
Abstract
A therapeutic error as a multifactorial phenomenon in psychotherapy and counseling is an action and behavior that is committed by the therapist and leads to treatment failure or client dissatisfaction with the treatment process. Thus, the treatment method deviates from the intended practical and scientific techniques. To this end, the present study aimed to identify the counselor’s perceptions of therapeutic errors in the treatment room. This qualitative study was conducted using conventional content analysis. The data were collected through in-depth and semi-structured interviews with counselors and psychotropics with at least 3 years of experience in psychotherapy and counseling in various fields. They were selected through purposive sampling in 2021 in Tehran. The data were saturated by interviewing 24 counselors and psychotherapists and analyzed by the content analysis approach. The findings showed that therapeutic errors occur for different reasons and in various forms and involve different aspects of the therapist-client interaction. The most important therapeutic errors were intrapersonal and organizational errors including; treatment errors, lack of practicality of the treatment, the therapist’s errors, mistakes committed due to the treatment space, non-compliance with ethical principles and standards, and not informing the clients. The occurrence of these errors and mistakes in the treatment session leads to the abandonment of the session by clients, negative experiences invoked by treatment sessions, and most importantly damage to clients and a range of negative consequences. The findings of this study can have some implications for understanding various forms of treatment errors, preventing errors in treatment sessions, and avoiding harm to clients in treatment sessions.
Plain Language Summary
The results of the present study indicated that it is better to look for the errors that occur in the treatment process instead of attributing the causes of abandonment and ineffectiveness of psychotherapy to the clients and the clients’ resistance. Training and attending specialized courses and high experience alone cannot protect clients from the psychotherapist’s mistakes because the therapist’s vulnerabilities and cognitive distortions can affect the training outcomes. Clients are emotionally disturbed and overwhelmed by their problems when they seek psychotherapy and counseling and do not notice the mistakes and harm that the therapist inflicts on them. Perhaps receiving feedback from clients, colleagues, and professors, continuous review of treatment sessions, individual treatment before entering the psychotherapy profession, and also conducting more extensive studies in this field are some measures that can be taken to reduce the frequency of therapeutic errors.
Keywords
Introduction
Psychiatric diseases are among the major health concerns in the community, and 25% of people might meet the diagnostic criteria for a psychiatric illness at some point in their lives (WHO, 2007). In 2021, on the occasion of World Mental Health Day, the World Health Organization (WHO) announced that the COVID-19 pandemic has had a major impact on people’s mental health. Thus, this global catastrophe is an opportunity to identify problems and strengthen mental health systems not only in emergencies but also in the long term (Vigo et al., 2020). Treating COVID-19-induced mental disorders and their consequences on work and personal and social life usually imposes substantial costs on society and necessitates attention to their treatment and management (Kohn et al., 2004).
Counseling and psychotherapy have been recognized and established in many health systems around the world, and many research studies have been published in this area in recent decades (Lambert, 2013). Many mistakenly consider counseling and psychotherapy to be a simple process in which a person talks about his/her problems and the therapist asks him/her to describe his/her childhood experiences, and then the therapist interprets the true meaning of the experiences, and the person in question gains some insight into how to solve the problems (Phares & Trull, 2002). Some efforts have been made to prove the positive effects of psychotherapy (Barth et al., 2013). Different approaches to psychotherapy help many people with different mental disorders (Lambert, 2013). However, many patients do not benefit from treatment, even if the treatment provided is effective (Castonguay et al., 2013). Most studies have highlighted the positive effects of psychotherapy. However, a point to note is the negative effects and consequences of psychotherapy (Mohr, 1995). Psychotherapy is one of the most common activities of clinical psychologists and they devote most of their time to psychotherapy activities including diagnosis and evaluation. Nevertheless, the point to consider is why, despite the extensive work of psychologists, we see little improvement in clients.
A commonly held belief attributes the patients’ unsuccessful recovery to his/her resistance to the treatment process (Becker & Rosenstock, 1984; Davis, 1966; Gordis, 1967). Despite effective psychotherapy and medication techniques (Mulrow et al., 1999), only a small proportion of patients with common mental disorders are adequately treated within a year (Kessler et al., 1999). Clients’ withdrawal is a serious problem in the treatment of mental health (Edlund et al., 2002). Numerous studies report clients’ withdrawal from treatment. Approximately one-third of clients do not return after the initial interview, and nearly half of them withdraw from treatment after the second session. Most therapists do not know the reason(s) for withdrawal (Schartz & Fliwers, 2006). Those clients who return to the treatment sessions also do not achieve tangible results and continue treatment for an average of another 10 sessions before concluding that psychotherapy is not effective (Stewart & Chambless, 2008). This also holds for 10% to 20% of clients who get worse in treatment. It is also estimated that 5% to 15% of patients experience a negative treatment experience, but little research has been done on this subject (Hardy et al., 2017).
