
Abstract
The Covid-19 pandemic has had an irreversible impact on the global economy and industries, particularly in the healthcare sector. The rush to respond to the pandemic, particularly in terms of getting treatment and vaccines and technology to market, has created a huge opportunity for undisclosed corruption and misconduct in the research and development and procurement processes. Effectively responding to current and future global health corruption threats is critical if the world is to provide health care to all. Due to a lack of research in preventive corruption measures in the healthcare industry, this paper aims to provide an overview of anti-corruption efforts among healthcare companies listed on the main board of Bursa Malaysia. The disclosure index is made up of 47 items derived from a review of previous literature and the Malaysian Anti-Corruption Act. The content analysis research method is used to analyze information from 13 companies listed in 2020’s anti-corruption policies and procedures published on their website, board charter, whistleblowing policy, code of ethics and conduct, annual report, sustainability report, and corporate governance report. According to the findings, Malaysia’s healthcare industry has demonstrated a strong commitment to fighting corruption, with 76.9% of companies scoring higher than average on the disclosure index.
Plain Language Summary
Purpose: This paper aims to provide an overview of anti-corruption efforts among healthcare companies listed on the main board of Bursa Malaysia. The disclosure index comprises 47 items derived from a review of previous literature and the Malaysian Anti-Corruption Act. Methods: The content analysis research method is used to analyze information from 13 companies listed in 2020's anti-corruption policies and procedures published on their website, board charter, whistleblowing policy, code of ethics and conduct, annual report, sustainability report, and corporate governance report. Conclusions: According to the findings, Malaysia’s healthcare industry has demonstrated a strong commitment to fighting corruption, with 76.9% of companies scoring higher than average on the disclosure index. Implications: Government should consider reducing political influences in private healthcare management to ensure a more transparent procurement process. Companies should conduct risk assessments for corruption, as an effective anti-corruption programme lies in assessing the corruption risk of a business organization. Accountability, transparency, and an open and fair tender system that does not favor well-connected interest groups are also essential; selection should be based on experience, knowledge, and managerial competencies. Limitations: This study only includes healthcare companies that are listed on the main board of Bursa Malaysia. As such, the finding cannot be generalized to other healthcare companies. Second, the results will undoubtedly raise issues about whether disclosures on anti-corruption policies mitigate corruption practices during the pandemic and what factors lead companies to disclose more on specific information while being hesitant to do so on other information. These issues deserve future research attention.
Keywords
Introduction
Corruption is one of the most significant barriers to many people around the world receiving quality healthcare. Corruption also impedes progress toward the goal of Universal Health Coverage (UHC), which is based on the principle that all individuals and communities should be able to access the essential health services they require without financial hardship (Via, 2020). According to the World Health Organization (WHO), corruption in the health sector is an open secret that leads to financial waste and has serious consequences for five dimensions of health system performance: access, quality, equity, efficiency, and resilience of health services. According to Transparency International, the world spends more than US$7 trillion on public health services each year, with approximately US$500 billion lost to corruption, far more than would be required to achieve universal health coverage. Corruption occurs not only in public health but also in legitimate corporate entities. The increased competition among pharmaceutical companies to enter emerging markets has increased the possibility of corrupt practices flourishing. Several multinational pharmaceutical and medical device companies, including Johnson & Johnson, Pfizer, Merck, Eli Lilly, and Medtronic, have been accused of bribing physicians and health officials (Mackey & Liang, 2012). Novartis, a Swiss-based global healthcare company, recently agreed to pay a fine of over US$678 million to settle violations of US anti-bribery laws for paying illegal kickbacks to doctors and patients to increase drug sales (Kohler & Wright, 2020).
Corruption in the health sector is more prevalent during a crisis or an emergency. The COVID-19 pandemic has exposed flaws in the healthcare systems of many countries, resulting in acute and severe shortages of essential equipment such as personal protective equipment, diagnostics, clinical management, and the need for financial assistance. According to Kohler and Wright (2020), urgency, demand, and scarcity have put a new strain on global supply chains, leaving many governments vulnerable to market-distorting effects such as price manipulation and purchases of defective or false goods. Furthermore, the covid-19 outbreak revealed serious flaws in national and international plans for pandemic containment, as well as a lack of focus on good governance and preventing corruption in the healthcare sector, particularly in the procurement process (Teremetskyi et al., 2021). Corruption will undermine the response and deprive people of health care in the absence of good governance and proper regulation, which should be the ultimate priority of all governments during pandemics.
