that children with cancer have a poorer quality of life than healthy children (Kinahan et al., 2012). This results in physical and psychological stress that requires various types of support, including the provision of information, symptom management, meeting psychosocial needs, financial support, and the need for high-quality medical care services. Therefore, attention should be paid to the mental health of parents. Studies have shown that brief, focused interventions targeting children with critical illnesses and their parents can help prevent and reduce parental trauma, as well as the parents’ anxiety reaction to their child’s illness (Kaushal et al., 2022).
Social care collaboration has a broad definition that includes the psychosocial systems and communication domains of healthcare provision. Care coordination covers several aspects, such as anticipation of patient needs for pain and symptom management, psychosocial needs management, and functional status (Strekalova et al., 2018). Collaboration between nurses and medical social workers in nursing work in the ward is important. Moreover, online counselling has become an effective and convenient channel to gain psychological knowledge (Strekalova et al., 2018). The positive outcomes of care coordination in the management of chronic diseases have been demonstrated (Hussey et al., 2014).
This study aimed to explore the effect of social care collaboration conducted by regular online psychological counselling sessions on the psychological state of the parents of children with leukemia. Therefore, our findings may provide evidence for developing an effective health education model for them.
Methods
Design
This was a prospective, single-center, randomized, controlled, and operationally feasible study. A case-control study design was used to randomly assign participants into observation and experimental groups. The control group used the traditional nursing health education model according to the standard of nursing work, including verbal education at admission, distribution of leaflets containing acute leukemia-related knowledge, health lectures, education, psychological care at any time during their child’s treatment, and discharge education. In the experimental group, online psychological counselling with the participation of medical social workers, as well as targeted health education by nurse educators were provided based on the traditional nursing health education model.
Within the first week of the child’s hospitalization, medical social workers reached out to the parents for initial communication and to conduct psychological assessments. Thereafter, online psychological counselling was conducted once a week (to explain the sources of stress and manifestations of stress reactions, as well as to perform small group activities and art therapy, online lectures, etc.). The evaluation of the psychological state and the implementation of psychological counselling were monitored and controlled by professional psychologists.
The nursing staff connected online with the parents once a week, using video conferencing software, such as DingTalk or Tencent Meetings (high-definition, smooth, convenient, easy to use, safe, and reliable video conferencing products) to conduct targeted lectures and explain relevant information on acute leukemia. As the groups to which parents were assigned were fixed, it facilitated communication and the release of emotions between the group members. Initially, the study planned to introduce 6–8 sessions of online services according to the social work regulations. However, based on the scoring in the second month, further communications with the psychologists led to an extension of the online social service model for 3 months, with a total of 12 sessions. In both the experimental and control groups, the psychological states of the parents were assessed at the time of the child’s diagnosis (within 7 days), as well as at 1, 2, and 3 months after diagnosis.
Participants
The parents of children diagnosed with acute leukemia at the Department of Haematology, XXX Hospital, from January 1, 2021 to December 31, 2021, were randomly chosen following the criteria below. The participants come from 10 provinces and three municipalities in China. They were divided into experimental and observation groups, each with 33 participants, making a total of 66 cases in the study. The inclusion criteria were as follows: (1) the child met the diagnostic criteria for acute leukemia, had a manageable disease state, had no other serious illness or chronic disease, and was <14 years; (2) the child’s parents agreed to their child receiving leukemia treatment; and (3) the study participant was either the father or mother of the child and was involved primarily in daily care. The exclusion criteria were as follows: (1) the child had other malignant diseases in addition to leukemia; (2) the parents were not able to understand the explanations accurately owing to differences in literacy or communication barriers; and (3) the child died during treatment. All parents who participated in the study did so voluntarily and gave their signed (written) informed consent.
