
Abstract
The importance of the first 1000 days of life for children has been acknowledged as a crucial phase for malnutrition prevention, where understanding the underlying causes of the problem should be done accordingly. Thus, the study’s objective was to find the factors associated with malnutrition in children under 2 years old. A crosssectional study was conducted involving mothers and children under 2 years old dyads (n = 244). A structured and validated socio-demographic and nutrition KAP questionnaire was used whilst weight and height were measured. In this study, 19.3%, 11.8%, and 10.2% of children were stunted, underweight, and wasted, respectively, according to the WHO Growth Reference cut-off. By using multiple logistic regression, this study found that children who have low birth weight and whose mothers have poor nutrition knowledge have higher odds of malnutrition. In conclusion, proper prevention planning considering these associated factors should be done to ensure the effectiveness of the malnutrition prevention program.
Keywords
Introduction
Malnutrition is defined as the deficiencies, imbalances, or excessive intake of energy and/or nutrients by a person (World Health Organization, 2020). It is one of the serious problems that has occurred for years in all age categories, including children under 5 years old. The prevalence of malnutrition in children under 5 years old worldwide has been well documented. It is estimated that in 2020, 45.4 million children were wasted and severely wasted, 149.2 million were stunted, and 38.9 million were overweight and obese (UNICEF/WHO/World Bank Group, 2020).
More than half of the malnourished children live in Asia. Although it has been documented that the prevalence of malnutrition among children in Asia, specifically in stunting, has decreased significantly from 37.8 million in 2012 to 21.8 million cases in 2020, the prevalence in Malaysia remained high (i.e., 18.3% in 2012 and 20.9% in 2020) (Institute for Public Health (IPH), National Institutes of Health, Ministry of Health Malaysia, 2019). Although many intervention programs have been implemented by the government in Malaysia, such as The Rehabilitation Program for Malnourished Children (PPKZM), Nutrition Counseling for mothers at the clinic, Baby-Friendly Hospital, and Breastfeeding Mother Support Group, there still exists heterogeneity in the interventions that focus only on children attending the government clinic and indigenous groups (Ministry of Health Malaysia, 2016). Malaysia is one of the upper-middle-income countries that face the dual burden of malnutrition, where one part of the children’s community suffers from obesity, and the other part of the children’s community suffers from stunting. The National Health and Morbidity Survey (NHMS) 2019 reported that the percentage of children underweight, stunted, and wasted in Malaysia was 14.1%, 21.8%, and 9.4%, respectively. Children from a household income of less than RM1000 and rural areas in Malaysia had much higher rates of stunting, wasting, and underweight than the household earning average (Institute for Public Health, National Institutes of Health, Malaysia Ministry of Health, 2016; Institute for Public Health (IPH), National Institutes of Health, Ministry of Health Malaysia, 2019). Other factors such as age, low birth weight, and unemployed mothers were also found to be associated with malnutrition in children (Baharudin et al., 2019; Cheah et al., 2012; Khambalia et al., 2012)
Approximately 45% of deaths among children under 5 years of age were due to malnutrition, specifically undernutrition (World Health Organization, 2015). It was found that there was an immunological alteration associated with malnutrition in children, which may contribute to mortality (Bourke et al., 2016; Hickson & Julian, 2018; Rytter et al., 2014). Children who were reportedly malnourished were often prone to illnesses and diseases due to a low immune body system, leading to morbidity and mortality. Other than that, it was also found that they often had an increased susceptibility to an accumulation of fat in the central region of the body, low-fat oxidation, lower energy expenditure, insulin resistance, and a higher risk of non-communicable diseases in adulthood, such as diabetes, hypertension, and dyslipidemia with reduced working capacity (Martins et al., 2011; Wells et al., 2020). In a systematic review, the most consistent factors found to be associated with child malnutrition were maternal education, household income, maternal nutritional status, age of the child, availability of sanitation facility at home, size of family, birth order in the family, and child’s birth weight (Katoch, 2022)
The childhood phase is the most vulnerable period of human life. Children depend highly on others to get their basic needs, thus making them fragile and vulnerable (Bagattini, 2019). The first 1000 days of life are important for optimal growth, brain development, health, and behavioral development (Beluska-Turkan et al., 2019). Thus, changes in nutrition and environment in children under 2 years old will affect their adulthood, making it a most challenging phase and critical for preventing malnutrition. A suitable intervention requires a proper understanding of the magnitude and underlying causes of the problem across different contexts. To the best of the researcher’s knowledge, limited studies were conducted regarding the underlying factors of malnutrition, specifically in children under 2 years old in Terengganu. Terengganu was chosen for this study as it is one of the states in Malaysia with a high rate of stunting (26.1%) and wasting (14%), exceeding the national stunting (20.7%) and wasting rate (11.5%) (Institute for Public Health, National Institutes of Health, Malaysia Ministry of Health, 2016). Therefore, the present study examined factors associated with nutritional status (underweight, stunting, and wasting), excluding the direct factors such as illness among children under 2 years old. This study filled in the knowledge gaps regarding malnutrition and provided better insight into the proper prevention program in Terengganu that will eventually reduce the malnutrition rates in this state.
