
Abstract
To examine the environmental aspects in labor and delivery rooms (LDRs) in Saudi Arabia according to mothers’ points of view, especially with the recent increased numbers of C-section deliveries. The study is based on a survey questionnaire, open-ended questions analysis and comparison between the findings in two samples. Mothers who experienced labor and delivery in Saudi hospitals during the last 5 years participated in the study. The questionnaire was distributed via email and text messages to participating mothers, and 236 questionnaires were completed by participants. Based on analysis of the qualitative data, several factors were highlighted including Psychological aspects (39.74%), Caregiver attitude (15.89%), Space Layout and Furniture arrangement (12.58%). Importantly, from the quantitative analysis, the study finds that during COVID-19, compared to Pre-COVID-19 period there was an increase in mothers’ perceptions of the importance of the labor environment. The needs of mothers in Saudi were similar to those in the UK sample, except for these aspects that were important to Saudi women but not to those in the UK: spiritual support, psychological support, and policies. Therefore, designing labor and delivery settings should consider these cultural differences.
Plain language summary
The purpose of this study is to examine the environmental aspects in labor and delivery rooms (LDRs) in Saudi Arabia according to mothers’ points of view, especially with the recent increased numbers of C-section deliveries. The study is based on a survey questionnaire, open-ended questions analysis and comparison between the findings in two samples. Mothers who experienced labor and delivery in Saudi hospitals during the last 5 years participated in the study. The questionnaire was distributed via email and text messages to participating mothers, and 236 questionnaires were completed by participants. Based on analysis of the qualitative data, several factors were highlighted including Psycho-logical aspects, Caregiver attitude, space Layout and Furniture arrangement. Importantly, from the quantitative analysis, the study finds that during COVID-19, compared to Pre-COVID-19 period there was an increase in mothers’ perceptions of the importance of the labor environment. The needs of mothers in Saudi were similar to those in the UK sample, except for these aspects that were important to Saudi women but not to those in the UK: spiritual support, psychological support and policies. Therefore, designing labor and delivery settings should consider these cultural differences.
Keywords
Introduction
Studies conducted in many countries regarding the mothers’ labor experiences showed different results from one country to another (Baranowska et al., 2020); therefore, it was very important to investigate these environmental aspects within a Saudi context. The importance of giving birth in an environment that decreases stress and encourages physiologic birth (Baranowska et al., 2020) is highlighted in the studies of this context. During labor, women might feel pressured in an unfamiliar environment with surrounding equipment; most wish to give birth in an environment where it feels comfortable and calm (Boucher et al., 2009). In addition, mothers vary in their expectations and needs in regard to the birth environment. Therefore, birth centers can help in supporting physiologic birth by offering a suitable environment and supportive leadership for this purpose (Stark et al., 2016). Boerma et al. (2018) find that the rates of C-section (cesarean section) delivery in the UK have increased from 19.7% in 2000 to 26.2% in 2015, putting it among the highest in Western Europe for use of the procedure (Boerma et al., 2018). In Saudi Arabia, Al-Kadri et al. (2015) contend that the recent increase in C-sections procedures is possibly associated with the changes in physicians’ practice rather than a change in maternal aspects. An increase of 70% was found in C-section deliveries (Saleh et al., 2017).
Previous research has shown that supporting the mother continuously in her labor could shorten the labor process while decreasing the risk of an emergency C-section and increasing the chances of having a normal vaginal birth. In addition, women with continuous support during labor were more likely to have a positive birth experience (Hodnett et al., 2013; Larsson et al., 2017). However, additional studies are needed to explore the influence of elements and factors on the labor experience, such as the psychological aspects of birth (Cavalcante et al., 2021; Olza et al., 2020).
Literature Review
Evidence suggests that birth environment has a strong correlation to women’s satisfaction and labor experiences (Baranowska et al., 2020; Hodnett et al., 2013), therefore there is growing attention in investigating the effect of the physical environment and its influence on women’s birth experiences (Lorentzen et al., 2021).
Although the labor room is arranged to create safe care for mothers and their babies, criticism of these rooms included that they were designed to look too technological, giving the impression that childbirth is a branch of biomedicine rather than an aspect of health (Nilsson, 2014). In many situations, the design of labor and delivery rooms looks like other hospital wards; a bed in the center, surrounded with medical equipment and minimum privacy (Zwelling, 2010). One study explored the mothers’ perception of the most essential requirements in birth facilities. The main topics arising were: control, professional care, hospital safety, and support of the partner. The study also highlighted the value of the communication skills of midwives, such as listening and providing precise information (Pereda-Goikoetxea et al., 2019). Another study found that one of the main predictors of positive labor experience is being informed and receiving information (Baranowska et al., 2020). Other factors affecting women during labor were policies and routine practices related to the delivery rooms. For example, policies on walking and moving around and the presence of people supporting the mother, which might enhance outcomes for women and infants (Bohren et al., 2017).
