
Abstract
Keywords
Introduction
Family quality of life (FQoL) is defined as conditions where the family’s needs are met, and family members enjoy their life together as a family and have the chance to do things which are important to them (Park et al., 2003). This concept is of utmost importance for both individuals and families (Zimmerman et al., 2022). In recent decades, the FQoL framework has been applied to various samples, including families of individuals with disabilities (Múries-Cantán et al., 2023), adolescents transitioning to adult care in the context of illness (Zimmerman et al., 2022), and families with young special needs children (Rivard et al., 2023). Findings from these studies offer theoretical insights and empirical knowledge on enhancing the FQoL of vulnerable groups.
Herein, rehabilitation patients are individuals undergoing a rehabilitative process to recover from injury, illness, or disability. As a vulnerable population, they have garnered increased research attention in recent years (Francis et al., 2019; Panzeri & Ferrario, 2020). Rehabilitation patients rely on additional care and support from their family members throughout their treatment and recovery, whether at home or in rehabilitation facilities. This places a significant burden on family members’ energy, finances, and time, potentially diminishing the family unit’s overall FQoL (Radina, 2013). Consequently, researchers have long recognized the criticality of family life quality for recovering patients’ well-being, often considering improved family life quality as the ultimate objective of rehabilitation and treatment (Pain et al., 1998; Radina, 2013).
In recent years, the FQoL construct has been applied within the realm of rehabilitation. Existing studies have explored various factors influencing FQoL, including pathological elements (Ammann-Schnell et al., 2021), demographic factors (Glinac et al., 2017), psychological factors (Vitorino et al., 2021), and rehabilitation-related factors (Ravens-Sieberer et al., 2001). However, comprehensive investigations encompassing this array of influencing factors have been scarce. Hence, further research in the field of rehabilitation is warranted to comprehensively examine the factors influencing FQoL and better assist families of recovering patients in navigating the challenges encountered during this critical period.
Notably, the Global Burden of Disease Study on Rehabilitation, published by The Lancet in 2020, revealed that the total number of individuals in need of rehabilitation in China exceeds 460 million, a significant portion of whom rely on their families’ presence and support. Given China’s large population of rehabilitation patients and the importance of FQoL, this study explores the factors influencing the quality of life among families of rehabilitation patients in China.
Literature Review
FQoL and its Application in Vulnerable Groups
The body of literature on FQoL has grown both conceptually and empirically since the concept first appeared in the late 1990s (Bailey et al., 1998). This multidimensional construct has been defined in various ways, encompassing the general notion of “the goodness of family life” (Brown & Brown, 2004, p. 29) and, more specifically, “a dynamic sense of well-being of the family, collectively and subjectively defined and informed by its members, in which individual and family-level needs interact” (Zuna et al., 2011, p. 262). Multiple validated measures have been developed to investigate FQoL and its determining factors (Hu et al., 2011). This study utilized the Beach Center Family Quality of Life Scale (Summers et al., 2005). This scale was derived from a qualitative grounded theory study that explored the perspectives of families of children and youth with disabilities regarding the meaning of FQoL (Poston et al., 2003). According to this measure, FQoL is defined as the “[conditions] where the family’s needs are met, and family members enjoy their life together as a family and have the chance to do things which are important to them” (Park et al., 2003, p. 368).
The theory of health-related family quality of life (HR-FQoL) extends the concept of FQoL to the domain of disease and disability. The Beach Center’s work specifically addresses how FQoL relates to illness and disability in families with disabled children (Radina, 2013). Scholars commonly used the scale to evaluate the effectiveness of family support (e.g., family interaction, parenting, emotional well-being, physical/material well-being, and disability-related supports) for family members with disabilities and illness and assess subjective satisfaction with family life (Summers et al., 2005), for which its validity and reliability have been confirmed and refined. As such, it is theoretically reasonable to incorporate an FQoL perspective into research on rehabilitation patients.
Factors Affecting Family Quality of Life for Vulnerable Groups
Research focusing on FQoL among rehabilitation patients is limited. However, studies of the FQoL of other vulnerable populations, such as disabled individuals and patients, can provide valuable insights. Existing studies categorize the factors influencing the FQoL of disabled individuals into several domains, including pathological factors, demographic factors, psychological factors, and rehabilitation factors.
