
Abstract
Using a questionnaire, this study investigated the numerous factors affecting the Jordanian population’s rejection of COVID-19 vaccines. The data were collected in 2020 to 2021. Using the chi-square test, t-test, Cramer’s V-test, and analysis of variance, we found that most of the Sample (72.6%) obtained information on COVID-19 and its vaccines from social media, radio, and television. In comparison, 31.1% and 35.4% of the Sample obtained from government/official sources or health specialists, respectively, with a lesser share relying on colleagues (13.7%) and scientific lectures (17.5%). Furthermore, depending on the participants’ characteristics, there were significant differences in the information sources or abstinence factors. Several factors were associated with vaccine refusal and hesitancy, including contradictory/conflicting information, lack of trust in vaccines/manufacturers, doubt about the vaccines’ effectiveness, and the belief that the risks of COVID-19 are minimal. Based on these findings, we present several recommendations for policymakers.
Plain Language Summary
Factors associated with vaccination refusal among a sample of the Jordanian population This study aimed to comprehend what causes Jordanians to refuse vaccinations. Most participants of the present study learned about COVID-19 and vaccines from radio, television, and social media. Fewer of them turned to official and professional sources. Conflicting information about COVID-19, skepticism about the effectiveness of vaccines and potential side effects, skepticism toward vaccine manufacturers and media sources, uncertainty regarding the efficacy of vaccines, and mistrust in information sources regarding the virus and vaccines have led to confusion and resistance to following health recommendations. These factors resulted in vaccine rejection by considerable percentages of the Jordanian population.
Introduction
The COVID-19 outbreak was an unprecedented and extraordinary event at the global level, with the resulting pandemic causing the deaths of millions of people worldwide and many more suffering severe consequences such as long-lasting health complications. The pandemic has undermined individuals’ health stability and prompted preventive and precautionary measures in all countries, such as curfews, movement restrictions, and social distancing (Alajmi et al., 2022; Alasmari, 2020). MacDonald and SAGE Working Group on Vaccine Hesitancy (2015) provided a comprehensive overview of vaccine hesitancy, defining it as a delay in accepting or refusing vaccination despite its availability. The development of vaccines and efforts toward widespread vaccination has been met with doubts and rejection (Mannan, 2020; Qattan, 2021; Schwarzinger et al., 2021; World Health Organization [WHO], 2020a; World Health Organization [WHO], 2020b).
Social media networks have fostered skepticism, fear, and vaccine rejection. Platforms like Twitter are inundated with negative messages about vaccines, including claims that vaccination is unnecessary, and the survival rate of COVID-19 is high, and concerns about vaccines’ safety, efficacy, and potential side effects (El-Elimat et al., 2021; Nuzhath et al., 2020; Sallam et al., 2021). Additionally, there is a pervasive lack of trust in the vaccines, skepticism about the rapid vaccine development process, and doubts about the effectiveness of Chinese vaccines (Al-Qarem, et al., 2021; Callaghan, 2021; Elhadi et al., 2021; Kalyani, et al., 2020; Nuzhath et al., 2020). Commercial motives behind vaccine promotion are also a concern (Al-Mohaithef & Padhi, 2020; Kalyani, et al., 2020). A study conducted in Qatar highlighted safety concerns and side effects as significant factors contributing to vaccine hesitancy (Alabdulla et al., 2021). Explicit refusal or reluctance to vaccinate has been associated with gender, age, education level, and compliance with previous vaccinations (Al-Mohaithef & Padhi, 2020; Alabdulla et al., 2021; World Health Organization, 2015). Political beliefs also play a crucial role, as conservative views and support for Donald Trump have been linked to a higher likelihood of vaccine rejection (Callaghan et al., 2021).
Riad, Abdulqader, Morgado, et al. (2021) conducted a study to determine the global prevalence and drivers of dental students’ COVID-19 vaccine hesitancy. They found that approximately one-third of dental students worldwide reported vaccine hesitancy. The primary drivers of vaccine hesitancy among dental students were concerns about vaccine safety and efficacy, distrust in vaccine developers, and the influence of social media. In another study by Riad, Pokorná, Antalová, et al. (2021), the prevalence and drivers of COVID-19 vaccine hesitancy among Czech university students were investigated. They reported that vaccine hesitancy was prevalent among Czech university students, with approximately one-third of the participants expressing hesitancy. The main factors contributing to vaccine hesitancy among students included concerns about vaccine side effects, lack of trust in vaccine safety, and perceived low susceptibility to COVID-19.
Klugar et al. (2021) also conducted a study in Czechia to examine COVID-19 vaccine booster hesitancy among healthcare workers, revealing that a significant proportion of them expressed hesitancy toward receiving a COVID-19 vaccine booster. Factors associated with booster hesitancy among this population included concerns about vaccine safety, doubts about the necessity of boosters, and previous vaccine-related adverse events. Kateeb et al. (2021), Lazarus et. al. (2021) and Sun et al., (2021) also identified several predictors of vaccine willingness, including trust in vaccine safety and efficacy, confidence in healthcare professionals, previous vaccine acceptance behavior, and belief in the importance of vaccination for personal and public health.