Even though corruption in the healthcare sector is one of the prominent issues to be discussed, our reading indicates that there has been little interest in studying corruption in the health sector, particularly in Malaysia. Similar to other ASEAN countries, Malaysia’s environment is characterized by a plurality of healthcare options, a sizable unregulated health market, and lax regulatory standards, all of which have contributed to favorable conditions for corruption (Naher et al., 2020). Therefore, this research aims to provide evidence of health-related companies’ commitment to preventing corruption by examining the extent of anti-corruption efforts through transparency among healthcare companies listed on the main board of Bursa Malaysia, particularly during the first year of COVID-19 pandemic. Transparency in anti-corruption efforts is critical for improving companies’ ability to establish policies and procedures and improve the effectiveness of internal controls against corruption (Nobanee et al., 2020), especially during significant health crisis. The disclosure also provides evidence of a well-implemented program rather than a paper-based but ineffective compliance program (Hess, 2012). As previous crises have demonstrated, anti-corruption measures are even more crucial during times of medical emergency. For instance, corruption hampered the response to both the Ebola and the H1N1 pandemics because public funds were wasted, there was a lack of transparency, and pharmaceutical companies were included in the decision-making process for their own gain (Bîzoi & Bîzoi, 2022).
It is crucial to study the seriousness of healthcare providers in preventing corruption since the government has made a sizeable financial commitment to delivering high-quality healthcare services. For 2023 budget. Malaysia’s health ministry has received RM36.3 billion, mostly for medicines, reagents, vaccines, and consumables, as well as the replacement of old equipment. The proportion will also be used for the appointment of new medical officers, dentists and pharmacists for permanent and contract positions (Budget, 2023). Even though the budget is for the public health system, it has an impact on the private healthcare provider since majority of Malaysian private healthcare companies are government-owned (Lee, 2015). Additionally, actors of health sector in both public and private sector need to join force to combat corruption and strengthen the healthcare system. A healthcare system that is rife with corruption will result in the misappropriation of public funds for the benefit of unreliable individuals or groups. Government funds that should have been used to improve the country's health status have been lost because of this situation, depriving citizens of their constitutionally guaranteed access to quality healthcare. Consequently, preventing corruption in the healthcare sector is crucial to ensuring a better healthcare system and supporting the advancement of Sustainable Development Goal (SDG) No. 3 of the United Nations (UN), to improve healthy lives and promote well-being for all, particularly in achieving universal health coverage (UHC), including access to quality essential health care services and access to safe, effective, quality, and affordable essential medicines.
This paper contributes to the literature in several ways. First, it focuses on the attitudes of healthcare companies toward corruption. Despite being one of the most vulnerable industries to corruption, this sector is rarely investigated in Malaysian corruption cases. Second, our study provides regulators with information on the commitment of healthcare industry players to combating corruption, which indirectly assists regulators in determining the adequacy of the health sector’s anti-corruption program. The rest of this paper will go as follows. The review of the literature is presented in Section 2. Section 3 describes the methodology, followed by Section 4’s analysis of the results. The conclusions and discussions are presented in Section 5.
Literature Review
Corruption in the Healthcare Sector
Healthcare is a big business all over the world, which makes it an appealing target for corruption. Although corruption in the health sector is a problem in all nations, it is particularly severe in emerging and transitional economies where public resources are already limited. The sector is prone to corruption due to a combination of factors such as the complex environment marked by high public spending, a mix of public and private sector providers, market uncertainty, and asymmetry of information in which numerous actors such as regulators, providers, payers, suppliers, and consumers interact at multiple levels and involved in illness care, the uncertainty that surrounds the illness experience, and the challenges of ensuring accountability in complex health systems (García, 2019; Mackey et al., 2016; Naher et al., 2020). Furthermore, the healthcare industry is one of the world’s largest employers, employing thousands of health professionals who treat millions of patients, creating a breeding ground for petty corruption (Teremetskyi et al., 2021).
Another reason for the persistent corruption is the presence of vague and ambiguous concepts, where certain activities may lack clear guidelines or regulations, creating confusion and uncertainty. Consequently, individuals seeking to access healthcare services might perceive bribery as the only option available to navigate the system effectively (Sánchez-Duque et al., 2021). Certain features in today world also make the issue of corruption in the healthcare sector is on the rise. For instance, increasing health care costs, an ageing population, the complexity of chronic and non-chronic diseases, pandemics, pressure to buy expensive, high-tech equipment, and expensive drugs pushed by powerful pharma companies place increasing pressure on the health system and governments and act as havens for corruption (Bîzoi & Bîzoi, 2022).
