
Abstract
Stunting is an important issue as it leads to many adverse consequences on children’s health. Pakistan is in public health crisis due to higher stunting rates in children. World Health Organization entails the prevalence of stunting to be less than 2.5% in a healthy population, but every third child is stunted in Punjab (largest province of Pakistan by area and population). By using the Multiple Indicator Cluster Survey (MICS) Punjab, 2018 and employing multilevel logistic regression analyses, this study finds that children whose mothers are educated and have better access to drinking water and antenatal care have lower odds of stunting. Access to better and accessible health care, education especially of girls/women, and clean water can reduce stunting in children. The government needs to give special attention to these factors to help children grow healthy.
Keywords
Introduction
World Health Organization’s (WHO, 2014b) Health Assembly in 2012, set the target of reducing the stunting prevalence, in children less than 5 years of age, from 167 million in the year 2012 to 100 million in 2025; a 40% reduction in almost a decade and a half. Stunting (deficit in height-for-age of a child) is declining worldwide, although the progress is very slow. Across the globe, about 149 million (21.9% globally) children under 5 years of age were stunted in the year 2018 (United Nations Children’s Fund [UNICEF], 2019). For better monitoring of child growth, stunting is a crucial indicator. Childhood Stunting indicates chronic under-nutrition and reflects the consequential cumulative effects of recurrent infections especially in the first 1,000 days (start of conception to first 2 years after birth) of a child’s life (Black et al., 2008)
Although the world looks off track to achieve the reduction of stunting (40% reduction) goal and hence need concerted and scaling up of efforts at national and sub-national levels. Furthermore, half (50%) of the children’s deaths are attributed to undernutrition globally (Black et al., 2013). Stunting results from nutritional deprivation, poor environmental and socio-economic conditions, and inadequate childcare conditions. Of note, stunted children start their life as deprived children and continue to have impacts throughout their lives in terms of lack of cognitive development, deteriorating performance at school, productivity gap from normal children, and facing difficulty in community participation (Black et al., 2013; de Onis & Branca, 2016; Stewart et al., 2013; UNICEF, 2019; WHO, 2014a). A study using data from Kingston Jamaica estimated that the prevalence of stunting in children before the age of 2 years restricts their cognitive development and educational achievement in adolescence (Black et al., 2013; Walker et al., 2007). Furthermore, longitudinal studies, estimated that stunted children in Brazil, India, Guatemala, the Philippines, and South Africa, are having reduced schooling attainment (Adair et al., 2013; Martorell et al., 2010).
The overwhelming majority of undernourished children reside in Sub Saharan Africa and South Asia (33.1% and 33.4%, respectively, in the year 2018) which is very high (de Onis et al., 2019; UNICEF, 2019; UNICEF-WHO-The World Bank, 2019). Pakistan is one of the South Asian countries facing an acute problem of childhood stunting. According to the National Nutrition Survey (NNS) of Pakistan, there is an increase in stunting prevalence in Pakistan from 31% in 2001 to 40.2% in 2018 (UNICEF Pakistan, 2018). Nevertheless, the recent Pakistan Demographic and Health Survey 2017 to 2018 put the stunting prevalence a bit lower at 38.6% still very high according to cutoff points set by WHO (2014b) of stunting prevalence of approximately 2.5% in the healthy population. Although, an agricultural country, Pakistan is under serious category level on Global Hunger Index and stands at 94 numbers out of 117 countries (Von Grebmer et al., 2019).
Stunting seriously undermines the development potential of Pakistan, as an anthropometric disadvantage. A loss of 1% height of a child due to stunting is associated with a 1.4% loss in productivity estimated by a World Bank study. Food and Agriculture Organization (2017) of the United Nation estimated a reduction in Pakistan’s Gross Domestic Product (GDP) by up to 3% to 4% due to undernutrition. In addition to economic and political impediments, Pakistan is facing a silent crisis of childhood stunting. Being the worst in South Asia, the reduction in stunting over the last four decades has been modest (44% in 2013 vs. 38.6% in 2018) which itself is an alarming situation (WHO, 2014b).
Punjab, the largest province by population (56% of the total national population according to census 2017) of Pakistan and having a GDP share of about 57.6%, has a stunting prevalence of under-5 children 31.5% in the year 2018 (Bureau of Statistics Punjab; Government of the Punjab, 2018). In Pakistan, after the devolution of power through the 18th constitutional amendment, provinces are now responsible for their financial resource allocation, policymaking, and its implementation (United Nations, 2016), to achieve the Sustainable Development Goal of zero hunger and poverty and to achieve the Global Nutrition Targets, 2025 set by WHO (2014b). Punjab, having the largest share of the population of the country, needs special attention especially in the (significant) reduction of stunting prevalence which will help bring the prevalence of stunting down not only in the province but also in Pakistan.
