
Abstract
How much time parents spend with their children is likely to influence their judgments of children’s behaviors and the behaviors themselves. In the diagnosis of children with attention-deficit/hyperactivity disorder (ADHD), parents are key informants and decide whether their children should receive medication. This exploratory study investigates the relationship between working parents’ willingness to medicate ADHD-like behaviors and the time they can spend with their children during a regular workday. The participants (409 parents of 5- to 17- year-old children reporting having no child with emotional or behavioral problems and 87 reporting having such a child) were drawn from a population-based telephone survey of parents stratified by race and ethnicity in two urban Florida counties. Path analysis models, controlling for selected sociodemographic and household variables, showed that spending more time with one’s children during a regular workday and self-identifying as African American were negatively related to willingness to medicate among parents of children with problems. Among parents reporting no children with problems, only the number of children in the household and the parent-type household showed relationships to willingness to medicate, while mothers were more likely than fathers to spend more time with children. These observed relationships were of moderate effect but underscore the importance to initiate studies using valid measures of quantity and quality of parental time spent with ADHD children, and to query parents on these points when assessing the information they provide to clinicians.
Keywords
Introduction
According to data from parental reports analyzed by the Centers for Disease Control (CDC, 2010), the number of children in the United States diagnosed with attention-deficit/hyperactivity disorder (ADHD) increased annually by 5.5% between 2003 and 2007, and represents about 10% of school-aged children. In addition, according to these parental reports, approximately 66% of diagnosed children receive prescribed psychoactive medications. Parents’ perceptions of their children’s behavior largely determine whether a child will be diagnosed and medicated. This study investigates the relationship between working parents’ willingness to medicate children’s ADHD-like behaviors and the time these parents are able to spend with children during a regular workday.
Literature Review
The possibility of a relationship between parental time and willingness to medicate children’s problematic behaviors and the pertinence of exploring this relationship rest on well-validated observations. These are that spending time with one’s children appears very beneficial for their emotional well-being, health, and academic performance (Hofferth & Sandberg, 2001; Hsin, 2009; Kalenkoski, Ribar, & Stratton, 2007; Waldfogel, 2006). Unfortunately, such time is not abundantly available to all parents. Moreover, perception of time varies from one person to another depending on circumstances. One understanding from consumer research suggests that people perceive time by converting “objective” time into their “subjective” time (Hornik, 1984; Hornik & Zakay, 1996). So, different people perceive the passing of time differently—regardless of the objective time—depending on their mindset. For example, a 1-hr class lecture feels like a few minutes for the passionate professor but could feel like 3 hr for a disengaged student. In turn, how much time one perceives to have available affects one’s ability to judge and reason (Carstensen, Isaacowitz, & Charles, 1999). The socioemotional selectivity theory proposes that when time is perceived as open-ended, people prioritize knowledge-based decision. They spend time considering alternatives and think about what is the best course of action. The opposite happens when people are pressured for time. In this case, their emotions take over and guide decisions (Carstensen et al., 1999). In sum, how much time parents spend with children is likely to influence children’s behavior as well as parents’ judgment of that behavior.
Given the lack of biological markers to diagnose ADHD, the judgments of parents and teachers about children’s behaviors are the essential ingredients in its diagnosis and treatment by clinicians (Fernández & Arcia, 2004; Gornall, 2007). Judgments about children’s behavior are likely to be influenced by how much time parents have to think and reason about the nature of the behaviors, the different options to manage them—and the consequences of the behaviors and the options. In an empirical study attempting to determine reasons behind parents’ choice to medicate their autistic child, for example, it was found that parental stress, rather than the severity of the child’s symptoms or impairment, was the stronger predictor (Konstantareas, Homatidis, & Cesaroni, 1995).
The literature has documented the difficulties experienced by parents of ADHD children as they attempt to determine whether their children’s behavior is normal (Kendall, 1998; Hansen & Hansen, 2006), as they “battle” with health care and educational systems (Blum, 2007), as they decide whether to medicate their children or not (Taylor, O’Donoghue, & Houghton, 2006), or as they struggle with the trial and error phase once they choose to medicate (Dennis, Davis, Johnson, Brooks, & Humbl, 2008). What is not documented in the literature, however, is the amount of time these parents generally spend with their children, or the amount of time they might require to decide whether to medicate their children or not.