During the Covid-19 pandemic, the risk of corruption heightened in the healthcare sector due to increased supply and demand imbalances, the presence of uncertainty, distraction from core activities, and the disruptive changes introduced in response to the crisis. These factors collectively provided fertile ground for corrupt actors to take advantage of the situation, leading to the undermining of healthcare systems and compromising the delivery of critical services during a time when they were needed the most (Teremetskyi et al., 2021). Rose-Ackerman (2021) argue that covid 19 pandemic has created more incentives for corruption in healthcare sector, since the sector has market imperfections, particularly in the insurance markets. Some support the private sector’s reliance, claiming that it can develop necessary medical solutions successfully without government intervention and favors individual choices over lockdowns. This viewpoint, however, ignores the healthcare market’s inherent flaws. Customers frequently lack knowledge of appropriate treatments, highlighting the demand for skilled and moral healthcare professionals. Because people may not accurately disclose their health conditions, which can affect pricing and the availability of coverage, the insurance industry is vulnerable to moral hazard and adverse selection. Moral hazard results in excessive healthcare demands, rising insurance costs, and coverage restrictions.
According to Lewis (2019), the most insidious and deeply ingrained corruption in the health sector is organized crime, which deals in fake drugs and substandard inputs, undermining patient treatment. One of the most well-documented examples of this was high-level forgery drugs trading in Nigeria in the early 2000s, when 70% of drugs in circulation were forgeries, resulting in unnecessary deaths and the exodus of major pharmaceutical companies unable to compete with illegal producers. Similarly, Vian (2020) reports that a systematic review and meta-analysis of 96 studies published before November 2017 discovered that 13.6% of essential medicines tested in low and middle-income countries failed quality analysis overall, with an 18.7% regional prevalence in Africa and 13.7% in Asia. In accordance with a World Health Organization (WHO) report, 17% of antibiotics, 20% of malaria medications, and 9% of anesthetics/analgesics that were distributed worldwide were either substandard or fake (Glynn, 2022). One possible factor causing the circulation of fake medical supplies is poor governance in many low- and middle-income countries, where the regulatory capacity is insufficient to ensure the authenticity of these products. This regulation is made more challenging by the fact that many of these supplies are the end product of complex global supply chains (Glynn, 2022).
Another significant issue in the industry is corruption in the recruitment and promotion of healthcare workers, which leads to a decrease in the motivation and working capabilities of front-line health providers. Personal and political recruitment leads to subpar healthcare and an increase in the community’s death rate. Choosing less qualified and unsuitable candidates over deserving candidates, as well as elevating underqualified professionals, has irreversible and catastrophic consequences for the community (Sánchez-Duque et al., 2021). Besides, absenteeism is another issue relate to personnel, where health worker is legally employed but frequently absent without a valid excuse. One factor that contributes to a high absenteeism rate is when doctors spend their paid time in private practices, use public resources such as equipment and facilities to treat private patients, or simply use the public system to refer patients to their private practice. All of these activities result in a significant waste of money and public resources (Nordberg & Vian, 2008).
In addition, healthcare professionals accept informal payments as another form of corruption at different stages of patient care to receive better care, such as paying to enter a facility, reserve a bed in a hospital, or use a trolley to transport patients (Naher et al., 2020). According to Vian (2020), a recent systematic analysis of 38 studies on the methodology and burden of informal patient payments discovered that 2 to 80% of respondents had made informal payments. In many cases, receiving unofficial payments from patients is acceptable to supplement the meager salaries that medical professionals receive in those nations. Although the majority of healthcare consumers make informal payments in order to receive better care, informal payments are sometimes made as a sign of gratitude for the services received in other countries (Zuniga, 2018).
Effect of Corruption to Health System
Health sector corruption comes at a high price in terms of lives lost and resources wasted. Children’s deaths and other adverse health outcomes are also significantly predicted by corruption. According to a World Health Organization (2019), corruption is responsible for 140,000 child deaths annually, which is more than the combined toll of rabies, cholera, and Ebola. Corruption in the health sector has severe consequences for i) access, ii) quality, iii) equity, iv) efficiency, and v) efficacy of healthcare services (Hussmann, 2020; Usman et al., 2022). Access to health care can be harmed significantly by medical staff absenteeism and the use of official working hours for personal affairs or side work. Theft, embezzlement, bribery, and demands for informal payments or bribes in exchange for services that citizens are entitled to receive for free also jeopardize access to critical medications, equipment, and supplies (Zuniga, 2018). According to a review of studies conducted in Eastern Europe and Central Asia, corruption in the form of unofficial payments for care restricts access to services, especially for the poor, and slows down the behaviour of those who need care (Nordberg & Vian, 2008; Vian, 2020).