Several empirical studies have investigated the factors associated with stunting in sub-provincial and/or districts, city, or rural-urban area level (Arif et al., 2012, 2014; Ibrahim, 1999; Iram & Butt, 2006; Mushtaq et al., 2011; Nuruddin & Hadden, 2015) but the paucity of studies is present; which empirically examine the correlates of stunting using large and provincially representative data set in Pakistan. All of these studies used either Ordinary least square or logistic regression models to estimate the factors associated with the undernutrition of under-5 children (Asim & Nawaz, 2018) which is empirically challenging if the data structure is hierarchical in nature. In these empirical studies child sex, family size, income/wealth status of the household, breastfeeding, and child age are important predictors of childhood undernutrition. According to a number of studies (Asim & Nawaz, 2018; Khan et al., 2019; Titaley et al., 2019), the age of a child is an important indicator of childhood stunting and its prevalence. Furthermore, the low height-for-age of children in the age group of 2 to 3 years shows the continuous phenomenon of failing to grow (stunting) and for older children shows having failed to grow (stunted; de Onis & Monika, 1997). According to various data sources, like Pakistan Demographic Health Survey (PDHS), MICS Punjab, and Sindh, undernutrition prevalence in Pakistan especially stunting is increasing with the increase in age of the child. Furthermore, in settings of low socio-economic status and augmented risk of frequent exposure to hostile conditions such as lack of water and sanitation and illness, the prevalence of stunting rises with the age especially at the age of 3 months and above.
The aim of this study is to identify different demographic, socioeconomic, and health-related factors on stunting in their first 2 years of age at individual and household level in Punjab. Additionally, authors tend to investigate the effect of different factors in rural and urban Punjab.
Methodology
Data Source and Study Design
The study conducts analysis based on the provincially representative data of the Multiple Indicator Cluster Survey (MICS-2018), Punjab conducted by Punjab Bureau of Statistics in collaboration with the United Nations Children’s Fund (UNICEF), as part of the Global MICS Program. MICS data has covered a variety of dimensions pertaining to a wide range of indicators on the situation of children and women residing in rural and urban areas of the province. MICS data covers all 9 administrative divisions and 36 districts (Sub-Division) of Punjab province of Pakistan. The MICS Punjab, 2017 to 2018 data was collected during December 2017 and March 2018. A multi-stage, stratified cluster sampling, using strata of the region (urban/rural) and districts used for the selection of the survey respondents. The sampling frame is based on the 2017 Country Census of Population and Housing. The primary sampling units (PSUs) selected at the first stage were the enumeration areas (EAs) defined for the census enumeration and were selected using probability proportional to the size. From each EA 20 households were selected. The entire households (secondary sampling units, SSUs) was drawn from 2,692 Primary Sampling Units (PSUs), of which 1,893 were from rural Punjab and 799 were urban. The total sample size was 53,840 households (secondary sampling units). The MICS 2018 Punjab data has a women/caretaker response rate of 93.1% and children of less than 5 years response rate of 93.8%. For further details of MICS Punjab 2018 are provided elsewhere (Bureau of Statistics Punjab; Government of the Punjab, 2018). The focus of this study is on children less than 2 years of age hence the number of respondents in our sample is 10,080 (total number of children of <5 years in the survey: 39,799) children for which we have all the data is available excluding missing observations.
Variables
Outcome Variable
This study used data from Punjab Multiple Indicators Survey 2017 to 2018 that provides data for children for their weights (kg) and heights (cm) across the Punjab province. In this study, we are using children of less than 2 years (0–23 months) to empirically examine the prevalence and factors associated with childhood stunting. Stunting is calculated using WHO child growth study cut-off points and a child is categorized as stunted if his/her height-for-age Z score is less than −2SD (World Health Organization; United Nations Children Fund, 2009). Our outcome variable stunting (lower height for age of child <2 years age) is dichotomous and takes the value of 1 if a child is stunted and otherwise 0.
Potential Predictors
This study follows the UNICEF (2013) framework for analyzing the factors associated with childhood stunting. There are four levels of predictors: Child, Parental, Household, and Regional level. Child level characteristics include age, sex, child size at birth, and vitamin and zinc intake of child. Parental level factors include mother and father’s education, mother currently breastfeeding, place of delivery, antenatal care (ANC) received, and ANC visits. Household and regional characteristics include the region of residence, wealth index, animal ownership, source of drinking water, treatment of drinking water, and sanitation.