Data Collection
The participants completed questionnaire surveys. The questionnaire was divided into four sections: general information, the Zung Self-Rating Anxiety Scale (SAS) (Zung, 1971), the Zung Self-Rating Depression Scale (SDS) (Zung, 1965), and the Symptom Checklist-90 (SCL-90) (Derogatis et al., 1976). The SAS scale consists of 20 items, with the score threshold set at a T score of 50 points, where a higher score indicates a more pronounced tendency toward anxiety. Scores of 50–59, 60–69, and ≥70 points indicate mild, moderate, and severe anxiety, respectively. The SDS scale consists of 20 items, with each item scored as one of four levels. The cumulative scores of all the items were considered the raw scores, which were converted into standard scores and processed statistically, with a normal upper reference value of 53 points. A total standard score of 53–62, 63–72, and ≥72 points indicated mild, moderate, and severe depression, respectively. The SCL-90 scale consists of 90 symptoms, which are divided into 10 subcategories: somatization, obsessive-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobia, paranoia, psychoticism, and other symptoms. Each symptom of the SCL-90 is scored on a 5-point scale, ranging from 1 to 5 points, indicating “normal,”“mild,”“moderate,”“severe,” and “extremely severe” symptoms, respectively. Depression is defined when the total score of 90 symptoms is higher than 160 points or when the positive items are more than 43 (items scored 1–4 points are considered positive). This test was performed synchronously with the Zung SAS and SDS.
The scoring for both groups of parents was conducted using a standard script and completed independently by parents within 7 days of their child’s admission. If the parents could not understand the questions, the nurses provided explanations to help them, without directing their responses.
Ethical Considerations
The study protocol was approved by the Ethics Committee of the XXX, with ethical review number XXXXX and confidentiality was maintained throughout the study. The study was conducted in accordance with the 1995 Declaration of Helsinki.
Data Analysis
Statistical analyses were performed using SPSS 22.0 (IBM Corp., Armonk, NY, USA). The measurement data were expressed as means ± standard deviations. The t-test was used to compare the means, with p < .05 representing a significant difference. Linear regression was used to compare the slopes of the two data sets. The inspection level was set as .05 and the statistical power was .9.
The Zung SDS score of the control group was determined based on the literature and previous clinical experience, while the SDS score of the experimental group was calculated using the Power Analysis and Sample Size (PASS) software (NCSS, LLC. Kaysville, UT, USA).
Results
The basic information of the experimental group and the control group is summarized in Table 1. Based on the SAS scale scores, 94% of the parents in both groups experienced different degrees of anxiety states on the seventh day of their child’s leukemia diagnosis. Meanwhile, the percentage of parents in the experimental and control groups who suffered different degrees of depression according to the SDS scores was also 94%. None of the participants was classified as having severe anxiety and depression (Table 2). Analysis of the relationship between several general factors and the degree of anxiety and depression showed that the degree of anxiety and depression differed significantly between parents of different income levels (p = .047). However, the degrees of anxiety and depression in the parents were not significantly different based on sex, age, occupation, education level, and leukemia classifications (Table 3).
Basic Information of Participants.

Degree of SAS and SDS of Parents with Children Diagnosed with Leukemia on the Seventh Day of Diagnosis.

Note. SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale.
Influences of Different Factors on the Level of Anxiety and Depression.

SAS, SDS, and SCL-90 Scale Assessments
As shown in Table 4, assessment using the SAS and SDS scales revealed that the anxiety (51.31 ± 6.64 vs. 53.32 ± 6.62 points) and depression (55.90 ± 8.27 vs. 53.83 ± 8.81 points) scores were significantly different between the experimental and observation groups (p < .05). In the assessment using the SCL-90 symptom scale, the t-test was used to analyze the differences between the two groups among all the factors. The anxiety and depression factors as well as obsessive-compulsive symptoms, interpersonal sensitivity, appetite, and sleeping, showed significant differences between the experimental and observation groups (p < .05). In contrast, hostility, phobia, paranoia, and psychoticism factors did not show significant differences between the two groups (p > .05).
Comparison of the Differences Between the SAS Scale, SDS Scale, and SCL-90 Scale for Parents of Children Diagnosed with Leukemia.

Note. SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; SCL-90 = Symptom Checklist-90; SD = standard deviation.
p < .05. **p < .0.