Corruption can significantly impede the quality (satisfaction) of care and medical drugs, as patients may be charged for fake diagnostics, substandard treatments, or no treatment. Drug fraud can result in serious illness, even death, as well as the spread of bacterial or viral strains that are resistant to common antibiotics both domestically and internationally (Hussmann, 2020). Other issues affecting quality include referrals motivated by kickbacks, unnecessary procedures, and denials for high-quality medicine (Gonzalez-Aquines et al., 2021; Hussmann, 2020). Vian (2020) state that informal payments result in lower service quality, as evidenced by lengthy wait times, a shortage of medicines, a lack of staff, and disrespectful behaviour.
Corruption’s impact on equity is a major source of concern. Equity dictates that cases with similar facts must be handled similarly, while cases with different facts must be handled differently (Kang et al., 2020). Informal payments contribute to health inequities, tending to deter poorer people from using both essential and non-essential services, leading to untreated morbidity (Friel & Melzer, 2020). Families become impoverished further when they are forced to sell assets or incur debt to pay bribes for health services they should have received for free (Hussmann, 2020). Further, (Vian, 2020) suggest that dual practice may lead to inequity in health worker distribution particularly in low-income or rural areas. Healthcare professionals might prefer to work in urban or wealthy areas where the private sector offers higher wages and better working conditions. This results in fewer healthcare providers serving underserved areas, which causes disparities in access to healthcare services and health outcomes.
Furthermore, the availability and use of scarce resources are particularly affected by corruption, which has a significant impact on the efficiency of the health sector, which results in increased drug prices and eventually reduced public spending on education, health, and social protection (Hussmann, 2020). Resources within the healthcare system may be misallocated because of corruption. It is possible to embezzle or divert money meant for medical equipment, supplies, and infrastructure in the healthcare industry. A lack of vital resources could result from this, which would make it more difficult to deliver healthcare services effectively and would compromise patient care. Additionally, healthcare professionals who witness or experience corruption might lose hope and their commitment to supplying effective and efficient care.
Finally, in terms of efficacy, corruption in the health sector has a detrimental effect on the population's health and is associated with poor health outcomes, posing a barrier to the long-term goal of universal health coverage, (Hussmann, 2020). Infant, child, and maternal mortality are more pervasive in nations with higher levels of corruption. According to estimates, corruption may be indirectly responsible for 140,000 child deaths annually, or 1.6% of all child fatalities worldwide (Vian, 2020).
Healthcare Sector in Malaysia and Pandemic Management
Malaysia is one of the Southeast Asian countries that provide medical tourism with advanced private medical centers which offer high-quality treatments at lower prices. This creates a significant separation between public and private healthcare providers and the distinct population in the country. There are two healthcare systems in Malaysia: a public-private system, in which the Ministry of Health (MOH) serving as the primary central administrative authority for the delivery of public health service. This allows the mobilization of appropriate resources from national to state levels to support response at the facilities (Md Hamzah et al., 2021). The MOH has played a tripartite role as a funder, provider, and regulator (Lee, 2015). The public health provider is scattered throughout Malaysia, from rural areas to large cities; meanwhile, private healthcare centers are developed in urban areas to cater middle class, which pursue exclusive and faster medical treatment (Barraclough, 1997). The public healthcare system is mostly financed through taxation and other public income. Public healthcare is substantially subsidized, with extremely low user fees and estimated revenue collection of approximately 2% of its expenditures (Lee, 2015). The private healthcare sector is underpinned by private healthcare insurance funds, patients' out-of-pocket expenditures, and private and non-profit institutions (Ching et al., 2021).
The budget allocation by the government to MOH is important to enable the ministry to provide essential healthcare facilities and services to the public, especially in dealing with the Covid-19 pandemic (Arumugam, 2020). A substantial proportion of the budget has been allocated to MOH every year due to its significant impact on the public. In the latest 2021 Budget, the healthcare sector is among the top three ministries which received the highest allocation of the budget after the education and finance ministries. More funds allocated are expected to enhance the healthcare sector by providing an effective national healthcare system. The consumption includes the development of more hospitals and clinics, supported with the latest medical vehicles and equipment and also used in upgrading and maintaining the existing hospitals and clinics (Syed Jaafar, 2020). In 2019, Malaysia was ranked 18th out of 195 countries in a global health security index study for its overall readiness to face a disease outbreak, based on its capabilities to prevent, detect, and respond to an epidemic, including its overall health system, risk management, and compliance with international norms. In 2020, among all sectors in Bursa Malaysia, the healthcare sector outperformed the most, gaining a 93.8% year on year change in market capitalization driven by higher demand for medical gloves due to the pandemic (Security Commission Malaysia, 2020).