Materials and Methods
The following section describes the methodology described in the study, listing the selected design, the study’s participants, and how data was collected.
Study Setting and Design
A cross-sectional study assessed the factors associated with nutritional status in children under 2 years old. Two out of eight districts in Terengganu were randomly selected: Kuala Nerus and Kuala Terengganu, representing a sample population of Terengganu. Kuala Terengganu and Kuala Nerus are districts in Terengganu. Both districts are situated on the eastern side of Peninsular Malaysia, facing the South China Sea, and have over 250,000 residents, with the majority being Malay Muslims.
Participants and Sampling
The study involved 244 children below 2 years old and their mothers. The inclusion criteria were mothers who can read/write/understand the Malay language and children under 2 years old, including infants with no physical disabilities. Children who could not be measured because they were too ill or because of postoperative immobilization were excluded. The list of mothers with children under 2 years old was obtained from the district office. All the mothers who had children under 2 years old who fit the inclusion and exclusion criteria were approached during the home visit and were given consent forms to participate in the study. This purposive sampling was done until the sample size was achieved. The sample size was determined by applying a regression formula using G-power software with an additional 20% dropout rate. Then, a minimum sample size of 244 was required.
Data Collection and Tools
The independent variables in this study were sociodemographic factors, birth weight, and maternal knowledge, attitude, and practice (KAP) of child nutrition. The sociodemographic factors included were the age of the children, gender of the children, age of the mother, educational level of the mother, household income, number of children, race, and the first pregnancy. Maternal nutrition KAP was assessed using a structured KAP questionnaire adapted from the Food and Agriculture Organization of the United Nations (Food and Agriculture Organization (FAO), 2014). The KAP questionnaire was validated during the pilot test and is reliable with a KR-20 value and Cronbach alpha of .715, .613, and .823, respectively. The questions comprised the prevention of malnutrition, feeding practice in infants and young children, exclusive breastfeeding, water, sanitation, and hygiene. The knowledge and practice sections comprised multiple-choice answers. One mark was given for a correct answer, zero for a wrong answer, and do not know option. While the attitude section was based on the level of agreement ranging from “strongly agree” to “strongly disagree” with a five-point Likert scale: 5-scores were given for “strongly agree” and one score was given for “strongly disagree” in each positive statement whereas the reverse scoring was applied in each negative statement.
Weight was measured using a calibrated digital scale, SECA 374 (SECA, Germany). The weight-for-age Z-score (WAZ) was divided into three groups: severe underweight (less than − 3 Z-score), moderate underweight (−3 ≤ Z-score < −2), and normal (−1 ≤ Z-score ≤ +3). The weight-for-length Z-score (WLZ) was divided into three groups: severe wasting (less than −3 Z-score), moderate wasting (−3 ≤ Z-score < −2), and normal (−1 ≤ Z-score ≤ +3). Height or length was measured by the validated SECA 233 (SECA, Germany), which is the measuring rod that can be attached to the SECA 374. Measurement was taken two times on the same day, and the mean value was calculated. The height-for-age Z-score (HAZ) was divided into three groups: severe stunting (less than −3 Z-score), moderate stunting (−3 ≤ Z-score < −2), and normal (−1 ≤ Z-score ≤ +3). All were based on the WHO Growth Reference cut-off (WHO Multicentre Growth Reference Study Group, 2006).
