
Abstract
Early-life adversity (ELA) and recent stress experiences are relevant explanatory factors in the understanding of health differences across the life span. However, their particular role in explaining the vast health heterogeneity in older adulthood has yet to be defined. To address this gap, this study examined (a) the health of older individuals with differing levels of ELA and recent stressful experiences; and (b) the type (i.e., linear, curvilinear) of the expected stress-health relationships. Longitudinal quantitative data were collected on health, ELA, and stressful life experiences of the previous 21 months in N = 216 participants (Mage = 69.8 years, 45.8% female). Findings support linear (rather than curvilinear) stress-health relationships for ELA and recent stress with physical and mental health. Furthermore, ELA significantly moderated the relationship between recent stress and physical illnesses. As the detrimental health impact of ELA can still be detected in older adulthood, ELA may be critical for understanding later life health heterogeneity.
Plain language summary
Older age is characterised by its vast disparity in health. There exists a wide array of empirical literature on factors linked to this health disparity. While differing levels of early-life adversity (ELA) and recent stress are potentially explanatory factors, their role in later life is insufficiently understood. This study examined the health disparity of older individuals with differing levels of ELA and recent stressful experiences, as well as the type of the expected stress-health relationships. More specifically, this study examined, whether the relationships between stress and health follow a linear or a curvilinear fashion. A longitudinal quantitative study has been conducted in Switzerland to collected data on health, ELA, and stressful life experiences of the previous 21 months in 216 participants. The participants had a mean age of 69.8 years and were 45.8% female. The findings of this study support linear (rather than curvilinear) stress-health relationships for ELA and recent stress with physical and mental health. Furthermore, ELA significantly acted as a moderator in the relationship between recent stress and physical illnesses. As the detrimental health impact of ELA can still be detected in older adulthood, ELA may be critical for understanding later life health heterogeneity.
Keywords
Introduction
To understand interindividual differences in health, the previous stress experiences of an individual must be considered. However, the majority of the existing studies examining stress-health relationships have only applied linear models in young to middle-aged participants. Potential curvilinear stress-health relationships have received substantially less research attention, particularly in studies with older individuals. Therefore, this study set out to examine the current health of Swiss older adults with differing levels of early-life adversity (ELA) and recent stressful life experiences; and to investigate the type (i.e., linear or curvilinear) of these stress-health relationships.
Older age is characterized by vast interindividual health differences (e.g., Nguyen et al., 2021). This suggests that chronological age alone does not sufficiently explain the health heterogeneity in later life (Lowsky et al., 2014). A broad set of factors has previously been examined to deepen the understanding of this wide health disparity in later life, and in particular, to better apprehend more favorable health outcomes in older age. This line of research has revealed various factors related to better health in later life, including health-related behaviors (e.g., non-smoking, higher level of physical activity), as well as higher socio-economic status (SES), and education (e.g., Hodge et al., 2013).
The majority of factors that have previously been linked to better health outcomes in later life have also been shown to be negatively impacted by stress. For instance, regarding early-life stress, a recent Swiss study with older survivors of ELA (e.g., physical abuse, emotional neglect) found that survivors smoke more often, have a lower (satisfaction with their) SES, and show lower levels of educational achievement in comparison to age-matched controls ((Thoma et al., 2021).With regard to recent stressful life events, research has shown that higher levels of stress are linked worse health outcomes via various affective, behavioral, and physiological pathways, which can impact health-related factors (Cohen et al., 2019). Such studies suggest that the previous stress experiences of an individual must be considered in order to better understand the vast health disparity observed in older adults.
In the investigation of stress-health relationships, the (implicitly) expected relationship follows a linear, dose-response pattern (i.e., the more stress, the worse the outcome). Such assumptions derive from theoretical stress models, such as the Vulnerability- (or Diathesis-) Stress Model (Adler, 2009; Engel, 1977). However, on the basis of the more recently proposed Steeling Effect Theory (Liu, 2015; Rutter, 2012), non-linear (i.e., curvilinear) stress-health relationships could also be expected. While there is a large body of empirical support for the existence of linear, dose-response stress-health relationships; an increasing number of studies are providing evidence for non-linear relationships between various stress indices and health outcomes (for a review see Höltge et al., 2018). However, the assessment of the type of stress-health relationship (i.e., linear, curvilinear) has been neglected in older age groups. Given the increasing number of individuals reaching the maximum life span across the world (World Health Organization [WHO], 2021), it is essential to identify relevant stress(-ors) and examine their relationship with (better) health outcomes in later life.