In addition, both mothers and care providers noticed that offering comfortable, clean and relaxing labor environments with flexible visiting hours were effective in promoting the maternity care. In this study, mothers from different countries indicated the importance of access to medical and nonmedical tools, helping them to feel safe and encouraged (Shakibazadeh et al., 2018
There are many ways to support mothers during labor. For instance, understanding the role that endogenous oxytocin plays in the psychological and neuroendocrinological process during labor would benefit the mother and her partner (Olza et al., 2020). However, other studies showed negative effects on the birth experience appeared when giving birth with the use of pain relief medications such as epidural analgesia, and the occurrence of OASI (Johansson & Finnbogadóttir, 2019).
In addition, to help support physiologic birth, the environment must be soothing and stress-free (Stark et al., 2016). One study compared home-like to conventional institutional settings; the results of the study showed homely settings were related to advantages such as fewer medical interventions and higher maternal satisfaction (Hodnett et al., 2009). The study also showed that women who gave birth in modified settings reported that nurses spent more time with them than those in standard labor rooms (Hodnett et al., 2009). The labor room is not just a physical structure, it is also a culture, and the care providers’ philosophy, the presence of a doula, and the nurses’ dedication to providing support can impact this birth culture (Stark et al., 2016). One study was conducted in Pakistan; the mothers did not prefer giving birth at hospitals as they believe obstetric interventions are harmful to them. They mistrust the healthcare staff, which is a major factor that encourages them to give birth at home (Sultana et al., 2022).
Other useful techniques that were investigated in some studies are music therapy and breathing techniques; they were correlated with higher PPI (Positive Presence Index questionnaire scores) (Hunter, 2009). In general, mothers need both bound and unbound spaces to experience spatial security and safety. “Bound spaces” provide privacy, shelter and protection, such as the privacy needed in the shower or tub. “Unbound spaces” (Hunter, 2009, pp. 820–821) provide a feeling of freedom and openness. Therefore, if the birth environment is too bound or unbound, the women’s negative feelings such as stress might increase (Stenglin & Foureur, 2013).
Another study review summarizes the results of 22 trials involving 15,288 women, and reported that those who were allocated continuous one-to-one support were more likely to have a spontaneous vaginal birth and less likely to have intrapartum analgesia or report dissatisfaction (Hodnett et al., 2013).
One of the aspects affecting the labor experience is midwives. The central proposition of the theory of Birth Territory is that when midwives create and maintain maximum ideal environmental conditions, support is provided to the woman in labor and delivery, resulting in an increased likelihood of the woman giving birth under her own power, being more satisfied with the experience and adapting well in the postpartum period (Fahy & Parratt, 2006, p. 15). However, one study showed that half of the women who were interviewed about their birth experiences reported that midwives did not care for them, judging from their disregarding and humiliating behavior and actions. They were not prepared to fulfill the mothers’ wishes and expectations or to ease their suffering, but rather upset their sense of dignity by ignoring and disbelieving them, handling their body in a careless manner, and putting the blame on them (Eliasson et al., 2008, p. 508). In midwives’ and nurses’ care models, they should provide personal attention and continual, one-on-one labor support (Stark et al., 2016). Studies also emphasize the necessity for a new approach to care that understands the mother’s physiological and psychosocial needs, and promotes health and wellbeing (Smith et al., 2017; Olza et al., 2020).
In addition to the needs of studying the physiological and psychosocial demands of mothers during labor, the environment for birth requires greater consideration to enhance the challenges in obstetric practice, such as the increased number of interventions during labor and delivery. Yet limited research was conducted to investigate the impact of the design of the labor and delivery rooms (Lorentzen et al., 2021). Therefore, this study will investigate what the factors are that matter to mothers who delivered their babies in Saudi hospitals, and what are the differences in these preferences between the Saudi mothers and the UK mothers; the UK sample was reported in a previous study (Page & Singh, 2003). Investigating in the context of Saudi Arabia will fill the research gap on Saudi and Middle East context since this is one of the very first studies in this context.
Materials and Methods
To explore what design aspects of labor and delivery rooms mattered to mothers, the study carried out a survey called Better Birth Environment by National Childbirth Trust (NCT), UK in Saudi Arabia. The survey (Appendix 1) was developed to find out:
The elements of the physical environment that are important to mothers.
The sense of control mothers had over the environment during labor (Page & Singh, 2003).
The questions related to the topic of the study were chosen and translated to Arabic. These questions help to understand the labor experience of Saudi mothers. The survey was given to mothers who had given birth in a Saudi hospital during the last 5 years. The sample was collected via communicating with mothers through a number of gynecologists, and by sharing the survey with a description of the study in WhatsApp.
Inclusion criteria were mothers who gave birth in a Saudi hospital, during the last 5 years, and knew how to read Arabic. As for the exclusion criteria, these were mothers who did not deliver their babies in hospitals located in Saudi Arabia, and the delivery was not in the last 5 years.