A large number of studies have suggested that psychotherapy is moderately effective. However, 30% to 60% of patients do not benefit from treatment (Lambert, 2013). About 5% to 10% of patients get even worse during the treatment process (Lambert, 2013). Although the effectiveness of cognitive-behavioral therapy has been confirmed in many disorders, many patients do not benefit from this treatment. This failure depends on several factors, including clinical errors that often occur in the treatment process. Lack of knowledge about the changes in cognitive-behavioral therapy and its effective presentation may be due to clinical errors that play a role in poor therapeutic outcomes. Clinical errors are mistakes that therapists may make when presenting cognitive-behavioral therapy in their clinical judgment (Kim et al., 2016). The range of potential injuries is not limited to worsening symptoms and withdrawal (McKay & Jensen-Doss, 2021; Lilienfeld, 2007) but includes potential harm to the client’s family members and friends and possible non-assessed risks of some treatments and false claims of abuse. Most academic works on clinical errors are in the literature on medicine (O’Donohue & Engle, 2013). Errors in physical problems are more visible than in psychological problems. Clinical errors are inevitable, and we need to equip the next generation with psychotherapy skills and processes. One of the most difficult aspects of clinical error analysis is not the error itself, but rather the process that leads to the error and the post-error state of affairs (Budge, 2016). Given the potential negative consequences associated with dropout from the treatment, identifying potential predictors and risk factors can help prevent this decline in treatment (Zimmermann et al., 2017). Little systematic research has addressed specific behaviors of specialists that may lead to traumatic outcomes. Dimidjian and Hollon (2010) argue that dropout in treatment is a traumatic outcome because it drains clients of emotional and financial resources and restarting treatment requires the reuse of these depleted resources. Kottler (2003) suggested that failure in any task, especially in complex tasks such as treatment, is affected by many factors. A follow-up study of client dropout has shown that most clinicians did not know why their patients stopped the treatment process and why they were satisfied with their decision. Some clients stop the treatment process without informing the therapist. However, their clients specifically pointed out treatment errors or weaknesses of their therapist, such as feeling uncomfortable talking to their therapist, as possible reasons (Hynan, 1990). Lilienfeld et al. (2014) revealed that psychotherapists have a misunderstanding of the effectiveness of treatments on clients. They introduced four fundamental obstacles for cognitive impediments to accurately evaluating and assessing improvement in psychotherapy, including naive realism, confirmation bias, illusory causation, and the illusion of control.
Many patients may follow their problem for years and refer to several therapists, but they still suffer from the same problems without any prospect of recovery. The patient may generalize his/her previous failures to the current therapist. This is one of the main obstacles to effective treatment (Freeman & McGloskey, 2003). This suggests that therapists’ errors in the treatment room deprive clients of the opportunity to revisit and thus they assume that their problem will not be solved. A recent meta-analytic study by Swift et al. (2012) found that approximately one in five clients still stops psychotherapy before completing it. Even if a lower dropout rate is found than was estimated 20 years ago, early termination of the treatment process is still a major problem. Following the previous studies in the literature, it can be concluded that one of the reasons for people avoiding seeing a psychologist and counselor is the medical errors that occur during treatment by therapists. One of the obvious medical malpractices is to leave objects in the patient’s body during the operation, which manifests itself with infection, but in counseling and psychotherapy, beliefs and thoughts can be left in the patient’s mind, with the difference that the infection is not visible and the patient may live with this infection for a long time. Lazarus and Fay (1982)defined resistance as an excuse from an incompetent therapist who failed to find the dominant problem that governed patient behavior and believed that instead of attributing the cause of lack of progress or failure of treatment to patients’ resistance, we should look for our scientific incompetence and personal problems. It is hoped that further research will prevent these errors from occurring and identify these limitations and problems so that clients can benefit from the psychotherapy and counseling process. To this end, the present study aimed to explore counselors’ and psychotherapists’ experiences and perceptions of their errors in the treatment room. This study, unlike the previous ones, has comprehensively examined this phenomenon that has been rarely dealt with in previous studies.
Method
This qualitative study was conducted using a conventional content analysis method. One of the distinct advantages of the conventional approach to content analysis is gaining direct information from participants without imposing preconceived categories or theoretical perspectives (Hsie & Shannon, 2005). Conventional content analysis is used to make pure and valid inferences from the content of data to provide knowledge, new insights, facts, and practical guidance for action (Krippendorff, 1980). The participants were selected using purposive sampling. The end of sampling was determined using the theoretical saturation technique that is, data collection continued until it was not possible to access new categories, codes, or explanations. The data were collected through semi-structured interviews that were conducted using a general guide and a list of questions with predetermined topics.
Interview Questions
The interview questions are mostly focused on the experiences and behaviors that psychotherapists have shown in the past in the process of psychotherapy and counseling. The questions were asked in the following order:
Examples of interview questions were:
- What is your perception of treatment errors, or what do treatment errors mean to you?
- Following your experience of psychotherapists and clients, what are the reasons that make clients stop the treatment process?
- Some clients, despite not having a positive experience of psychotherapy activities, continue it. In your opinion, what strengthening factors cause their reappearance in treatment?
- Can you name some of the mistakes you made in the treatment session? And what do you think was the cause of these mistakes?
Participants
In this study, participants needed to have certain characteristics to provide rich information about the subject in question. For this reason, the inclusion criteria were being a psychotherapist and counselor with 3 years of clinical experience, living in Tehran, and having the desire to talk and participate in the study. The exclusion criteria were not wanting to be interviewed, having a chronic illness, etc.
Following the objectives of the study, the participants were selected using purposive sampling. The end of sampling was determined using the theoretical saturation technique. Based on this technique, the selection of participants continued until the interview with new people did not provide the researcher with new information and the added information was almost repetitive. Thus, the data were saturated after interviewing 24 counselors and psychotherapists. The selection of participants was tried to be proportionate, as much as possible, in the sense that the number of participants had a good previous justification.
The participants were invited to the interviews via an invitation letter containing necessary information about the study and its procedure, a phone number, and an email address prepared by the researcher. To this end, the researcher visited well-known and reputable clinics and submitted invitation letters to the clinic manager or founder. Some counselors and psychotherapists also participated in this study through online media. All participants were selected by the researcher based on the characteristics required in the study. The participants in this study were counselors and psychotherapists living in Tehran. Most of them were offering psychotherapy and counseling services in reputable and well-known academic and private clinics and psychiatric hospitals.
Instrument and Procedure
An interview is the most common form of data collection in qualitative research and can be adapted to a variety of research situations (Punch, 2009). An interview is a great way to evaluate perceptions, meanings, definitions, and situations, and construct reality, and it is also one of the most powerful ways to understand others. Indeed, interviewing has been used to understand the personal reality constructs of therapists’ experiences (Punch, 2009). Since, this study was conducted during the COVID-19 pandemic, the data were collected using both face-to-face interviews and telephone and video call interviews. The minimum and maximum interview times were 15 and 180 minutes. The interview time varied depending on the psychotherapists’ condition. The interviews with all participants took a total of 1,213 minutes. The interviews were conducted from April to early July (about 2.5 months). At the beginning of the interview, a safe environment was provided for therapists to speak more confidently about their experiences. Besides, the interviews did not begin until the participants expressed their consent.