How much time parents spend with children seems to relate to various sociodemographic variables. These variables include parents’ work status and satisfaction (Beaujot & Andersen, 2007; Roeters & Treas, 2011), gender (Abroms & Goldscheider, 2002), race and ethnicity (Golden, 2008), and education, income, and characteristics of their children such as age and gender (Milkie, Raley, & Bianchi, 2009), as well as whether parents head one- versus two-parent families (Hofferth & Sandberg, 2001). The strengths of these relationships vary across studies, however, and apparent consistency exists in the literature only concerning the observation that working parents perceive that they have less available time compared with other parents (Roxburgh, 2012). Thus, it appears relevant to pursue the aim of this study: to explore whether a relationship exists between the time spent with children and willingness to medicate ADHD-like behaviors for working parents, while controlling for other probably relevant sociodemographic variables identified in the literature. If such a relationship were observed, this would warrant conducting more focused studies of the role of parental time in the complex genesis and management of children’s behavioral and emotional problems.
This study tests path analytic models to evaluate whether the amount of time that parents report spending with their children relates to their willingness to medicate ADHD-like behaviors and to estimate the strength of various sociodemographic factors on parental time and willingness to medicate. The conceptual model for this study is depicted in Figure 1. In the absence of any previous work on the subject, no specific hypothesis was formulated, although the researchers did expect that parents who are able to spend more time with their children would be less willing to medicate ADHD-like behaviors. Furthermore, it was expected that this relation would be stronger for parents reporting having a child with emotional and/or behavioral problems, because these parents’ answers were assumed to more closely reflect the attitudes of parents who find themselves within complicated dynamics involving teachers, doctors, and their children’s behaviors.
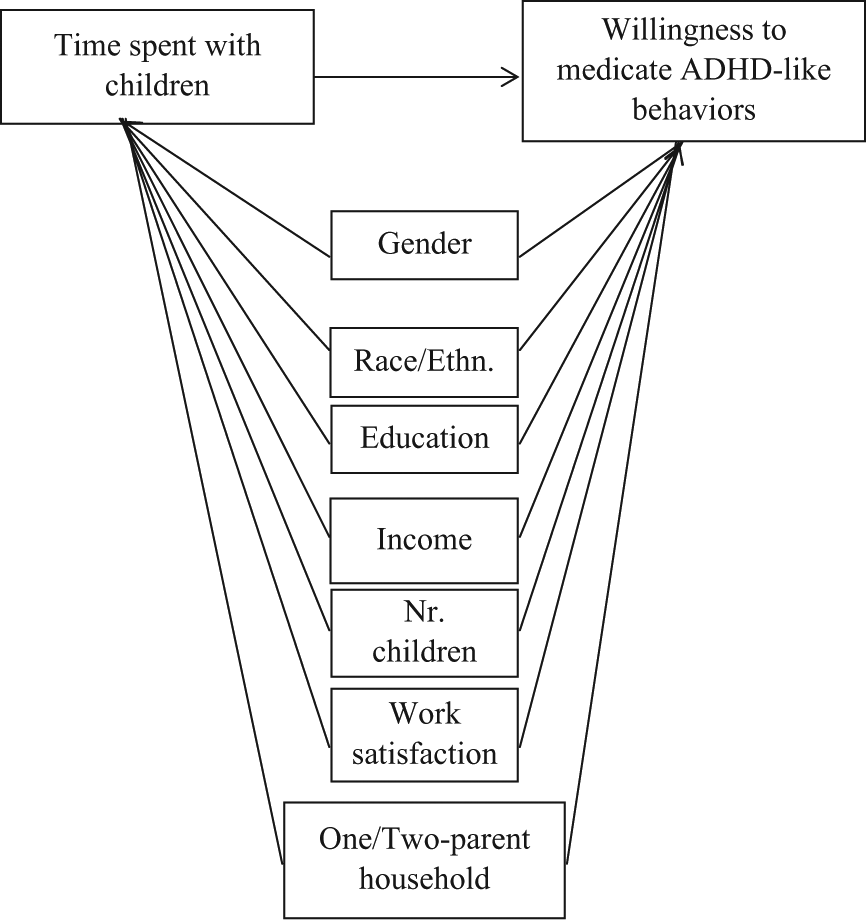
Conceptual model.
Method
This is an exploratory cross-sectional study. The data were gathered from parents of children 5 to 17 years, living in the adjacent Miami-Dade and Broward counties of South Florida and interviewed by telephone between May and October 2009 in a larger study of cultural factors influencing willingness to medicate children for emotional and behavioral problems. The sampling strategy in the original study was designed to select three similar-sized (n = ~400) groups of parents considering themselves African Americans or Black, Hispanics of any race, and non-Hispanic Whites. Complete details concerning sampling and data collection are reported by Cohen, Dillon, De La Rosa, and Gladwin (2013). The study was approved by the Office of Research Integrity of Florida International University.