It is therefore the aim of this study to examine the health disparity of older individuals with differing levels of ELA and recent stressful life experiences. The type of stress-health relationships will be examined from the perspective of different stress models. On the basis of the Vulnerability- (or Diathesis-) Stress Model (Adler, 2009; Engel, 1977), and the extensive body of research in support of dose-response relationships between stress and health; linear, rather than curvilinear relationships are expected between ELA and physical and mental health (hypothesis 1a), as well as between recent stressful life experiences and physical and mental health (hypothesis 1b). Based on the (expanded) Stress Sensitization Model (Hammen et al., 2000), it is further expected that ELA will moderate the relationship between recent stressful life experiences and physical and mental health (hypothesis 2).
Methods
Participants and Procedure
Half of the participants (risk group, RG) were older adults who were formerly affected by compulsory social measures and placements (CSMP) as a minor in Switzerland up to 1981 (see Federal Office of Justice, 2021). These individuals were at high risk to have experienced child abuse and neglect (Leuenberger & Seglias, 2008). The other half of the participants were age-matched, non-affected individuals (control group, CG). For the purpose of the analyses, these two sub-groups were collapsed into one group to ensure the largest possible variation of adversity within one sample, which is necessary in the investigation of the steeling effect (i.e., curvilinear relationships) (Höltge et al., 2021; Seery et al., 2010). Inclusion criteria were language (i.e., native Swiss German), age (i.e., 50 years or older), and for the RG only, having been affected by CSMP for a minimum of 1 year before age 18.
This prospective, longitudinal study consisted of a baseline and follow-up quantitative assessment, conducted at the University of Zurich, Switzerland. The study procedure has been extensively described in Thoma et al. (2021) and is briefly summarized in the following: Two baseline (A1, A2) and two follow-up assessments (A3, A4) were conducted 21 months apart, each including a face-to-face clinical interview and a broad set of questionnaires that were completed by participants before, during, and after each assessment. Each baseline (July to December 2019) and follow-up (May to October 2021) assessment lasted for no longer than 2 hr. At 3 month intervals between the baseline and follow-up assessments, brief phone interviews (lasting between 15 and 30 min) were conducted with participants to assess their current health and stress (data not reported here). For the complete study participation, participants received 480 Swiss Francs (approximately $500 US dollars). The study was approved by the Ethics Committee of the Faculty of Arts and Social Sciences in the University of Zurich (ID: 19.4.3; ID: 20.12.24). Written informed consent was provided by all participants.
Measures
The following data was used for this study:
Socio-Demographics and Information Related to the Welfare Experience
Socio-demographic information was assessed with a self-report questionnaire.
Health-Related Information
Physical Illnesses
Physical illnesses (e.g., diabetes, heart problems, high/low blood pressure) were assessed using part of the general health section of the structured clinical interview for diagnosing mental disorders (DIPS; Margraf, Cwik, Pflug, et al., 2017; Margraf, Cwik, Suppiger, et al., 2017). The 16 assessed physical illnesses were summed to give a total number of physical illnesses diagnosed between the baseline and follow-up assessments (i.e., within the previous 21 months).
Health Indicators
The Short-Form Health Survey Version 2 (SF-36 V2; Bullinger et al., 1995; Morfeld et al., 2005) was used to assess two health dimensions: The physical component summary (PCS) and the mental component summary (MCS). The PCS (α = .93 in the current study) and the MCS (α = .92 in the current study) are composite weighted scores of eight sub-scales (i.e., physical functioning, physical role functioning, bodily pain, general health perceptions, emotional role functioning, social role functioning, psychological well-being, vitality). Higher scores indicate better health.
Stress and Early-Life Adversity
Early-Life Adversity
The Adverse Childhood Experiences Questionnaire (ACE, Wingenfeld et al., 2011) was used to index ELA (e.g., sexual abuse, emotional neglect) within the CSMP (RG) or core family (CG). It contains 10 dichotomous items (0 = “no,” 1 = “yes”), with a higher total sum score (range = 0 to 10) indicating a higher number of experienced ELA (α = .74 in the current study).