According to MacDonald and SAGE Working Group on Vaccine Hesitancy (2015), “Vaccine hesitancy is complex and context-specific, varying across time, place, and vaccines.” It is influenced by factors such as complacency, convenience, and confidence.” Developing and implementing effective vaccines has been critical in combating the spread of the virus. However, vaccine hesitancy and refusal have emerged as significant obstacles to achieving widespread vaccination coverage. For example, in Jordan, despite the Jordan government’s repeated warnings and encouragement of citizens to get the COVID-19 vaccine, most people have not received it, and a high percentage intend not to take it (Al-Qarem, et al., 2021; El-Elimat et al., 2021). Therefore, this study investigates the factors associated with vaccine refusal among the Jordanian population and aims to answer the following research questions: (a) What are the most used sources of information regarding COVID-19 vaccines in Jordan? (b) What factors influence Jordanian society’s refusal to receive the vaccines? (c) Do gender, age, marital status, education, occupation, and family income affect vaccine abstinence?”
Methodology
Research Design
An analytical survey-based cross-sectional study was conducted to explore Jordanian attitudes toward receiving the COVID-19 vaccine. The study utilized a self-administered questionnaire disseminated online through WhatsApp groups to collect data from the target participants.
Study Locations
This study was conducted in the three central regions of Jordan: North, Middle, and Southern.
Study Population and Sample
The study population included Jordanians who did not receive a COVID-19 vaccine or who abstained from receiving one. Convenience sampling was utilized on a sample of individuals in Jordan, whose total population was 11,057,000 in 2021 (Department of Statistics (DOS) & Government of Jordan, 2021). Individuals who received a COVID-19 vaccine were excluded from the study. The sample size was 212. The sample was selected based on snowball techniques, as the questionnaire was distributed to various WhatsApp groups and through other social media contacts; we also contacted people who refused vaccination and asked them to lead us to others who did so. This process takes time and effort; after receiving 212 questionnaires, we thought that the number satisfies the immediate need to explore the phenomenon of vaccine refusal.
Studied Variables and Instruments
Variables
The variables studied include select sociodemographic variables (gender, marital status, monthly income level, education level, and employment status), sources of information (social media, radio, and TV; medical and health professionals; family and friends; governmental and official agencies; circulars; scientific lectures; and colleagues), and factors associated with vaccine refusal, of which there were 30, covering the following main categories: vaccine quality, safety, misinformation and distrust in sources of information, commercial motives of vaccine manufacturers, conspiracy and denial of the existence of COVID-19, and the belief that there is no need for vaccines.
Instrument
A special questionnaire was designed to collect data. The questionnaire design was based on previous literature (Alabdulla et al., 2021; Al-Mohaithef & Padhi, 2020; Al-Qerem & Jarab, 2021; El-Elimat et al., 2021; Elhadi et al., 2021; Kalyani et al., 2020) and consultation with specialists. “In addition, a short pilot survey was sent to a select group of people concerning what they perceived as being the main reasons for vaccine abstention in Jordan.” The questionnaire included sections on participants’ sociodemographic characteristics, sources of COVID-19 and vaccine information, and factors influencing vaccine refusal.
The instrument’s reliability was determined using Cronbach’s alpha and the Guttman split-half method. Both reliability measures show acceptable values (Table 1).
Reliability of the Study Instrument.

Data Collection and Statistical Analysis
The online self As The online self-assessment questionnaire was electronically distributed to participants using emails, social media (WhatsApp, Facebook), and colleagues who knew people who refused to be vaccinated. Two hundred and twelve questionnaires were received and used for data analysis.
Descriptive and advanced statistics were used to describe the Sample and for sources of information on COVID-19 and vaccines. Quantitative descriptions (means and standard deviations) were used for factors associated with vaccine refusal. The chi-square test, t-test, analysis of variance (ANOVA), and Cramer’s V-test were used to examine the effect size.
Ethical approval for the present study was obtained from the relevant institution. The nature of the study was explained to the participants as a requirement for their consent. They were informed that their participation was voluntary, they could withdraw from the study at any time, and that anonymity and confidentiality of the data were assured. Only those who agreed with the ethical requirements and provided informed consent participated in the study. The informed consent form was placed on the first page of the online questionnaire.