Studies focusing on pathological factors have examined the impact of specific diseases on FQoL. For instance, Golics et al. (2013) conducted semi-structured interviews with 133 family members of mostly chronically ill patients, revealing the significant, yet similar, impacts illness can have on the FQoL of patients’ family members. Ammann-Schnell et al. (2021) used a semi-standardized questionnaire to investigate the effect of rare and severe neurological disorders on parents’ FQoL and their families’ everyday lives, while a study concerning parents of children with sickle cell disease (SCD) found a negative association between the conditions of SCD and parents’ quality of life (Al Jabri, 2023). These studies consistently highlight the substantial impact of disorder severity on FQoL and the emotional strain experienced by family members.
Demographic factors have also been found to influence FQoL, primarily through caregiver stress. Mothers of children with spina bifida, for example, tend to experience increased levels of stress as their child ages and the effects of the disorder become more apparent (Datta et al., 2002; Kyzar, 2010). Additionally, the quality of life for families with chronically ill patients is significantly affected by demographic factors such as education level, income, age, and level of family support (Glinac et al., 2017). The current body of research predominantly employs HR-FQoL theory as a conceptual framework to assess the FQoL of individuals with disabilities (Radina, 2013). However, it is important to acknowledge that family members may have varying perceptions of FQoL (Mellon, 2002); therefore, exploring subjective perceptions of FQoL from patients’ perspectives is valuable.
Psychological factors have been strongly correlated with quality of life in numerous studies (Ajayi, 2021; Han, 2022; Vitorino et al., 2021). Ajayi (2021), for example, investigating individual psychological factors as predictors of FQoL among civil servants, found that psychological functioning and perceived stress were significant independent predictors of FQoL. Similarly, Glinac et al. (2017) found that anxiety and depression significantly impacted individuals’ satisfaction with their quality of life in the context of chronic diseases. In another study involving 1156 community-dwelling adults, Vitorino et al. (2021) explored the negative correlation between mental health (including depression, anxiety, optimism/pessimism, and spiritual/religious coping) and quality of life. While much of the research on psychological factors and FQoL among disabled populations has focused on negative psychological factors, such as anxiety and depression, it is important to consider both positive and negative psychological variables. For example, other studies have shown the beneficial effects of dispositional gratitude (Valikhani et al., 2019) and mindfulness (Han, 2022) on quality of life, because it helps better feel the emotions of family members and form a more harmonious family atmosphere.
Regarding rehabilitation factors, Pain et al. (1998) emphasized that the ultimate goal of rehabilitation therapy is to aid patients in recovering faster and better while enhancing their overall quality of life. Rehabilitation has positive effects on both individuals and their families; for instance, Aprile et al. (2008) examined the quality of life of stroke patients after rehabilitation and found significant improvements in physical and social functions. Chouksey et al. (2023) conducted a follow-up study on patients with maxillary defects and found significant enhancement in their quality of life after the use of surgical obturators. Umunnah et al. (2023) compared the quality of life of persons living with disabilities before and after a community-based rehabilitation program, finding that it improved significantly after the program. However, while research has steadily demonstrated the effectiveness of rehabilitation on FQoL, little research has systematically examined and compared the impact of different rehabilitation factors (e.g., duration, methods) on FQoL. Exploring the influence of rehabilitation factors on the FQoL of rehabilitation patients’ families in the rehabilitation group is a meaningful step toward filling this research gap.
Overview of Literature and the Current Study
In summary, existing research has established that pathological, demographic, and psychological factors and rehabilitation effects influence individuals’ quality of life, providing a foundation for investigating how these might also impact FQoL. However, most empirical studies have focused on vulnerable groups such as patients, disabled individuals, and their caregivers, with limited attention given to rehabilitation patients. Extending this line of inquiry to the context of rehabilitation can enhance our understanding of factors influencing FQoL. The current research primarily concentrates on the impact of rehabilitation effects on patients with specific diseases, neglecting the examination of rehabilitation methods, duration, and other factors that may influence FQoL among rehabilitation patients, with few studies comparing these effects between different rehabilitation patient populations. In light of these gaps, this study’s main objective is to investigate the factors influencing FQoL among rehabilitation patients in mainland China. Based on the literature, three research hypotheses are proposed:
Hypothesis 1: Demographic variables, including gender, income, age, education, and occupation, will significantly affect FQoL.
Hypothesis 2: Psychological variables, such as psychological stress, will have a significant negative effect on FQoL, while positive factors like family interactions and grit will positively influence FQoL.
Hypothesis 3: Rehabilitation factors, such as treatment modalities, duration of rehabilitation, and satisfaction with rehabilitation, will significantly affect FQoL.