The interview process was led by the interviewer, empathy was observed, no value judgment was made about the answers, the purpose of the research was not forgotten during the interview, and flexibility was observed as much as possible. At the beginning of the interview, a safe environment was provided for therapists to speak more confidently about their experiences. Besides, the interview did not begin until the participant agreed with it.
Demographic data including age, treatment approach, the field of treatment, activity history, and educational degree were first recorded. Then, the questions were asked in order. During the interview, if there was a need to make the story clearer, more exploration was added. The questions were first general and then became more detailed. Finally, the interview was terminated by asking the participants to add any comment or further information if they wished. The participants were 13 women and 11 men, aged 27 to 47 years. They were working in the field of psychotherapy for at least 3 years and at most 24 years. Six participants held a PhD in psychology, three held a PhD in counseling, six persons held a master’s degree in psychology, four held a master’s degree in counseling, and four were PhD candidates in psychology. The most frequent approaches used by the participants were schema therapy, cognitive-behavioral therapy (CBT), and emotion-focused techniques to solve individual and adult problems.
Table 1 shows the participants’ demographic data:
The Participants’ Demographic Data.

Data Analysis
Following the objectives of the study and the fact that there is not enough knowledge in this field, the inductive method was used. The inductive method moves from specific data to general and broad data. In this study, according to Streubert Speziale and Carpenter (2007), the themes were extracted directly from the text of the interviews using the inductive method, and the researcher’s theoretical presuppositions were not imposed on the data.
The collected data were analyzed using the content analysis approach proposed by Graneheim and Lundman (2004): (1) Transcribing the interviews and reviewing them several times to come up with a full understanding of their content, (2) Extracting meaning units and categorizing them as condensed units, (3) Labeling the extracted categories, (4) Arranging the subcategories based on their similarities and differences, and (5) Selecting a core category that can cover the resulting categories.
Part 1: Extracting Units of Meaning and Classifying Them as Condensed Units
This step is done by selecting a unit for analysis. A unit of meaning may be more than one sentence in which there are several meanings. Depending on the research question, the unit of analysis can be a letter, a word, a sentence, and part of the pages or words, the number of participants, or the time in question (Robson, 1993; Polit & Beck, 2004). The units that were selected for analysis depended on the research question and as the degree of abstraction and interpretation in the conventional content is low, more emphasis was placed on overt content for analysis, and hidden meanings such as silence, sighs, laughter, etc., were not considered in data interpretation.
Part 2: Preparing Meaning for the Data
According to Dey (1993), when reading the data, questions are “who says this? Where did it happen? When did it happen? What happened? and why?” The goal is to immerse oneself in the data. Therefore, the text of the interview is read several times at this step and no insight or theory comes to mind from the data until it is fully understood Polit and Beck (2004). After the data is given meaning, they are analyzed based on the inductive approach.
Part 3: The Organizing Step
This step involves open coding, classification, and abstraction. In open coding, the notes and titles of the units of analysis were rewritten as they were read. After open coding, the subcategories were sorted based on the similarities and differences between the subcategories and the purpose of this classification was to reduce the multiplicity by transferring the data that were similar or different to higher and more comprehensive classifications. When the classifications were formed, it was decided which code would fall into which category.
In the abstraction step, the general description was regulated through the production of categories. The categories, which were named in the previous step, were placed next to each other based on their similarity and relationship and considered the main categories. At this step, the categories were converted into a more general meaning.
Rigor
Content analysis emphasizes diversity in content and multiplicity. Thus, there must be adequate data to cover significant changes. Furthermore, to enhance the dependability of the data, the sample size was determined in a manner to have adequate data based on the objective of the study. To enhance the transferability of the findings, the participants were selected with great care and sensitivity. Moreover, it was tried to provide a rich and accurate description of the literature in the field. The data were also codified and categorized in cooperation with other experts in the field. To further increase the credibility of the data, the researcher reviewed the previous studies in the literature. This helped the researcher to find out how to develop the question and analyze and interpret the data. Data analysis was performed through peer checking to increase the credibility of the findings. A common problem in conventional content analysis is the extraction of categories at different levels of abstraction and their interpretations. This problem not only threatens the authenticity of the findings but also threatens their reliability. Thus, the researchers quoted the participants’ statements to help readers judge the credibility and rigor of the data.
Results
Data analysis revealed two main categories (the therapist’s intrapersonal and organizational errors), six sub-categories, and 41 open codes, as shown in Table 2. The coding and consequently the categorization of the study began at the same time as reading the text or interview.
The Open Codes and Sub-Categories Identified in the Study.