The construction of each variable is provided here. The child level factors include the age of the child categorized into; 0 to 5, 6 to 11, and 12 to 23 months. The gender of a child is a binary variable containing two categories namely boy and girl. Child size at birth is categorized into large (combining larger than average and very large child size), average child size, and small (combining very smaller and smaller than the average size). Whether a child drinks or eat vitamin or mineral supplements or any medicines yesterday, during day or night is categorized codeas yes andno. The same categorization is used for zinc intake. The place of delivery of a child is categorized into home and hospital. . Parental factors include mothers’ and fathers’ education level that is categorized into no education, primary (1–5 years of schooling completed), middle (6–8 years of schooling completed), secondary (9–10 years of schooling completed), and higher (10 and above years of schooling completed).
Mother currently breastfeeding a child is a binary variablehaving categories of yes and no. The antenatal care (ANC) of a mother is measured through two variables first is whether a mother received ANC or not and second if the mother received ANCeit is categorized into two categories: mother received up to four ANC visits and more than four ANC visits. Household and regional level characteristics include a region of residencenamely urban and rural. The wealth index quintile of the household is categorized into five categories: poor, poorest, middle, rich, and richest. If the households own any animal, then it is coded as yes and no otherwise. Drinking water used by households if improved is coded as 1 and 0 as unimproved. Improved water sources include piped water, piped into dwelling, compound/yard/plot/neighbor, public tap or standpipe, tube well/borehole, motorized pump, hand pump (mechanical), protected spring water collection, and protected dug well. Unimproved sources of water include unprotected dug well, unprotected spring water collection, tanker truck, the cart with small tank/drum/cane, bottled water, surface water (river, dam, lake, pond, stream, canal, and irrigation channel), and any other. The variable of drinking water is binary variables with two categories of improved and unimproved. . The type of sanitation facility used by households has two categories of improved and unimproved. However, improved sanitation facility includes flush/pour flush to piped sewer system/septic tank/pit latrine, pit latrine with slab, and ventilated pit latrine. Unimproved sanitation facility includes flush/pour flush to open drain or elsewhere, pit latrine without slab/open pit, having no facility/bush/field, and any other. The definitions of improved and unimproved water and sanitation are according to WHO (2019) guidelines.
Data Analyses
Descriptive data analyses involved three steps; first, we describe the frequency and %age of socio-demographic variables. Second, we describe the childhood stunting of under 2 years old children using socio-demographic and other predictors of childhood stunting. Third, we have measured the association of each predictor with that of stunting (our outcome variable) using chi-square (p < 0.05). All the descriptive statistics are weighted to make them representative at the provincial level. Besides, descriptive analysis, our study used multilevel logistic regression analysis because of the hierarchical nature of data. MICS, Punjab is a clustered and hierarchical data where observations in the same group are related to each other, for example, the height of children within families. Data may contain different levels (hierarchies) where finding variations at each level may give exciting results at a disaggregated level for better policy and interventions (Raudenbush & Bryk, 2002). We have an estimated two-level hierarchical model (level 1: children, level 2: households) using fixed and random effects where the random effect is measured by its variance (Allison et al., 2015; Gelman & Hill, 2007, p. 247).
In this paper using multilevel logistic analyses, we have estimated four models where Model 1 is an empty (Null model) that includes only intercept term which gives the mean of stunting of children less than 2 years of age and its variation at the household level. Model 2 includes all the child, parental, household, and regional factors associated with stunting prevalence at the provincial level. Model 3 and Model 4 are estimated at urban and rural Punjab levels respectively. Finally, the variance partition coefficient (VPC) is estimated using variance from Model 1 to 4. The results of multilevel logistic regression are presented as odds ratios with their 95% confidence intervals (95% CI). The statistical analyses are carried out in this study with the help of STATA 15 software (STATA Corp, College Station, TX, USA).
Ethical Statement
The Multiple Indicators Survey (MICS) Punjab 2017 to 2018 data is publicly available, and the data is de-identified. The access to MICS Punjab data was granted for legitimate research after registering at the MICS data official website (http://mics.unicef.org/surveys). Informed consent was taken from all the respondents in the MICS, Punjab 2017 to 2018. Hence for the use of MICS data, no ethical clearance is required.