Data Collection
A total of 35,311 randomly generated, potential landline telephone numbers in the two targeted counties were computer-dialed during most afternoons and early evening hours. The selection of participants occurred in a three-step process: excluding as many out-of-scope numbers as possible (e.g., nonexistent numbers, place of business, fax lines, n = 5,985), screening remaining possibly eligible numbers (e.g., no answer, answering machine, no child in household, immediate hang up, immediate refusal, n = 28,023) to identify qualifying households (n = 1,303), wherein 1,145 parents completed full interviews.
Among the 1,145 participants in the study, 763 reported working outside of their homes, and only these parents were queried concerning the time spent with children. From this latter group, the 496 parents with complete data on all nine variables included in the conceptual model were selected for the analysis (409 reporting having no child with problems and 87 having a child with problems).
Measures
Endogenous variable
The endogenous variable, willingness to medicate children, was measured with an item taken from the 1998 General Social Survey (GSS). Respondents were asked, “How likely would you be to give doctor-prescribed medication to your child or a child you were responsible for” if the child “is not paying attention in school, does not follow through with schoolwork or chores, has difficulty organizing activities, is easily distracted, talks excessively, and seems to run around and fidget constantly?” Possible answers ranged from “very likely” (scored 4) to “very unlikely” (scored 1).
Intervening variable
Time spent with children is an intervening variable in this study because it is simultaneously an exogenous and endogenous variable. The path analysis estimates the possible relationship of time spent with children on willingness to medicate and the possible effects of sociodemographic variables on time spent with children.
To measure the available time parents spent with their children, participants who indicated that they were employed were asked this open-ended question: “How many hours are you able to spend with your child or a child you are the caregiver of, during a regular workday?” Only two parents did not respond. Most gave a precise number or a range (e.g., “2 to 4 hr”) in which case the midpoint value was selected (e.g., 3 hr in the preceding example). Answers from 11 parents were removed because they could not be quantified (e.g., “with them constantly,” “during workdays none because I work the night shift,” “I am divorced and only see my children 3 times a week,” “not enough,” “all the time,” “as many hours as possible”). In addition, 108 respondents reported spending between 7.5 and 24 hr per day with their children. We considered it difficult to judge the accuracy of these answers (which were visible outliers in a boxplot graph) given the very low likelihood to work full-time outside one’s home and still manage to spend more than 7.5 hr per day with one’s child. Therefore, it was decided to exclude these 108 participants to minimize error.
Exogenous variables
Two questions measured race and ethnicity. The first asked participants, “With which of the following racial groups do you identify yourself: White, Black, Asian, American Indian, or something else?” The second question was, “Are you of Hispanic or Latino descent?” Combining both answers, the following categories were created: non-Hispanic White, Hispanic, and African American. Parents who could not be classified into these three categories (n = 55) were excluded.
The interviewers wrote down gender once a parent agreed to participate in the study. There were no missing answers on this variable.
For the variable of parent-type household, participants who reported being married, or not married but living together with a partner, were categorized as being in a “two-parent household,” and all others as being in a one-parent household. For this variable, eight parents had missing answers.
Education was measured by asking parents, “What is the highest level of education that you have completed?” Possible answers were categorized ranging from “grade school” (scored 1) to “graduate degree” (scored 6). Only one parent did not answer this question.
For the number of children in the household, parents were simply asked, “How many children younger than 18 live with you?” Their answers were grouped as none, one, two, three, and four or more (scored from 1 to 5, respectively). There were no missing answers for this variable.
Household income was measured by asking parents, “We don’t want to know your exact income, but would you tell me approximately what is your annual household income before taxes?” Answers were categorized ranging from “under $10,000” (scored 1) to “over $80,000” (scored 6). As expected, a substantial number (n = 126) of respondents chose not to provide an answer regarding their household income and were excluded from the path analyses.
Work satisfaction was measured by asking parents, “How satisfied are you with your current employment?” Answers could range from “very satisfied” (scored 4) to “very unsatisfied” (scored 1). Three respondents did not provide an answer.
Another important variable for this analysis was having a child with emotional and behavioral problems. Parents were asked, “Do you have any children with psychological, emotional, or behavioral problems?” This variable divided the two groups of parents in this study. Only three respondents did not provide an answer.