A pilot was done based on the focus group of five mothers to test their understanding of the questions and if any modifications are required. All five participants provided feedback and understood all questions. However, they provided some feedback on the Arabic sentence structure of two questions. Therefore, the structure of the sentences of the two questions was modified based on their feedback, and their data were excluded.
The data collection was from 2018 to 2021, and the analysis was divided into pre-COVID-19 and post-COVID-19, as the pandemic impacted individual perceptions toward the environment and many other aspects of life. The participants rated environmental aspects in the survey using Likert scale, and answered open-ended questions. Based on the inclusion and exclusion criteria, this questionnaire was sent to 548 mothers in Saudi Arabia. Of the 548 mothers, 236 replied. All the questions were answered; however, some mothers didn’t fill in all the open-ended questions which were not mandatory for the participants. Hence, the response rate was 43.07%. There were 153 responses during the pre-COVID-19 period and 83 responded during COVID-19 (see also Table 6).
The quantitative questionnaire data were analyzed using SPSS. The qualitative data from the additional comments were analyzed using a thematic approach. In terms of research ethics, the ethical approval was granted to conduct the research. In the questionnaire, the respondents’ consent for using a questionnaire to collect data and their anonymity were assured.
There are some limitations associated with the questionnaire survey utilized in this study. For instance, non-responses may introduce biases to the results and findings. According to Alreck and Settle (2004), non-responses may present a serious problem in a study with a low response rate, for instance, below 10% of response rate. However, the effects of non-response biases are relatively small due to the higher response rate (43.07%) of this study.
Results
The results in Table 1 showed that hospital beds, en-suite bath, clean room, not be in sight of or overlooked by others, and homely looking room (not hospital-like) are the five highest important features of the physical environment during labor.
Importance of 25 Different Features of the Physical Environment during labor.
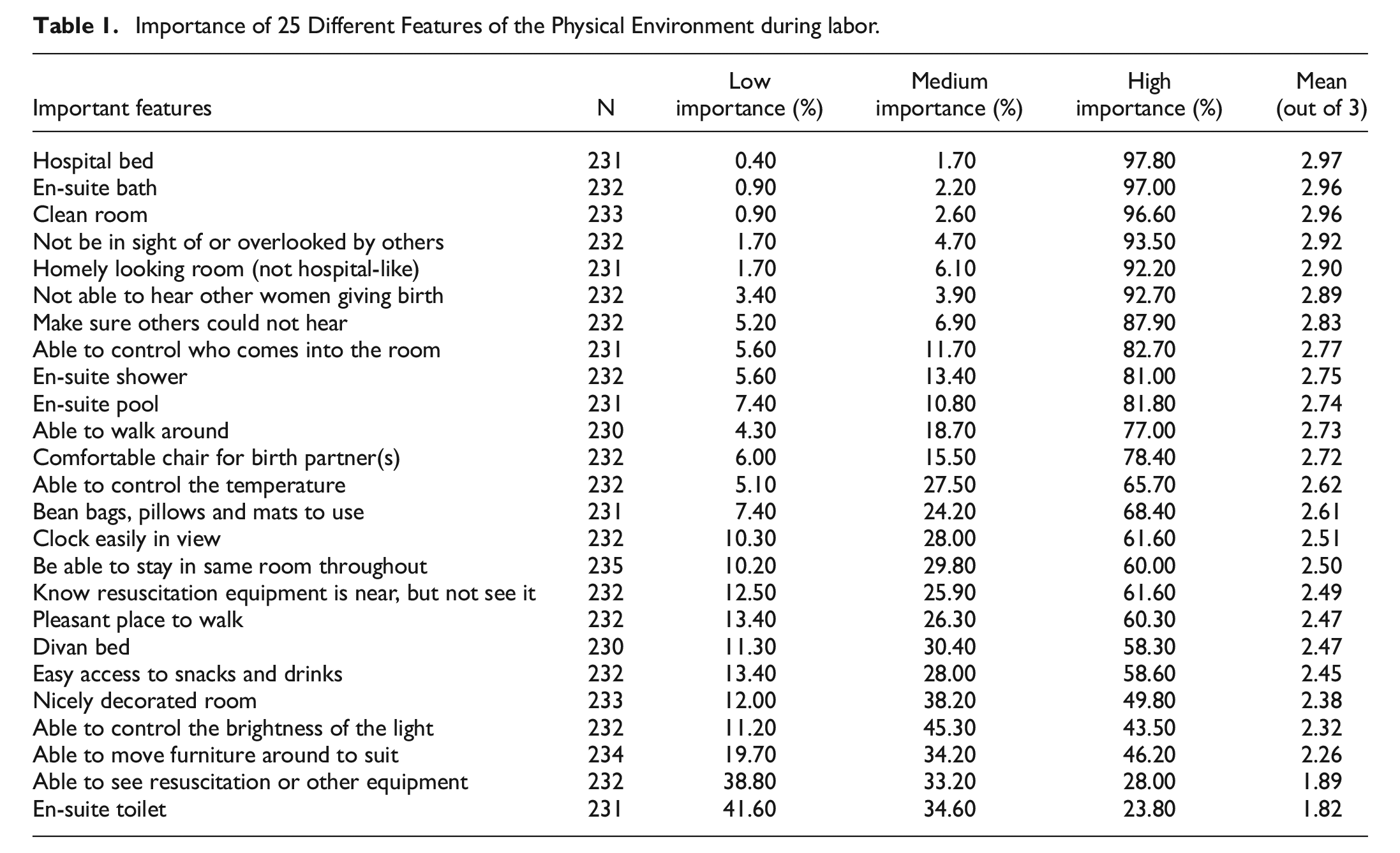
Table 2 shows the result of the comparison between the group of mothers who filled in the questionnaire prior and during COVID-19 in regards to the importance of different features of the physical environment during labor. The mean scores showed an overall increase in the rating of all the 25 features of the physical environment for those who answered during the COVID-19, except of the ability to control the temperature, divan bed, homely looking room, ability to see resuscitation or other equipment, which were slightly lower rated, and being sure others could not hear rating was the same prior and during the COVID-19 era.