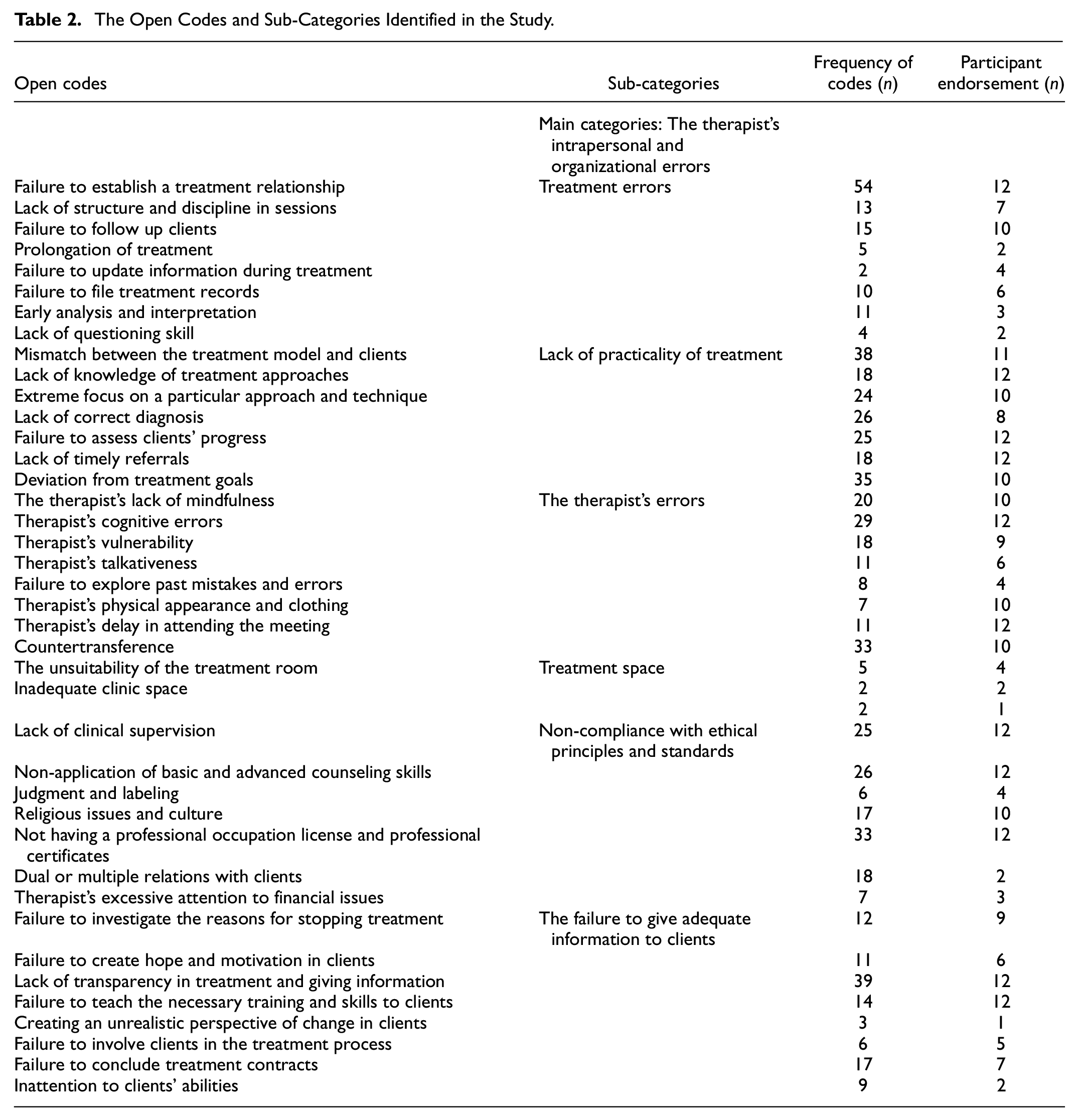
As Table 2 shows, the frequency of sub-categories refers to the number of times the open codes have been repeated by the participants in the text, and participant endorsement refers to a number in the member checking process, for which 12 participants were selected, who approved the codes and interpretations in the process.
Subcategories
The results revealed six subcategories: The therapist’s intrapersonal and organizational errors, treatment errors, lack of practicality of treatment, the therapist’s errors, treatment space, non-compliance with ethical principles and standards, and the failure to give adequate information to clients.
Treatment Errors
The extracted codes related to this sub-category were the failure to establish a treatment relationship, lack of structure and discipline in sessions, failure to follow-up clients, prolongation of treatment, failure to update information during treatment, failure to file treatment records, early analysis and interpretation, and lack of questioning skill.
One of the most frequent codes was the failure to establish a treatment relationship (n = 54) which was mentioned by the participants and was considered one of the most important errors and causes of the termination of the treatment relationship. In this regard, a participant mentioned, “One of the most important problems is that if an effective therapeutic relationship is not established between you and the client, for any reason, the client cannot trust you or cannot receive empathy from you and the rapport is not established, your treatment is not effective” (Participant 5, Male, 43, MA in Counseling). The next code was lack of structure and discipline in sessions (n = 13), hence sessions go ahead without previous structure and agenda. Perhaps one of the most important reasons for discontinuation of treatment and recurrence of clients, according to participants, is failure to follow up clients (n = 15) after treatment or during treatment, “we never follow our patients. Where is the person who has come 5 sessions or 17 sessions? Where is he 6 months later? Where is he two months later?!” (Participant 5, Male, 34, MA in counseling). One of the treatment errors is the prolongation of treatment (n = 5) and staying in treatment for a long time. “Sometimes it is necessary to see the person two times a week, but it is not possible, so the treatment takes too long, it makes him tired” (Participant 19, Female, 19, MA in Counseling).
Another code is failure to update one’s information during treatment (n = 2). Reading new articles and research in the field of psychotherapy and counseling can increase awareness and prevent treatment failure, “Sometimes I have clients I do not know how to treat or how to challenge, but I go and see, for example, there are many books and articles about these clients” (Participant 1, Male, 37, PhD in Psychology). It is very painful for clients to see their therapist has forgotten their information, and failure to file treatment records (n = 10) with details can lead to forgetfulness. From one participant’s perception, “Another mistake is that consultants do not write files and trust their memory. Memory does not work at all; the client file must be written between the sessions” (Participant 22, female, 30, PhD Candidate in psychology). Early analysis and interpretation (n = 11) regardless of the client’s readiness may cause treatment discontinuation, “when the client cries in the first session, we immediately start confronting him, or conversely, the client who is very cold-blooded, and has a high resistance, then his defense is very strong” (Participant 6, Female, 37, PhD in psychology). Lack of questioning skill (n = 4) is also one of the mistakes that many therapists commit, “Asking questions in time; well, I think this is a skill that helps a lot, and if we are not aware, if we are not in the moment, it will become our weakness” (Participant 6, Female, 37, PhD in psychology).