Results
Bivariate Descriptive Analysis
We have a total respondentsof 10,080 children under 2 years of age and around 30% of children (2995) are stunted. Table 1 presents the demographic and socioeconomic characteristics of the respondentsat the child, parental, household, and regional levels. The p-value of chi-square of each variable with the childhood stunting has also been presented. It also presents the prevalence of stunting in each category through frequency distribution. The sample for this analysis is based on children less than 2 years of age (0–23 months) of which about 52% are boys and 48% are girls. Almost one-third (32%) of boys and around more than one-fourth (27%), girls are stunted. Around half of the children (51%) of the children belong to the age group 12 to 23 months. The prevalence of stunting in each age group of 0 to 5, 6 to 11, and 12 to 23 months is 25%, 24.7%, and 34% respectively. The overwhelming majority of children (about 41.5%) having smaller than the average size at birth are stunted compared to about 22% of children having large size and 27% of children having an average size at birth. One-fourth (25%) of children who took vitamins and 28% of children who took zinc are stunted. Almost 35% of children are currently breastfed and of those 70% are stunted. Of 91% of women who received prenatal care, about 28% of their children were stunted. In thisstudy, 44% of women have no education have 40% of the stunted children whereas women having primary education have about 29% of the stunted children under 2 years of age. Around 39% of children delivered at home are stunted. Besides, about 50% of children belong to poor households. Of them, three fourth (75%) are stunted. In richer households, about 32% (almost one-third) of children are stunted. Similarly, 24% of children residing in urban areas are stunted compared to 32% in rural areas. Households having unimproved drinking water available at home, water not treated for making it safe for drinking, and having unimproved sanitation facility at home having respectively 24%, 30%, and 41% prevalence of stunting of less than 2 years old children (see Table 1 for details).
Descriptive Statistics of Socio-Economic and Demographic Characteristics Punjab (MICS 2017–18).

Note. The values in brackets are the p-value of chi-square test between the dependent (stunting) and the independent variables.
Multivariate Analysis
Multilevellogistic regression analysis results are presented in Table 2. The results show that compared to boys, girl child has significantly lower odds (OR = 0.72, 95% CI [0.66, 0.79]) of stunting. Similar trend follows in urban (OR = 0.82, 95% CI [0.66, 1.02]) and rural (OR = 0.69, 95% CI [0.62, 0.77]) areas as well. The prevalence of stunting is significantly higher around more than three times (OR = 3.28, 95% CI [2.66, 4.05]) in children having a small size at birth compared to children having a large size at birth for the whole province. Whereas, around two (OR = 2.11, 95% CI [1.27, 3.52]) times for urban areas and more than three and half times (OR = 3.69, 95% CI [2.90, 4.69]) for the rural area of Punjab. Children not taking vitamins, a day before the survey (yesterday), are significantly more likely to be stunted (OR = 1.16, 95% CI [1.03, 1.29]) for the Punjab respondentsand rural area (OR = 1.28, 95% CI [1.13, 1.46]) whereas insignificant for urban areas. The survey used a question to gather data about the vitamin intake of a child where the child was asked whether he has taken a vitamin a day before (Yes/No). The face value of the question suggests that a vitamin taken yesterday cannot have long-term impacts (such as stunting). The vitamin, taken by a child a day before the survey indicates two options which are: first, the child takes vitamins usually/regularly and has also taken a day before the data was collected, second, the child happened to take a vitamin supplement a day before the data collection. The probability of the latter event is very less. The vitamin taken a day before indicates that a conscious effort has been made to provide vitamins to the child and recurrence of that conscious effort is very probable.