Pre-COVID-19 and COVID-19 Mean Comparison Based on the Importance of Different Features of the Physical Environment During Labor.

All the participants in the study assessed the access to facilities during their last labor experiences (Table 3). This showed that half of the participants agreed that they had a clean room, easy access to a toilet, and a comfortable bed during their labor experiences. In addition, rooms that looked homely and easy access to a shower were rated highly as two facilities that were available to them.
Women’s Access to Facilities During Their Last Labor.

As for the qualitative analysis from the additional comments, the results showed several themes emerging from the mothers’ insights regarding LDRs. These include psychological aspects, such as social support and privacy; caregivers’ attitudes; space layout and furniture arrangement; interior space elements, such as lighting and ventilation; and spiritual support. Figure 1 and Table 4 show the ranking order for all the aspects that were discussed by the participants.

The effect of physical environment in birth.
Ranking Order of Features of LDRs.

The participants were asked if they thought the environment of the labor and delivery rooms could influence their labor experience and the reasons behind their answers. During the COVID-19 period, the mean score was 3.17 out of 4 and 3.15 before COVID-19 (see Table 9 also).
Overall, the participants listed a number of helpful aspects and elements in the labor rooms, including being in a private room “isolated from the rest of the hospital” [Interviewee 17].
As shown in Figure 2, 38.44% of the participants discussed certain concerns with the physical environment, 46% correlated the environmental effect to psychological aspects including social support, privacy, and tension. Twenty-four per cent discussed the caregivers’ attitudes, including their ability to communicate, and concluded that the staff, including doctors and nurses, required training in this aspect. Also, 10% discussed space layout and furniture arrangement as factors affecting their birth experiences, and 10% mentioned interior and décor as reasons for thinking that labor environment can affect their experiences.

Factors for an ideal physical environment for labor and or birth.
Several participants commented on religious and spiritual aspects. For instance, one participant said:
Some mothers have the capability to adapt easily to the physical environment and they believe that the only one who controls the easiness or the difficulty of labour is God. The second type of mother, maybe due to their young age or being spoiled in their families, expects to be spoiled during labour, and these days most women belong to the second type [Interviewee 5].
The spiritual support was discussed by a number of participants. Their suggestions included listening to the Quran or reading quotes from the Quran posted on the walls. One of the participants commented that it would be nice to have “a TV screen with a Quran channel on all through labor.”
Some comments were made about the availability of machines and equipment in the labor room, which made them feel safe. One of the questions (Q4) asked what you would include if you were designing a labor/birth room. Eighty-nine percent of the answers mentioned the importance of space layout and furniture arrangement, and 28% discussed the interior and décor. Also, there were comments about the size of the room, whether it was too small or too large, referring to the lack of space for accommodating their partners and guests. In addition, there were suggestions of providing a space for mothers to walk freely. One of the mothers described her ideas for LDR design:
The room would include a bed, a space for the baby close to the mother’s bed, and another bed for the partner. Also, a reasonable number of chairs for visitors around six, and a full bathroom inside the room [Interviewee 21].
Lighting and ventilation are also environmental topics that emerged in the participants’ discussion. One participant described the labor room that she would design as
A wide spacious room that is not too hot or too cold, with natural and artificial light and a view of trees, plants, and flowers or any natural view; also, the availability of a comfortable bed and all the devices I need for me or the baby [Interviewee 17].
In one of the questions (Q6), the participants were asked to list three physical aspects of the room in which they went into labor that they found most helpful for encouraging the type of birth they wanted.
