
Abstract
Conspiracy theory (CT) beliefs are thought to be related to a number of individual differences that make certain individuals more prone to this style of reasoning. In this study, we investigate (a) the relationship between CT beliefs and a standardized measure of judgment (the Bias Against Disconfirmatory Evidence task or BADE) and (b) the extent to which BADE scores are related to specific measures of psychopathology, including schizotypy and delusion-proneness, as measured by the Peters et al.’s Delusions Inventory. The BADE is an evidence integration bias and captures the extent to which individuals display a reduced willingness to integrate disconfirmatory evidence. A total of 358 individuals recruited from an online panel completed standardized measures of CT beliefs, measures of psychopathology, and a standardized BADE task. The results showed that CT-prone individuals showed a stronger BADE effect (i.e., biases against confirmatory and disconfirmatory evidence and a stronger liberal acceptance of absurd statements) and overall poorer evidence integration. Our results suggest that a reduced tendency to revise beliefs in the face of disconfirmatory evidence may contribute to the maintenance of CT beliefs, despite the availability of extensive counter-evidence.
Introduction
Conspiracy theories (CTs) are belief systems that propose that many events in the world are deliberately caused by purposive forces of agents working together to bring about outcomes that serve the interests of a higher power (van Prooijen, 2018). In most cases, these outcomes are inimical to the interests of the general public (Swami et al., 2017). Although some CTs (e.g., Watergate, Iran Contra Scandal, Pentagon Papers) appeared to have been justified and arose out of healthy skepticism, many forms of CT reasoning appear to be less functional or adaptive (Swami et al., 2014; Uscinski, 2018). CTs can lead to skepticism about the value of vaccinations, fluoridation of water, the cause of AIDS, and the truth behind mass shootings (e.g., the Sandy Hook Elementary School shooting in Connecticut, United States; Galliford & Furnham, 2017; Oliver & Wood, 2014). Research supports the view that there are individuals who are particularly prone to conspiracy style beliefs and that beliefs of this nature often tend to be correlated and clustered, which suggests the existence of CT style thinking as well as common CT preoccupations and constructs (Jolley & Douglas, 2014; Wood et al., 2012).
Different psychological explanations have been advanced to explain why some individuals appear more prone to these beliefs than others. According to van Prooijen and Douglas (2018), CT beliefs are likely to be strongly influenced by sociological factors. Groups or communities who are subject to political, social, or economic stress will look for explanations to explain their situation. According to these views, some CT beliefs can be seen as a natural human reaction to uncertainty, although many of the views might be incorrect or based on erroneous evidence. CTs tend to be resistant to falsification because believers tend to search confirmatory evidence rather than disconfirmatory evidence (McHoskey, 1995) and will often base their beliefs on more heuristic or emotion-driven reasoning styles rather than more analytical or systematic approaches (Swami et al., 2014). As a result of these findings, it has been found that erroneous beliefs can be reduced by greater information, better education, and by encouraging a more analytical reasoning style that establishes the validity of theories based on a balanced appraisal of evidence (van Prooijen, 2017). Such views suggest that CT beliefs appear to be less to do with psychopathology or mental illness and more to do with maladaptive reworkings or responses to uncertain or stressful situations (Anthony & Moulding, 2019; Goreis & Voracek, 2019; Swami et al., 2016; van Prooijen, 2018; van Prooijen & Douglas, 2018).
Although there is merit to the explanation of van Prooijen and Douglas (2018), a difficulty is that many CT beliefs appear to be quite extreme and irrational (e.g., beliefs in humanoid reptilians) and often appear to occur across multiple domains of knowledge. Thus, the person who is suspicious of governments or international bankers will also hold erroneous beliefs about well-established laws of science, or exaggerated suspicions regarding tainted water and food supplies (Jolley & Douglas, 2014; Lewandowsky et al., 2013). Such findings suggest people can demonstrate a more generalized “conspiracy thinking style,” which rather points toward the use of “a set” of common underlying cognitive processes. Importantly, there are a number of studies that have found correlations between endorsement of CT beliefs and elevated scores on measures of schizotypy, delusion-proneness (Barron et al., 2014, 2018), and related measures associated with maladaptive personality traits (i.e., callousness, narcissism, or excessive anomalistic beliefs; Brotherton et al., 2013; Bruder et al., 2013; Darwin et al., 2011). The relationship between CT belief and schizotypy, in particular, is thought to arise from schizotypal individuals being more open to arguments in support of CTs as a result of their suspiciousness of others and constant fear of the dangers posed by external factors and agents (Darwin et al., 2011; Holm, 2009).