Multivariate Logistic Regression Model of Factors Associated With Childhood Stunting (MICS 2017–18).
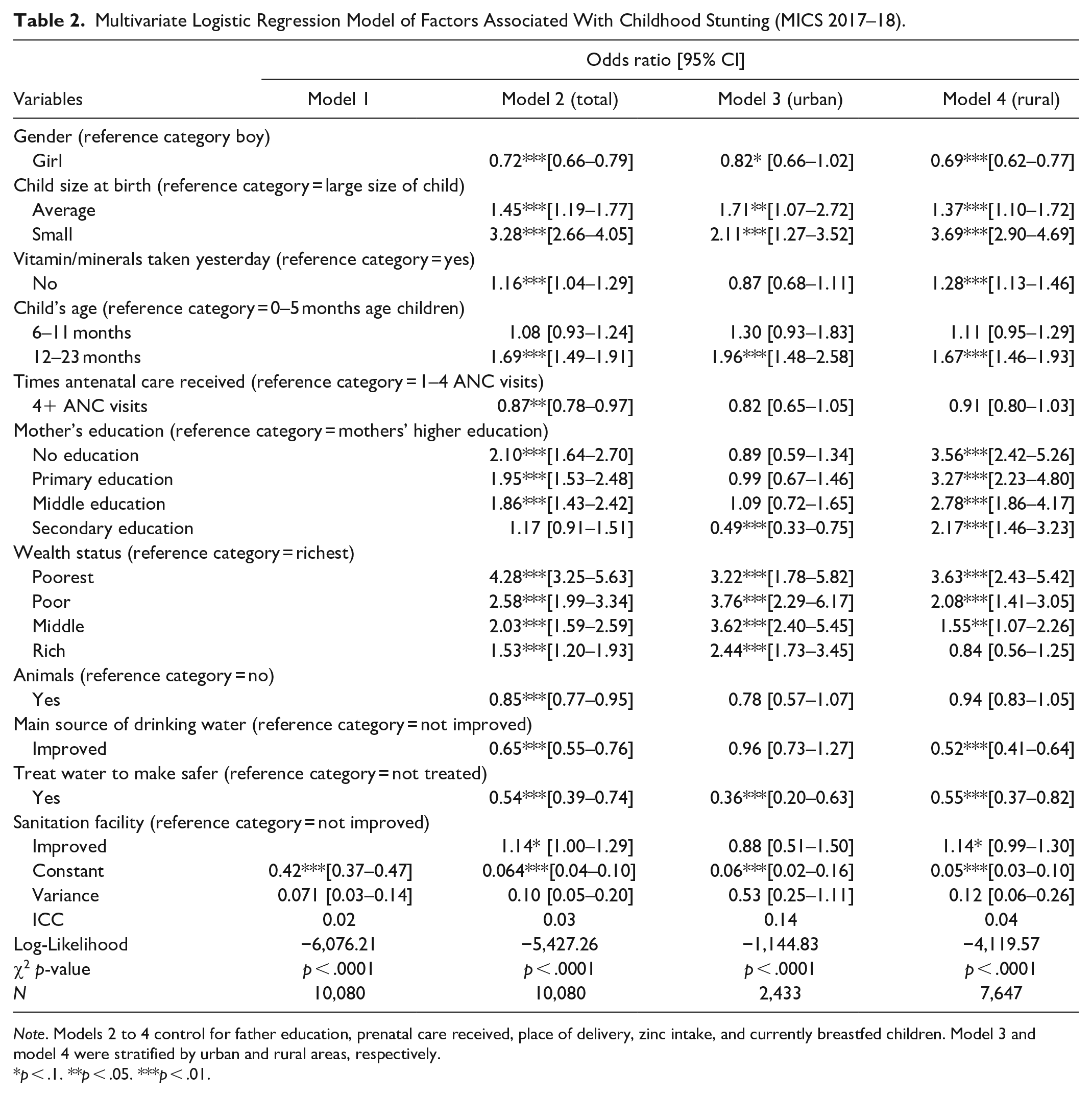
Note. Models 2 to 4 control for father education, prenatal care received, place of delivery, zinc intake, and currently breastfed children. Model 3 and model 4 were stratified by urban and rural areas, respectively.
p < .1. **p < .05. ***p < .01.
Odds of children of age 12 to 23 months indicate that they are highly likely to be stunted compared to children of age 0 to 5 months in the Punjab (OR = 1.69, 95% CI [1.49, 1.91]) and rural Punjab (OR = 1.67, 95% CI [1.46, 1.93]). Nevertheless, children of urban Punjab are twice (OR = 1.96, 95% CI [1.48, 2.58]) more likely to be stunted.
Furthermore, children of women receiving more than four antenatal care visits during pregnancy have lower odds (OR = 0.87, 95% CI [0.78, 0.97]) of their children being stunted compared to those mothers who received less than four ANC visits. Furthermore, children born to the poorest household are experiencing four times more odds of stunting (OR = 4.28, 95% CI [3.25, 5.63]) compared to children born to the richest household. The odds of a child being stunted born to a poor family is around more than two and a half (OR = 2.58, 95% CI [1.99, 3.43]) and born to a middle-income household are twice (OR = 2.03, 95% CI [1.59, 2.59]) likely to be stunted. Moreover, a child born to a rich household is one and half times more likely to be stunted (OR = 1.53, 95% CI [1.20, 1.93]) compared to the child born to the richest household. A similar pattern of odds of children being stunted is observed in rural and urban areas of Punjab according to wealth quintile. The odds of children born to mothers with primary education (OR = 1.95, 95% CI [1.53, 2.48]) and middle education (OR = 1.86, 95% CI [1.43, 2.42]) are almost twice compared to mothers who attained higher education in the entirePunjabrespondents. The odds of children being stunted of women having secondary education are not significantly different from those having higher education. In urban Punjab, surprisingly, only the odds of children being stunted to mothers having secondary education are statistically significantlylower (OR = 0.49, 95% CI [0.33, 0.75]) compared to women with higher education.
Children of households owning animals (especially milking animals) are significantly less likely to be stunted (OR = 0.85, 95% CI [0.77, 0.95]) for the entire respondents. Similarly, children belonging to households having improved sources of drinking water are 35% less likely to be stunted compared to households having unimproved sources of drinking water. In rural areas, households having improved sources of drinking water have significantly lower odds of their children being stunted (OR = 0.52, 95% CI [0.41, 0.64]). A household using water treatment for making it safe to drink is significantly less likely to experience childhood stunting (OR = 0.54, 95% CI [0.39, 0.74]). Moreover, the association between sanitation and stunting was only significant at a 10% level of significance for overall Punjab and rural Punjab. It was insignificant for urban Punjab. A multilevel analysis suggests that the stunting of children under 2 years of age varies 3% at the household level. Table 2 shows the intraclass correlation (ICC) which indicates the similarity of responses of households within the same cluster. The correlation in responses between two children belonging to the same household is 14% in urban areas and 4% in rural areas. ICC is calculated based on residuals and reports the amount of variation unexplained by any predictor in the model.