Methods
Participants
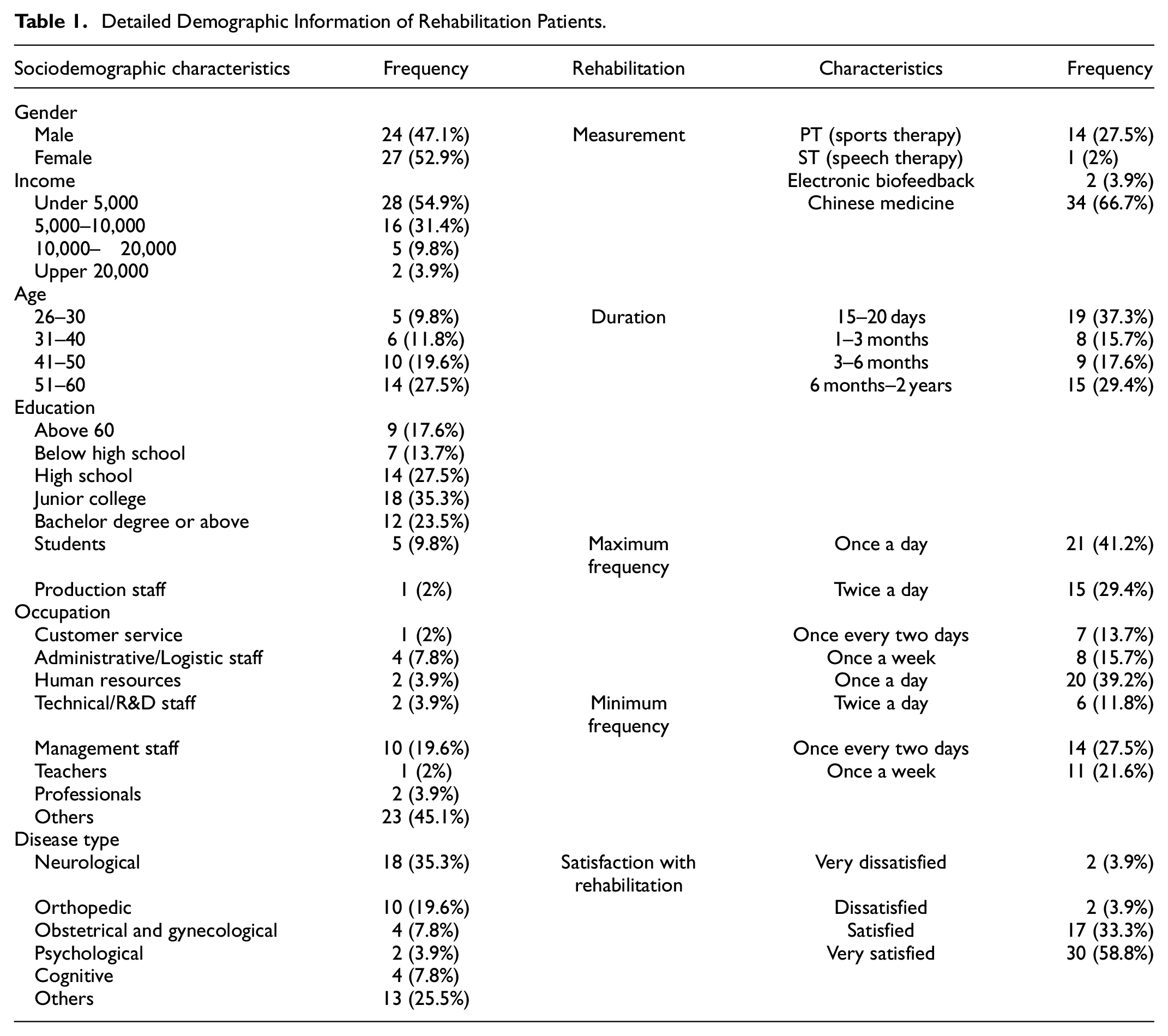
The participants in this study were recruited from various locations within Shandong Province in mainland China, conveniently selected from rehabilitation centers in the area. The number of rehabilitation patients in these institutions was limited, with a total of 51 rehabilitation patients (average age 40) being included in the final research cohort. See Table 1 for the participants’ detailed demographic information. In the whole sample, the highest proportion of patients had neurological issues (N = 18, 35.3%), and the lowest proportion had psychological issues (N = 2, 3.9%). More than half (N = 34, 66.7%) chose the traditional rehabilitation treatment modality, Chinese medicine, while nearly one-fifth of participants preferred exercise therapy (N = 14, 27.5%). The patients’ main treatment and rehabilitation durations were short-term (15–20 days, N = 19, 37.3%) and long-term (6 months–2 years, N = 15, 29.4%).