Despite the debate about the relative importance of psychopathological factors in CT belief formation, there is general support for the view that cognitive biases play an important role (van Prooijen & Douglas, 2018; van Prooijen et al., 2018). People who believe in CTs engage in a lot of active searching for confirmatory information and likeminded individuals and tend to dismiss evidence that offers a contrary position (Freeman et al., 2002; Garety & Freeman, 1999; Johnson-Laird, 2006; Leman & Cinnirella, 2013; McHoskey, 1995). This type of behavior that appears to be prevalent in CT reasoning has been the focus of experimental studies and, in particular, has been applied to populations of people with clinical and subclinical conditions. It has been formally described as a Bias Against Disconfirmatory Evidence (BADE; Woodward, Moritz, & Chen, 2006; Woodward, Moritz, Cuttler, & Whitman, 2006). Although the concept has so far not been formally investigated in relation to conspiracy beliefs, it has been studied in relation to conditions (e.g., schizotypy and delusion-proneness) and related clinical disorders (e.g., schizophrenia) that are known to be related to a susceptibility to CT beliefs (Georgiou et al., 2019). The BADE is thought to contribute to the maintenance of delusions in clinical cases of schizophrenia (McLean et al., 2017; Sanford et al., 2014; Woodward et al., 2008) and some forms of delusional thinking. BADE tendencies have also been found to be associated with schizotypal traits (Orenes et al., 2012; Sanford et al., 2014; Speechley et al., 2012; Wood et al., 2012; Woodward, Moritz, Cuttler, & Whitman, 2006) and those who score higher on delusion-proneness as measured by the Peters’ Delusion Inventory (PDI; Balzan et al., 2014; Buchy et al., 2007; Woodward et al., 2006a, b). Within this literature, symptoms of psychosis (i.e., delusional thinking) are seen as dimensional in nature and are distributed along a “psychosis continuum” rather than being present only in clinical populations (van Os et al., 2009). Such research suggests that evidence of BADE effects will be observed in a significant proportion of the general population (Bronstein & Cannon, 2017; Buchy et al., 2007; Kaplan et al., 2016).
In support of this view, experimental research has sought to examine whether the people located across a supposed “psychosis spectrum” are susceptible to the BADE, by examining whether the phenomena exists in at-risk, subclinical populations who may experience psychosis-like symptoms (Menon et al., 2013; Woodward et al., 2006a, b, 2008). For example, it has been found that both nondelusional and nonclinical samples that possess certain schizotypal personality characteristics (i.e., magical thinking, hallucinated experiences, or ideas and delusions of reference) have been shown as more susceptible to the BADE effect compared with the general population (Eisenacher & Zink, 2017b; Menon et al., 2013; Orenes et al., 2012; Sanford et al., 2014; Speechley et al., 2012; Ward & Garety, 2019; Woodward, Moritz, Cuttler, & Whitman, 2006; Zawadski et al., 2012). Poorer performance on the BADE has also been associated with poorer analytical thinking (Bronstein et al., 2019) that has found to be a predictor of CT beliefs (Swami et al., 2014). Such findings are consistent with other literature that suggests that people who are prone to paranormal and other unusual beliefs may differ in their cognitive style (Williams & Irwin, 1991), or whether they have a greater need for consistency or “cognitive closure” (Leman & Cinnirella, 2013) or ways to make sense of uncertainty in the world (Hergovich et al., 2008; McKay et al., 2006, 2007).