Data Analysis
Preliminary analyses were undertaken to check for linearity, normality, and homoscedasticity by means of bivariate scatterplots, boxplots, and simple frequencies. All the variables included in this model were linear and showed no problematic skewness or kurtosis. Once the dichotomous variables were coded, Pearson correlations could be calculated to check for possible confounding variables (Table 1). No correlation coefficient exceeded .49, suggesting independence and absence of collinearity.
Correlation Coefficients for all the Variables Included in the Study.
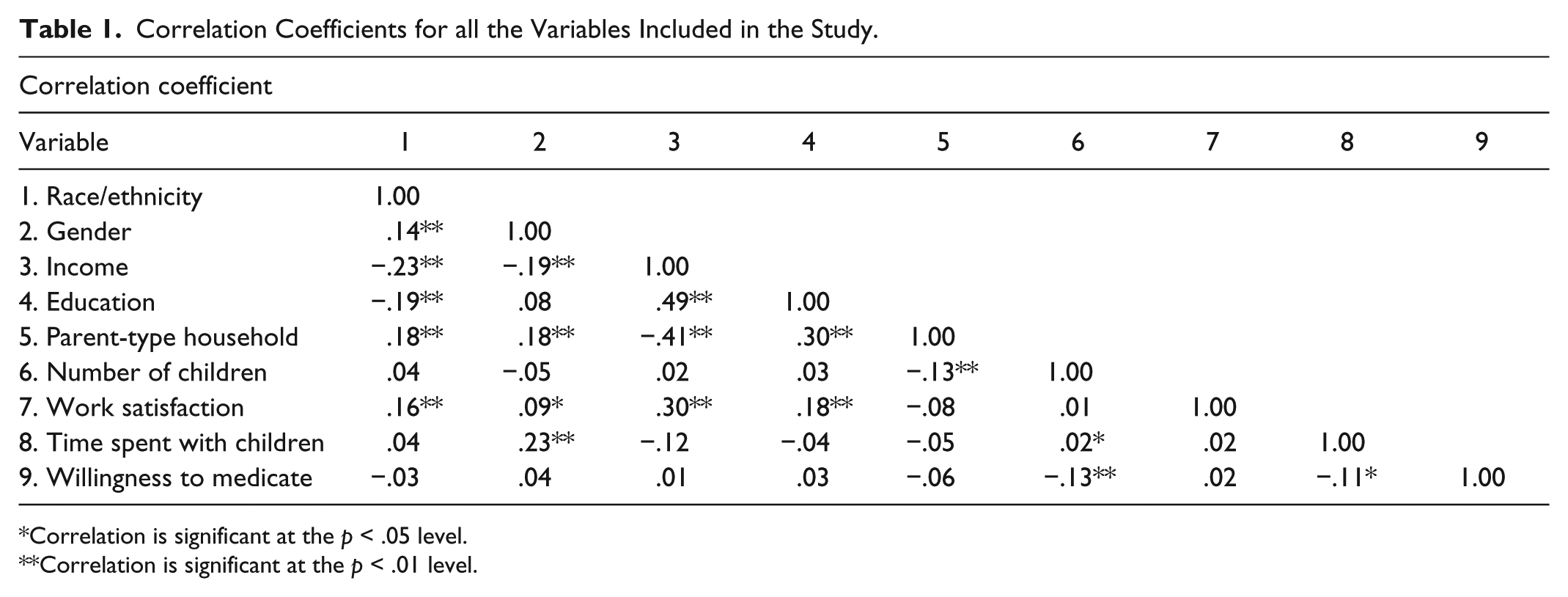
Correlation is significant at the p < .05 level.
Correlation is significant at the p < .01 level.
Categorical and dichotomous variables (race/ethnicity, gender, and parent-type household) were transformed into dummy variables, considered appropriate for this research design after a consideration of effect coding and contrast coding (Aguinis, 2004). Race/ethnicity was transformed into two dummy variables: African American parents were assigned a 1 and everyone else 0, and Hispanic parents were assigned a 1 and everyone else 0. Therefore, White parents were the comparison group for African American and Hispanic parents.
Two path analyses—one for parents reporting children with, and one for parents reporting children without problems—were conducted to estimate the effect of the intervening variable (parental time spent with children) on the endogenous variable (willingness to medicate ADHD-like behaviors). Each linear model estimated the direct and indirect effects of exogenous variables (gender, race/ethnicity, family income, family type, education, number of children per family, and work satisfaction) on the endogenous and the intervening variable. The path coefficients (β) represent the strengths of the linear relationships between pairs of variables with the effects of all other variables in the model held constant (Babbie, 2010).