Detailed Demographic Information of Rehabilitation Patients.
Measures
A demographic sheet, a sheet concerning rehabilitation, and the four inventories mentioned above were used to collect data. The sociodemographic characteristics addressed included a person’s gender, age, education level, monthly household income, and occupation.
Five aspects of rehabilitation characteristics were examined: (a) type of disease (e.g., neurological, orthopedic, pediatric, obstetrical and gynecological, psychological, cognitive, etc.), (b) therapeutic tools used in rehabilitation (e.g., sports therapy, speech therapy, electronic biofeedback, Chinese medicine), (c) duration of rehabilitation treatment (e.g., 15–20 days, 1–3 months, 3–6 months, 6 months–2 years), (d) maximum or minimum frequency of rehabilitation participation (e.g., once a day, twice a day, once every 2 days, once a week), and (e) satisfaction with rehabilitation results (very dissatisfied, dissatisfied, neutral, satisfied, very satisfied).
The Psychological Stress Questionnaire
To gain insight into the psychological stress experienced by individuals undergoing rehabilitation, we used the Psychological Stress Questionnaire, a new, self-report, five-point Likert scoring inventory developed by Wang et al. (2020) in relation to the COVID-19 pandemic. The scale comprises nine items assessing three dimensions: (a) risk awareness, which captures the subject’s self-assessment of their resilience toward environmental risk (example statement: “I am highly vigilant and defensive”); (b) physiological and psychological response, which uncovers the subject’s stress response to their immediate surroundings (example statement: “When negative thoughts arise, my heart rate increases and I experience physical discomfort”); and (c) optimistic hope, which mirrors the subject’s confidence in overcoming the epidemic and maintaining optimism during the current outbreak (example statement: “My general mood tends to be predominantly positive”). In this study, the scale’s internal consistency reliability was 0.80, consistent with that of Wang et al. (2020).
The Chinese Version of the Multidimensional Scale of Perceived Social Support (MSPSS-C)
To assess the influence of social support on rehabilitation, we employed the MSPSS, a 12-item scale used to evaluate individuals’ perceptions of the social support they receive from their family, friends, and significant others. Participants are asked to rate their agreement using a seven-point Likert-type scale, ranging from “strongly disagree” to “strongly agree” (Chou, 2000). Three sample items are: “There is a special person who is around when I am in need,”“My family really tries to help me,” and “I can count on my friends when things go wrong.” The MSPSS has been translated and back-translated into Chinese by bilingual professional translators Chou (2000), with both versions demonstrating good reliability and validity (Chou, 2000).
The present research adopted the MSPSS-C. The term “special person” was replaced with “friends,” as the former may be difficult to understand, and participants’ support came mostly from family and friends, consistent with Cheng and Deng’ s (2023). The alpha coefficient for the adapted MSPSS-C was .97.
Self-Reported Short Grit Scale (Grit-S)
To assess rehabilitation patients’ level of perseverance, we employed the Short Grit Scale (Grit-S), a self-report measure developed and validated by Duckworth and Quinn (2009). The Grit-S consists of two subscales: perseverance of interest and perseverance of effort. The scale is comprised of eight items, with example statements such as “I am able to stay focused under pressure (perseverance of effort)” and “I can always stick to the things I love (perseverance of interest).” Participants were asked to evaluate each item on a five-point Likert scale, ranging from 1 = “not at all like me” to 5 = “very much like me.” The Chinese version of the Grit-S has demonstrated good reliability, as verified by Li et al. (2018). Previous studies have reported Cronbach’s α values of .73 to .83 for the self-reported scale. The subscales’ Cronbach’s αvalues ranged from .58 to .71 in China and demonstrated good reliability in the current study (α = .732).