Recent Stressful Life Experiences
An adapted version of the Social Readjustment Rating Scale (SRRS; Hobson et al., 1998) was used at follow-up (A3) to assess stressful life experiences (0 = “no”; 1 = “yes”) between the baseline and follow-up assessments (i.e., within the previous 21 months). The original 51 stressful experiences were extended with nine additional stressors to account for age-specific stressors (e.g., loneliness, moving into a nursing home) (Höltge et al., 2021). Higher scores (range = 0 to 60) indicate a higher number of stressors experienced within the previous 21 months (α = .81 in the current study).
Data Analysis
SPSS version 28.0 (IBM Corp, 2021) was used to conduct the descriptive statistics (e.g., mean scores, SD), dropout analyses (via t-test, U-test, Chi-squared test), as well as checking the requirements for performing a regression (such as normality via Kolmogorov-Smirnov test, and detecting outliers via Mahalanobis distance). The following effect sizes were used: Cramer’s V (for Chi-squared tests); Pearson’s r (for U-tests), where a value of .10 is interpreted as small, .30 as medium, and .50 as large; and Cohen’s d (for t-tests), where a value of .20 is small, .50 is medium, and .80 is large.
RStudio version 4.1.3 (RStudio Team, 2022) was used to analyze missingness in the data (via Little’s test, which showed that the data was completely missing at random: χ2 (86) = 95.19 p = .234), to impute missing data using a random forest approach, and to test the regression models.
To test hypothesis 1a and 1b, a generalized linear regression model was applied to predict PCS and MCS via ACE and recent stressful life events, respectively. As the number of physical illnesses is a count variable, a generalized linear regression model based on a negative binomial distribution was used to predict the number of physical illnesses. To test if a curvilinear model was a better fit to the data than a linear model, a quadratic term for ACE and recent stressful life events was added to each model and tested via the two-lines test (Simonsohn, 2019). Age and gender were used as covariates in all analyses. The incidence rate ratio (IRR) was used as an effect size. Values of >1 indicate the percentage increase in the outcome variable for a one-point increase in the predictor. Values of <1 reflect a decrease.
To test hypothesis 2, moderation analyses were conducted to investigate if ACE moderated the relationship between recent stressful life experiences and the outcome variables: total number of physical illnesses, PCS, and MCS. Post hoc analyses involved plotting the interaction at different standard deviations of the moderator, as well as conducting a t-test to examine whether the simple slopes differed significantly.
The statistical analyses are extensively described in the Appendices (see Supplemental Appendix A, Data Preparation and Main Analyses).
Results
Participant Characteristics
The final data set included N = 216 participants (Mage = 69.8 years, SDage = 10.6, 45.8% female). While the RG (n = 99) and CG (n = 117) showed a small effect with respect to gender (V = .10) and no effect with respect to age (d = 0.08), a large effect was found for reported ACE (d = −0.90), and a small effect for recent stressful life experiences (r = .22). For further details see Supplemental Appendix B, Additional Results, Participant Characteristics, Supplemental Table A1, and Table A2.
Group Comparisons of Health-Related Information
In the total sample, the mean number of diagnosed physical illnesses within the previous 21 months was 1.3 (SD = 1.4). Group differences in the number of diagnosed physical illnesses were observed between the RG (M = 1.7, SD = 1.6) and CG (M = 0.9, SD = 1.1), with a small effect size (z = −3.90, p < .001, r = .27). Group differences (with small effect sizes) were found for high/low blood pressure (V = .16), gastrointestinal problems (V = .14), diabetes (V = .20), and heart problems (V = .18). Regarding health indicators, group differences (with small effect sizes) were found for the PCS (r = .27), physical functioning (r = .22), bodily pain (r = .19), physical role functioning (r = .16), psychological well-being (r = .14), vitality (d = 0.28), and general health (d = 0.35). For additional details see Supplemental Appendix B, Group Comparisons of Health-Related Information and Supplemental Table A3.