Results
Description of the Sample
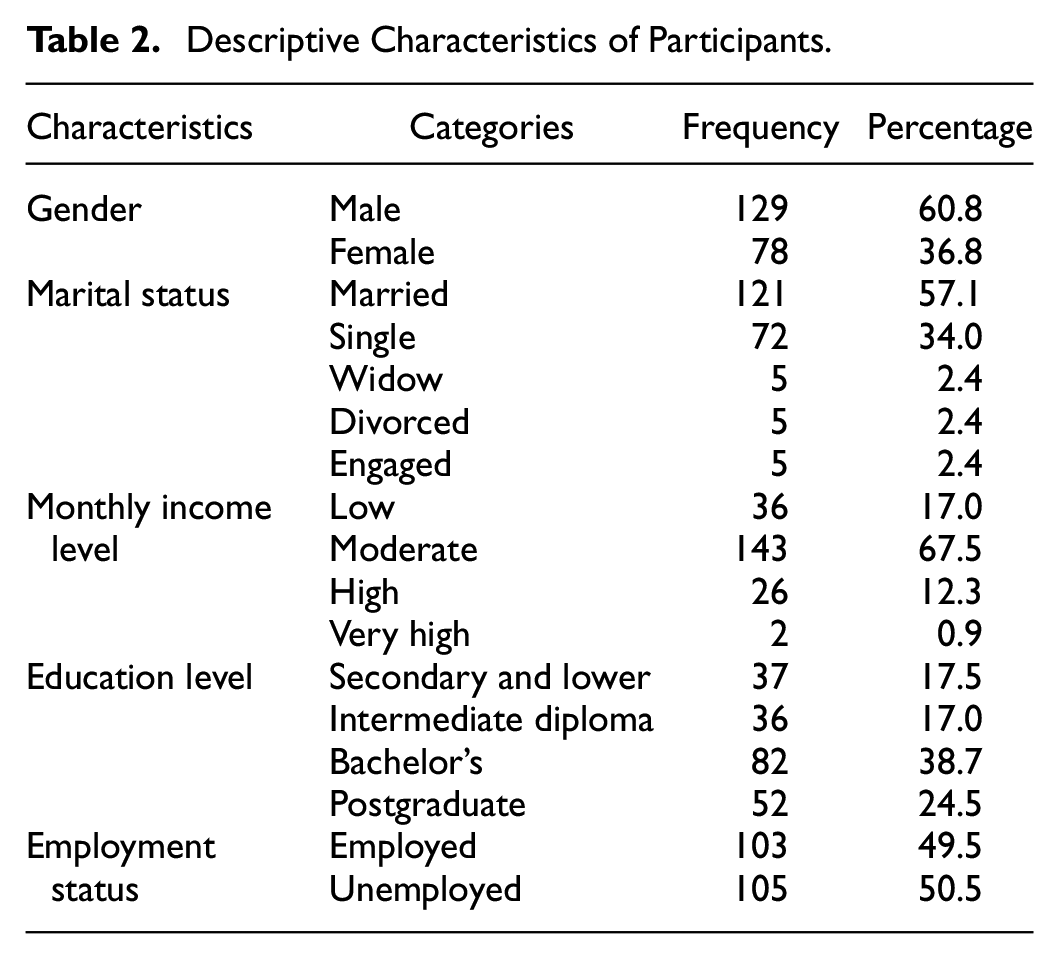
Over two-thirds of the Sample (60.8%) were females, and more than half (57.1%) were married. Moreover, more than two-thirds of the participants had a moderate income (67.5%). Over one-third (38.7%) had bachelor’s degrees, while 24.5% had postgraduate degrees (24.5%). Regarding employment, 49.5% were employed. Table 2 lists all of the participants’ descriptive characteristics.
Descriptive Characteristics of Participants.
Sources of Information on Vaccines
Table 3 ranks the various sources of information on COVID-19 and its vaccines. The ranking g was based on the values of the arithmetic mean. The higher the values, the more agreeing respondents. It indicates the importance of the reasons behind vaccine refusal. According to the findings, around two-thirds of the participants obtained information about the COVID-19 vaccines from social media (72.6%), and more than half relied on radio and television news. In comparison, only 31.1% of the Sample obtained information from government and official sources, while 35.4% obtained it from health specialists. A lesser share relied on colleagues (13.7%) and scientific lectures (17.5%).
Ranked Sources of Information for the Total Sample and Male–Female Comparisons.