Despite being among the highest receiver of government funds, the MOH is still striving to provide the optimum level of services using its facilities, equipment, and technologies. Common issues include the healthcare staff attitudes, unhygienic facilities and equipment, patient’s long waiting time, insufficient medicine and the tendency to compromise the health-related safety and security procedures by both staff and patients (Malakoane et al., 2020). Even though Malaysia surpasses the World Health Organization’s ratio of doctors to population, which Malaysia recorded a ratio of 1:482 (Ministry of Health Malaysia, 2020), compared to the world ratio, that is, 1:1,000 (Kumar & Pal, 2018), the audit report by the National Audit Department revealed that the emergency and trauma department (ETD) at Malaysian hospitals are deal with understaffing, overcrowded patients, underfunded and inadequate facilities and equipment (Aliman, 2019).
During the Covid-19 pandemic, the government of Malaysia followed the procedures set by World Health Organization (WHO) to control its spreading and transmission. The MOH was instrumental in ensuring maximum preparedness to contain the spread of the virus. Malaysia’s public healthcare systems are under a heavy burden due to the country’s high rate of susceptible COVID-19 patients, as Malaysians were also not well prepared to combat the pandemic, due primarily to the concurrent political crisis. Hence, MOH had to approach to the private sector to collaborate in managing the pandemic. Finally, patients with Covid-19 were also treated at 95 private hospitals with internal medicine specialties in collaboration with the MOH (Ching et al., 2021). Further, The COVID-19 Fund was launched by the government to raise money for patients, particularly those who have been financially impacted by the quarantine procedure, to help alleviate the consequences of COVID-19. Donations worth a total RM 1 million from the public and private sectors established this fund. Contributions from people and NGOs were also welcomed. During the quarantine and treatment processes, a direct cash assistance was distributed through this fund to those who had no other source of income. Additionally, the funds were used to cover medical costs, including the acquisition of essential resources and other supplies. After the general election in November 2022, Ministry of Finance (MOF) had acknowledged several breaches involving the funds, and in the middle of December 2022, Malaysia Anti-Corruption Commission (MACC), raided nine companies and eight government agencies for their alleged involvement in misappropriation of RM92.5billon in Covid-19 funds (Perimbanayagam, 2022).
Vaccination is another strategy to combat the Covid-19 pandemic, and the government of Malaysia provides free vaccinations to its citizens in stages. There are reports that doctors or other parties may be solicited bribes to issue vaccination certificates even though no vaccines were administered. In addition, under the state of emergency, the minister of the Department of Health confessed that many of the department’s procurement processes did not adhere to proper protocol. Corruption in the procurement process in the healthcare sector is not a new problem in Malaysia. There are several cases reported and charged by MACC regarding corruption in medical suppliers to public hospitals involving hospital staff and officials. For example, in 2013, a doctor was charged for demanding a bribe to recommend a few medical supplies to the hospital (Army Doctor Charged in RM700,000 bribery case, 2013). During the Covid-19 pandemic, MACC opened 25 investigation papers regarding corruption in the procurement of medical equipment and medicine.
Methodology
This paper examines the anti-corruption efforts in the healthcare industry in Malaysia during the pandemic covid 19. There are 13 companies listed in the healthcare sector on the main board of Bursa Malaysia in 2020. Companies listed in this sector are either involved in pharmaceuticals, owners, or providers of healthcare facilities, including hospitals, clinics, nursing homes, rehabilitation centers, manufacturers, and distributors of healthcare equipment and services, including lab testing services and dialysis centers. As for capturing data for companies’ anti-corruption efforts, this study uses content analysis. While content analysis has limitations, such as subjectivity in text interpretation (Lombardi et al., 2019), it is a method that is widely used in corporate disclosure studies and is relevant in measuring anti-corruption reporting (Dissanayake et al., 2011; Joseph et al., 2016). This instrument produced a quantitative scale, and the disclosure level can be treated as a continuous variable. A vital step in employing this approach is to determine a set of rules of “what” and “how” to code, measure, and record the documents (Sari et al., 2021). Hence, a unit of analysis is first needed to determine for coding, measuring, and recording the disclosures examined in this study.