The Present Study
Given the evidence that supports a connection between psychopathology (e.g., elevated scores on schizotypy and delusion-proneness) and CT beliefs, but also a similar connection between these traits and measures of the BADE, a question arises as to whether CT-prone individuals will score higher on BADE tasks. CT individuals would appear to display evidence of being prone to confirmatory bias influenced reasoning and often appear to adopt belief structures that appear difficult to falsify (McHoskey, 1995). However, static CT measures do not test for differences in judgment. Thus, it is important to understand whether CT-prone individuals display differences in how they consolidate evidence using a dedicated cognitive task. For this reason, a standardized BADE task may provide some useful insights into understanding individual differences that may make some people more prone to conspiracy style thinking.
Accordingly, a study was conducted in which participants drawn from an international online sample completed validated measures of CT beliefs and the BADE. It was hypothesized that higher CT beliefs will be positively associated with a resistance to modify commitment to existing information in the face of disconfirmatory evidence. To control for the fact that differences in BADE performance might be accounted for by other factors known to influence BADE performance (Balzan et al., 2012) and CT beliefs (Georgiou et al., 2019), we also included measures of psychopathology. These included the PDI and a measure of schizotypy. This enabled us to examine whether any association between CT beliefs and BADE performance still held after controlling for these related individual difference variables.
Method
Participants
A total of 358 participants (210 men, 148 women) with an age range of 18 to 80 (M = 25.16, SD = 13.18) years completed the study that had a cross-sectional design. Participants were drawn from a number of nations, with 80% from North America, the United Kingdom or Australia and another 20% principally from continental Europe. Participants reported varying degrees of education: non-high school completion (7%); 21.2% had completed high-school and 21.8% had completed a certificate or Diploma equivalent. Half had completed a bachelor’s degree or higher.
Sampling Procedure
The participant recruitment site Prolific was used to recruit participants from the general internet community. Participants completed the survey online for monetary compensation (just under Aus$10). Ethics approval was obtained from the Human Research Ethics Subcommittee in the University of Adelaide’s School of Psychology. The sample size was determined on the basis of achieving statistical power of 0.8 for correlational values of at least 0.2. The aim was to obtain at least 300 cases, but this was exceeded when the survey was closed in May 2018.
Study Design
The study design involved a single online survey and online judgment task. The survey included demographic questions and a range of psychological assessments as well as measures of CT belief. This study represents a companion piece for the previously published paper (Georgiou et al., 2019) that was principally focused on psychometric measures and which did not have the scope to examine any of the experimental evidence. Participants then completed a computerized version of the BADE.
Measures
Demographics
Several items of demographic information were collected, including their age, gender, highest level of education obtained, and nation of origin.
The Beliefs in Conspiracy Theory Inventory (BCTI)
This measure comprises 15 items and was developed by Swami et al. (2011). The measure captures a number of well-known CTs (i.e., “A powerful and secretive group, known as the New World Order, are planning to eventually rule the world”). Each item is rated from 1 (completely false) to 9 (completely true). Items are then summed to yield a total score, with higher scores indicating greater endorsement of CT beliefs. The internal reliability of the measure was very good in this sample (α = .87).
The Generalized Conspiracy Beliefs Scale (GCBS)
This measure was developed by Brotherton et al. (2013) and has 15 items. It measures general conspiratorial beliefs as opposed to the more specific beliefs captured by the BCTI (e.g., “Certain significant events have been the result of the activity of a small group who secretly manipulate world events”). The scale has been shown to have good test–retest reliability and content-criterion validity (Brotherton et al., 2013; Barron et al., 2018). Participants respond by rating statements on a 5-point scale from 1 (definitely not true) to 5 (definitely true). Scores can range between 15 and 75, with higher scores reflecting greater conspiracy ideation. The internal reliability for this study was very good (α = .83).
The PDI
This 21-item measure was developed by Peters et al. (2004) to capture delusion ideation in normal nonpsychotic populations. Each item requires participants to indicate Yes/No whether the statement applies to them. They are then asked to rate, on a scale of 0 to 5, how much distress the belief causes them (scores can range from 0 to 105) and the level of preoccupation with the thought (scores range from 0 to 105). Participants also rate how much they believe the thought to be true (scores from 0 to 105). Any item that is not endorsed is given a value of 0 for these three follow-up dimensions. A total score on the PDI is obtained by summating the yes/no scores and the scores on each dimension (scores from 0 to 336). The internal reliability for this measure in the present study was very good (α = .81).