The most highlighted factors were being in a spacious private room with (I) a comfortable bed, (II) a high level of hygiene, and (III) necessary medical equipment. Interior and décor, a pleasant view, and access to lighting and temperature control were also mentioned in the answers. Other factors that were emphasized, although they were not physical features, were caregivers’ attitudes and availability, policies related to the patient in the labor room, and spiritual support such as being able to hear or read the Quran. Overall, caregivers’ attitude and availability, hygiene, and a quiet private room (not shared) were the highest ranked factors in this question (see Tables 2 and 3).
As for privacy, a visual barrier was requested between the examining area and the guest area in the room: “a curtain to separate the bed from the guest space during the medical check.” It was also suggested to customize a gown to cover their bodies during labor.
A total of 166 reflections were observed from all the participants (Factor I—69 reflections, Factor II—5 reflections, Factor III—42 reflections; see Table 5). As for the analysis on the data collected in 2021 (during the COVID-19 pandemic), the comments in the qualitative section showed more concerns regarding the importance of labor and delivery rooms and how these rooms were designed. For instance, [Interviewee 193] stated that “A good environment helps to facilitate labor, in contrast, an organized environment caused pressure and reflects negatively on the labor process and the mother’s psychology.”
Three Factors Ranked in Order of Importance in Encouraging the Motheramp#x02019;s Preferred Birth Type.

Interviewee 189 highlighted the importance of the labor environment “Because when I enter a soothing quiet environment with full audio privacy, it prepares the person that all will be easy. Not, however, an isolated room with unpleasant colors and arrangements, which will cause fear and panic and will result in a high degree of stress among the women.”
Interviewee 155 said “When you are in pain and going through labour while looking at trees and water fountains, this will be different than being in pain and facing a blue curtain in a dark room that is so depressing.”
The participants from the sample that was collected during the COVID-19 pandemic, gave a number of suggestions regarding the design of the labor room. These suggestions included (see Table 5):
- Spiritual support including the availability of speakers to listen to the Quran, or the Quran on the TV, as well as providing a prayer mat for the partner.
- Well-designed spaces for walking other than the hospital hallways.
- Pleasant view of nature and greenery, such as trees, flowers, and water features.
- Tools and equipment to facilitate the desired mode of labor such as birthing balls, yoga fabrics, chairs etc.
- Appropriate space for the partner including bed and seating.
- A comfortable bed, that stays with the mother post-delivery.
- A large window for daylight and ventilation.
In regard to helpful environmental factors within the labor and delivery room from their last birth experiences, Table 6 shows that the mothers mentioned the following as important factors that encourage the mother’s preferred birth type from the samples:
- Caregiver attitude and availability in the labor room.
- Spacious and Comfortable Room
- Private quiet room
- Clean room (Hygiene)
- Availability of equipment
Combined Factors Ranked in Order of Importance in Encouraging the Mother’s Preferred Birth Type.

A total of 98 reflections were observed from all participants (Factor I—46 reflections, Factor II—29 reflections, Factor III—42 reflections; see Table 7). The last question concerned the elements of the labor room that participants found not encouraging to the type of birth they wanted (see Tables 7 and 8)
- Caregiver attitude, such as not allowing them to use the furniture they needed for a comfortable labor.
- Space layout that is not convenient to the mothers’ needs.
- Lack of privacy, especially when the room or the toilet is shared with other patients.
- Furniture that is not adequate to the mothers’ needs, such as a lack of furniture for the family and partners.
Three Factors Ranked in Order of Importance in Failing to Encourage Mother’s Preferred Birth Type.

Combined Factors Ranked in Order of Importance in Failing to Encourage Mother’s Preferred Birth Type.

In addition, from the qualitative analysis two themes emerged revolving around spiritual support: hearing the Quran [Interviewees 26, 27, 161, 170, 231] and policy-related factors: suggestions to enhance privacy such as “to have a curtain to separate the bed from the guest space in case I need a medical check when they are in the room” [Interviewee 8] and “providing a specifically designed gown to cover me during labour” [Interviewee 9]. Additionally, participants suggested having family members with them during labor to support them socially, which is not allowed in some medical centers. Also, they suggested allowing them to take their mobile phones with them during the labor. Visiting hours were also discussed in the comments; one participant said “visiting hours and mealtimes should be different for the mothers than for other patients” [Interviewee 7]. Policies regarding doctor’s visits were also mentioned, the number of medical check-ups: “every 15 minutes is too much and prevents me getting rest” [Interviewee 3]. In contrast, caregivers’ attitudes and availability were mentioned as a helpful factor, for example, facilitating communicating with nurses using the help button [Interviewee 12].
Some unhelpful aspects in the labor room were too much furniture, too much noise and being able to hear other women screaming [Interviewee 6], sharing the room with other patients [Interviewees 8, 6], an uncomfortable bed and a lack of supportive elements such as birth balls and pools. Another factor was being in too small a room to offer any comfortable place for the partner.