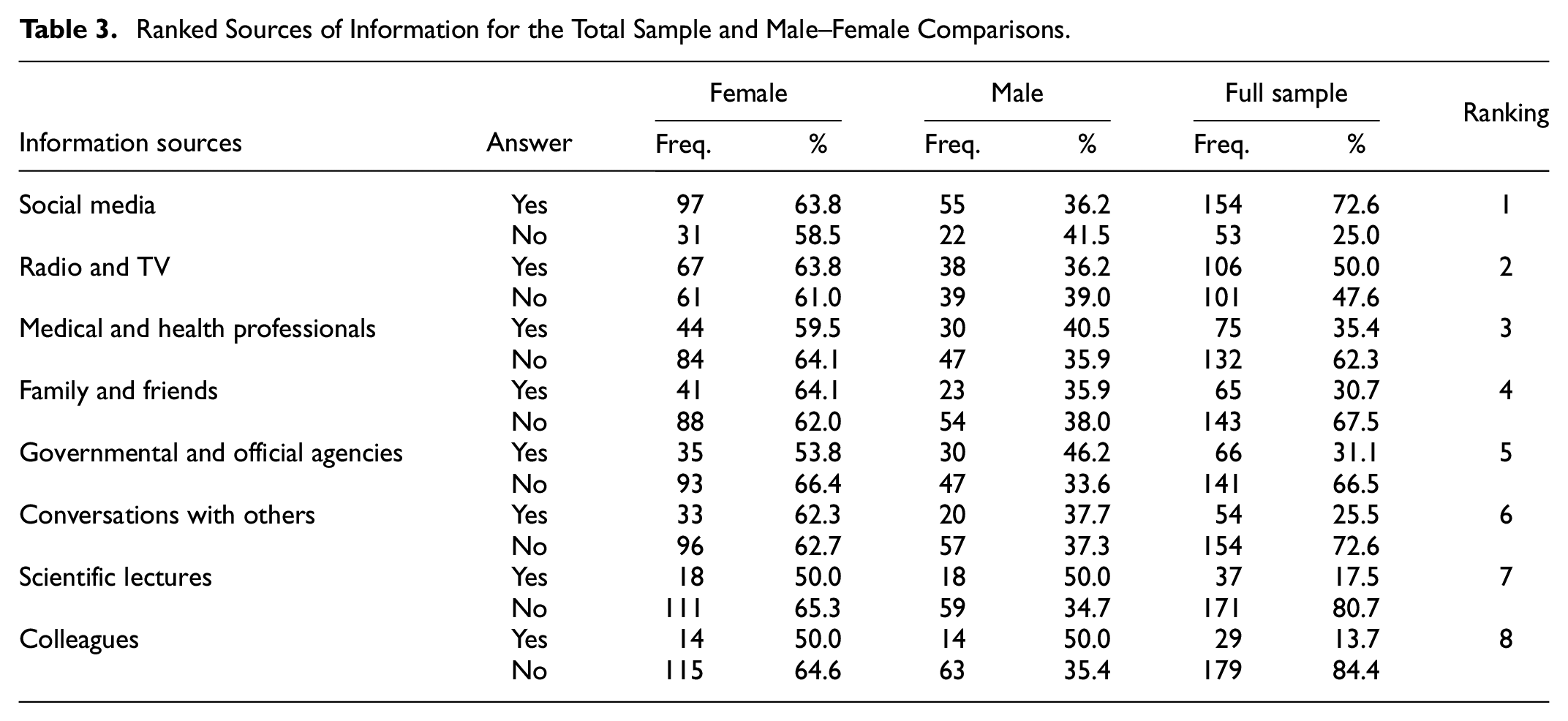
We analyzed these rankings by gender using the chi-square test. No statistically significant differences were found between males and females. We then used Cramer’s V-test to examine the effect size. It was evident that the size of the differences was minimal and did not indicate significant differences between the two groups. Thus, we concluded that males and females used the same sources of information on COVID-19 and its vaccines.
Table 4 ranks the factors associated with vaccine refusal by mean. The most widely reported reasons behind individuals’ refusal to take the vaccines were fear of future side effects (Mean = 7.99 and SD = of (2.84) and fear of current side effects (Mean = 7.52 and SD = 3.14). Furthermore, there was a lack of trust in the vaccines’ efficacy due to the vaccines’ short development time (Mean = 7.28 and SD = 3.29), and individuals also cited the vaccines’ limited protection as a concern (Mean = 7.28 and SD = 3.29). The least cited reason was the complicated process of taking the vaccines (Mean = 3.41 and SD = 3.48).
Factors Associated With Vaccine Refusal.