Beach Center Family Quality of Life Scale
We utilized the Beach Center Family Quality of Life Scale (Hoffman et al., 2006) to evaluate the quality of life of families. This scale gauges the level of satisfaction of the respondents with various aspects of family life that may influence the overall quality of life. The scale comprises five domains, encompassing a total of 25 items. For instance, example statements include “My family enjoys spending time together” (family interaction, five items); “Family members help the children learn to be independent” (parenting, five items); “My family has the support we need to relieve stress” (emotional well-being, five items); and “My family gets medical care when needed” (disability-related support, five items). A five-point Likert-type scale ranging from 1 (very dissatisfied) to 5 (very satisfied) is employed as a response options. To obtain a total score, the mean score for all 25 items is calculated. Domain scores are determined by calculating the mean of the items within each domain. The overall Cronbach’s alpha for the scale was reported as .88 by Hoffman et al. (2006), and a subsample of participants demonstrated significant test-retest reliability after 3 months. In this study, Cronbach’s alpha was calculated as .978, indicating good reliability.
Procedures
The study received ethical approval from the Institutional Review Board. Researchers initiated communication with rehabilitation centers across Shandong Province in mainland China and obtained their consent. Subsequently, participants in the rehabilitation centers were provided with detailed information about the survey, emphasizing its potential advantages. Rehabilitation patients were then guided to scan the QR code on the questionnaire and encouraged to complete it at their convenience. A total of 51 individuals who had completed rehabilitation participated in the survey, all of whom provided valid responses (100% completion rate).
Before participating, all study participants were required to provide informed consent, emphasizing their voluntary participation and the confidentiality of the information collected. The demographic sheet and four inventories were completed online, taking approximately 20 min. As a token of appreciation, participants received random red packets with a one-in-three chance of containing a reward, as previously communicated.
Data Analysis
SPSS 21.0 and STATA 15 were used to analyse the data in the present study. There were no missing data, as the survey was conducted online, and only fully completed surveys could be submitted.
The reliability values for the four inventories mentioned above were first estimated using Cronbach’s alpha coefficient. Descriptive statistics were also calculated. Data screening was conducted, including analyses of “frequency” and “explore.” Furthermore, assumptions of homogeneity of variance and normality were examined. If these assumptions were met, a Multivariate Analysis of Variance (MANOVA) would be conducted. However, in the case of non-homogeneous variances, a series of Kruskal–Wallis (K–W) tests were performed to investigate the relationship between demographic variables and rehabilitation patients’ FQoL.
Finally, linear regressions were conducted to predict the FQoL from grit, psychological, and MPSS with relevant demographic factors being controlled for; specifically, multiple regressions were performed separately for each of the five dimensions of FQoL.
Results
Descriptive Statistics and Normal Distribution Test
Descriptive analyses were conducted. Means and standard deviations for each scale of parenting style, parental involvement, and psychological stress measures are reported in Table 2. Since this study adopted face-to-face questionnaire collection, there were no missing samples.
Means (M) and Standard Deviations (SD) of Psychological Distress, FQoL, Social Dupport, and Grit.

Given the relatively small sample size of this study, the Shapiro-Wilk test was utilized to evaluate the normality of the data. The results indicated that the data did not adhere to a normal distribution (w = 0.86, p < .05).
Demographic Factors on Family Quality of Life
Due to the small sample size and non-normal distribution of the data (w = 0.86, p < .05) in this study, the Kruskal–Wallis (K–W) test was employed to investigate the heterogeneity of FQoL concerning age, education level, income, occupation type, and disease type. This section addresses Hypothesis 1. Though there were no significant differences in demographic variables in FQoL statistically, we can still make a preliminary analysis based on the approximate differences in means.
First, there was no significant difference in FQoL and its various dimensions in terms of age. However, upon comparing means, it was found that those aged 26 to 30 undergoing rehabilitation exhibited a slightly higher FQoL score than other age groups.
Second, an examination of mean values revealed that those with a high school education or below rated their FQoL the highest. They reported being the most cared for within their families, experiencing no life pressures or economic burdens. Participants with a bachelor’s degree or higher education ranked second, reporting stable, well-paying jobs and attention to family interactions. Conversely, individuals with a high school education or a junior college education rated their FQoL the lowest.
Figure 1 illustrates the impact of income on FQoL. The middle-income group (earning between 10,000 and 20,000) reported the highest levels of FQoL, with a mean score of 4.97 ± 0.42. The high-income group (earning above 20,000) followed with a mean score of 4.2 ± 0.74. Conversely, the low-income group (earning less than 5,000) reported the lowest level of FQoL, with a mean score of 4.04 ± 0.92. Notably, the middle- and upper-income groups displayed higher levels of family interaction, parenting, and physical and mental health. Families in the high-income group scored high on all dimensions except for family interaction.