Discussion
This study empirically examined the household level Multiple Indicators Cluster Survey (MICS-2018) data for Punjab province of Pakistan for children under 2 years of age. The analyses confirm that the issue of stunting is multidimensional and thus tries to explore various factors affecting stunting prevalence using multilevel (hierarchical) logistic regression analyses. The prevalence (weighted) of child stunting, for children less than 2 years of age, in Punjab is about 30%. Stunting is a major problem prevailing in low-income countries in general and in Pakistan in particular (Black et al., 2013; Lobstein et al., 2015).
The gender of a child is a strong predictor of childhood stunting in Punjab. According to our analyses, the prevalence of stunting and odds of being stunted are higher for boys compared to girls in Punjab, Pakistan. This may be due to the reason that a male child needs relatively more calories to grow and develop in the early years of life especially in the first years (Kavosi et al., 2014). Nevertheless, a study from rural Pakistan (Shah et al., 2003) reported a non-significant gender effect on stunting prevalence. Furthermore, the gender of the child and its relationship with undernutrition (stunting) is inconsistently reported in the literature, for example, a meta-analysis from 16 demographic and health surveys of Sub-Saharan Africa (SSA) reported that in 10 out of 16 countries male children were more likely stunted. Of note, a study using data from India pointed toward the intersectionality of the gender of a child with wealthy status, religion, and caste identities and found sex differences do exist in upper-caste Hindus (Mukhopadhyay, 2016). The issue of the gender of a child is important in the case of Pakistan, where, it is normally believed, due to traditional patriarchal norms and value system the girl child is at more disadvantage which is in contrast with the results of our study and other studies from Pakistan (Kavosi et al., 2014). The findings of association of gender with stunting are in agreement with current studies for Asia and other countries (Khara et al., 2018; Song et al., 2019). Furthermore, this finding is in line with a study that used the Pakistan demographic and Health Survey Data (PDHS 2012–2013) and reported higher odds of a male child being stunted (Khan et al., 2019; Mahmood & Nasir, 2001). However, an in-depth analysis is called for child gender and its association with undernutrition.
The size of a child at the time of birth is an important predictor of childhood stunting prevalence. In our study, the size of a child at birth is also a significant predictor of stunting. Compared to the large size of a child at birth, children with small size at birth have significantly higher odds of stunting (three times higher for the entire respondents, around more than three and half times for rural, and two times for urban). The association between childbirth weight (less than 2500 grams) is explained with the vulnerability of a child, having a small birth size, to illnesses like diarrhea, anemia (Haque et al., 2015; Khanal et al., 2014). These findings are consistent with previous studies (Mistry et al., 2019).
Similarly, vitamin intake was found to have a significant effect on childhood stunting in Punjab. In our estimations, children not taking vitamins have significantly higher odds of stunting. It is pointed in previous studies, that vitamin intake increases the height of children and reduces their chances of stunting. Any community intervention to improve the nutrient value in children helps them to improve their immunity and fight infections (Bhutta et al., 2008, 2013; Vaivada et al., 2017). The findings of a study (Tariq et al., 2018) from Pakistan using Pakistan Demographic and Health Survey (2012–2013) data is in contrast with our finding as they find no signficant relation of micronutrient deficiency in children and stunting. It is worth mentioning here that vitamin deficiency is different from micronutrient deficiency as micronutrient deficiency is a broader concept and vitamin is one part of micronutrient. Although, several studies confirm that children with low consumption of vitamins are at a higher risk of stunting compared to those children having micronutrient-rich diet intake (Akhtar et al., 2013; Imdad & Bhutta, 2011; Ramakrishnan et al., 2009; Rammohan et al., 2012). Furthermore, vitamin deficiency (i.e., micronutrient deficiency) in children can instigate a cycle of illness due to weakening immunity of children and make them vulnerable to diseases like blindness, anemia, and morbidity, and child mortality (Ahmed et al., 2012; Bhaskaram, 2002). Pakistan’s Multi-sectoral Nutrition Strategy (2018–2025) is a welcome step in dealing with the issue of malnutrition and talks about vitamin A supplementation, zinc supplementation, and nutrition counseling for the risky population especially, children of less than 5 years (6–59 months), although, implementation is a daunting challenge (Ministry of Planning, Development & Reform and World Food Programme, 2018). The vitamin intake has been found a significant predictor of other srudies as well (Haszard et al., 2019; Stewart et al., 2013; World Health Organization; United Nations Children Fund, 2009).