Ethical clearance for this study has been obtained. The Head of the District in Kuala Nerus and Kuala Terengganu granted the permission to collect the data. All parents provided informed consent prior to study participation.
Data Analysis
Data was analyzed using SPSS software program version 26 (IBM SPSS Corp., Armonk, New York, USA). The sociodemographic data and the nutritional status of children were presented in frequency (%) for categorical variables and mean and standard deviation (SD) for numerical variables. Simple logistic regression was carried out to identify the potential significant related factors. Variables with a p-value of <.25 in univariable analysis were selected for multivariable analysis. The p-value of <.25 was chosen to retain an important confounding variable, resulting in slightly richer models. Next, Multiple logistic regression with the forward method was performed to identify the associated factors of the nutritional status. The final results were presented using crude and adjusted odds ratio (OR) and p-value. The study’s significance level (α) was set as less than .05.
Results
Sociodemographic Characteristics, Birth Weight, and Maternal KAP
The study enrolled 244 mother-children aged below 2 years old. The mean ± SD age for the children was 13.16 ± 5.99 months, with more than half (54.5%) of the children’s gender being boys (n = 133) and 45.5% of children (n = 111) being girls. Of these, 14.3% (n = 35) participants had low birth weight (LBW), below 2.5 kg. For mothers, the mean age was 32.07 ± 4.68 years old. Half of them had a tertiary level of education (55.3%, n = 135). All the participants were Malay, and most had lower household incomes (86.5%, n = 198). The majority of them had one to two children (54.1%, n = 132). The result of maternal knowledge and attitude on nutrition topics showed that almost two-thirds (76.2%, n = 186) of the mothers had a good knowledge of this topic, and 91.8% (n = 224) of the mothers had a good attitude. The summary of the sociodemographic factors, birth weight, and maternal KA is shown in Table 1.
Sociodemographic Characteristics, Birth Weight, and Maternal KAP (n = 244).

In Malaysia, household income is categorized into three main income classifications: Bottom 40% (B40), Middle 40% (M40), and Top 20% (T20).
For the practice section, only 216 participants aged 6 to 24 months old were included. Others were excluded as they were below 6 months of age.
Achieved minimum dietary diversity refers to the proportion of children aged 6 to 24 months old who received at least a food from five to eight food groups in the last 24 hr.
For the practice section in the KAP Questionnaire, only mothers with children aged 6 to 23 months were analyzed (n = 216). There were almost two-thirds (73.1%, n = 158) of the mothers currently breastfeeding their children after 6 months of age. 81.9% (n = 177) of the mothers met the minimum dietary diversity score, 63.4% (n = 137) met the minimum meal frequency, and 54.6% (n = 118) met the minimum adequate diet. Following WHO/UNICEF guidelines, a child was considered to have met minimum dietary diversity (MMD) if the children aged 6 to 23 months received at least five out of the eight food groups in the last 24 hr, as per Table 2. The consumption of food items in the last 24 hr was shown in Table 2 as well, where 95.8% (n = 207) of children took grains, roots, and tubers, 43.5% (n = 94) took legumes and nuts, 83.8% (n = 181) took dairy products, 86.1% (n = 186) took flesh food, 67.1% (n = 67.1) ate eggs, 92.1 (n = 199) took vitamin A rich fruits and vegetables, 75.9% (n = 164) took others fruits and vegetables and 73.1% (n = 158) were still given breast milk. Next, a child was considered to have met the minimum meal frequency (MMF) if, in the last 24 hr, he/she received the minimum frequency for appropriate complementary feeding (i.e., 6–8 months = two times; 9–11 months = three times, 12–23 months = more than or equal to three times; non-breastfed children = four times. Last but not least, a child was considered to have met the minimum acceptable diet (MAD) if he/she had met both MMD and MMF.