The caregivers’ attitude was mentioned repeatedly as unhelpful; “the midwife was not available to help when needed” [Interviewee 11], “bad attitude from the medical staff” [Interviewee 7], “no nurses around me and my baby” [Interviewee 3], and “talking in a loud voice” [Interviewee 10]. Further, “supporting and encouraging the patient, and a good reception for the patient are needed” [Interviewee 8]. The availability of equipment was also discussed, including a lack of resources [Interviewee 15], a broken contractions monitor [Interviewee 12], and the mother’s experience of being attached to the monitor all the time [Interviewee 1].
Impact of COVID-19
According to Cavalcante et al. (2021, p. 1), “COVID-19 is more common among reproductive-age young adults than in older adults.” However, the existing information on COVID-19′s impact on pregnant women is still insufficient globally, including with regard to Saudi Arabia. According to the Saudi Ministry of Health, “there is limited data available on COVID-19 during pregnancy that suggest an increased risk of miscarriage or preterm birth if a pregnant woman is infected with COVID-19.”
There were 153 responses for the pre-COVID years and 83 responses during the COVID-19 period (see Table 6). The comparison between the two samples showed a slight increase in the perception of mothers in regard to the importance of the labor environment in both quantitative and qualitative analysis for the sample during COVID-19 (3.17 During the COVID-19 period and 3.15 in the Pre-COVID-19 years). It means that what people have been through during the COVID-19 pandemic including lockdown, social distancing, hygiene precautions might impact the mothers’ perceptions and they strongly believed that the labor environment has an impact on their labor experiences more than before (see Tables 9–12).
Group Statistics on Mothers’ Perceptions on Whether the Environment Is Important or Not.

Independent Samples Test.

Independent Samples Effect Sizes.
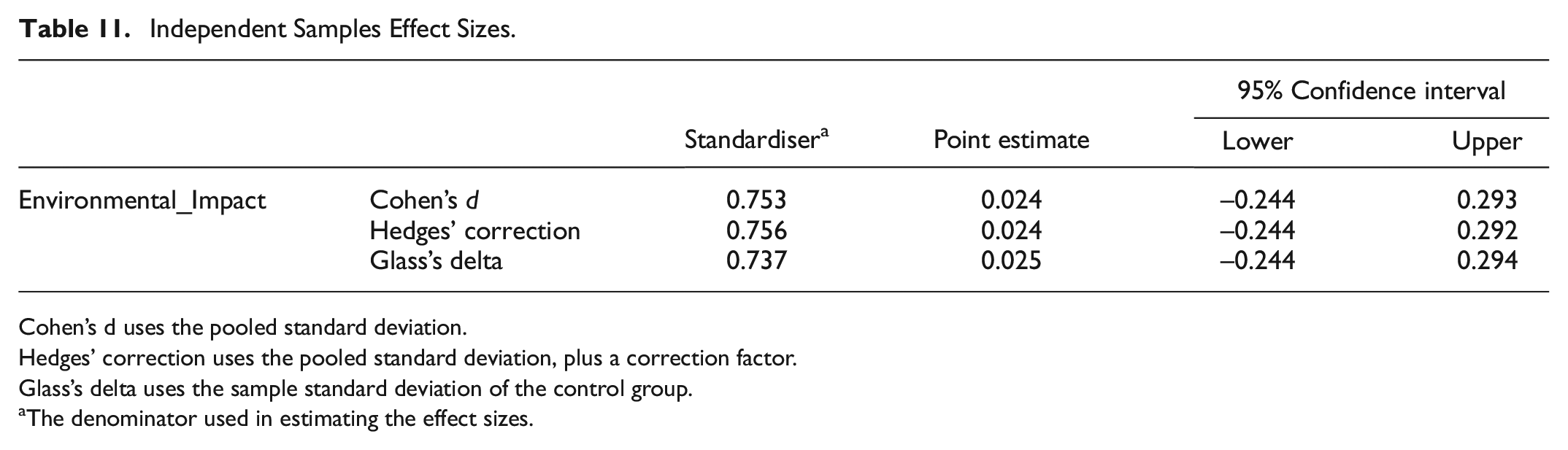
Cohen’s d uses the pooled standard deviation.
Hedges’ correction uses the pooled standard deviation, plus a correction factor.
Glass’s delta uses the sample standard deviation of the control group.
The denominator used in estimating the effect sizes.
Bayesian ANOVA.

Dependent Variable: Environmental_Impact.
Model: YEAR.
Assume standard reference priors.

Assume standard reference priors.