Lack of Practicality of Treatment
Another sub-category is the lack of applicability of treatment for clients, despite its being effective, which includes the following codes: mismatch between the treatment model and clients, lack of knowledge of other treatment approaches, extreme focus on a particular approach and technique, lack of correct diagnosis, failure to assess clients' progress, lack of timely referrals, and deviation from treatment goals. One of the codes that many participants referred to is the mismatch between the treatment model and clients (n = 38): “The client feels no, this treatment does not work for me” (Participant 2, Male, 33, PhD candidate in psychology). The one-dimensionality of the therapist’s approach may be an obstacle to dealing with clients who fit another treatment model, hence according to the participants’ statements, the lack of knowledge of other treatment approaches (n = 18) may lead to treatment failure, “As a therapist, I do not say that you should know dynamic psychotherapy, but if you do not know about it, you cannot deal with the client” (Participant 2, Female, 36, PhD in psychology). The next code is the extreme focus on a specific technique and approach (n = 24), which results in applying a protocol to all clients without realizing their differences. One of the participants stated, “I think one of its reasons is that a therapist who has only one weapon, uses that weapon for everyone” (Participant 5, Male, 43, MA in Counseling). Incorrect diagnosis (n = 26) and understanding of the clients’ problem along the treatment path will also lead to difficulties and maybe another important treatment error.
Perhaps one of the factors that make clients frustrated with continuing treatment and also make the therapist unaware of the treatment process is the failure to assess clients’ progress (n = 25). Lack of this evaluation causes the client to continue treatment even if they do not have a positive experience, “After a while, when the person is here again, we should ask the degree of the patient’s satisfaction of his changes. What is the percentage of his changes so far in his opinion?” (Participant 21, Female, 31, MA in Psychology). Lack of timely referrals (n = 18), this code revealed that, the therapist may not be a specialized approach for their client’s treatment, but he/she did not refer client to specialist therapist, “In my opinion, one of them is the clients’ waste of time. For example, sometimes they know they cannot treat the client, but they do not refer he/she to another counselor.” (Participant 22, Female, 30, PhD candidate in psychology). Deviation from treatment goals (n = 35) is another frequent error that the therapist can make: “I think the therapist’s mistake is something that disrupts the treatment process and its goals. The goal of treatment is determined by the therapist and the client. So, when we have a goal, for example; our client wants to reduce his obsessive-compulsive symptoms, but the counselor chooses another aim, the treatment error occurs” (Participant 2, Female, 36, PhD in psychology).
The Therapist’s Errors
The therapist’s errors were highlighted by many participants. These errors include the therapist’s lack of mindfulness, cognitive errors, vulnerability, talkativeness, physical appearance and clothing, delay in attending the meeting, countertransference, and the failure to explore past mistakes and errors.
Lack of mindfulness (n = 20) in the session is one of the things that many therapists, willingly or unwillingly, experience in the treatment session, “This in itself causes errors. That is, his mind is left somewhere else and I am not giving my full attention” (Participant 18, Female, 30, MA in Counseling).
Therapists’ cognitive errors (n = 29) are also of the important points mentioned by the participants, “Naturally, the therapist enters the treatment room with some presumptions, which are the cognitive distortions that we are talking about, and of course, the therapist himself/herself makes a series of mistakes” (Participant 1, Male, 37, PhD in psychology). Therapist’s vulnerability (n = 18) can divert the treatment from the main route. One participant said, “Unfortunately, sometimes the therapist’s pathological damage is higher than the client. That is, the therapist himself has not received treatment. There are traces of the problem in him. These traces come and ruin the work” (Participant 7, Male, 38, PhD in counseling). Another code is the therapist’s talkativeness (n = 11), “In some places we say it is speech, for example, sometimes the clients feel that I am talkative, instead of listening to his pains, I am talking about my pains” (Participant 8, Male, 36, PhD in counseling). Some participants acknowledged that sometimes therapists with more experience have more errors because they do not explore past errors. Another code is the failure to explore past mistakes and errors (n = 8). “If a person faces difficulties in the treatment and is a professional, skillful therapist, he can explore where the problem is and what he wants to work on. In my opinion, the things that come to my mind are these, which form treatment errors” (Participant 12, Male, 37, MA in Psychology). The therapist’s physical appearance and clothing (n = 7) is also one of the items that may have been less addressed but is an important issue for clients, “The therapist’s clothing is important. His appearance is important, his style is important, and if it is not observed, it can be a behavioral error that has a very negative impact on the patient. The patient thinks that the therapist is depressed because he does not care about his appearance” (Participant 24, Male, 39, PhD in counseling).
The therapist’s delay in attending the meeting (n = 11) can cause a bad feeling in the clients. One participant said about her experience “Time is another important issue for me. If I want to teach discipline and punctuality to the client, I should not be late” (Participant 21, Female, 31, MA in Psychology).
Countertransference (n = 33) is also one of the codes that have been repeatedly mentioned. “Therapeutic error, for me, is the first thing that comes to my mind; a transfer of my feelings and beliefs to the client” (Participant 16, Female, 31, MA in Psychology).
Treatment Space
The treatment space was one of the specific sub-categories whose importance was perhaps less dealt with in the previous studies. The errors related to the treatment space were caused by several factors such as the unsuitability of the treatment room and inadequate clinic space. One of the important codes is the unsuitability of the treatment room (n = 5) in which the client cannot feel comfortable and safe, “I think the therapist room is very important. The color, the plants and flowers in it, enough lighting, and things like that are very important” (Participant 21, Female, 31, MA in Psychology). Another code is inadequate clinic space (n = 2) and the waiting room, “Well, there are many general factors. I think some factors are related to the clinic itself that affect the treatment space. I mean the clinic setting is very important and affects the clients when they enter it” (Participant 14, Male, 33, PhD candidate in psychology).
Non-Compliance with Ethical Principles and Standards
Non-compliance with ethical principles and standards is mainly caused by factors such as lack of clinical supervision, non-application of basic and advanced counseling skills, judgment and labeling, religious issues and culture, not having a professional occupation license and professional certificates, dual or multiple relations with clients, and therapist’ excessive attention to financial issues.