Consumption of Food Items in the Last 24 hr (for children aged 6–24 months) (n = 216).

Nutritional Status of Children Under 2 Years Old
Table 3 shows the nutritional status of the children below 2 years old in Terengganu. Overall, 15.6% (n = 38) of the children were moderately stunted, 3.7% (n = 9), 10.2% (n = 25), and 1.6% (n = 4) were severely stunted, moderately, and severely underweight, respectively. Meanwhile, 8.2% (n = 20) and 2.0% (n = 5) of the children were moderately and severely wasted, respectively.
Nutritional Status of the Children (n = 244).

HAZ = height-for-age.
WAZ = weight-for-age.
WHZ = weight-for-height/length.
Factors Associated With Being Underweight, Stunting, and Wasting
Table 4 shows the univariable analyses for three separate models. Simple logistic regression analysis of stunting showed that the significant associated factors were the age of the child (crude OR 1.09, 95% CI [1.03, 1.16], p = .003), low birth weight (crude OR 3.56, 95% CI [1.64, 7.69], p = .001), poor maternal knowledge (crude OR 2.75, 95% CI [1.39, 5.43], p = .004), and poor practice (MDD) (crude OR 2.64, 95% CI [1.23, 5.64], p = .012). Multiple logistic regression was carried out to determine the predictors of stunting in children below 2 years old. Table 5 showed that the age of the child (adj OR 1.11, 95% CI [1.04, 1.20], p = .003), low birth weight (adj OR 3.79, 95% CI [1.63, 8.79], p = .002), poor maternal Knowledge (adj OR 2.29, 95% CI [1.06, 4.99], p = .036) and poor practice (MDD) (adj OR 2.64, 95% CI [1.11, 6.29], p = .029) were significant predictors of stunting in children below 2 years old in Terengganu.
Univariable Analysis of the Association Between Sociodemographic Characteristics Knowledge, Attitude, and Practice With Stunting Among Mothers and Children Below 2 Years Old Dyads (n = 244).