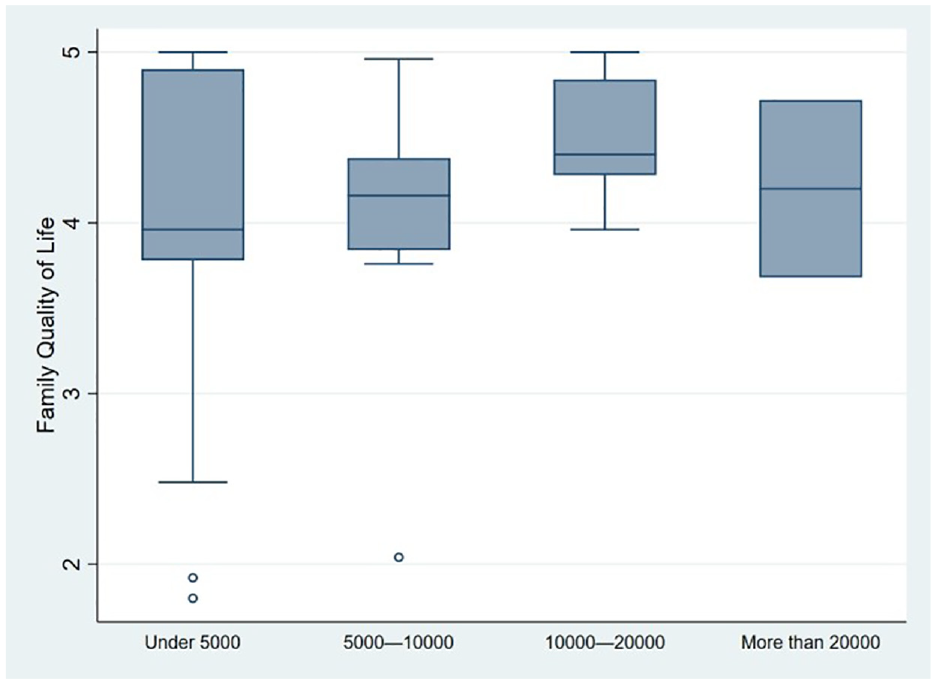
FQoL of families with different income.
In terms of the impact of patients’ occupations on FQoL, teachers reported the highest FQoL (mean score = 4.84), followed by administrative staff (mean score = 4.59 ± 0.53) and technicians (mean score = 4.34 ± 0.08).
Figure 2 illustrates the effect of disease type on FQoL. Pediatric rehabilitation patients were excluded from the sample as they were unable to complete the test independently. Comparative analysis revealed that patients with “other” diseases (mean score = 4.26 ± 0.71) reported the highest FQoL, followed by those with neurological diseases (mean score = 4.32 ± 0.77) and orthopedic diseases (mean score = 4.18 ± 0.72). Furthermore, families of individuals with mental illness (mean score = 2.94 ± 1.44) reported the lowest FQoL. It is noteworthy that patients with mental illness reported the lowest FQoL across all dimensions.

FQoL of families with disease.
Psychological Factors on Family Quality of Life
In analysing the variability of FQoL concerning psychological factors, this study addressed Hypothesis 3. The regression results revealed that two dimensions of psychological factors, namely risk awareness and physical and mental responses, had significant effects on all dependent variables except disabled support. Risk awareness negatively predicted FQoL (β = −.34, p = .007), family interaction (β = −.34, p = .008), parenting (β = −.389, p = .008), emotional well-being (β = −.32, p = .025), and physical and material well-being (β = −.41, p = .005). Among the dimensions of the Multidimensional Scale of Perceived Social Support (MSPSS), only family support was found to significantly affect FQoL (β = .28, p = .046), with other dimensions showing no significant impact. Regarding rehabilitation patients’ grit, perseverance was found to predict FQoL (β = .29, p = .007), family interaction (β = .34, p = .002), parenting (β = .33, p = .007), and physical and material well-being (β = .27, p = .03). Consistency, however, only had a positive impact on FQoL (β = .16, p = .034).