There are two general approaches to determining units of analysis. First, the approach is based on the disclosure’s amount, extent, or richness. The amount of disclosure reflects the degree of importance that a company attaches to the issue. To measure the level of disclosures, prior literature has relied on the number of sentences, the number of words, or the number of pages. The second approach is based on a dichotomous measure to assess the availability of thematic disclosure or index measure. This approach often uses a basic binary coding scheme, which records the information’s presence or absence. For example, an item in the research disclosure index scores one if disclosed and zero if it is not disclosed. There is no penalty if the information disclosed is not relevant to the disclosure index. Finally, each item’s scores were then added to derive a final score of the disclosure index. As such, this study used the second approach. The availability of the thematic disclosure of anti-corruption activities will be coded as “1” if the item is disclosed and “0” if not. The disclosure of information related to anti-corruption was derived from annual reports 2020, corporate governance reports, board charters and companies’ websites from June to December 2020.
The data were collected based on the analysis of annual reports, corporate governance reports, sustainability reports, codes of ethics, and board charters for the year 2020. The index for anti-corruption reporting is adapted from (Barkemeyer et al., 2018; Islam et al., 2018; Issa & Alleyne, 2018; Joseph et al., 2016). The index was categorized into nine (9) themes with forty-seven (47) subcategories. The themes include 1) Accounting for combating corruption; 2) Board and senior management responsibility; 3) Building human resources to combat bribery; 4) responsible business relation; 5) External verification and assurance; 6) Codes of conduct relates to corruption practice; 7) Whistleblowing policy; 8) Action taken in response to corruption; 9) Risk exposure related to corruption. The score of each nine categories and the total disclosure score is calculated as follow:

Where: N = number of items expected for j firm,
Xj = total number of items disclosed
Analysis of Result
Table 1 below depicts the disclosure index score on anti-corruption for thirteen healthcare companies listed on Bursa Malaysia’s main board. The index score is calculated for every theme. Overall, all companies have disclosed their anti-corruption practices as Bursa Malaysia has amended the listing requirement for the main board, which requires the listed issuer and its subsidiaries to establish and maintain anti-corruption and whistleblowing procedures. Another amendment requires a listed issuer to publish an anti-corruption policy and whistleblowing policy and procedures on its website. However, what is more crucial about the procedures is the quality of the information disclosed during the procedure. From the table, the lowest score is 0.426, the highest score is 0.777, and 10 companies or 76.9% of total companies score more than average, indicating a good commitment from the companies in the healthcare sector to disclose information about anti-corruption.
The Score of the Anti-Corruption Disclosure Index for 13 Healthcare Companies in Malaysia.
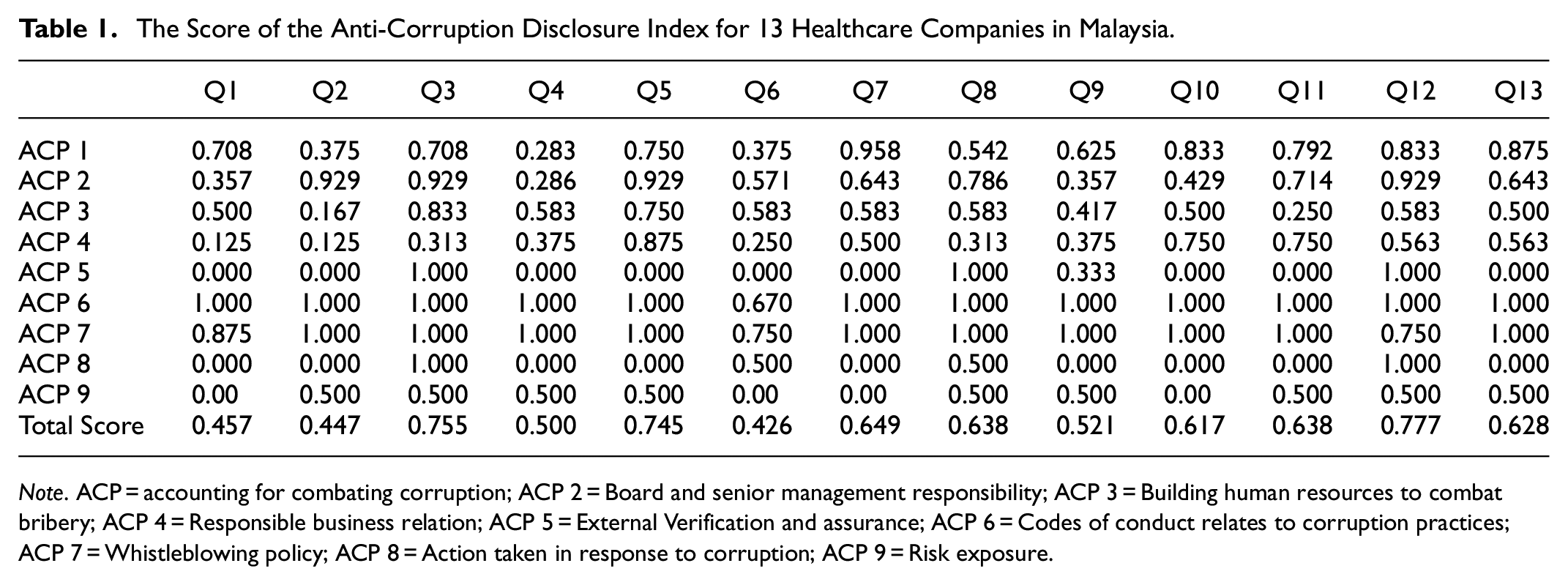
Note. ACP = accounting for combating corruption; ACP 2 = Board and senior management responsibility; ACP 3 = Building human resources to combat bribery; ACP 4 = Responsible business relation; ACP 5 = External Verification and assurance; ACP 6 = Codes of conduct relates to corruption practices; ACP 7 = Whistleblowing policy; ACP 8 = Action taken in response to corruption; ACP 9 = Risk exposure.