Significance level for the inclusion in the next model p > 0.25.
Multivariable Analysis of the Association Between Sociodemographic Characteristics, Knowledge, Attitude, and Practice With Stunting Among Mothers and Children Below 2 Years Old Dyads (n = 244).
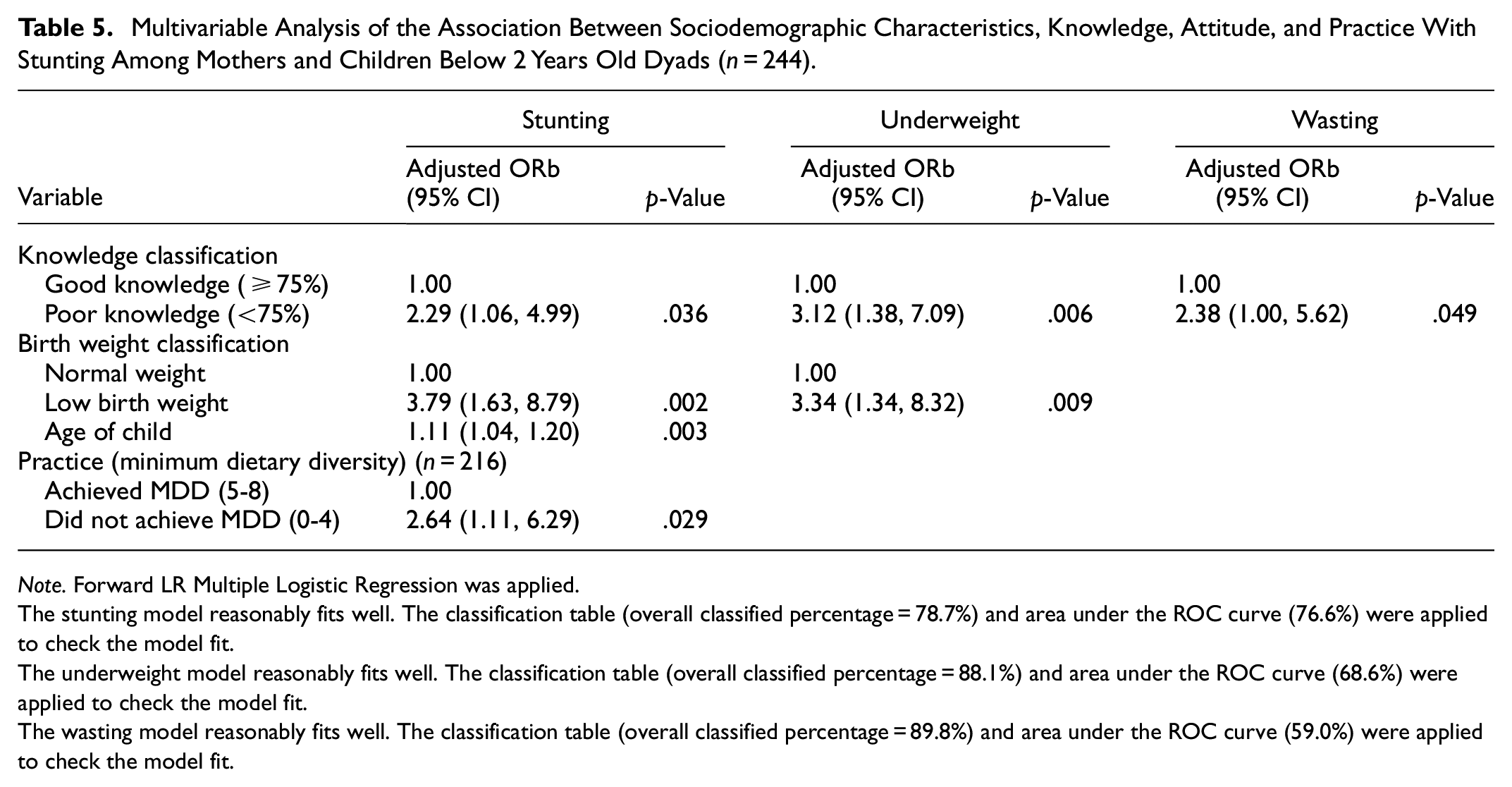
Note. Forward LR Multiple Logistic Regression was applied.
The stunting model reasonably fits well. The classification table (overall classified percentage = 78.7%) and area under the ROC curve (76.6%) were applied to check the model fit.
The underweight model reasonably fits well. The classification table (overall classified percentage = 88.1%) and area under the ROC curve (68.6%) were applied to check the model fit.
The wasting model reasonably fits well. The classification table (overall classified percentage = 89.8%) and area under the ROC curve (59.0%) were applied to check the model fit.
Simple logistic regression analysis of underweight showed that the significant associated factors were the age of the child (crude OR 1.09, 95% CI [1.01, 1.16], p = .022), low birth weight (crude OR 3.27, 95% CI [1.35, 7.94], p = .009), and poor maternal knowledge (crude OR 3.07, 95% CI [1.38, 6.85], p = .006). Multiple logistic regression was carried out to determine the predictors of underweight in children under 2 years old. Table 5 showed that low birth weight (adj OR 3.34, 95% CI [1.34, 8.32], p = .009) and poor maternal knowledge (adj OR 3.12, 95% CI [1.38, 7.09], p = .006) were significant predictors of underweight in children below 2 years old in Terengganu. For wasting, poor maternal knowledge was found to be a significant predictor of wasting even after controlling all the confounders in the multiple logistic regression (adj OR 2.38, 95% CI [1.00, 5.62], p = .049).