Rehabilitation Factors on Family Quality of Life
In addressing Hypothesis 4, the study examined the effects of rehabilitation treatment, duration, and satisfaction on FQoL by the K–W test. However, post hoc tests could not be conducted due to small sample sizes for e-biotherapy and speech therapy. Even after excluding these two types of samples, the K–W test did not reveal significant differences (p > .05). Though this study aimed to include as many existing rehabilitation methods as possible in the questionnaire design, the results indicated that patients primarily selected exercise therapy (PT), speech therapy (ST), electronic biofeedback, and traditional Chinese medicine. Figure 3 illustrates that patients undergoing electronic biofeedback therapy (mean score = 4.44 ± 0.57) and exercise therapy (mean score = 4.27 ± 0.80) reported the highest FQoL. Those using Chinese medicine therapy (mean score = 4.08 ± 0.74) had moderately high scores. Conversely, patients receiving speech therapy (mean score = 2.04) had the lowest scores on the total dimension and all subdimensions of FQoL (Figure 3).

FQoL of families with treatment.
The K–W tests for treatment duration (F = 1.812, p = .16) did not yield significant differences. Examining the impact of recovery time as shown in Figure 4, it was observed that the highest FQoL was reported when the recovery time was the shortest (M = 4.13 ± 0.51) or the longest (M = 4.31 ± 0.51).

FQoL of families with treatment duration.
A positive relationship was found between rehabilitation satisfaction and FQoL, indicating that higher rehabilitation satisfaction corresponded to higher FQoL (mean = 4.256 ± 0.67). Linear regression results demonstrated a significant positive predictive effect of rehabilitation satisfaction on their FQoL (β = .27, p< .05). Finally, regression analysis was employed to further examine the influence of rehabilitation treatment and rehabilitation time on FQoL. However, the regression results did not yield significant findings.
Discussion
The current study explored the influence of demographic, psychological, and rehabilitation factors on rehabilitation patients’ FQoL.
First, regarding demographic factors, it was found that middle-class participants had the highest FQoL and better family interactions, parenting style, and physical and mental health. This could be attributed to the specific occupational distribution of the Chinese middle class, which typically includes teachers, administrators, and technical personnel. These individuals typically hold Bianzhi status (i.e., are officially identified as civil servants), which comes with various benefits such as wages, subsidies, and endowment insurance that are significant in the Chinese government’s human resource administration systems (Zhou et al., 2015). Middle-class participants had relatively stable employment and substantial income; they were not at risk of losing their jobs even if they needed to stay in a rehabilitation center for an extended period. They were also not burdened with the risk and stress of unemployment, as their basic livelihood was guaranteed. Consequently, they had ample time to spend with their families. This finding aligns with the results of Glinac et al.’s (2017) study, which demonstrated that respondents with a higher financial status reported better quality of life than those with medium or poor financial status. Glinac et al. (2017) proposed that “respondents with better material status have provided the funds needed for medical expenses, the purchase of necessary supplies, the provision of services related to care, and that can have a positive effect on psychological functioning of the person. Social status is a factor that can influence people’s subjective view of what makes a good quality of life.” (Glinac et al., 2017, p. 170)
Second, in terms of psychological factors, it was observed that rehabilitation patients with mental illness had the lowest FQoL, consistent with findings from previous studies (Glinac et al., 2017; Vitorino et al., 2021). The perception of risk and patients’ physical and mental responses are closely intertwined with the recognition of FQoL. However, psychological distress did not significantly impact the dimension of disability support. Instead, family support emerged as the primary predictor of FQoL, exerting a significantly positive influence. This suggests that family support plays a more direct role in patients’ perception of family life quality than support from friends, as patients spend the majority of their time with their families (Connell et al., 2012). Additionally, individuals with greater grit or perseverance tended to have higher recognition of FQoL, which could be attributed to their enhanced resilience in the face of setbacks and their ability to maintain a positive attitude during the treatment process. These individuals actively cooperated with their rehabilitation institution’s treatment plan and maintained harmonious relationships with their family members.
Rehabilitation factors did not show a statistically significant impact on FQoL in this study, possibly due to the limited sample size. However, it is still possible to discuss the findings based on mean comparisons. The most common forms of treatment in the study were exercise therapy and traditional Chinese medicine, with individuals receiving these treatments reporting the highest FQoL. Exercise therapy offers natural advantages, such as improving health-related quality of life, reducing symptoms of depression and anxiety, and lowering the risk of non-serious adverse events (Bricca et al., 2020). Traditional Chinese medicine can be traced back more than 2,000 years to Huangdi’s Internal Classic (Huang Di Nei Jing). Chinese individuals easily accept it (Lu et al., 2022) and its holistic perspective on various diseases, which aims to restore the body’s various components’ balance and functioning and support normal physiological activities without side effects (Shao & Zhang, 2013). On the other hand, electronic biotherapy and speech therapy are less frequently chosen treatments, and the sample of participants receiving these therapies was small and not representative. Furthermore, the duration of rehabilitation period and FQoL formed a U-shaped curve. Patients in the transition period of 1 to 3 months of rehabilitation often experience conflicts, frictions, and compromises among family members, significantly impacting the overall family atmosphere and quality of life. The overall satisfaction with rehabilitation significantly and positively influenced FQoL, possibly because rehabilitation satisfaction elicits positive emotions. While there is not enough evidence in existing studies to demonstrate the direct impact of rehabilitation satisfaction on an individual’s FQoL, many studies have shown that an individual’s rehabilitation outcomes can affect both themselves and their family members (Kim et al., 2021; Öztürk & Küçük Alemdar, 2023; Umunnah et al., 2023).