Results
Table 2 presents distributions and mean scores where appropriate of all the variables in this study for each group of parents (with and without a child with problems). The distributions of most characteristics are similar for both groups of parents with the exception of race/ethnicity and willingness to medicate. Whites were over-represented, and African Americans strongly under-represented among parents who reported having a child with problems. In this latter group also, as was expected, 3 times as many respondents (27.6%) indicated that they were “very likely” to medicate ADHD-like behaviors as were other parents (8.6%).
Sociodemographic Characteristics and Willingness to Medicate of Parents Reporting Child With (n = 87) and Without (n = 409) Behavioral or Emotional Problems and Respective Chi-Squares and t Tests.

Significant (p value) of t test of difference of means between groups at p < .06.
Significant (p value) of χ2 test of independence at p < .05.
In both groups of working parents, approximately 57% spent between 3 and 5 hr per day with their children. An approximate average of spending 4 hr per day with one’s child was estimated for both groups (slightly higher for parents reporting no child with problems). The range of time spent was also quite similar for both groups (1 to 7.5 hr for parents reporting no child with problems, compared with 1 to 7 hr for parents reporting a child with problems).
Parents Reporting Having a Child With Problems
Tables 3 and 4 provides the unstandardized coefficients, standard errors, standardized coefficients, and confidence intervals of all the variables tested in both models. As shown in the upper portion of Figure 2, parents who indicated spending less time with their children were more willing to medicate (β = −.24; p < .02), and African Americans were less willing to medicate (β = .25; p < .05) ADHD-like behaviors. No other statistically significant paths were observed.
Standardized (β) and Unstandardized (B) Coefficients for Both Groups of Parents on Willingness to Medicate ADHD-Like Behaviors.
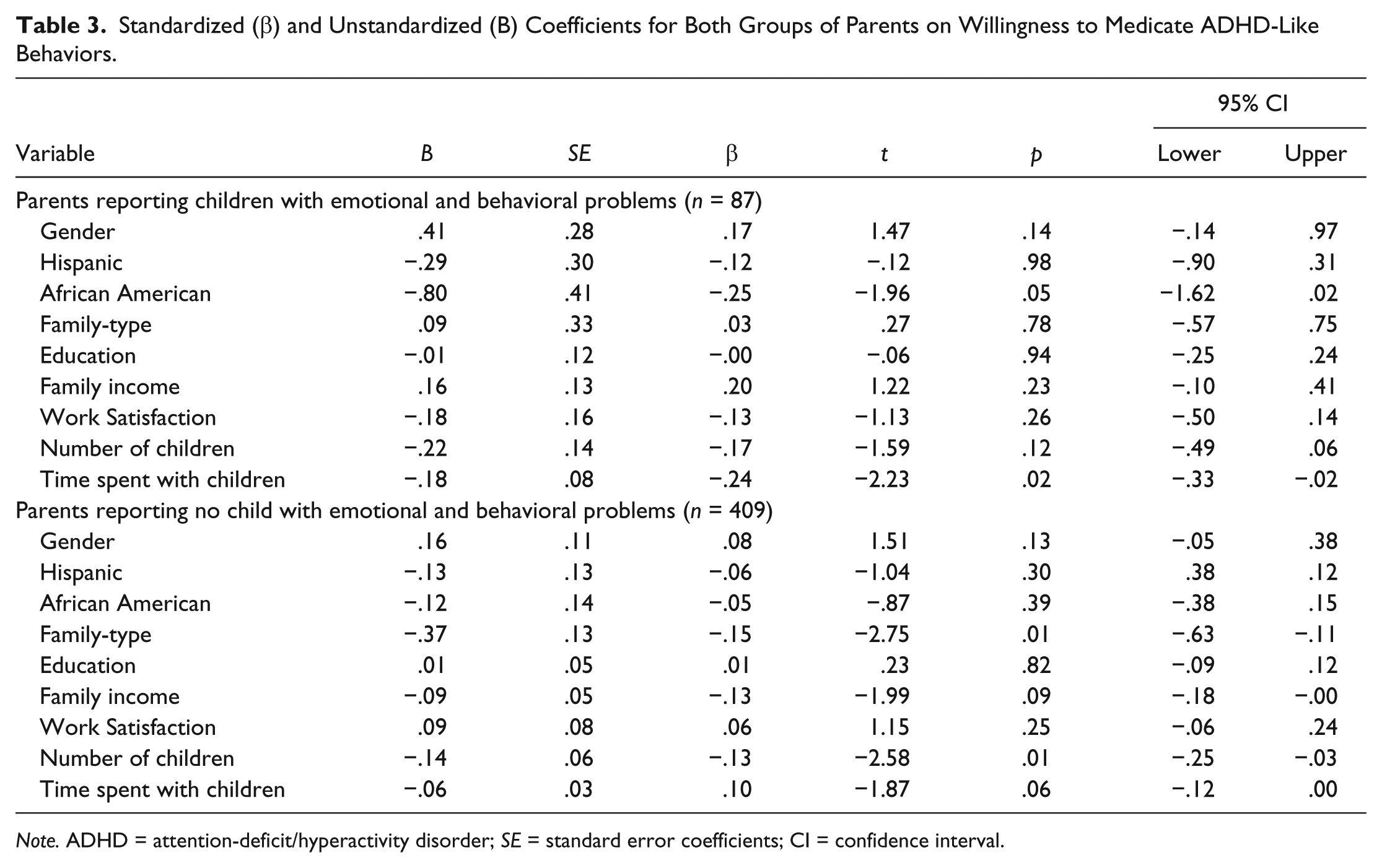
Note. ADHD = attention-deficit/hyperactivity disorder; SE = standard error coefficients; CI = confidence interval.