Discussion
The results of our study showed that poor maternal knowledge was a significant predictor of all the malnutrition markers, such as stunting, underweight, and wasting in children under 2 years old in Terengganu after controlling all the confounders. Children whose mothers have poor knowledge are 2.29, 3.12, and 2.38 times at higher odds of being stunted, underweight, and wasted, respectively. At the same time, low birth weight was a significant predictor of stunting and underweight, whereas the age of the children and not achieving MDD were significant predictors of stunting only. Children born with low birth weight had 3.79 and 3.34 times higher odds of being stunted and underweight, respectively. The results of the final model implied that children with lower birth weights, older age, failure to meet MDD requirements and have mothers with poor knowledge of nutrition are at a higher risk of experiencing stunted growth.
Nutritional Status of the Children
Stunting was the leading form of malnutrition in this community, affecting 19.3% of the children under 2 years old, followed by underweight (11.8%) and wasting (10.2%). The stunting rate observed was comparable with the national stunting rates (20.7%) and slightly lower than the state rates (26.1%) based on the national survey (Institute for Public Health, National Institutes of Health, Malaysia Ministry of Health, 2016). The percentages of underweight and wasting were also quite low and comparable to the national survey (13.7% and 11.5%), respectively (Ministry of Health Malaysia, 2016). Notwithstanding the difference in the prevalence rates between the current study and the national survey, the underweight, stunting, and wasting rates are still high, depicting the need for further investigations on the factors associated with it and how to overcome them for a better future. Other than that, the malnutrition rate in this study was lower than in other studies conducted at the local level, which was 29.8% underweight, 43.0% stunting, and 5.8% wasting in Sarawak and 69.0% stunting, 63.4% underweight, 40.0% wasting in Kelantan (Bong et al., 2018; Cheah et al., 2012). It could be because both studies were done in rural areas in Sarawak and Kelantan, which may have had a higher rate of malnutrition cases. The current study included all the areas, such as rural, semi-urban, and urban areas.
Maternal Characteristics Association With Nutritional Status
It was postulated that maternal knowledge is a key driving factor for good practice, which leads to the healthy growth of children. Thus, it is recommended that the mother attend nutrition classes and regular counseling during pregnancy for early nutrition education and guidance. As shown in the current study, this activity is important, whereby maternal knowledge was found to be associated with all the nutritional status markers. The result is similar to studies in Egypt, Iran, and India (Jain et al., 2018; Manzour et al., 2019; Mohamed Ahmed Ayed et al., 2021; Yeganeh et al., 2018). Poor maternal knowledge was a significant predictor of nutritional status, considering the mother plays the main role in providing nutrition for children. Mothers provide the sole nutrition for the developing infants during pregnancy and in the first 6 months of life when exclusive breastfeeding is required (Marangoni et al., 2016). Mothers are also responsible for designing the child’s food intake through their dietary intake, meal planning, food availability, and food preparation at home (Kueppers et al., 2018; Saleh et al., 2021).
Most of the mothers in the current study were in their thirties and had a secondary and tertiary level of education. There was no association between the mother’s age and formal education with nutritional status. It was similar to the local studies conducted in Terengganu that found that most mothers aged 30 years and above with secondary and tertiary education levels had no association with stunting (Khor et al., 2016; Saleh et al., 2021). However, a similar study found that a high proportion of stunted children have a mother with a low education level, even though it was insignificant (Saleh et al., 2021). Furthermore, because the study was conducted not only in the rural area but also in other areas, including urban areas, formal education might have less influence on health, nutrition, and sanitation choices than it would have in a rural setting, where access to information is more complex (Syeda et al., 2021).
In practice, more than half of the mothers still breastfeed their children. It is similar to the study conducted in Malaysia in which the percentage of mothers who still breastfed their children after 6 months was 57.1% (Khor et al., 2016). Compared to the National Health and Morbidity Survey (NHMS) in 2016, the percentage of mothers who reported still breastfeeding their children at 2 years of age was 39.4%, with Terengganu being the third highest, which was 45.6% (Institute for Public Health, National Institutes of Health, Malaysia Ministry of Health, 2016). However, the current study could not find the association of breastfeeding with any nutritional status marker. The result was supported by the study conducted in Pakistan (Syeda et al., 2021). It could be due to the fact that weight changes in children below 3 years old were greatly influenced by other behaviors and environmental effects (Syeda et al., 2021). Other than that, the association between breastfeeding duration and nutritional status still needed to be clarified and had conflicting results, which required further investigation. Other Infant and Young Child Feeding Practice (IYCF) indicators were Minimum Acceptable Diet (MAD), Minimum Dietary Diversity score (MDD), and Minimum Meal Frequency (MFF).