Discussion and Conclusions
Based on the quantitative survey analysis, the results of the study showed some differences in the rank of the environmental aspects among the Saudi sample and the UK one. The results suggest greater difference on LDR between Saudi Arabia and the UK. This calls for policymakers to adjust policies regarding labor and delivery environment and facilities. The highest rate goes to hospital bed, en-suite bath, clean room, not being in sight of or overlooked by others as the most important aspects in the 25 listed ones, while the UK sample listed having control over the brightness of the light and the temperature of the room, being in a room that looked homely, having an en-suite bath, and having easy access to food and beverages (Page & Singh, 2003). Such differences were documented in the literature, as the way these labor rooms are designed differ and mothers’ perceptions are also varied among cultures. For instance, Baranowska et al. (2020) discussed the differences in satisfaction with care during birth experiences among a sample from Poland in comparison to Sweden (Baranowska et al., 2020).
The results from Saudi data showed the highest-rated facilities for women during their last labor were: clean room, easy access to a toilet, comfortable bed, room that looked homely, and easy access to a shower (see Table 3). However, the sample from UK data showed that the highest-rated facilities for women during their last labor were: clean room, privacy and not in sight to others, being able to walk around, able to stay in the same room, having a comfortable chair for their partner, easy access to a toilet (Page & Singh, 2003). These differences were also supported by the qualitative findings as reported in Tables 5 to 8. The mothers from Saudi emphasized having more privacy, and nicely designed places to walk.
Based on the qualitative analysis from the additional comments, the helpful aspects in the Saudi sample were caregiver attitude and availability, spacious and comfortable room, private quiet room, clean room and hygiene, and availability of equipment to encourage mother’s preferred birth type (see Table 6). On the other hand, the UK sample shows that the most helpful aspects were space for movement and walking around, a birthing pool or a large bath, en-suite bathroom, a comfortable, adjustable bed, adjustable lighting, privacy and a quiet room (Page & Singh, 2003). This comparison will be beneficial if healthcare providers take them into account when designing labor and delivery centers. For instance, the Saudi sample highlighted the need for well-designed spaces for a walk, which seems the first-rated helpful element for the sample from the UK.
Based on mothers’ perceptions in Saudi, the not helpful aspects during the birth included caregiver attitude in supporting mothers, space layout, a lack of privacy, and furniture that assists different labor modes (see Table 8). The UK samples show a small room with little space to move around, clinical atmosphere in rooms, an uncomfortable bed, lack of privacy, and a toilet outside the room (Nilsson, 2014). Both samples frequently emphasized the need of the availability of a comfortable, adjustable bed that is also movable and stays with the mother for the whole admission time. This can be one direction for future research in this field, from the ergonomic side.
Overall, studies documented the positive impact on women’s experiences when providing a comfortable labor environment (Baranowska et al., 2020; Stark et al., 2016; Stenglin & Foureur, 2013; Foureur et al., 2010). Privacy, freedom from distracting noises, and freedom of movement and position changes gave the required comfort and reduced stress (Walker et al., 2014; Foureur et al., 2010); Baranowska et al., 2020; Stenglin & Foureur, 2013). One of the aspects highlighted by the participants was the need to be in a single room, not shared by other patients, and having the freedom to walk. A single room allowed the mother and her family to stay in one space from the time of admission to discharge. These results are similar to other studies that found mothers listed respect and privacy as crucial elements for a positive childbirth experience (Baranowska et al., 2020). The rooms are designed to be homely with additional privacy and the required freedom to achieve a physiologic labor (Stark et al., 2016). A telemetry that allowed mothers to walk and move more freely, and waterproof telemetry that allowed for showering and hydrotherapy (Hodnett, 2002; Hodnett et al., 2013).
It was suggested to have a space in the room for the new-born, as birth centers keep the new-borns in the nursery most of the time. According to Zwelling and Phillips, ideally, the new-born should be with the mother all the time after birth, and one caregiver for the mother and new-born (Zwelling, 2010). Other recent studies discussed the benefits of caregivers’ availability, their attitude and the continuous support of women during the delivery experience (Hodnett, 2002; Hodnett et al., 2013; Stark et al., 2016). Part of the support from caregivers is to be able to know what is available and how to use these comfort measures (Stark et al., 2016). It is very important for the mother to feel that midwives share similar philosophy about childbirth (Hunter, 2009).
Participants suggested providing a supportive environment to encourage natural labor such as pillows, pools and birthing chairs. Birth centers offer facilities that may contribute to physiologic childbirth such as: birthing stool and ball, a birth bath and shower, and personal support from a maternity care assistant. However, the use of these facilities depends on other factors such as the mother and her partner’s perception of childbirth and expectations (Hermus, Boesveld et al., 2017).
In Hermus, Hitzert et al.’s (2017) study, which was conducted in the Netherlands, 74% of participants’ birth centers achieved a homelier environment in contrast with conventional birthing rooms within obstetric units. In this present study, 44% wanted a more efficient space layout and furniture arrangement, and 14% wanted to see elements related to interior and décor such as pleasant wall coloring and access to a calming view, in addition to other physical elements such as lighting and ventilation.