Linear Regression Analysis of Anxiety and Depression Over Time
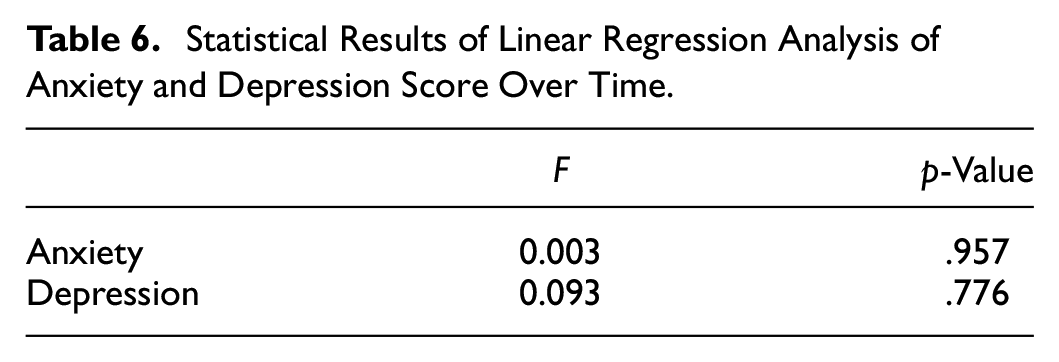
During the study, which lasted 3 months, the psychological states of the parents of children with leukemia in both groups were assessed at the time of diagnosis (within 7 days), and at one, two, and 3 months (Table 5). The SAS and SDS scores of both groups decreased with time. However, a linear regression analysis showed no significant differences in the downward trends in either group (p > .05) (Table 6).
SAS and SDS Scores of Parents with Children Diagnosed with Leukemia at Regular Intervals Post-Diagnosis.
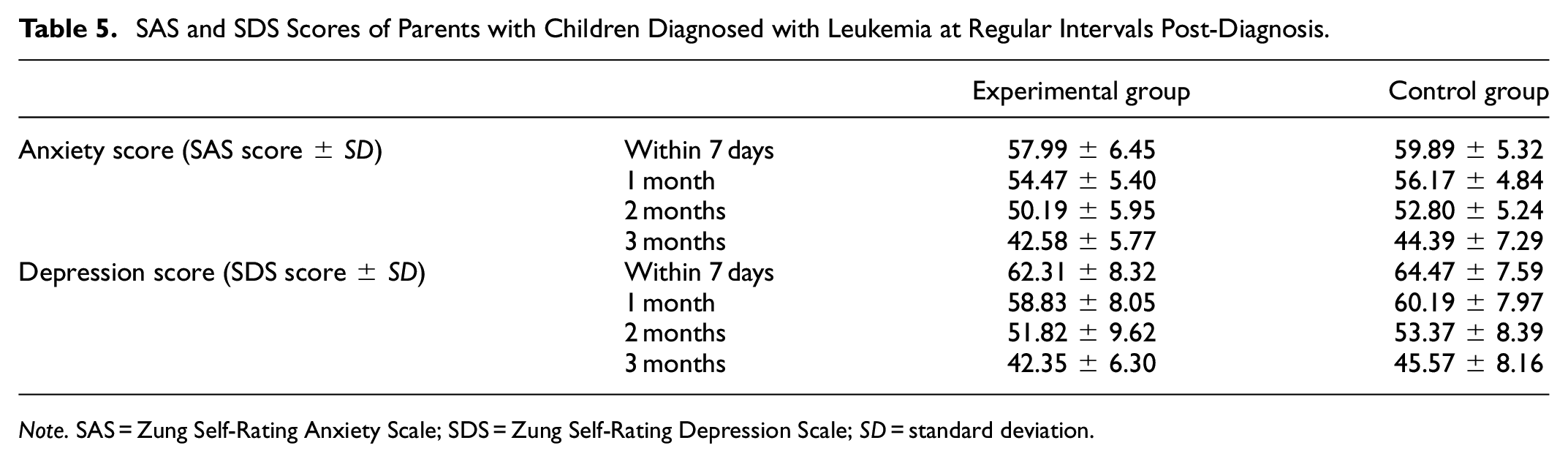
Note. SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; SD = standard deviation.
Statistical Results of Linear Regression Analysis of Anxiety and Depression Score Over Time.