The Schizotypy Personality Questionnaire–Brief Revised (SPQ-BR)
This measure, revised by Cohen et al. (2010), comprises 31 items that capture all nine diagnostic criteria for schizotypal personality disorder. Respondents have to indicate whether they agree with a range of beliefs on a 5-point scale with the following anchor points: 0 (strongly disagree) to 5 (strongly agree). Scores can range from 0 to 160, with higher scores indicating a greater likelihood of schizotypy. The SPQ-BR has three domains: cognitive-perceptual (CP), interpersonal (IP) and disorganized symptoms (DO). An abbreviated version of the SPQ is more often used for research and clinical screening purposes. The SPQ has been found to have good construct and convergent validity (e.g., Swami et al., 2017) and was found to have very good internal reliability in this sample (α = .89).
Cognitive task: The BADE task
The principal experimental task was a computerized version of the BADE test, originally devised by authors Woodward, Moritz, and Chen (2006) and Woodward, Moritz, Cuttler, and Whitman (2006). The current version consists of 16 written delusion-neutral scenarios that assess an individual’s persistence to hold certain beliefs in the face of disconfirmatory evidence. The BADE assessment involves participant ratings of the plausibility of four statements for their fit to a specified scenario, which is based on a single piece of information (i.e., “Jenny can’t fall asleep”). Each scenario had one true interpretation, two lure interpretations, and one absurd interpretation from the four statements. The plausibility of the four interpretations is rated for each scenario from a scale of 0 (poor) to 10 (excellent).
Each scenario starts with the statement (e.g., “Jenny can’t fall asleep”) and participants rate the four statements provided. After this initial round of ratings, a second piece of information is displayed (i.e., “Jenny can’t wait until it is finally morning”). The participants then rate the four statements again. This is repeated with a third and final piece of information (i.e., “Jenny wonders how many presents she will find under the tree”). The true interpretation (“Jenny is excited about Christmas morning”) appears uncertain initially, but becomes clearer as additional information is revealed (e.g., “Jenny is nervous about her exam the next day”), which should prompt the participant to update their choices. Meanwhile, the lure interpretations appear plausible initially, but become increasingly less implausible as additional information is revealed (e.g., “Jenny loves her bed”). Of the 16 trials, three were “fillers” where the true interpretation appears to be plausible after the first statement is presented, which reduces the tendency for participants to develop a response strategy of identifying the “true” interpretation from the outset; these filler trials were not analyzed.
Statistical analysis
Prior to commencing analyses, the data were screened to determine its suitability for parametric testing. Ten scores on the PDI and the SPQ-BR were found to be outliers through the examination of box plots and stem-and-leaf plots. An inspection of their standardized values found that all were extreme cases, exceeding the +3SD above the mean. The examination of the data suggested all variables were normally distributed and parametric assessment was suitable. Analysis was conducted using version 24 of IBM SPSS Statistics software. Pearson’s r correlation analysis was used to examine the relationship between performance on the BADE and the psychometric measures.
BADE calculations followed the methods recommended in the meta-analysis conducted by McLean et al. (2017). Similar methods are used in Woodward et al. (2007) and other papers, including Eisenacher and Zink (2017a) and Prike et al. (2018). First, BADE was calculated by examining the difference between the first lure ratings and final lure ratings across the scenarios (Neutral Lure 1 − Neutral Lure 3 and Emotional Lure 1 − Emotional Lure 3). The values capture the decrease in endorsement of the lures following the presentation of additional evidence. A greater decrease indicates a smaller BADE effect. Second, we calculated a BACE (Bias Against Confirmatory Evidence) metric by calculating the difference between ratings for the third and first true ratings across all scenarios (True 3 − True 1). Smaller values indicate greater BACE and that participant endorsement of truthful statements did not increase as strongly in the face of additional supporting evidence. One would therefore expect a negative association between these scores and other measures that are hypothesized to capture a greater BADE effect. We also calculated a measure of “liberal acceptance” based on the mean of the absurd ratings across all scenarios to capture how willing participants were to endorse absurd or generally implausible interpretations. Liberal acceptance was expected to positively correlate with belief measures.