Testing the Linear, Dose-Response versus Curvilinear Assumptions (Hypotheses 1a and 1b)
Based on the two-lines test, no evidence was found for a meaningful curvilinear effect in any of the models (see Supplemental Appendix B3). Hence, results only support a positive, linear, dose-response relationship between ACE and physical illnesses (IRR = 1.15), as well as between recent stressful life experiences and physical illnesses (IRR = 1.06) (see Table 1 for the generalized linear regression models with physical illnesses). Moreover, a decrease of 51% (IRR = 0.49) in PCS was linked to each additional recent stressful life experience. Also, a decrease of 65% (IRR = 0.35) in PCS was linked to each additional ACE. Furthermore, a decrease of 58% (IRR = 0.42) in MCS was linked to each additional recent stressful life experience. Similarly, a decrease of 56% (IRR = 0.44) in MCS was linked to each additional ACE. Results indicate that higher levels of ACE and more recent stressful life experiences are both linked to worse physical and mental health, as well as more physical illnesses (for the generalized linear regression models see Table 2 for PCS and Table 3 for MCS).
Generalized Linear Regression Models With the Total Number of Physical Illnesses as a Negative Binomial Log Link Function of Linear and Curvilinear ACE, and Linear and Curvilinear SRRS.
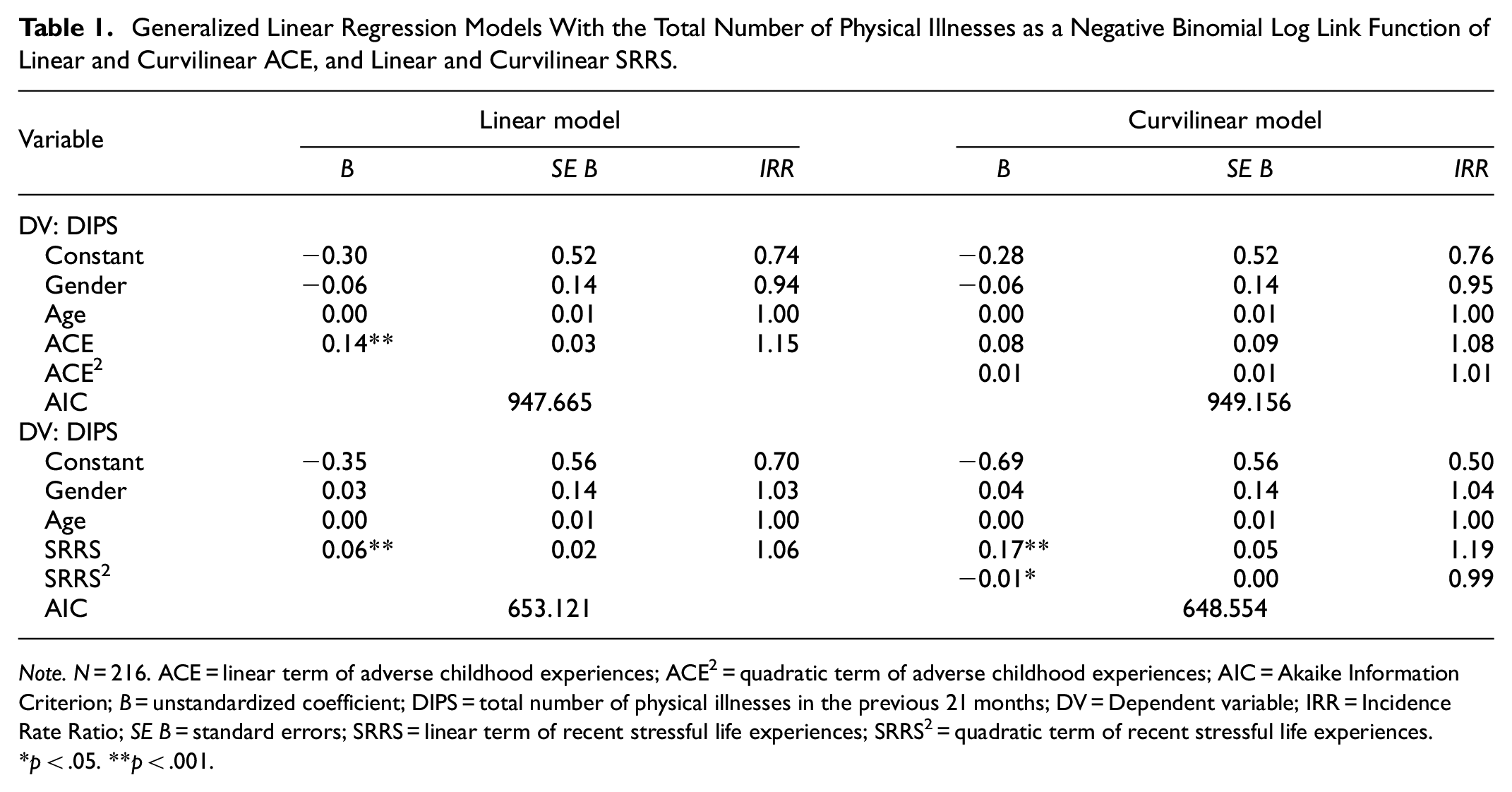
Note. N = 216. ACE = linear term of adverse childhood experiences; ACE2 = quadratic term of adverse childhood experiences; AIC = Akaike Information Criterion; B = unstandardized coefficient; DIPS = total number of physical illnesses in the previous 21 months; DV = Dependent variable; IRR = Incidence Rate Ratio; SE B = standard errors; SRRS = linear term of recent stressful life experiences; SRRS2 = quadratic term of recent stressful life experiences.