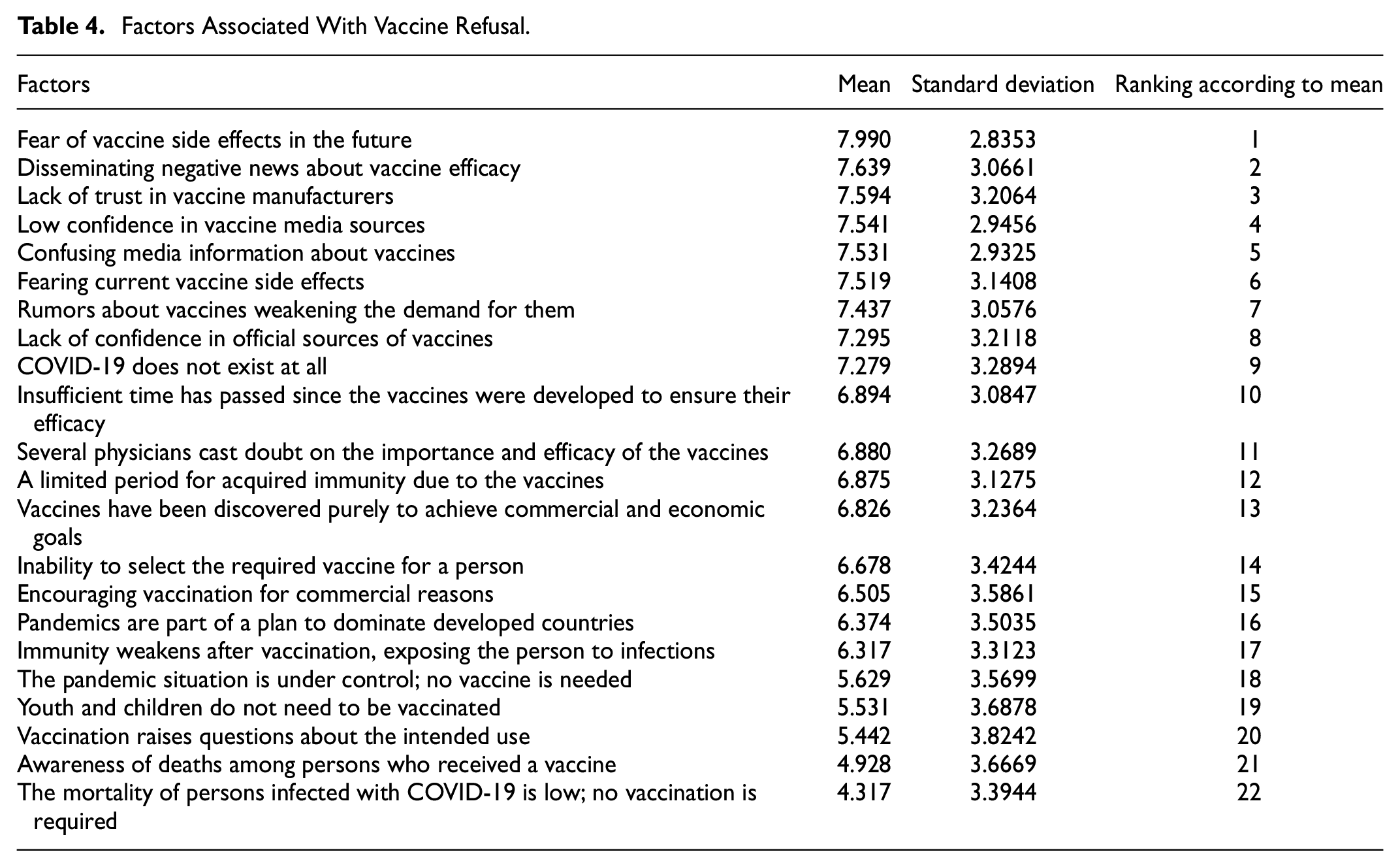
Several participants cast doubt on the vaccines’ effectiveness (Mean = 6.88, SD = 3.27), preferring to rely on natural methods and healthy nutrition for protection (Mean= 6.43, SD = 3.38). Other participants indicated that they believed that “there is no need for youth and children to take the vaccine” (Mean = 5.53, SD = 3.69) and that there have been “deaths among people who have received the vaccine” (Mean = 4.93, SD = 3.67). In addition, some noted that the incidence of death among those infected by COVID-19 is low; thus, there is no need for vaccination (Mean = 4.32, SD = 3.39). “Furthermore, some participants noted that infection of persons by the virus protects them from re-infection (Mean = 3.95, SD = 3.06); thus, there is no need for vaccination.”
“The two most important factors regarding doubts about the vaccines were the commercial goals of vaccine manufacturers and the fact that capitalist industries control the vaccines.” The results show that items “the vaccines were discovered to achieve purely commercial and financial aims” (Mean = 6.83, SD = 3.24), “pandemics are part of a plan to impose the industrial states’ dominance on the world” (Mean = 6.37, SD = 3.50), “encouraging vaccine use is for commercial reasons” (Mean = 6.51, SD = 3.59) were X.
Table 5 show the comparisons based on ANOVA. The t-test revealed statistically significant differences between males and females on the item “inability to choose the type of vaccine required for the person” (p = .043, with means of 7.03 and 6.01 for males and females, respectively). They also differ on the item “insufficient time has passed since the vaccines were developed to ensure their efficacy” (p = .012, means of 7.7 and 6.4 for females and males, respectively). We also found that employed participants were more likely to report that the “vaccines are insufficiently available” (p = .016, means of 3.14 and 4.25 for the employed and the unemployed, respectively). These groups also differed significantly on the items “the vaccines were found to achieve purely commercial and financial aims” (p = .009, with means of 7.4 and 6.2 for the employed and unemployed, respectively). And “awareness of deaths among persons who received a vaccine” (p = .022, with means of 5.5 and 4.36 for the employed and unemployed, respectively). The latter result indicates that employed participants were more knowledgeable of the occurrence of deaths among those vaccinated.