A final metric was an evidence integration score (as recommended by correspondence with Professor Woodward). This was based on the sum of the ratings given to absurd ratings, the erroneous statements at the third administration and by subtracting the rating of the final true statement: Evidence Integration = [Absurd rating at Statement 1 + Absurd rating at Statement 2 + Absurd rating at Statement 3 + Neutral lure rating at Statement 3 + Emotional lure rating at Statement 3] + [True rating at Statement 3 × − 1]. The values summed were the Z-values calculated for each statement after we had determined the mean for each statement type across the scenarios. Higher scores on this measure indicate poorer Evidence Integration.
Pearson’s correlation analysis was used to examine the relationship between the principal measures. Multiple regression was then used to examine whether evidence integration scores on the BADE correlated with CT beliefs after controlling for education and psychopathology measures.
Results
Demographics
Demographic differences in CT beliefs were initially analyzed to understand whether factors such as age or gender might need to be controlled in subsequent analyses. One-way analysis of variance (ANOVA) showed that there were no age group differences in CT belief scores F(5,342) < 1. Welch independent-samples t test also indicated no significant gender differences, t(346.77) < 1.
Descriptive Statistics
A summary of descriptive statistics for the sample is provided in Table 1. The results indicate that most respondents scored in the lower possible range of the PDI, but that scores ranged up to as high as 268 of 360. Schizotypy scores generally fell within the mid-range of possible scores. Mean GCBS and the more specific BCTI scores were generally below the mid-point of the scale, with scores ranging from the minimum (no endorsement of conspiracy beliefs) up to scores which were very close to the maximum. We found no differences due to age or gender, but scores on both conspiracy scales were significantly lower for the U.K. respondents than for the other groups (mean of 30.0 for the GCBS and 40 for the BCTI).
Descriptive Statistics for Principal Psychological Measures (n = 348).

Note. PDI = Peters’ Delusion Inventory; SPQ-BR = Schizotypy Personality Questionnaire–Brief Revised; GCBS = Generalized Conspiracy Beliefs Scale; BCTI = Beliefs in Conspiracy Theory Inventory.
Correlations Between Psychometric Measures
Table 2 shows the Pearson’s correlations between the psychometric measures. Both psychopathology measures (PDI and schizotypy) were positively correlated with each other and positively associated with both CT scales. The two CT scales were highly correlated.
Correlations Between Psychometric Measures.

Note. PDI = Peters’ Delusion Inventory; SPQ = Schizotypy Personality Questionnaire; BCTI = Beliefs in Conspiracy Theory Inventory; GCBS = Generalized Conspiracy Beliefs Scale.
p < .05. **p < .01.
Correlation Analysis of BADE Performance and Other Measures
Table 3 summarizes the correlation between the different BADE-derived measures and the psychometric measures. Both BADE and BACE measures (for lure and true difference scores, respectively) showed a similar pattern of results, where those who scored higher on conspiracy or delusional-like belief measures were less likely to update their endorsement of lure and true interpretations in the face of new evidence (i.e., less down-rating of lures and less up-rating of true interpretations from Statements 1 to 3). Liberal acceptance was positively related to all the measures, with the largest effects being observed for the PDI and the BCTI (specific conspiracy beliefs), suggesting these beliefs were associated with a tendency to accept or endorse implausible hypotheses. Finally, as expected, the Evidence Integration measure positively correlated with conspiracy belief measures (i.e., poorer integration of evidence) and the PDI.
Correlation of BADE-Derived Metrics and Self-Report Measures.