Standardized (β) and Unstandardized (B) Coefficients for Both Groups of Parents on Time Spent With Children.

Note. SE = standard error coefficients; CI = confidence interval.
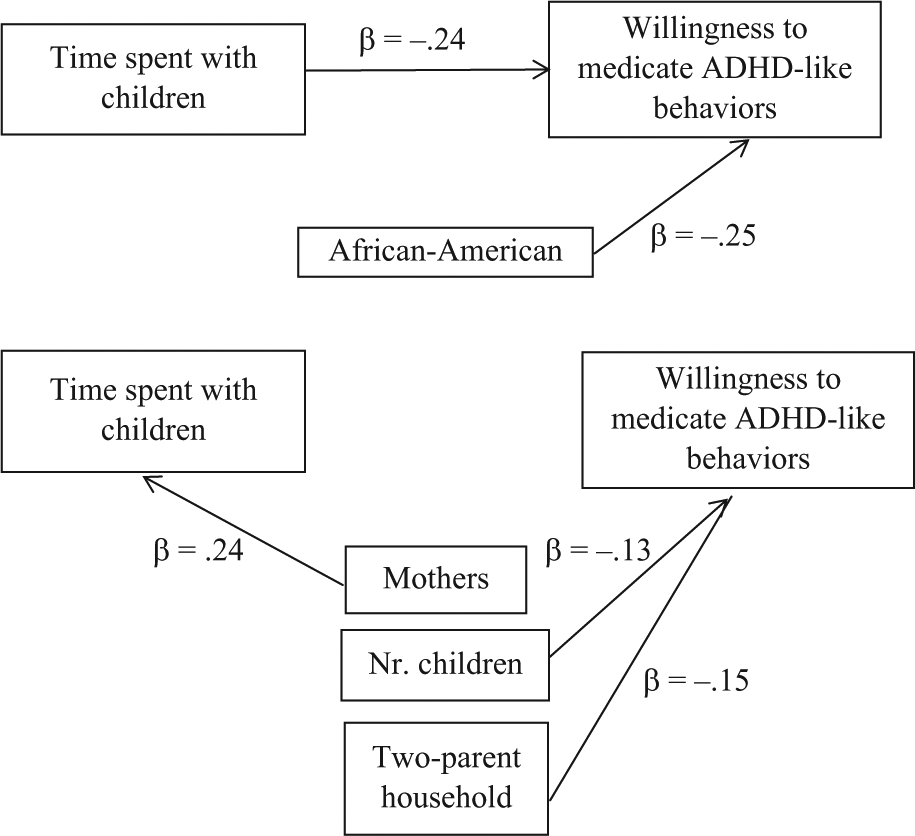
Statistically significant standardized path coefficients (β), from analyses of parents reporting child with problems (n = 87, upper) and parents reporting no child with problems (n = 409, lower).
Parents Reporting Having No Child With Problems
The significant paths among the variables in the analysis of the 409 parents reporting no child with problems are represented in the lower portion of Figure 2. Time spent with children is not related to willingness to medicate ADHD-like behaviors (β = .10; p < .06). This second model revealed three other significant relationships: (a) Mothers reported spending more time with children, (b) parents living in households with more children were less willing to medicate ADHD-like behaviors, and (c) single parents were less willing to medicate ADHD-like behaviors.