One of the most important errors that therapists make is not reviewing treatment sessions with qualified people, which was repeatedly referred to by participants as the lack of clinical supervision (n = 25), “I should receive supervision, and when I do not receive it, I do what I think is the right thing, what should be right is different from what I say.” (Participant 12, Male, 37, MA in Psychology). Non-application of basic and advanced counseling skills (n = 26) is also one of the most basic weaknesses in the treatment room. In this study, many participants considered it as an obvious error of the therapist, “One of my weaknesses is the absence of basic or advanced skills and I must continue to strengthen this experience when dealing with my clients” (Participant 24, Male, 39, PhD in counseling). The next code is judgment and labeling (n = 6). Contrary to the perception that psychologists and counselors should strictly avoid judging and labeling, many therapists, unfortunately, do it and hence discourage clients from continuing treatment or harm them, “The next thing is that the client is judged. For example, the client comes and says something. I will say, did you really do that? How dared you!?” (Participant 8, Male, 36, PhD in counseling). Religious issues and culture (n = 17) were also mentioned by participants. The participants believed that having the same religion and culture is important in psychotherapy and counseling, “The issue of religion is very important. It is also an issue that may disrupt therapeutic communication. This has happened to me” (Participate 21, Female, 31, MA in psychology). Unfortunately, many clients do not pay attention to the therapist’s not having a professional occupation license and professional certificate (n = 33), and some therapists work without passing specialized courses and having employment licenses, “When a client who comes to the treatment session sees the professional license, he becomes a little relieved that his choice was the right one. He can trust the therapist. If the consultant does not have a work permit, she/he may lose her/his trust” (Participant 14, Male, 33, PhD candidate in psychology).
Dual or multiple relations with clients (n = 18) is one of the errors. The client may not notice the harm of this relationship and the therapist may create this friendship. One of the participants said, “Well, in my opinion, this happens often that a client becomes a friend and a companion for the therapist, or even sometimes, a financial source, especially the clients who are well-off” (Participant 14, Male, 33, PhD candidate in psychology).
The Failure to Give Adequate Information to Clients
One of the sub-categories that may attract less attention in the field of medical errors is the lack of providing the clients with knowledge in the treatment process. The failure to give adequate information to clients is caused by many factors including the failure to investigate the reasons for stopping treatment, failure to create hope and motivation in clients, lack of transparency in treatment, giving information, failure to teach the necessary training and skills to clients, creating the unrealistic perspective of change in clients, failure to involve clients in the treatment process, failure to conclude treatment contracts, and inattention to clients’ abilities. One of the codes that many participants cited for discontinuation of treatment is failure to investigate the reasons for stopping treatment (n = 12), which leads to the therapist’s unawareness of the cause of his mistakes during treatment, “The first reason is why he left the treatment, that is, we may even spend a session exploring to see what problems have been in me, in the counseling session, or in that person” (Participant 18, Female, 30, MA in Counseling). Another code is the failure to create hope and motivation in clients (n = 11). Many clients do not have the readiness, motivation, and hope for treatment. The therapist should explore this important issue and give hope to the client and motivate him to continue his treatment, “First of all, in psychotherapy, I try to keep that client motivated. I ask the client questions related to his life background and his purpose of attending the treatment session” (Participant 3, Male, 33, MA in Psychology).
Another code is lack of transparency in treatment and giving information (n = 39). One of the participants said, “The thing that can most help to solve these problems is that I as a therapist make everything clear for the client. We can tell the client what problems we can or cannot solve for them” (Participant 14, Male, 33, PhD candidate in psychology). The next code is failure to teach the necessary training and skills to clients (n = 14). The Therapists must equip the clients in the treatment sessions in a way that they can solve their problems, “One of the most important general treatment goals is patient self-management and teaching skills to the client. When I do not teach my client problem-solving skills, it is clear that he/she will come to me whenever there is a problem. If, instead of offering solutions, I teach problem-solving skills they will know what to do, say, when they are asked by their son” (Participant 2, Female, 36, PhD in psychology). The next code is creating the unrealistic perspective of change in clients (n = 3) to which some participants referred, “Or hope in you; hoping wrongly; a part of this can be the therapist’s own mistake. Giving a lot of hope. Giving the wrong hope” (Participant 13, Female, 39, MA in Counseling).
Sometimes, directive counseling methods will not get the counselor/therapist anywhere. One of the most important errors is failure to involve clients in the treatment process (n = 6), “I have the experience of changing my line and getting involved in what I thought was more important. Well, perhaps it was more important but it was not my client’s complaint. It was as if I became more catholic than the pope. I used to do this a lot in the first years.” (Participant 17, Female, 47, PhD in psychology). Another most frequent codes is failure to conclude treatment contracts (n = 17), pointed out by many participants, “And, writing a treatment contract, in my opinion, is one of the factors that a qualified therapist does not forget in the first sessions and puts them in the treatment plan” (Participant 14, Male, 33, PhD candidate in psychology). The last code is inattention to clients’ abilities (n = 9). The participants noted that one of the common psychotherapists’ committed errors is not showing the clients their strengths, “The hopes that my client has brought back with himself/herself in the session, for example; the hopes he/she has for the future or a better life are very important to me” (Participant 24, Male, 39, PhD in counseling).
Discussion
Treatment Errors
Treatment errors account for a high percentage of the causes of medical errors as the majority of the participants mention this dimension. All participants, without exception, considered one of the most significant treatment errors to be the lack of empathy and therapeutic communication. As Blair (2005) has pointed out, empathy is a multidimensional construct consisting of at least one cognitive and emotional component. In many psychiatric disorders, such as depression and personality disorders, empathy is missing. Hence, is empathy still teachable? Is it possible to ensure the health of the psychotherapist so that he/she can create this empathy? Norcross and Lambert (2018) in their comprehensive review of the factors affecting the psychotherapy relationship, concluded that work unity, cooperation, goal consensus, positive attention and approval, therapist empathy, and use of feedback are significantly effective. Finsrud et al. (2021) presented information on how patients perceive and evaluate common communication factors in psychotherapy in six areas (i.e., goal agreement, task agreement, therapist empathy, client expectations, therapist expertise, and treatment credibility).