The age of a child is an important predictor of stunting. In this analysis, the age of child 6 to 11 and 12 to 23 months is significantly associated with child stunting status as compared to children of age 0 to 5 months. The recent PDHS (2017–2018) also points toward this phenomenon. For example, stunting prevalence in children of less than 6 months is 22% and it increases to 39% for children of age 18 to 23 months (National Institute of Population Studies, 2018). The initiation of childhood stunting starts in the womb (gestation period) and pointed toward the first 1,000 days as a window of opportunity for better child health outcomes. The second stage is when children rely on breastfeeding and complementary feeding (Asim & Nawaz, 2018). Empirical studies from Pakistan (Khan et al., 2019) and Tanzania (Sunguya et al., 2019) confirm that the age of a child is an important predictor of stunting. The reasons explained in various studies for this significant association are not timely initiation of supplementary feeding practices, and poor diet quality (Tiwari et al., 2014). Also, it is with the increasing age that the exposure of a child increases to poor quality and unhygienic food and water, sanitation, and hygiene (WASH) conditions and thus retard linear growth of a child (Titaley et al., 2019).
A mother’s education is also important to affect childhood stunting. Maternal education is found to have a significant impact on child stunting, as the mother’s education increases, the odds of stunting decrease. The mothers having lower education have higher odds of having stunted children in Punjab (whole) as well as in rural Punjab. This result is also confirmed by a study from South Asia (Krishna et al., 2018) and Tharparkar-Sindh (Sand et al., 2018). The odd of stunting is not being affected significantly by different levels of education in urban areas except for the secondary level of education. In urban areas, as compared to higher education, mothers having secondary education have lower odds (51% lower odds) of their children being stunted. Mothers having the secondary level of education living in urban areas have access to better health facilities and with use of media, they can get efficient use of the resources available. As acompared to a higher level of education, mothers having a secondary level of education may have more time to nurture their children because they are usually less educated for the urban labor market. Women with higher education despite having all the facilities and education may lack time to provide the child with ample care and usually depend on daycares where the caretaker is usually less educated. On contrary, in rural areas, the odds of stunting in children of mothers with secondary educations is twice compared to mothers having higher education. The risk of undernutrition, the socioeconomic disadvantage is substantially higher in rural children coupled with lack and access to health care facilities (Fox & Heaton, 2012; Khuwaja et al., 2005; Shah et al., 2003). Mother’s education and its significant association with childhood stunting can be explained through these three channels. First, highly educated mothers are relatively more aware of food rich in nutrition, second, can have better healthcare information and feed their children in a better way and finally, educated mothers are relatively more aware of the hygienic environment for their household in general and their children in particular (Sharaf et al., 2019; Som et al., 2007). Focus on women’s literacy will help lower the incidence of stunting as is confirmed in Nepal and Bangladesh (Headey et al., 2015; Headey & Hoddinott, 2015).
In our analysis, ANC visits of more than four times are associated with significantly lower odds of stunting. During ANC visits, pregnant mothers get interaction with healthcare providers (doctors or lady health workers) that enhances their knowledge about pregnancy, their health, and of their children (Hamel et al., 2015). Due to enhanced awareness of mothers about proper diet and health care and timely identification of any prevalent health issue, the chances of stunting of a child reduces. Antenatal care visits (ANC) are significantly associated with childhood stunting in Punjab, Pakistan. The antenatal care has been found to be a significant predictor of stunting by previous studies as well (Aguayo et al., 2015; Hong et al., 2006).
The wealth status of households significantly affects the odds of their children being stunted. Our result confirms for Punjab that children with a poor background as compared to the richest have significantly higher odds of being stunted. As the wealth status of the household increases, the odds of children being stunted decrease, and this pattern is confirmed in both urban and rural areas. Our result is also in line with the study conducted in Pakistan (Khan et al., 2019). Moreover, the studies from Bangladesh, Peru, Pakistan, Tanzania, and Nepal confirm that odds of stunting are significantly higher in households with low socioeconomic status (Akombi et al., 2017; Asim & Nawaz, 2018; Das & Gulshan, 2017; Sunguya et al., 2019; Tiwari et al., 2014). It is because poor households have limited access to healthcare services and safe and sufficient food which may lead to growth retardation in children (Chowdhury et al., 2016). Of note, poor households (especially in urban areas) are unable to afford nutritious food such as meat, poultry, milk, and fruits that leads to nutritional deprivation of children and thus stunting (Ahsan et al., 2017; Vorster, 2010).