Social support, including the partner and other family members attending the labor, was one of the highlighted aspects, in addition to allocating a space or bed for the partner in the room. Previous studies showed that mothers who had a companion to support them during labor had a positive effect, such as fewer complications during birth and less postpartum depression (Gjerdingen et al., 1991; Maimbolwa et al. (2001). Researchers also developed instruments to measure social support due to its important impact on policy makers and health planners, such as BCSQ (Dunne et al., 2014).
Research shows emerging evidence on the low levels of social support and the increase of PTB (preterm birth) risk among high-stress women. Additional studies on the effect on women who are experiencing high levels of stress should be considered, to help decision makers developing and implementing social support programs (Hetherington et al., 2015).
According to Bélanger-Lévesque et al. (2014), fathers can feel isolated from the delivery experience, whether by the partner or the care providers. Also, in one study, the social support affected women’s decisions in choosing a home environment to deliver their babies, as they feel greater emotional support from their families and midwives which increases their feelings of security and empowerment (Sultana et al., 2022). Therefore, taking into consideration both the mother and father’s birth experiences, it is very important to deliver the needed support surrounding the birth. Social support can be also provided by the doulas, their role includes encouraging and assisting the mother in positive communication with the caregivers and with the mother’s partner (Arnold, 2001).
In addition, spiritual support was one of the factors highlighted by the Saudi sample. This support included the availability of speakers to listen to the Quran, or the Quran on TV, as well as providing a prayer mat for the partner.
This finding is similar to Callister and Khalaf’s (2010) results; childbirth is one of the best settings to acknowledge the spiritual aspect of mothers. Most of the women in Callister & Khalaf’s study considered childbirth as a spiritual experience; this theme was identified in all the reviewed data. Likewise, the spirituality of Muslim mothers makes the birth experience sacred; they described how rituals, such as prayer, served as helpful coping mechanisms during labor (Callister & Khalaf, 2010).
Another study showed that mothers during labor perceived the spiritual forces as the third most valuable caring behaviors, while midwives and nurses considered it one of the least important behaviors (Al-Maharma et al., 2021). Therefore, understanding the spiritual aspects of women helps to establish new women-centered norms in spiritual and health practices, and support the healthcare experience holistically (Lauver, 2000).
One of the suggestions in regard to the design of the labor rooms was enhancing the lighting. In contemporary room design, consideration is given to types of lighting, the reduction of noise, and privacy (Phillips & Fenwick, 2000; Stark et al., 2016). Keeping the door of the room closed, maintaining dim lighting in the room, playing music, using comforting items from home and keeping visitors to a minimum contribute to a calm, quiet atmosphere (Baranowska et al., 2020).
To support physiologic birth, women in labor should be given oral fluids and light food low in acid, sugar, and salt so as not to slow gastric emptying (Walker et al., 2014; Goer & Romano, 2012). The mothers in this study frequently mentioned that food and beverages were not available when needed. This is similar to what was mentioned in the study of Stark et al. (2016); the availability of food and fluids in hospitals and birth centers is limited, and nurses should support the mothers by providing fluids and foods that are needed for hydration and nutrition.
Mothers in this study discussed the importance of caring nurses and medical staff to encourage them during the labor experience. This supports what is found in literature, according to Nilsson’s study (2014) and, women in delivery rooms must be offered not only medical, but also emotional and existential safety, and nurses’ support during all stages of the labor can support physiologic birth (Stark et al., 2016). They also need to be involved in decision-making and given the opportunity to express themselves based on received information (Baranowska et al., 2020). In contrast, mothers disliked midwives who showed uncaring attitudes, treated them in a dehumanizing way, leaving them feeling invisible and that they lacked control (Eliasson et al., 2008; Elmir et al., 2010; Nilsson, 2014).
Birth philosophy and the configuration, size and shape of the birth room need additional investigation and research (Setola et al., 2019). Effective support of mothers during labor is influenced by many factors, including routine practices and policies related to the birth environment. The policies in regard to freedom to move and the presence of people to support mothers may enhance outcomes for women and infants, including increased spontaneous vaginal birth, shorter duration of labor, fewer cesarean births, less use of any analgesia, a low 5-minute Apgar score and fewer negative feelings about the childbirth experience (Bohren et al., 2017). This request was discussed by the participants in this study. They suggested many changes in the birth centers’ policies, including changing the visiting hours, allowing the mother to keep her mobile phone during all stages of labor, and access to food and beverages.
Footnotes
Appendix 1: The Study Questionnaire
Acknowledgements
The author thanks the participants for their involvement in the study.
Author Contributions
R.A. is the sole author of the article. R.A. contributed to “Conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing—original draft preparation, and review and editing.”
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
This study was approved by an Institutional Review Board IRB-2018-10-002.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data will be available based upon the request.