Discussion
Parents of children with acute leukemia often suffer from adverse emotions, such as anxiety and depression. Studies have shown that caregivers of patients with leukemia who are at high risk have a relatively greater psychosocial burden (Yucel et al., 2021). A higher stress level was observed in the direct caregivers of pediatric patients than that of elder patients. The stress faced by the parents of pediatric patients is mainly a psychological burden (Posluszny et al., 2019). Although most of the parents are working adults, health insurance can cover some financial impact. However, frequent invasive procedures at the beginning of the treatment, such as lumbar punctures, bone marrow punctures, and long treatment cycles, contribute to elevated levels of anxiety and depression (Peterson et al, 2020). For parents of children with cancer, although both the mother and father participate in the daily care of their child, the mother often assumes the primary caregiving role. As mothers in developing countries assume more responsibility in providing care and nurturing to their children, they are more vulnerable to adverse psychosocial factors. This can seriously affect the parents’ psychological and physical health, resulting in the manifestation of anxiety and depression. In addition, parents’ emotions can affect the condition of their child’s disease, including their physical and mental health, recovery and prognosis, and even quality of life, as they are the primary caregivers of the child (Aburn & Gott, 2011; Meyler et al., 2010; Yamazaki et al., 2005).
Therefore, psychological interventions are important for parents of children with leukemia, which have been demonstrated to result in positive health outcomes for both the child and the parents (Eccleston et al., 2015). A previous study reported that the lower the psychosocial burden the caregivers have and the more prepared they are for their role, and the better care they can provide for their patients (Yucel et al., 2021). A comprehensive and effective psychological service should include pediatric hematologists and oncologists, social workers, psychologists, and professional nurses to help the parents understand and cope with the stress that they face, as well as answer their questions regarding psychological and disease-related issues. They should listen patiently, help them express their emotions, provide explanations, and offer advice and support (Sherief et al., 2015).
In this study, the psychological states of the parents were evaluated using the SAS, SDS, and SCL-90 scales at the time of their children’s diagnosis of acute leukemia. Anxiety and depression to varying degrees were observed in the results. In total, 25 and 29 participants experienced mild and moderate anxiety, respectively. Moreover, 17 and 37 participants presented mild and moderate depression, respectively. Mild or moderate anxiety and depression were present in 94% of the participants. In the results of the SCL-90 scale, the scores of the five factors—somatization, interpersonal sensitivity, depression, anxiety, and hostility—showed a significant increase compared with the standard domestic level. These findings indicate that the parents of children with leukemia commonly suffer psychological problems to a varying degree.
It should be noted that parents who directly cared for children with acute leukemia showed no significant differences in the anxiety, depression, or symptom scores at different levels of disease risk. This may be related to the fact that children were the main population that the caregivers cared for and that the caregivers’ focus was on their children’s illness; thus, after the shock of the diagnosis, they may not have been able to relieve distress. Acute leukemia in children is a rapidly changing disease, and there is high risk during treatment, regardless of the level of risk determined by the medical professionals at the early stages of the disease. The findings regarding parental income and anxiety level versus the anxiety-depression levels were inconsistent with those of studies conducted in other countries (Posluszny et al., 2019), and may be related to the relative concentration of quality healthcare resources in China, the broader source of patients, and the fact that regional income is not balanced. Most of the children with acute leukemia in this study were under the long-term direct care of their mothers.
To assess the psychological condition of the parents of children with leukemia, we implemented targeted, planned, systematic, and professional psychological guidance with health education using an online platform. This aimed to help the parents understand information relevant to the care of children with leukemia, thereby reducing the adverse effects of their negative emotions, and achieving the purpose of promoting the physical and mental health of both the child and the parents. The social care collaboration model was applied to the experimental group, while the traditional health education model was used in the observation group. The results show that the number of parents with anxiety and depression psychological states was significantly lower in the experimental group, which indicates the positive effect of the social care collaboration model on the psychological state of parents of children with leukemia.
In a previous study, researchers effectively utilized hands-on training and interactive sessions, and created a safe and supportive environment to allow the parents of children with leukemia to express their emotions (Kaushal et al., 2022). There is also evidence that targeted interventions enable the parents to be more expressive and communicative. The distress and anxiety of caregivers can be significantly improved through interventions, such as relaxation techniques and nursing health education, which, by extension, improves their mental health condition (Bevans et al., 2014). Thus, such interventions make them feel supported and cared for, which helps create harmonious family relationships and improve the condition of their children (Langer et al., 2018).