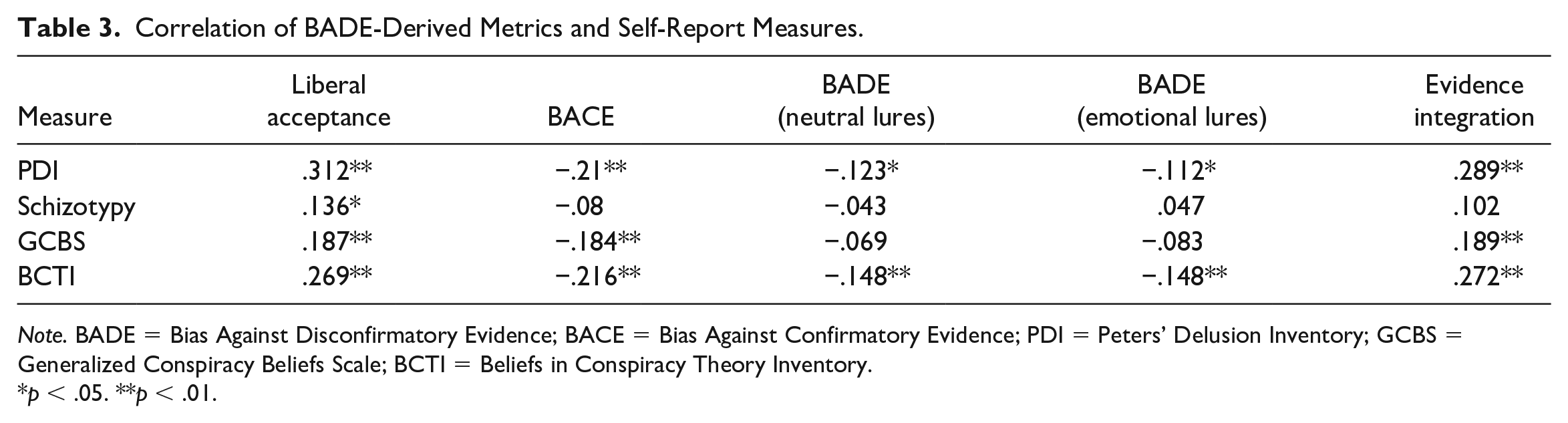
Note. BADE = Bias Against Disconfirmatory Evidence; BACE = Bias Against Confirmatory Evidence; PDI = Peters’ Delusion Inventory; GCBS = Generalized Conspiracy Beliefs Scale; BCTI = Beliefs in Conspiracy Theory Inventory.
p < .05. **p < .01.
Multiple Regression
The overall BADE Evidence Integration score was used as the principal measure for this final analysis because it consolidated much of the information in the other measures. Given the association between the Evidence Integration measure and other measures (e.g., PDI and SPQ), it was important to examine whether the association between the BADE and BCTI scores still held after controlling for the other measures. Table 4 summarizes the results of a hierarchical multiple regression. Education was entered on the first step (Model 1), the psychopathology measures on Step 2 (Model 2), and evidence integration on Step 3 (Model 3). As shown, the addition of the PDI and SPQ measures in Model 2 explained 21% of variance. Addition of the BADE Evidence Integration variable in Model 3 explained an additional 1.6% of variance (quite small), but this measure remained significant after controlling for the other variables.
Hierarchical Regression: Predictors of Conspiracy Belief (BCTI Scores).

Note. BCTI = Beliefs in Conspiracy Theory Inventory; SPQ-BR = Schizotypy Personality Questionnaire–Brief Revised; PDI = Peters’ Delusion Inventory; EI (BADE) = Evidence Integration measure from Bias Against Disconfirmatory Evidence.
p < .05. **p < .01.
Discussion
Previous work has suggested that the BADE is associated with psychopathological characteristics (e.g., schizotypy and delusion-proneness) that have been shown to be associated with measures of CT beliefs. Accordingly, the aim of this study was to investigate whether individuals who hold more conspiratorial beliefs display a poorer ability or unwillingness to update their beliefs based on new information in a structured task. Overall, the results were consistent with the principal hypothesis. People who scored higher on CT belief measures displayed a stronger BADE effect, characterized by a stronger BADE (i.e., down-rating lures), confirmatory evidence (i.e., up-rating true interpretations), and greater liberal acceptance (i.e., acceptance of absurd or implausible hypotheses). There were also shown to have overall poorer Evidence Integration, a metric that combines these three effects. Such findings appear consistent with the previously documented connection found between specific psychopathological conditions known to predict either poorer performance on the BADE (Woodward et al., 2007; Woodward, Moritz, & Chen, 2006) or stronger endorsement of CT beliefs (Georgiou et al., 2019). The results also confirm the findings of Prike et al. (2018) who found that poorer performance on the BADE task was associated with stronger endorsement of anomalistic beliefs.