Yalom (2003) pointed to case writing and stated that if therapists are to be historians of the treatment process and seek to maintain the continuity of the sessions, they need to keep a history of events somewhere. Furthermore, if there is nothing important in the meeting to write, it means that the treatment is stagnant and my patient and I have not started any new topics (Yalom, 2003). Beck (2005) reported that the most common errors committed by therapists include clinical misdiagnosis, incorrect treatment plan, incorrect treatment alliance, incorrect list of behavioral goals, improper structure or timing, and incorrect application of treatment techniques (Beck, 2005).
They also highlighted the importance of the therapeutic relationship and treatment techniques. Yalom (2003) stated that patients who were dissatisfied with their previous treatment claimed that their therapists distanced themselves too much from them, withdrew, were not supportive, and behaved coldly, and they had never heard any patient complaining about excessive self-disclosure (Yalom, 2003). In the present study, the findings revealed that new treatment errors such as the failure to establish a treatment relationship, lack of structure and discipline in sessions, failure to follow-up clients, prolongation of treatment failure to update information during treatment, failure to file treatment records, early analysis and interpretation, and lack of questioning skill are the reasons for maltreatment.
Lack of Practicality of the Treatment
Despite the effectiveness of many therapeutic approaches, some of the approaches are not effective for some clients and some therapists. In line with the findings of this study, Knox et al. (2020) described the error as using an approach that is not helpful to the client/psychotherapist. Furthermore, Trimboli et al. (2016) have pointed out 12 common errors in the course of psychotherapy, including deciding on the focus and form of treatment. Freeman and McGloskey (2013) also described the lack of skills or experience, unrealistic, vague, and ambiguous treatment goals or disagreement with the patient in goal setting, lack of cooperation and weakness in the therapeutic alliance, as well inflexibility in the treatment plan as treatment barriers.
Yalom (2003) believed that the therapist should try to create a new treatment for each patient. Castonguay et al. (2013) considered strict adherence to the use of psychotherapy techniques as a potentially harmful behavioral therapy. Freeman and McGloskey (2003) showed that the timely application of therapeutic interventions is often an important factor in the success of therapy. Beck et al. (2004) considered the use of effective techniques at inappropriate times as the reason for the patient’s non-compliance with treatment.
Evaluating clients’ progress is also important. Accordingly, many therapists acknowledged that the most common reason for giving up the treatment was that clients were unaware of how well they were progressing in the treatment process. Thus, the therapists must have some tools to measure clients’ progress in the treatment sessions. Schartz and Fliwers (2006) believe that if the results of these evaluations indicate progress, positive expectations of treatment are reinforced, and if no progress is made, clients and therapists can adjust the treatment approach more effectively.
The Therapist’s Errors
Resolving individual errors of the therapist requires the therapist’s self-awareness and mindfulness in the treatment session. The therapist needs to reach self-knowledge to be able to recognize and name his/her distortions. There is a serious barrier to treatment when the therapist’s cognitive distortions match the patient’s distortions. Oasi et al. (2019) considered the therapists’ errors to be wrong diagnosis, acting out, inappropriate interventions, collusion, pejorative communication or even the non-recognition of the goals achieved or reachable by the patient, attributing them to unsolved relationship problems of the therapist. They also suggested that a high level of narcissism can harm a positive and emphatic attitude. In a qualitative study of clients’ experiences of successful psychotherapy, Oasi et al. (2019) stated that the most prominent issue is having a relationship with a wise, warm, and competent professional. Binder et al. (2009) and Grenyer and Lewis (2012) reviewed the data on client complaints and found that older psychologists and those with higher education were less likely to be exposed to client complaints. However, most participants in the study acknowledged that experience, age, and education were not associated with errors during their professional careers. In addition, several studies on the therapeutic effects have shown that some of them can be potentially harmful to the patient and worsen the patient condition compared to their colleagues (Saxon & Barkham, 2012). According to Swift et al. (2018), one of the most implicated concepts in unsuccessful psychotherapies is the therapeutic alliance and, in particular, the therapist’s ability to repair alliance rupture when they occur. In other words, age, antisocial behavior, level of intelligence (O’Keeffe et al., 2018), or intrapsychic functionality (Rubin et al., 2018) are certainly involved in the premature termination of the treatment. Trimboli et al. (2016) considered psychotherapists themselves as an alternative way to prevent treatment errors. An increasing number of studies have supported the idea that individual therapy enhances professional growth by increasing empathy for clients, learning and mastering healing skills, and understanding their own problems, conflicts, and values (Orlinsky et al., 2011). Psychotherapists’ subjective experiences seem to be associated with the belief in increased therapeutic competence (Moe & Thimm, 2021). Bruce et al. (2010) pointed to the role of therapist mindfulness in the treatment process, which can pave the way for developing a useful clinical relationship and psychotherapist characteristics such as empathy, openness, acceptance, and compassion (Grenyer & Lewis, 2010).
Furthermore, it seems that the therapist’s self-awareness of how empathy, positive attention, originality, unity, goal consensus, and cooperation affect the outcome of treatment is essential for the therapist’s growth (Moe & Thimm, 2021). Lindgren and Rozental (2021) reported that the clients' complaints were the constant cancellation of sessions, the change of schedule, and the difficulty in contacting a psychologist, or a change in treatment. Yalom (2003) considered their life as the best way for them to become aware of and learn about psychotherapy. Therapist interaction can play an important role in psychotherapy outcomes, especially in the treatment of personality disorders (Colli & Ferri, 2015).