There are several limitations to consider in this study. Firstly, the sample size of 51 participants is relatively small, leading to an uneven distribution of samples across different demographic variables. Although statistical methods such as mean comparisons and regression analysis were used to the best extent possible, it is important to acknowledge the need for future research to expand the sample size in order to validate and enhance the existing findings. Furthermore, this study is cross-sectional in nature, relying mainly on mean comparisons and regressions to draw conclusions; this made it challenging to establish cause-and-effect relationships between the variables examined. However, the methods employed in this study still hold a certain significance as they shed light on potential factors that may influence the FQoL in rehabilitation patients. These factors offer valuable insights for future intervention and control methods, and serve as a basis for further verification and enrichment of the study’s findings.
This study adopted an integrated approach to explore the influence of demographic, psychological, and rehabilitation factors. Although some of the statistical results may not be significant because of the limited sample, there were slight differences observed in means between different groups. While the study cannot draw definitive conclusions based solely on these statistical results, it does provide insights and directions for further exploration. The findings indicate that demographic factors (e.g., economic and educational levels) and psychological factors impact how rehabilitation patients evaluate their FQoL. This highlights the importance of considering these factors when assessing and addressing the needs of rehabilitation patients and their families. By focusing on the direct elements of rehabilitation, the study highlights the significance of factors such as the duration and mode of rehabilitation. This provides actionable suggestions for patients to have a better psychological experience during the rehabilitation process, which can have important implications for the well-being of vulnerable groups. Further research with larger sample sizes and more rigorous research designs could build upon and help validate these initial findings, ultimately enhancing our understanding of how to support the well-being of rehabilitation patients and their families.
Based on this study’s main findings, several recommendations can be made for rehabilitation practice. First, it is important to provide health knowledge lectures specifically targeting rehabilitation patients with low educational levels, as this could help improve their health awareness and encourage their active cooperation in their treatment. Rehabilitation institutions should also consider proposing alternatives for rehabilitation patients from families with suboptimal economic status, ensuring that financial constraints do not hinder their access to necessary rehabilitation services.
Second, when providing physical rehabilitation to patients, it is crucial to evaluate their psychological status. If necessary, psychological interventions should be considered, such as mindfulness interventions, meaning-making interventions, and psycho-spiritual interventions. This holistic approach takes into account both the physical and psychological needs of them, promoting their overall well-being.
Third, effective communication with the rehabilitation patient’s relatives is essential to understanding the patient’s needs and providing appropriate support. Rehabilitation centers should strive to strengthen this communication channel and provide families with scientific advice on how to best accompany and support the patient throughout the rehabilitation process.
Fourth, when considering the influence of rehabilitation factors on patients’ quality of life, it is noteworthy that the effect of recovery time on family satisfaction follows a U-shaped curve, suggesting the need for closer collaboration between medical rehabilitation institutions and the community to help rehabilitation patients adapt to the recovery period more effectively. This could be achieved through community outreach programs, support groups, and the provision of resources and services that assist them in their recovery journey.
By implementing these recommendations, rehabilitation practice can be tailored toward the specific needs of rehabilitation patients and their families, ultimately improving their quality of life and facilitating a more successful rehabilitation process.
Footnotes
Acknowledgements
All the thanks will be given to all the participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shandong Province Taishan Scholar Project Special Fund (No: tsqn202306071).
IRB Details
In this study, informed consent was issued to the subjects before the investigation. After obtaining the consent of the subjects, conduct the survey.
Data Availability Statement
The data were obtained from the team’s research, fully guaranteeing their authenticity and effectiveness. Readers can request data from the authors after the project is completed. Data will be provided to applicants if possible.