p < .05. **p < .001.
Generalized Linear Regression Models Predicting PCS via Linear and Curvilinear ACE, and Linear and Curvilinear SRRS.

Note. N = 216. ACE = linear term of adverse childhood experiences; ACE2 = quadratic term of adverse childhood experiences; AIC = Akaike Information Criterion; B = unstandardized coefficient; DV = Dependent variable; IRR = Incidence Rate Ratio; PCS = physical component summary; SE B = standard errors; SRRS = linear term of recent stressful life experiences; SRRS2 = quadratic term of recent stressful life experiences.
p < .05. **p < .001.
Generalized Linear Regression Models Predicting MCS via Linear and Curvilinear ACE, and Linear and Curvilinear SRRS.

Note. N = 216. ACE = linear term of adverse childhood experiences; ACE2 = quadratic term of adverse childhood experiences; AIC = Akaike Information Criterion; B = unstandardized coefficient; DV = Dependent variable; IRR = Incidence Rate Ratio; MCS = mental component summary; SE B = standard errors; SRRS = linear term of recent stressful life experiences; SRRS2 = quadratic term of recent stressful life experiences.
p < .05. **p < .01. ***p < .001.
Testing of the Stress Sensitization (Hypothesis 2)
A moderation analysis examined whether ACE moderated the relationship between recent stressful life experiences and the number of physical illnesses in the previous 21 months. The interaction term (b = −0.01, SE = 0.00, χ2 (1) = 4.52, p = .034; IRR: 0.99) indicated that the relationship between recent stressful life experiences and physical illnesses was not uniform through the range of ACE. Specifically, a simple slope analysis showed that recent stressful life experiences were positively associated with the number of physical illnesses at ACE 1 SD above the mean (b = 0.03, SE = 0.02, χ2 (1) = 4.41, p = .036; IRR: 1.03), at the ACE mean (b = 0.06, SE = 0.02, χ2 (1) = 15.06, p < .001; IRR: 1.06), as well as at ACE 1 SD below the mean (b = 0.08, SE = 0.02, χ2 (1) = 14.59, p < .001; IRR: 1.09). Visual inspection of the interaction plot (see Figure 1) showed that individuals with lower (compared to higher) levels of ACE had a lower number of physical illnesses at low and mean levels of recent stressful life experiences. However, at high levels of recent stressful life experiences, individuals with lower (compared to higher) levels of ACE had a higher number of physical illnesses. This may indicate the relevance of the recency of (high levels of) stressful life experiences over past ACE in relation to physical illnesses.