ACP 1 represent the strategy disclosed in accounting for combating corruption, where only 23.1% of the companies score lower than average score showing decent disclosure on the process of internal control systems in combating corruption. Most companies omit the information regarding the prevention of maintaining off-the-books accounts and feedback mechanisms on the internal control system. ACP 2 provides information regarding board and senior responsibility for anti-corruption. There are seven indicators under this category, and only two companies provide only two or less information on this category. The board of directors of all 13 companies assures that they are committed to complying with all relevant anti-corruption laws and made compliance with the anti-corruption program mandatory for the board of directors and top management. But most companies did not provide information on the commitment by any responsible management to periodically report the anti-corruption procedure review result to the board.
ACP 3 illustrates information on practices in human resources to combat corruption. Eighty-five percent of the companies make sure that their directors, managers, employees, and agents receive appropriate training on anti-corruption programs showing the anti-corruption programs have been well communicated to the members of the companies. However, only 38.5% of the companies keep records percentage of employees trained. ACP 4 demonstrates disclosure on business dealing with associates, including agents, consultants, suppliers, joint ventures, and many others. Most companies score lower than average score. None of the companies ensures that agents are only paid for legitimate services, but all companies are committed to conducting fair and transparent procurement practices. In contrast to the commitment, only seven companies undertake due diligence in evaluating their business associates before appointment and engagement and very few conduct regular monitoring on significant suppliers.
ACP 5 presents external verification and assurance, and the result indicates that only a small portion of companies provide external assurance statements. Meanwhile, ACP 6 provides information on codes of conduct related to corruption practices. It can be seen from the table that almost all companies get full scores for this category. Only one company scored 0.67 for not monitoring the implementation of the code. ACP 7 demonstrate information regarding whistleblowing practices. 76.9% of the companies earned a total score, indicating that most of the companies have established, reviewed, and implemented policies on whistleblowing. ACP 8 illustrates action taken for any corrupt offence. Only two companies provided information on the number of confirmed employees and contracts terminated due to corrupt activities. While the other two companies only provided information on employee-related corruption incidents. Lower reporting of external verification and confirmed corruption cases may be due to the company’s belief that reporting on these two pieces of information will negatively affect a company’s reputation, as companies involved in corruption are expected to face negative consequences, particularly from business associates.
Finally, ACP 9 presents information on risk disclosure. Nine of the companies scored 0.5, which indicates the companies made a report on the corruption-related risk identified through risk assessment. And none of the companies reported on the percentage of the operation units assessed for corruption risk. Even though risk exposure is a fundamental element in anti-corruption practices and is the first step in developing effective anti-corruption policies, some companies do not conduct any assessment of risk at all. This is not a good sign of effective anti-corruption strategy as risk assessment is most critical part in anti-corruption strategy because it identifies vulnerabilities, allows for targeted interventions, optimizes resource allocation, and promotes transparency and accountability. It assists organizations and institutions in taking proactive steps to prevent corruption, detect and respond to corrupt practices, and foster an integrity and compliance culture.