These findings support the view that people who score more highly on CT beliefs are more likely to score higher on specific subclinical psychopathological traits than others. These traits make individuals more prone to perceiving casual connections between events or actions and behaviors that are not perceived by others (van Prooijen et al., 2018). Once such connections are established, CT-prone individuals may be less motivated to alter their beliefs because they receive reinforcement from others with similar views and because this creates a feeling of dissonance. The results obtained using the BADE show that CT-prone individuals appear to have less ability to alter their views once they have become fixed on an initial hypothesis. However, whether this is due to differences in how the task is initially perceived or to do with how subsequent information is integrated afterward remains clear. Consequently, this remains an important area for further investigation with more refined experiments.
These findings, which emphasize the role of cognitive factors in the etiology of conspiracy beliefs, should not, however, be seen as sitting in opposition to the views of van Prooijen (2018) and others who have emphasized the role of sociological factors and education. On the contrary, we support the view that social factors such as feelings of uncertainty, powerlessness and suspicion as well as poorer education are all factors that are likely to make people more prone to CT beliefs. However, our view is that certain people in society are more likely than others to be drawn to these beliefs because of dispositional or psychopathological factors. In particular, we argue that those who fall in the clinical or borderline range on measures such as schizotypy are particularly at risk. Individuals who fall into these subclinical groups appear to process information, and integrate it, differently. This may due to a greater desire for certainty or “cognitive closure” (Leman & Cinnirella, 2013), differences in causal reasoning, or a coping strategy where adhering to fixed views is a way to allay fears and uncertainty about aspects of their life (Schumaker, 1987; Williams & Irwin, 1991).
Several factors need to be taken into account when interpreting these findings. Although attempts were made to obtain an international sample from the broader community and to use standardized and structured measures validated in other published studies, it is important to note that different findings might be obtained in the results were undertaken using different cultural groups. For example, it is not clear whether people from Asia or those living in other non-English-speaking countries would respond to the measures the same way. Second, we cannot rule out the possibility that some individuals may have possessed other unmeasured co-morbid conditions that might have influenced the results. A third potential limitation of the current study that could be addressed in future research is that the content and presentation of the 16-item BADE assessment may not necessarily reflect real-world scenarios that prompt the judgment processes responsible for CT belief. In addition, the themes themselves used in the BADE task could be remodeled to focus on more emotionally relevant topics relevant to CT beliefs so that Emotional-lure (EL) and Neutral-lure (NL) statements would mirror themes common within most CT structures (i.e., political collusion, insidious threat to self). It is possible that using more realistic scenarios may strengthen the magnitude of the effects observed. Nevertheless, the fact that we were able to demonstrate small to moderate-sized effects using a standardized and more neutral test is also informative and strengthens the view that BADE is potentially measurable behavioral tendency observable in populations that are more prone to CT beliefs.
Conclusion
The results showed that the BADE was a useful measure for detecting individual differences in people’s susceptibility to conspiracy beliefs. It confirms that CTs are likely to arise from differences in how people process information and that this is related to underlying differences in mental health functioning. The findings strengthen the view that enhancing people’s skills in analytical and critical reasoning may be beneficial in reducing the strength of these beliefs. People need to be encouraged to consider wider sources of information when making judgments about the nature of people and events (Prike et al., 2018). They need the skills to recognize biases in their logic, to reflect upon their initial judgment and be willing to update their impression based upon additional important. Some of this may come from education and public health messaging (e.g., “read widely,” fake-news awareness, consumer protection/information awareness). Other useful skills might emerge from work conducted in clinical contexts (e.g., Ward & Garety, 2019) where people are taught how to avoid jumping to conclusions using reflective techniques or meta-cognitive strategies (e.g., “have I thought of alternatives?”) or think more analytically rather than based on emotion or simple heuristic rules.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.