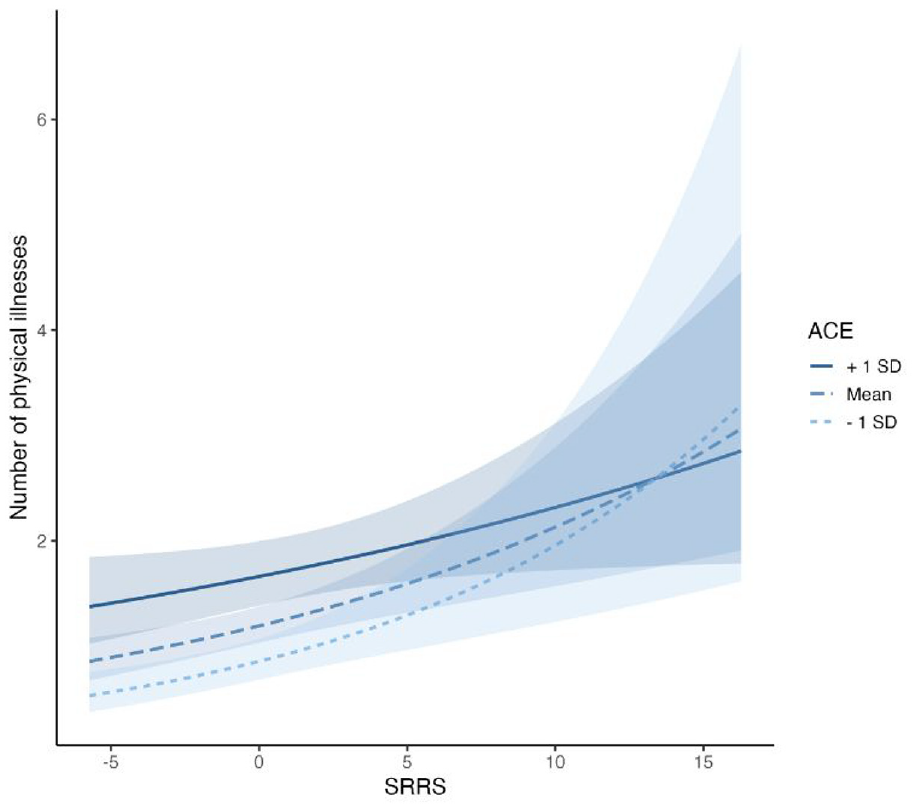
Interaction with 95% confidence intervals between recent stressful life experiences (SRRS) and early-life adversity (ACE) in predicting number of physical illnesses over a 21 month period.
The moderation analysis for PCS and MCS did not show any meaningful effects (see Supplemental Appendix B, Testing the Stress Sensitization [Hypothesis 2]).
Discussion
This study examined the heterogeneity in the health of older individuals with differing levels of ELA and recent stressful life experiences. It further aimed to examine the expected stress-health relationships (i.e., linear, curvilinear). Results showed that the RG (i.e., individuals with a higher risk for ELA) reported more physical illnesses diagnosed within the previous 21 months, as well as worse physical and mental health. These stress-health relationships followed a linear dose-response pattern. No substantial empirical support was found for a health steeling effect (i.e., a curvilinear relationship) by ELA nor recent stressful life experiences. Exposure to ELA was found to moderate the relationship between recent stress and physical illnesses.
The worse health outcomes observed in the RG compared to the CG were expected and corroborate existing research with other survivors of institutional abuse (e.g., Carr et al., 2019; Sigal et al., 2003). The meaningfully higher prevalence for diabetes, heart problems, gastrointestinal problems, and high/low blood pressure in the RG may hint at unhealthy stress coping behaviors (Cohen et al., 2007), as individuals in the RG were also more likely to be smokers and had a higher mean waist-to-hip ratio (see baseline data in Thoma et al., 2021).
The stress-health relationship in older adulthood seems to be best described by a linear, dose-response relationship, as can be expected based on traditional stress models (Adler, 2009; Engel, 1977). While this finding contrasts with reports of a curvilinear relationship between lifetime adversities and physical health in middle-aged adults (Seery et al., 2010); it is in line with an online survey study that found a linear (rather than curvilinear) relationship between ELA and physical health in later life (Höltge et al., 2019). As such, there currently exists no substantial empirical support for a health steeling effect by ELA or recent stressful life events in older adulthood.
The significant interaction term showed that individuals with higher levels of ELA reported fewer physical illnesses at high levels of recent stressful life experiences compared to those with lower levels of ELA. It may be that experiencing a higher level of ELA may prepare an individual for (dealing with) subsequent stressful life experiences, which would support the assumption of a steeling effect by ELA. However, this finding must be interpreted with caution, as it is only a trend finding, and the current sample also has a generally low level of recent stressful life experiences.