Analysis of Variance Comparisons (p-values).


Significant differences were also detected between married and single individuals on the item “Rumors about vaccines weakening the demand for them” (p ≤ .037, with means of 7.98 and 6.92 for single and married individuals, respectively). Moreover, single persons significantly differed from married persons on the item “encouraging vaccination for commercial reasons” (p ≤ .046, with means of 7.05 and 5.59 for single and married individuals, respectively). Thus, single individuals are more likely to believe that commercial reasons motivated the spreading of the vaccines than married ones. Further, statistically significant differences were found between married and unmarried respondents on their view of “discovering vaccines for purely commercial and financial purposes”, which indicates that married respondents were more likely to believe that vaccine promotion was related to commercial and financial gains. On another aspect, single participants were more inclined to regard the COVID-19 pandemic as a part of a scheme.
“Pandemics are part of a plan to dominate developed countries” (p ≤ .039, with means of 5.94 and 5.14 for married and single individuals, respectively).
Regarding the education level, significant differences were observed between university graduates and individuals with diplomas regarding their perceptions of certain items. These items include “the procedures for taking the vaccine are complicated” (3.65:4.6 and 1:5.39), “COVID-19 does not exist at all” (2.62, 5.1, 1:3.47), and “The pandemic situation is under control; no vaccine is needed” (p. 4.94, 7.63). These findings suggest that university graduates are more likely to cite vaccine complexity and the belief that the pandemic is under control as reasons for abstaining from or refusing vaccines. Conversely, the belief that there is no COVID-19 pandemic is more prevalent among school graduates. Additionally, statistically significant differences were found in income levels, with individuals in the middle-income bracket being more inclined to believe that “COVID-19 does not exist at all” compared to those in the lower income bracket (p ≤ .044; means of 5.03 and 3.14 for lower income and middle income, respectively).
Discussion
The COVID-19 pandemic has posed significant challenges to global public health, necessitating the development and distribution of vaccines to mitigate the spread of the virus. However, vaccine hesitancy has become a significant barrier to achieving widespread vaccination coverage (World Health Organization [WHO], 2015). Vaccine hesitancy is a complex phenomenon influenced by various factors, including individual beliefs, societal attitudes, and contextual influences (Larson et al., 2014). Vaccine hesitancy is not new, but it has gained heightened attention during the COVID-19 pandemic. Previous studies have highlighted the importance of understanding the factors contributing to vaccine hesitancy in designing effective interventions (Dror et al., 2020). Misinformation and misconceptions about vaccines, distrust in government and healthcare institutions, and concerns about vaccine safety and efficacy have been identified as common reasons for vaccine hesitancy (Dubé et al., 2013; Paterson et al., 2016).
The findings revealed that a significant proportion of the Jordanian population exhibited vaccine refusal or hesitancy. COVID-19 vaccine resistance could seriously impact public health initiatives to stop the virus’s spread. This study also indicates that individuals who abstained from vaccination primarily relied on social media for information about the COVID-19 virus, with a lesser reliance on radio and television news broadcasts. In contrast, a minority of abstainers sought information from health specialists, scientific lectures, or government and official sources. Social media was the most commonly used source of information (72.6%), followed by radio and television news. Government and official sources, as well as health specialists, were less frequently relied upon for information. There were no significant differences between males and females regarding their sources of information, suggesting that both genders were equally exposed to similar sources (Al-Qarem & Jarab, 2021). These patterns suggest a decline in confidence among abstainers in the information provided by healthcare professionals and scientific journals. It is essential to emphasize the significance of vaccination and its limited side effects compared to the risks associated with not getting vaccinated. Therefore, it is necessary to shift how vaccine information is presented and disseminated, contrary to the findings of previous studies by El-Elimat et al. (2021) and KEKST CNC (2021), which indicated the importance of reliance on scientific journals and Ministry of Health specialists for information. These findings suggest a change in people’s attitudes toward information-seeking.
The findings of this study align with previous research that has identified misinformation as a critical driver of vaccine hesitancy (Betsch et al., 2020; Smith & Anderson, 2018). A significant proportion of participants reported encountering vaccine-related misinformation on social media platforms. These findings are consistent with studies highlighting the rapid spread of false information through online platforms (Pennycook & Rand, 2019; Wardle & Derakhshan, 2017). Misinformation in social media poses a challenge for public health authorities and necessitates the development of targeted strategies to counteract false narratives and promote accurate vaccine information (Broniatowski et al., 2018). The erosion of trust in institutions can have far-reaching consequences for public health efforts, undermining the credibility of vaccine recommendations and interventions (Freimuth & Quinn, 2004). Therefore, interventions should rebuild trust by promoting transparency, providing clear and accurate information, and involving trusted community leaders in vaccine communication campaigns (Dubé et al., 2015; Uttekar et al., 2023). Moreover, our study identified a correlation between vaccine hesitancy and distrust in government and healthcare institutions. This finding aligns with previous studies that have demonstrated the role of trust in shaping vaccine attitudes (Callaghan et al., 2021; Larson et al., 2015; Lewandowsky et al., 2013; Schwarzinger et al., 2021).