Conclusion and Discussion
This study assesses the extend of anti-corruption disclosure among healthcare companies listed on the main board of Bursa Malaysia during the pandemic. Our results show a satisfactory level of disclosure made by healthcare companies on anti-corruption practices during the Covid-19 pandemic. 76.9% of the companies, or ten out of thirteen companies, score more than average for the total score of the anti-corruption disclosure index. This is higher than the mean score of the one Malaysian based descriptive study conducted by Joseph et al. (2016), where the range of the mean of anti-corruption policies for all seven themes in their study fell between 0.185 and 0.27. However, their sample only included 24 listed companies that participated in ACCA Malaysia Sustainability Reporting Awards (MaSRA) in 2011. The improvement in anti-corruption efforts may be attributable to the government’s mid-2020 enforcement of corporate liability under the MACC Act 2009, which requires companies to demonstrate that they have the adequate procedures in place to prevent their employees and/or associated persons from engaging in corrupt business practices. The most disclosed categories are information on codes of conduct related to corruption and whistleblowing policies. This could be due to the implementation of the Malaysian code of corporate governance (MCCG) 2017, which requires companies to establish a code of conduct and ethics to manage conflicts of interest, prevent abuse of power, corruption, insider trading, and money laundering. In addition, MCCG 2017 practice requires the board to encourage employees to report genuine concerns about a legal obligation breach through the establishment and implementation of whistleblowing procedure. As a result of these practices, almost every company received a perfect score for disclosure on code of conduct and whistleblowing policies. Meanwhile, the majority of the company indicated minimal disclosure on external verification and assurance, which is consistent with Dissanayake et al. (2011) and Joseph et al. (2016) as well as the action was taken in response to corruption. This could be because the companies believe that reporting those two pieces of information will negatively affect their reputation because companies involved in corruption expect to receive a negative outlook, especially from their business associates. Further, companies may be hesitant to conduct due diligence and regular monitoring of significant suppliers to mitigate trust issues and maintain positive relationships with suppliers. Additionally, some of the healthcare companies are government link companies (GLCs), whereby the board of directors consist of elites from the ruling coalition and retired government bureaucrats, or jointly with capitalists enjoying links with them that will help companies in securing government contracts and benefit from preferential treatment by bureaucracy (Lee, 2015).
In Malaysia, privatization of some government departments have resulted in civil service management politicization, which allows the elite Bumiputera (indigenous race) of the bureaucracy to take on senior business management roles and functions in GLCs (Sinnadurai, 2018). Government-affiliated political leaders’ privatization efforts have produced a suboptimal outcome expressed by greater expenses. Malaysia government has privatized its non-medical services segment since 1994, including pharmaceutical store, hospital support services and health examinations of foreign workers. The government’s medical stores and laboratory concession were awarded to a corporation that had no experience in the industry but had links to the government. Meanwhile, hospital support services which accounted for 14% of the MOH budget, were privatized to three corporations, after which MOH expenditure went up by 3.2 times. None of the companies, however, had a background in the provision of the services that they were supposed to provide but had direct links to the government and indirect links through political patronages. Further, all three companies had to undergo a restructuring process subsequent to the 1998 economic crisis due to mismanagement (Lee, 2015). This situation needs to be rectified to reduce conflict of interest and the risk of corruption in the management of the healthcare industry in Malaysia. Government should consider reducing political influences in private healthcare management to ensure a more transparent procurement process. Companies should conduct risk assessments for corruption, as an effective anti-corruption program lies in assessing the corruption risk of a business organization. Accountability, transparency, and an open and fair tender system that does not favor well-connected interest groups are also essential; selection should be based on experience, knowledge, and managerial competencies.
Our study is subject to certain limitations. First, it only includes healthcare companies that are listed on the main board of Bursa Malaysia as such, the finding cannot be generalized to other healthcare companies. Second, our study is purely descriptive study and does not provide any insight into the causes of such disclosure. Our findings will undoubtedly raise issues about whether disclosures on anti-corruption policies really mitigate corruption practices during the pandemic, as well as what factors lead companies to disclose more on specific information while being hesitant to do so on other information. These issues deserve future research attention.
Footnotes
Appendix
List of 13 Healthcare Companies Listed in Bursa Malaysia Main Board.

| 1 | Adventa Berhad |
| 2 | Apex Healthcare Berhad |
| 3 | Duopharma Biotek Berhad |
| 4 | Hartalega Holdings Berhad |
| 5 | IHH Healthcare Berhad |
| 6 | Kossan Rubber Industries Berhad |
| 7 | Kotra Industries Berhad |
| 8 | KPJ Healthcare Berhad |
| 9 | Pharmaniaga Berhad |
| 10 | Supermax Corporation Berhad |
| 11 | TMC Life Science Berhad |
| 12 | Top Glove Corporation Berhad |
| 13 | Y.S.P Southeast Asia Holding Berhad |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to thank the Accounting Research Institute (ARI HICoE) Universiti Teknologi MARA, Shah Alam Malaysia; Ministry of Higher Education Malaysia; and Research Management Centre (RMC), Universiti Teknologi MARA, Shah Alam, Malaysia, for the research fund (600-RMC/ARI 5/3(010/2023).
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.