A meaningful strength of this study was the heterogeneity of participants with respect to ELA. This contributed to the variability in the data, which is essential when examining a special phenomenon, such as the steeling effect (Höltge et al., 2018). Nonetheless, several limitations must be considered, which may have limited the detection of a steeling effect. The current study only considered physical illnesses diagnosed within the previous 21 months (as opposed to existing diagnoses or chronic illnesses). While this was done to determine the incidence of physical illnesses, also in relation to the stressful life events, the consideration of existing physical illnesses might have influenced the findings. Additional limitations are the retrospective assessment (mainly with respect to ELA), the self-selection of participants, potential biases related to self-report measures, as well as the historical uniqueness of the RG (which restricts the generalization of the reported results).
Recommendations
The results of this study provide support for a dose-response relationship between stress and health in older adults. No evidence was found for the assumption that some (i.e., moderate) stress may be beneficial for health in this particular sample. Stress, in the form of recent stressful life experiences and ELA, may therefore be regarded as potentially health-damaging factors. The prevention, or minimization of ELA exposure after detection, should therefore be a priority for policy makers, social workers, and health professionals. While psychotherapy is a specific and effective treatment intervention for survivors of ELA (e.g., Duberstein et al., 2018), it may not be equally accessible or affordable for all affected individuals. This is particularly relevant for older adults, as is the case in Switzerland, as older individuals may be comparatively reluctant to go to a psychotherapist with mental health issues. This may be due to (for instance) the stigmatization of mental health disorders, which may be more prevalent in older age; as well as having been raised in a time with differing sociocultural norms and expectations surrounding mental health and coping (Schuler et al., 2020). Future research efforts should therefore be directed toward the investigation of easily accessible, low-cost interventions to remediate the negative health impact of ELA (see for instance Donofry et al., 2021).
Conclusion
This was the first study to examine stress-health relationships in two groups of older individuals with differing levels of ELA. Even multiple decades after exposure to ELA, its detrimental health impact can still be detected in affected individuals. This suggests that previous stress exposure, in the form of ELA, may be a critical factor in dealing with subsequent stressful life experiences, and ultimately, in explaining the vast heterogeneity in health in later life.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241267141 – Supplemental material for Investigating Stress Sensitization and Steeling for Early-Life Adversity and Recent Stressful Life Experiences: Health and Illness in Older Adulthood
Supplemental material, sj-docx-1-sgo-10.1177_21582440241267141 for Investigating Stress Sensitization and Steeling for Early-Life Adversity and Recent Stressful Life Experiences: Health and Illness in Older Adulthood by Myriam V. Thoma, Simona-Viktoria Balsiger, Jan Höltge and Shauna L. Rohner in SAGE Open
Footnotes
Acknowledgements
The authors wish to thank all participants who shared their experiences for this study. We also extend our gratitude to all project members that were involved in various stages of the project: Lia Blanckenhorn, Nora Brenneisen, Selma Bruggisser, Julienne Buess, Fabian Caneve, Valentino Cirulia, Isabel Courage, Gabriela della Pietra, Michelle Eichenberger, Carla Eising, Keegan Evangelista, Anna Frangioudakis, Carmen Frey, Melinda Hofstetter, Juliana Holder, Tamara Lovrinovic, Elena Mayorova, Amelie Mazza, Jessica Michel, Sheena Müller, Jessica Paul, Dinja Plattner, Martina Preisig, Ronja Schmid, Sandro Stutz, Vera Tommer, and Andreas Maercker.
Author’s Note
This research was conducted while Dr. Shauna L. Rohner was at the University of Zurich, Institute of Psychology, Division of Psychopathology and Clinical Intervention. She is now at the Competence Centre for Mental Health, School of Health Sciences, OST-Eastern Switzerland University of Applied Sciences, 9001 St. Gallen, Switzerland; and may be contacted at
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swiss National Science Foundation, National Research Program 76, “Welfare and Coercion—Past, Present and Future” (grant number 407640_177355/1). This work was also supported by the Swiss Government Excellence Scholarship (ESKAS-Nr. 2016.0109) which funded the last author’s (Shauna L. Rohner) position until August 2019. Jan Höltge’s position was supported by a Postdoc.Mobility Scholarship from the Swiss National Science Foundation (grant number P400PS_194538). This study was also supported by the University Research Priority Program (URPP) “Dynamics of Healthy Aging” at the University of Zurich.
Data Availability Statement
Due to the sensitive nature of the data, the data cannot be published on a public data repository. Requests to access the datasets should be directed to
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.