Poor MDD score was associated with stunting in the current study. It was supported by the systematic review study, which found a possible association between low MDD in infants and children below 5 years concerning stunting (Molani Gol et al., 2022). Another study by Jones et al. also stated that MAD was associated with stunting but was largely driven by MDD (Jones et al., 2014). Providing enough macronutrients and micronutrients is important for the proper growth of children. For example, animal food sources were an effective strategy to reduce stunting and underweight in children (Adesogan et al., 2020; Ihab et al., 2014). It can be due to their socio-economic status since most of them belonged to the B40 household income, which limits access to various diets, thus making them lack the nutrition for healthy growth (Ali Naser et al., 2014). The systematic review found that taking enough protein and increasing micronutrient intake are most efficient for child growth, thus achieving MDD during infancy. It includes more nutrient-dense foods that may prevent malnutrition and improve health and nutrition status (Roberts & Stein, 2017). However, the result contradicted the Sarawak study, which found no significant association between the IYCF indicators of MDD, MMF, and MAD and underweight, stunting, and wasting (Bong et al., 2018). In this study, the scores of IYCF were 55.3% (MAD), 76.6% (MDD), and 83% (MMF). It is much lower compared to the current study. A better score in these IYCF indicators in the current study can be because these mothers are more socially and economically empowered in deciding for their children.
Child Characteristics With Nutritional Status
Next, the multiple logistic regression showed that children born with low birth weight had higher odds of being stunted and underweight. Similar findings were found in a systematic review study by Cheah et al. (2012), Katoch (2022), Omondi and Kirabira (2016), and Zoleko-Manego et al. (2021). Children born with low birth weight (LBW) tend to have greater morbidity due to poor physical growth and development (Shamme et al., 2017). They would be malnourished once born as low birth weight, and the result was not modified by other confounding issues (Shamme et al., 2017). Low birth weight in children could originally occur during the fetal period. Thus, the mother’s nutritional status during the pregnancy could lead to a low-birth-weight child. Several studies found that undernutrition in pregnant women was linked to intrauterine growth retardation and micronutrient deficiency, which results in low birth weight in infants (Katoch, 2022; Utami et al., 2018). Other than that, low birth weight led to a child underweight and stunting, which could be possibly be described by the increased chance of an LBW child more prone to infections such as diarrhea, respiratory infections, jaundice and loss of appetite compared to a normal birth weight children (Abbas et al., 2021; Pabbati et al., 2019; Rahman et al., 2016). Thus, greater morbidity in an LBW child leads to poor physical growth and development, which is perceived as malnutrition (Rahman et al., 2016). In addition, 14.3% of the children in the current study had low birth weight, which was above the national prevalence rate of low birth weight children (9.7%) (Institute for Public Health, National Institutes of Health, Malaysia Ministry of Health, 2016). Almost half of the current study’s LBW children (40%) were stunted. Therefore, special attention is required to reduce the prevalence of LBW in children to reduce the stunting rate in the future.