During the psychological intervention after the diagnosis, which lasted for 3 months, the changing trend of participants’ psychological state was also evaluated. The anxiety, depression, and symptom scores of the SCL-90 in the experimental and control groups decreased as time went on. This is consistent with a previous study that claimed that parental psychological problems are particularly pertinent at the time of diagnosis and can decline over time (Peterson et al., 2020). Even though the experimental group showed a slight improvement in a shorter time span compared to the control group, there is no significant difference in the degree of improvement of the psychological state between the two groups. However, the anxiety, depression, and symptom scores of the SCL-90 of the experiment group were always lower than those of the control group, which indicated the effect of psychological intervention in this research to some extent.
Our psychological intervention was applied on new media platforms, which is a relatively new way for psychological service. With the rapid development of the Internet and the digitalization of information, the forms of health communication are becoming increasingly diversified. The parents of children with leukemia are mostly young and middle-aged people who are familiar with WeChat, online videos, and popular media communication technologies and platforms, which have become essential communication tools. The use of online tools solves the problems of time and space requirements, enabling a more effective approach to psychological interventions. In addition, the concept of “humanistic care” formed under the new medical model has been emphasized and gradually promoted in clinical practice. Humanistic care helps in the care of diseases, meets the psychological needs of patients’ families, and improves treatment results and satisfaction.
During our research, it was observed that psychological support can help reduce parents’ psychological distress, provide health education, and systematic knowledge on disease care, and establish a positive attitude toward treatment among parents of patients. Thus, creating favorable conditions helps stabilize the child’s emotions during disease treatment and recovery. Through the use of psychological counselling and health education conducted online by medical social workers and professional nurses, the psychological problems of the parents can be solved as they receive professional nursing knowledge alongside their child’s treatment. These strategies have good application prospects, justifying their promotion and use in hospitals. When this method is implemented, medical social workers and professional nursing staff involved should be placed permanently to ensure continuity of quality care. This also helps to meet the requirement of reducing the number of people gathering as part of the “new normal” of the COVID-19 pandemic. Therefore, medical social workers lay the psychological foundation through psychological counselling while nursing work is carried out on an individual basis, with health education being made available on new media platforms. This model of health education, using psychological counselling, has prospects for use in hospitals and is a scientific and rational social care collaboration model.
In general, although our results were largely consistent with those of previous studies, there were limitations to our study. The number of participants that could be enrolled during the observation period was limited. Moreover, this study mainly focuses on the status and improvement methods of the caregivers’ psychological symptoms at the early stage of the disease. Thus, it lacks long-term attention and intervention for parents with psychological problems. It will be meaningful to confirm the effects on the parents’ psychological state at a long-term follow-up, as the caregivers may continuously adapt to their new roles after their children are diagnosed. This study lays a foundation for the psychological care of parents of children with whole-cycle leukemia in the future.
Conclusion
Collaboration between medical social workers and nursing staff in carrying out psychological counselling and health education was shown to be beneficial in relieving some negative emotions in parents of children with leukemia. In particular, more attention should be paid to anxiety, depression, and interpersonal relationships of parents in low-income families at the initial stage of diagnosis.
Footnotes
Acknowledgements
All the authors work at the Capital Institute of Pediatrics and are members of the research group. Thanks to all the members of the research group.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Capital Institute of Pediatrics [grant number GZ-2021-07].
Authorship Statement
CW and PF designed the study, BZ collected information, and CW analyzed the data and drafted the manuscript. All the listed authors meet the authorship criteria and are in agreement with the final content and submission of the manuscript.
Ethical Approval
The study protocol was approved by the Ethics Committee of the Capital Institute of Paediatrics Children’s Hospital, with ethical review number SHERLL2021049 and confidentiality was maintained throughout the study. The study was in line with the 1995 Declaration of Helsinki.
Data Availability Statement
All data in the manuscript are reasonably available from the corresponding author.