Discussion
To our knowledge, this is the first study that explores the possibility of a specific relationship between parental time spent with children and parents’ willingness to medicate children’s problematic behaviors. Spending more time with children and being African American independently decreased the likelihood of willingness to medicate ADHD-like behaviors for parents who reported having a child with problems. These relationships, however, were not replicated for parents who reported no child with problems. In that latter group, single parents and parents with more children were less willing to medicate ADHD-like behaviors, and mothers were more likely to spend more time with their children than fathers. The centrality of work outside the home in both these groups of parents’ lives is suggested by the fact that both groups reported spending nearly equal amounts of time with their children.
A major limitation of this study is its inability to establish cause–effect relationships between the two key variables of interest. The association observed between them may result from parents’ lack of available time or from a prior, independent willingness to medicate children’s ADHD-like behaviors, or from both. In addition, this study lacked measures of quality of time spent with children. Quality of time is an important subjective characteristic that may provide more valid indicators of the parents’ and their children’s relevant circumstances than quantity of time spent. Having indicators of quantity and quality of time—and from both parents in households, where relevant—would have strengthened this study’s internal validity.
In addition, 108 parents reported spending between 7.5 and 24 hr per day with their children during a regular workday. Although removed from the analyses, their answers suggest that these parents might have misunderstood the question (perhaps they included sleeping time or referred to the amount of time they wished they could spend with their children, etc.). Their answers raise the possibility that a misunderstanding might lurk in the answers of all respondents on this variable. Such internal validity issues should be clearly addressed in any subsequent work.
Race and Ethnicity and Willingness to Medicate
African American parents were less willing to medicate ADHD-like behaviors compared with White parents. This observed relationship accords with findings from studies that use parents of ADHD children as their primary informants (Pajo & Cohen, 2013). The finding may also indirectly accord with repeated observations that African American children are two and 3 times less likely than their White counterparts to receive psychoactive medications (Hudson, Miller, & Kirby, 2007; Zito, Safer, Zuckerman, Gardner, & Soeken, 2005). It appears important to examine the dynamics of race and ethnicity and medication of behaviors further to understand the reasons behind this observed difference. One possible explanation involves the complicated construct of “culture,” which is often used by society as a “conceptual short cut” to imply many different things (Mahler, 2012). There is nonetheless substantial agreement that culture comprises a learned and continually adjusted mindset that people use to make sense of the world around them. Cultural differences may or may not be apparent in ordinary events, but they may become salient or take priority when people are observed to face consequential situations, such as whether to diagnose a child with a mental disorder or to medicate that child to alter his or her behavior and emotions. As a group, African Americans appear to hold different health beliefs and treatment preferences (Jimenez, Bartels, Cardenas, Dhaliwal, & Alegria, 2012) and different beliefs concerning the nature of ADHD and the desirability of its drug treatment than the dominant White American majority (Bussing, Gary, Mills, & Garvan, 2003). Personal or “culturally available” attitudes may also interact with perceived or actual characteristics of the treatment system and providers. One study found that some barriers for treating African Americans diagnosed with obsessive compulsive disorder were stigma of mental illness, feeling no need for treatment, and believing that clinicians were unable to help (Williams, Domanico, Marques, Leblanc, & Turkheimer, 2012). Generally, the literature indicates that African Americans are less willing to seek medical help and are uncomfortable even when they do so (Griffith, Allen, & Gunter, 2011). All these factors, singly or in interaction, could contribute to African American parents’ reluctance to medicate ADHD-like behaviors among parents reporting that their children have emotional, psychological, or behavioral problems. Of note, the finding in this study that Black parents were less likely than other groups to report having a child with behavior or emotional problems accords with previously reported observations (e.g., Samaan, 2000).
Time Spent With Children and Willingness to Medicate
The present results suggest that spending less time with one’s children is related to being more willing to medicate children’s behaviors associated with ADHD—but only among parents reporting having a child with problems. Of note, such parents are more likely to have actually (and not merely hypothetically) contemplated the decision to medicate their children, and therefore, they more closely resemble “clinical” populations than other parents in the general population. This suggests that the observed relationship might well characterize many parents of ADHD-diagnosed children. In addition, this study showed that working parents reported spending similar amount of time with their children regardless of the presence of a child with emotional and behavioral problems.