A child’s age was found to be a significant predictor of stunting. The result is similar to the studies in Malaysia, Pakistan, and Rwanda (Cheah et al., 2012; Nshimyiryo et al., 2019; Tariq et al., 2018). Age also was found to be associated with stunting, with the odds of children aged 12 to 23 months indicating that they are highly likely to be stunted compared to children of age 0 to 5 months in Punjab (OR = 1.69, 95% CI [1.49, 1.91]) and rural Punjab (OR = 1.67, 95% CI [1.46, 1.93]) (Haq & Abbas, 2022). Another study also found that 12 to 23 months-old children were about four-folds (aOR 3.98; 95% CI [2.45, 6.46]) more likely to be stunted compared to infants aged 0 to 11 months, while 24 to 59 months children were about 4.5-folds (aOR 4.42; 95% CI [2.36, 8.28]) more likely to be stunted than infants (Vonaesch et al., 2017). It is important to ensure the proper height growth of children during infancy because it can predict their height during the age of two (Schwinger et al., 2017). It also can be because, with increasing age, the exposure of a child to poor quality and unhygienic food and water, sanitation, and hygiene (WASH) conditions increases and thus retard the linear growth of a child (Titaley et al., 2019). Other than that, it is highly explained by the effect of feeding transition from exclusively breastfeeding to breastfeeding until 24 months and to complementary feeding. Any disruption in this process, such as poor or limited choices of food and dietary diversity, might cause stunting in children at an older age (Wali et al., 2020).
However, the gender of the child was found not to be associated with nutritional status in the current study. It contradicts the study on children below 2 years old in Bangladesh and Pakistan (Chowdhury et al., 2020; Haq & Abbas, 2022). It might be explained by the fact that discrimination between genders in the allocation of food and healthcare within the household is rare in the current study compared to other countries. It was supported by the local study conducted in Kelantan and Terengganu, which found no association between gender and malnutrition in children (Cheah et al., 2012; Wong et al., 2014). One cross-country econometric analysis using data from 116 developing countries collected between 1970 and 2012 also found that gender equality was one of the key drivers of past reductions in stunting (Smith & Haddad, 2015).
Strengths and Limitations
To the best of the authors’ knowledge, this is the first study to explore factors associated with malnutrition in children under 2 years old in Terengganu. Other studies prioritized much older children, such as preschoolers (Bahtiar et al., 2021; Wong et al., 2014) and the Aborigine people (Bong et al., 2018). Thus, new insight from this study would fill the gaps in nutritional research. Other than that, the study’s external validity has been validated since the participants from Kuala Terengganu and Kuala Nerus were randomly selected from eight districts in Terengganu, and all the mothers who agreed to participate were included in the study. However, the study had a few limitations, such as mothers might have the Hawthorne effect. The mother might have guessed the answers in the knowledge questions since it was in the multiple-choice questions due to the chance of being observed, and it was also a self-administered questionnaire. Other than that, it was a cross-sectional study; hence, we cannot interpret our results as causality. Next, the study is provincially representative, but the results are not generalizable nationally. Finally, the results of this study may be underestimated or overestimated because they have not been controlled by the direct factor variables that affect malnutrition, namely food intake and diseases or illnesses suffered by the children.
Conclusion
In this study, the data analysis suggested that the odds of stunting are higher in children having a low birth weight, older age, those who have not achieved minimum dietary diversity, and children whose mothers have poor nutritional knowledge. In comparison, the odds of being underweight are higher in children with low birth weight and children whose mothers had poor nutritional knowledge. Next, the odds of wasting are higher in children whose mothers have poor nutrition knowledge. Poor maternal knowledge was associated with all the malnutrition markers, making it crucial information, especially for policymakers. Thus, it is recommended to provide a targeted nutrition intervention for children with LBW, low MDD, and mothers with poor nutrition knowledge. Other than that, nutrition counseling should be provided by nutritionists or dietitians to all mothers during pregnancy up until their children reach 2 years of age to increase their nutrition knowledge and, at the same time, to reduce the chance of having a low-birth-weight child. The government should also implement initiatives to help families with low household income by providing free health nutrition counselors visit at home and subsidies for food to ensure food diversity. It is to ensure that malnutrition rates are reduced significantly and effectively.
Footnotes
Acknowledgements
We would like to express our gratitude to all those who helped through the data collection process and the mothers and children who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance for this study was obtained from the UniSZA Human Research Ethics Committee (UHREC) (UniSZA/UHREC/2022/391). Permission to collect the data was granted by the Head of the District in Kuala Nerus and Kuala Terengganu. All parents provided informed consent prior to study participation.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.