The safety and efficiency of the vaccines are prominent factors behind abstinence or rejection. Those who refuse to take the vaccines doubt their effectiveness and have concerns about their current and future side effects. This finding aligns with previous research that has identified vaccine safety as a prominent factor contributing to vaccine hesitancy (Dubé et al., 2013; Larson et al., 2014). The fear of the future and current side effects of the vaccines was the foremost factor for people abstaining from the vaccines. Less noticeable factors were “the lack of confidence in the vaccines’ effectiveness due to the short time to discover the vaccine” and “the limited time for protection provided by the Vaccine.” The present study’s findings are consistent with the results of several studies (Al-Qarem, 2021; Callaghnan, 2021; Elhadi et al., 2021). Public health authorities must address these concerns by ensuring robust vaccine safety monitoring systems, communicating rigorous regulatory processes, and disseminating evidence-based information on vaccine effectiveness (Hinman et al., 2020; Larson et al., 2018).
The results suggest that addressing concerns related to vaccine safety, efficacy, and commercial motives could help increase vaccine acceptance in the population. Public health campaigns should focus on providing accurate information through diverse channels, including social media, to combat misinformation and enhance trust in vaccines. Tailored strategies that address the specific concerns of different demographic groups, such as males, females, and married individuals, could be developed to improve vaccine uptake (Al-Qarem & Jarab, 2021).
The study also explored gender differences in vaccine refusal factors. Significant differences were found in the belief that individuals should be able to choose the type of vaccine they receive, with males expressing a stronger belief in this regard. Females were more concerned about insufficient time since the vaccines’ development to ensure their efficacy. Employed participants were more likely to report that vaccines were insufficiently available and that they were aware of deaths among vaccinated individuals. Married individuals were more likely to believe in the commercial motives behind vaccine promotion and Rumors about vaccines weakening their demand (Al-Qarem & Jarab, 2021).
Notably, we observed that a highly educated segment of the population abstained from vaccination, suggesting that educational level alone does not necessarily increase awareness of the importance of vaccination and may even amplify vaccine apprehension. The reluctance of educated people to take the vaccines could be attributed to the absence of a scientific authority providing accurate and reliable information about vaccine composition, effects, importance, and other pertinent scientific details. Additionally, it seems that the private sector has been more stringent in enforcing vaccination requirements for its employees, corroborating the findings of studies conducted by the Al-Mohaithe & Padhi (2020), Elhadi et al. (2021), Schwarzinger (2021), Sonawane et al. (2023), and World Health Organization (2015)
Interestingly, educated people are more inclined to attribute their refusal to “the complexity of the vaccination procedures” and believe that “COVID-19 does not exist.” Thus, contrary to common sense, education does not contribute to a better understanding of the need for vaccination. This may be due to confusing information about vaccines from knowledgeable health personnel (Al-Mohaithe &Padhi, 2020). Married people are more likely to attribute their vaccine refusal to “Rumors about vaccines weakening the demand for them in traditional media and social networks media.” It was also evident that there are differences in income levels on “COVID-19 does not exist.” Employment has a significant positive correlation with three factors associated with vaccine refusal: the insufficiency of vaccines, the development of vaccines for commercial and financial purposes, and deaths caused by vaccination. These results are consistent with the Al-Mohaithef and Padhi (2020) and World Health Organization (2015) studies.
Furthermore, it appears that individuals hold beliefs regarding the economic, technological, and political control, and dominance of developed countries at the global level. They perceive these countries to prioritize their interests and wealth at the expense of weaker nations. This belief and conspiracy theories make people hesitate to trust the COVID-19 vaccines. These findings align with the results of studies conducted by Nuzhah et al. (2020) and Sallam et al. (2021), highlighting the role of these determinants in vaccine refusal. Factors such as complex procedures, limited availability of vaccines, and concerns about crowded vaccination locations have also contributed to vaccine hesitancy. One significant factor leading to some individuals’ reluctance to get vaccinated is the desire to have the option to select a specific vaccine, as there are fears that certain vaccines may have higher side effects or lower efficacy.
Conclusions
The present study contributes to the growing body of evidence on vaccine hesitancy by highlighting the role of misinformation, distrust in institutions, and concerns about vaccine safety and efficacy. These findings underscore the importance of implementing multifaceted interventions that address these factors. Regarding vaccine refusal factors, fear of future and current side effects were the most commonly reported reasons for not taking a vaccine. Lack of trust in the vaccines’ efficacy due to their rapid development and limited protection also contributed to vaccine refusal. Participants doubted the vaccines’ effectiveness and preferred natural methods and healthy nutrition for protection. Additionally, beliefs such as the notion that youth and children do not need a vaccine, the awareness of deaths among vaccinated individuals, and the low fatality rate among COVID-19-infected individuals influenced vaccine refusal (Al-Qarem & Jarab, 2021).