Implications for Policy and Practice
Taking at face value the linear association between time spent with children and willingness to medicate them for ADHD-like behaviors, and considering that, in general, spending less time with children may have weighty consequences on children’s development (Hofferth & Sandberg, 2001; Leibowitz, 2003), one may ask whether quantity and quality of time spent with children influence the inception and the evolution of ADHD-like behaviors. Entertaining such possibilities bears directly on the well documented controversy about the nature of ADHD and about the use of medications to treat children’s problematic behaviors (Mayes, Bagwell, & Erkulwater, 2009; Zwi, Ramchandani, & Joughin, 2000). Despite the absence of studies exploring the relationship between parents’ available time and the start of ADHD-like difficulties in children, several studies, in varying locales, report distinct associations between adverse family and environmental circumstances and ADHD-like difficulties in children (e.g., Counts, Nigg, Stawicki, Rappley, & von Eye, 2005; Du Prell Carroll et al., 2012; Malek, Amiri, Sadegfard, Abdi, & Amini, 2012). DeGrandpre (2000) proposed that the major increase in the diagnosis of ADHD starting in the late 1980s was due in large part to the increase in the hurriedness of American society, where things are constantly happening at a faster speed. Although he does not specifically discuss time as a concept, he argues that citizens in post-modern societies are exposed to more stimulators in a shorter period of time than in the past. DeGrandpre implies that more performance is expected from people/children as everyone moves along in this hurried culture and also that psychostimulants enable some children to adjust to the brisk, aimless pace.
After several decades of prescribed stimulant use for ADHD-diagnosed children, the consensus in the literature is that such medicating usually alters behaviors temporarily or for the duration of the medicating, but often at the cost of consequential adverse effects, including depression, irritability, weight loss, and stunted growth (Poulton et al., 2013). A focused review of medication and behavioral therapy for ADHD by Halperin and Healey (2011) concludes that despite short-term behavioral changes, “the lack of normalization of functioning for many children following treatment, lack of generalization of treatment effects, difficulties in long-term adherence, and lack of clear improvement in long-term functioning following the use of these interventions are discouraging” (p. 625). Among the options for attempting to produce long-lasting or permanent changes of ADHD-like behaviors before considering temporary ones associated with excess morbidity in terms of adverse effects, increasing parents’ time spent with their children appears like a desirable focus of research and practice.
If spending time with children is associated with parents’ willingness to medicate behaviors, then its role in how parents perceive behaviors should also, it seems reasonable to suggest, become a focus of research. It is clear from the literature that parents are the main actors involved in the entire process of diagnosing and treating children, although practitioners may overlook how parents interpret children’s behaviors. Because of the subjective judgments required to apply ADHD diagnostic criteria, without a thorough investigation of each child’s specific context and circumstances the diagnosis may be misleading. For parents to have a good understanding of their children’s behaviors, it seems reasonable that they should spend time with them, observing them and interacting with them in a variety of circumstances and activities. Thus, when describing or rating their children’s behaviors to health care professionals, parents should probably also report how much time they spend with children and what type of activities they do together. Such information might need to be considered carefully to understand how caregivers arrive at specific judgments about the frequency or nature of their children’s behaviors.
Manifest and Latent Functions of Purposive Actions
Robert Merton’s theory of purposive actions offers one useful way to frame the issue of available parental time in relation to the decision to medicate children’s ADHD-like behaviors. Merton (1936) defined purposive action as involving motives and consequently a choice between alternatives (p. 895). In Social Theory and Social Structure, Merton (1957) defined motives behind human actions as manifest and latent functions. Manifest functions are “those objective consequences for a specified unit (person, subgroup, social, or cultural system), which contribute to its adjustment or adaptation and were so intended.” Latent functions “refer to unintended and unrecognized consequences of the same order” (p. 117). Merton (1936) had proposed that “it is necessary to ignore the manifest function in order to concentrate and become aware of the latent function—one needs to move beyond the perceived obvious to grasp the implications of the less obvious” (p. 890). Later, Merton (1957) emphasized that “finding the latent function of a practice which is not common knowledge, unrecognized, and unintended, is a greater increment in knowledge than findings concerning manifest functions” (p. 122).
Conclusion
In a sample of working parents, spending less time with one’s child during a typical workday was associated—among families reporting having a child with behavioral or emotional problems —with a greater willingness to medicate children for such problems. These findings might be interpreted in light of Merton’s distinction between manifest and latent functions of people’s actions and his recommendation to look beyond the obvious (manifest) functions. Looking beyond the manifest functions for medicating ADHD-diagnosed children (i.e., to improve the symptoms of an alleged neurobehavioral disorder that causes disruption in their cognitive and social functioning) might mean that parents of children who experience emotional and behavioral problems may (unintentionally) opt for psychiatric medications to cope with the (actual or perceived) limited available time they have to spend with their children. The findings of the present study provide moderate support for this interpretation. This specific hypothesis should be tested using robust measures of the quantity and the quality of time spent with children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.