Treatment Space
Another dimension of errors that receives less attention is the treatment space. Many participants attributed the dropout and treatment errors to the treatment space. The findings of the present study highlighted the importance of the treatment environment and the clinic secretary’s treatment of clients, which perhaps can lead to treatment errors and complicate the process of psychotherapy. Holmes (2012) believes that some therapists do not care about their surroundings, and the room that the therapist uses and its arrangements are very important and it is important that the room is as quiet as possible. Pearson and Wilson (2012) consider the most important components of a treatment room to be the location of the chairs, the size of the room, the use of color, light, access to the outside, sound insulation, fresh air conditioning, and decoration.
Non-Compliance with Ethical Principles and Standards
The psychotherapists in the present study also highlighted the importance of professional ethics. Accordingly,Garger et al. (2020) reported professional ethics is important not only in medicine but also in psychotherapy. Moreover, Phares and Trull (2002) showed that one of the criteria for professional maturity is the degree of commitment of that profession to ethical standards. Welfel (1998) also showed that members of the profession claim that if professionals are to have a professional identity, they must either be familiar with ethical standards or adhere to them. Casement (2002) argued that one of the therapists’ errors is related to cultural factors (ethnic prejudices, belief systems, social values, etc.)
Breaking boundaries such as financial transactions, breach of confidentiality, over-disclosure, meeting extension, inter-session phone calls, out-of-office meetings, joint activities, etc. can also be potentially detrimental to the client's well-being. All of these unethical actions break the basic trust between the therapist/counselor and client. Moreover, poor professional standards, such as poor reporting, poor or fraudulent accounting, and rude or insensitive relationships are also forms of physician’s abuse. It is essential to identify therapist variables that are prone to treatment-induced deterioration and to examine their possible interactions with traumatic therapies (Wampold, 2001).
The findings of the present study indicated that dual or multiple relations with clients could be harmful for the therapeutic relationship between counselor/client. Consistent with the findings of this study, Hari (2018) maintained that some patient reports of negative experiences of treatment referred to therapists’ immoral behavior. In addition, some patients described therapists as lacking basic treatment skills, such as empathy and listening skills. Likewise, Hardy et al. (2017) showed that some clients were harmed, willingly or unwillingly in relationship with the therapist. Tompson and Rudolf (1996) also considered judging the client as one of the therapy’s errors and prohibitions.
The Failure to Giving Adequate Information to Clients
Gerger et al. (2020) also argued that during the course of psychotherapy, therapists should remain in dialogue with the patient about the process of change during or after the end of psychotherapy. One of the important things to consider is the strengths of the clients. According to Cozolino (2004), when diagnosing clients’ problems and treating them, always remember that each client has at least one strength.
One of the reasons that clients are reluctant to continue treatment is that they do not participate in the treatment process and do not have the necessary motivation for change. As Lindgren and Rozental (2021) noted, clients complained of a lack of cooperation between themselves and the therapist. Freeman and McGlossky (2003) considered the lack of motivation for change as a barrier to treatment and stated that clients need to have the motivation to go through the stages of change. Clients are often hardly involved in the treatment process (Hardy et al., 2017). From an ethical point of view, transparency in psychotherapy is essential and serves to respect and protect the patient's independence (Trachsel et al., 2021). Meyer et al. (2002) showed that when clients are induced to hope for treatment outcomes, the likelihood of their active participation increases. Furthermore, Schartz and Fliwers (2006) suggested that therapists need to search for clients’ capabilities and talents systematically as well as seek valid clinical diagnoses.
Conclusion
As Budge (2016) pointed out, the field of medicine is light years ahead of psychotherapy, with journals and conferences focusing specifically on the mistakes and errors that physicians make and how to address and prevent them. The results of the present study indicated that it is better to look for the errors that occur in the treatment process instead of attributing the causes of abandonment and ineffectiveness of psychotherapy to the clients and the clients’ resistance. Training and attending specialized courses and high experience alone cannot protect clients from the psychotherapist’s mistakes because the therapist’s vulnerabilities and cognitive distortions can affect the training outcomes. Clients are emotionally disturbed and overwhelmed by their problems when they seek psychotherapy and counseling and do not notice the mistakes and harm that the therapist inflicts on them. Perhaps receiving feedback from clients, colleagues, and professors, continuous review of treatment sessions, individual treatment before entering the psychotherapy profession, and also conducting more extensive studies in this field are some measures that can be taken to reduce the frequency of therapeutic errors.
Limitations
One of the limitations of the study was that some interviews were conducted through telephone and video calling due to the COVID-19 pandemic in Tehran at the time of the study. Another problem was the unavailability of clients and their treatment records due to the premature termination of the treatment process.
Implications and Suggestions
Given the different dimensions of therapeutic errors as highlighted in this study, quantitative studies need to examine the prevalence of each type of therapeutic error and its negative consequences among psychotherapists. Following the findings of this study, it is essential to develop a plan to evaluate psychotherapists’ mental health in the process of psychotherapy to ensure their mental health. There are many questionnaires and self-assessment tools in the profession of psychotherapy and counseling. Thus, following the insights from this study, a standard criterion can be developed to measure and evaluate therapeutic errors and this criterion can be used in all therapeutic approaches. Counselors and psychotherapists do not notice malpractices as they are overwhelmed by their problems, and of course, they hurt the clients in the treatment process. Thus, counselors can be informed of the errors commonly committed by them by preparing and reading the research findings and they can get help from other expert counselors.
Ethical Considerations
All participants in this study were aware of the goals of the study and everything that might affect their willingness to participate in the interviews. Thus, they were not forced to attend the interview sessions and written and oral informed consent was obtained from the participants. The interviews were recorded with the participants’ permission and the recorded voices were deleted after transcribing the content of the interviews. This research project was approved by research committee.
Footnotes
Acknowledgements
The authors would like to appreciate managers and staff of private counseling and psychotherapy clinics in Tehran and all participants in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
not applicable.