The COVID-19 pandemic has posed significant challenges worldwide, including vaccine hesitancy, and refusal. This study aimed to explore vaccine refusal in Jordan and the factors contributing to it. The findings revealed important insights into the attitudes and beliefs of Jordanian society regarding COVID-19 vaccination. The study population consisted of individuals in Jordan who had either not received a vaccine or abstained from them. The Sample included 220 participants, and data were collected using a self-administered online questionnaire. The study examined various sociodemographic variables, sources of information, and factors associated with vaccine refusal.
The results showed that fear of future and current side effects, lack of trust in the vaccines’ efficacy and development process, and limited protection were among the most common reasons for vaccine refusal. Participants doubted the vaccines’ effectiveness and favored natural methods and healthy nutrition for protection. Some participants believed that youth and children did not need vaccines and noted deaths among vaccinated individuals. Commercial motives and conspiracy theories were also cited as reasons for vaccine refusal. The study highlighted the sources of information used by participants, with social media being the most commonly relied upon, followed by radio and television news. Government and official sources, as well as information from health specialists, were less frequently utilized. However, there were no significant gender differences regarding sources of information.
Gender, employment status, and marital status were associated with specific reasons for vaccine refusal. For example, males were more concerned about the ability to choose the type of vaccine, while females expressed greater concerns about the time passed since vaccine development. Employed participants were more likely to report insufficient vaccine availability and the commercial motives behind vaccine promotion. Married individuals were more likely to believe in vaccine rumors and perceive commercial reasons for vaccine encouragement.
The findings from this study contribute to the understanding of vaccine refusal in Jordan and provide valuable insights for public health authorities and policymakers. Strategies to address vaccine hesitancy should consider the specific concerns and beliefs of the population, particularly regarding safety, efficacy, and trust in the vaccine development process. Tailored communication campaigns and education initiatives targeting different demographic groups could help address misconceptions and increase vaccine acceptance. It is important to note that this study had some limitations, including convenience sampling and reliance on self-reported data. Future research could employ more representative sampling methods and include qualitative approaches to understand the reasons for vaccine refusal better. Addressing vaccine hesitancy is crucial for achieving widespread vaccination coverage and effectively combating the COVID-19 pandemic. Addressing vaccine hesitancy is crucial for achieving widespread vaccination coverage and effectively combating the COVID-19 pandemic.
Strengths
Although the study sample was small, it included employed and unemployed people, married and single people, and people with varying education, and income levels. This comprehensive approach provides a more nuanced understanding of the factors associated with COVID-19 vaccine abstinence or refusal. This quantitative approach gives the findings more rigor and allows for a more objective interpretation. The study’s findings are consistent with previous research on vaccine hesitancy and the influence of social media on public perceptions. This consistency strengthens the study’s credibility and generalizability.
Limitations
The study’s Sample may not be representative of the entire population, as it only included individuals who were accessible and willing to participate. This sampling bias could limit the generalizability of the findings to a broader population. In addition, the data were collected within a specific timeframe, which may not capture changes in public perceptions or behaviors over time. The dynamic nature of the COVID-19 pandemic and evolving vaccine rollout strategies could affect the relevance and applicability of the findings in the future. Finally, our study focused on a specific country, and cultural, social, and economic factors specific to that context may influence the results.
Considering these strengths and limitations is essential when interpreting and applying the study findings. Further research with more extensive and diverse samples, longitudinal designs, and multi-country perspectives can provide a more comprehensive understanding of the factors influencing vaccine acceptance or refusal.
Policy Implications
The study emphasizes improving vaccine information dissemination and addresses vaccine safety and efficacy concerns. In addition, it emphasizes the importance of effective communication strategies in addressing vaccine hesitancy. Policymakers should address individuals’ concerns about the safety and efficacy of the COVID-19 vaccines. Efforts should be made before approval to provide clear and evidence-based information about the rigorous research, testing, and monitoring processes that vaccines undergo.
Given the influence of social media and traditional media on vaccine hesitancy, policymakers should collaborate with technology companies, media organizations, and fact-checking agencies to counteract the spread of false information and rumors. It is essential to strengthen public trust in healthcare professionals and scientific journals. This can be achieved through transparent and rigorous scientific processes, promoting the credibility, and expertise of healthcare professionals, and fostering trust in the scientific community through clear and consistent communication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the present study was obtained from the relevant institution. In addition, the nature of the study was explained to the participants as the requirement for their consent. They were informed that their participation was voluntary, they could withdraw from the study at any time, and the anonymity and confidentiality of the data were assured. Only those who agreed and consented to the ethical requirements and informed consent participated in the study. The consent form was placed on the first page of the online questionnaire.
Data Availability Statement
Data is available upon request from the corresponding author.