Animal (livestock) ownership can play a significant role in child stunting. Our analysis shows that having animals in the house significantly decreases the odds of being stunted by 15% in overall Punjab. The animals in the house have a direct effect as they become a source of food and nutrition such as milk and eggs and hence help in the reduction of childhood stunting. In addition to the direct effect, animal possession has also an indirect effect on child stunting. The animals serve as a source of wealth in times of crisis and help to reduce income constraints that can be used on child health. Surprisingly, animal possession is not significant in rural and urban Punjab and thus needs further investigation. This result was confirmed from studies from Uganda, Cambodia, and Eastern Africa (Azzarri et al., 2014; Ikeda et al., 2013; Mosites et al., 2015). The study using Demographic Health Surveys from Ethiopia, Kenya, and Uganda found that the presence of animals could be beneficial by reducing nutrient deficiency through the provision of animal-source food (Mosites et al., 2015).
Clean water and sanitation facilities can also improve the odds of not being stunted. Our analysis shows that the odds of being stunted decrease if the main source of drinking water is improved and treated. The association of improved sanitation facilities was found to significantly affect the odds of stunting at a 10% level of significance. Contrary to our findings, several studies (Cameron et al., 2013; Clasen et al., 2014; Cumming & Cairncross, 2016; Patil et al., 2014) found no association of sanitation with stunting. The provision of safe drinking water and improved sanitation can influence child stunting through the reduction in infectious diseases (Cumming & Cairncross, 2016). Multilevel analysis suggests that stunting has a 14% variation at the household level in urban areas, which means there are more factors involved at the household level besides included in our model, which can play an important role in explaining stunting. Further studies can investigate household level factors associated with stunting deeply in (urban) Punjab.
Our study has added to the debate of stunting in the following ways; first, it has analyzed a provincially representative large set of children (about 10,080 children of less than 2 years) data, which was hierarchical and provincially representative. Of note, we have made use of multilevel logistic analysis that was a suitable option as our data structure is hierarchical. Therefore, this study has estimated the variation at the household and child level for better policy formulation. Second, this study has focused on factors associated with the prevalence of stunting in children under 2 years of age in one of the largest provinces of Pakistan, Punjab that was a critical period of child growth, and this was not done before at the provincial level. Additionally, we have estimated the rural and urban models of factors associated with childhood stunting separately in this paper. Finally, it was in this study that we have analyzed the intake of the vitamin by children, household possession of the animal, drinking water, and sanitation as our main predictors, besides traditional variables, by following literature (Clasen et al., 2014; Headey et al., 2015; Patil et al., 2014).
This study has the limitations such as MICS is a cross-section data and hence, we cannot establish the causal relationship of our estimated coefficients with outcome variable, that is, stunting. Furthermore, MICS data does not provide the health status and women empowerment status both are crucial for better child health outcomes. In addition, MICS Punjab does not provide income and expenditures data that is a better variable to judge poverty and inequality links with stunting, whereas MICS has data for the wealth status of a household that is rather a weak proxy.
Conclusion
In this study, the analysis of the data suggests that the odds of stunting are higher in children having a smaller size at birth, children not taken vitamins, children whose mothers have received ANC four or more times and mothers having lower education. Furthermore, children belonging to the poorest and poor household wealth status as compared to the richest have a higher prevalence of child stunting. Our study has found individual, parental, household, and regional level factors, which can affect a child’s stunting. Women’s access to better and accessible health care, especially prenatal can improve both mother and child health outcomes. Recent government initiatives to distribute animals and livestock (chicken, cows, goats, etc.) to poor and marginalized households will help reduce relative poverty by reducing the income constraint and nutritional status of the household. Income support programs by the government will not only help in reducing poverty but will also contribute toward the better health of children.
This study has very important implications, especially for policymaking. Healthy children can make a healthy nation and can contribute to economic growth. Reducing health inequality is also the agenda of 2030 Sustainable Development Goals. A better health care system with improved access and awareness can play a vital role in improving children’s health and nutrition. Women’s access to better and accessible health care prenatal and postnatal can improve both mother and child health outcomes. Focus on women’s literacy will eventually increase maternal education level and can reduce the incidence of stunting.
Our study has found individual, parental, household, and regional level factors, which can affect a child’s stunting. Multilevel analysis suggests that stunting exists at the household level. Further investigations can be done to find more household, parental, and region level factors with a special focus on children under 2 years of age as that age are very critical for growth. The stunting can be compared with other health inequalities such as being underweight, arising from malnutrition.
Footnotes
Acknowledgements
We would like to thank Mr. Maqsood Sadiq for making us aware of the MICS Punjab 2017 to 2018 data and helped us understand the codes and various questionnaire modules.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research. Hence, a separate approval from committee was not required.