
Abstract
This research aims to advance the understanding of gamification in health care management using a systematic review of the literature through a multiphase analysis. To do so, first, we extract the relevant bibliographic data for our research according to a methodology of data generation structured in six stages and a descriptive analysis oriented to the technical characterization of the data. Then, we codify all the information, identify the main attributes with the collaboration of two independent experts and check their validity using the evaluation of two focus groups of professionals in gamification and health care management. We found seven attributes: (1) health care users, (2) psychology, (3) behavior, (4) activities, (5) health field, (6) technology, and (7) gamification elements. Within each of these seven attributes, there are a series of main elements that are detailed in the following for each of them. (1) Health care users: their age and the role they play in the health system. (2) Psychology: cognition, positive and negative emotions. (3) Behavior: healthy behavior encouragement, such as compliance, collaboration and responsibility. (4) Activities: physical activity and food. (5) Health field: preventive medicine and chronic diseases. (6) Technology: cell phones. (7) Gamification elements: different elements, but the number of articles in which these elements and their interactions are studied in depth is limited. Our results point toward a promising present and future research agenda that is in parallel with the development of relevant fields for the sector, such as chronic diseases, health education and preventive medicine.
Plain Language Summary
This research aims to advance the knowledge of gamification in healthcare management using a systematic literature review through a multiphase analysis. Our results point to a promising present and future research agenda parallel to developing fields relevant to the sector, such as chronic diseases, health education, and preventive medicine.
Introduction
The increase in life expectancy (Nigri et al., 2022) has led to a change in the objectives and operation of health services, which have thus had to focus on chronically ill individuals (Mazzucca et al., 2021) and promote healthy lifestyles (Barroso et al., 2021; Bossen et al., 2022). Furthermore, the patient has also undergone a paradigm shift from being a passive subject to becoming the protagonist of his or her own health (Grover et al., 2022). Therefore, it is necessary to provide this chronic and empowered patient with motivation mechanisms (Zahmatkeshan et al., 2021) to guide him/her in a stable and continuous approach toward new behaviors and health habits (Ippolito et al., 2020).
Thus, patient motivation becomes a necessity (L. C. M. Johnson et al., 2021; Reed et al., 2021), and gamification, which has proven in other areas to be useful for this purpose (Koivisto & Hamari, 2019; Murillo-Zamorano et al., 2023) and for changing behavior as, for example, in the case of hospital management where thanks to gamification it is possible that doctors provide patients with more personalized care (J. Kim & Castelli, 2021). Considering the above, gamification can be a great opportunity to facilitate and promote effective and successful health care management.
The concept of gamification was first used in 2008 (Deterding et al., 2011a), and, from there, different authors such as Zichermann and Cunningham (2011) or Werbach and Hunter (2012) have presented definition proposals, including the one that received a better reception in the scientific community, which was provided by Deterding et al. (2011b) and defines gamification as “the use of characteristic design elements of games in unrelated contexts.”
Since its conception, the level of attention given to gamification has not stopped growing (Deterding et al., 2011a), and the research on this subject, despite being new, presents a clear upward trend (Trinidad et al., 2021), which leads us to think that the concept responds satisfactorily to the needs of today’s society.
Its application, which is closely linked to innovation, is currently being carried out in very diverse contexts, such as education (Behl et al., 2022; Murillo-Zamorano et al., 2020), human resources (Murawski, 2021), tourism (Shi et al., 2022) and e-government (Contreras-Espinosa & Blanco-M, 2022). In the health field, gamification can be an effective tool to make people more committed to and responsible in their decisions such as, for example, the case of the patient adhering more easily and continuously over time to the treatments prescribed by the medical practitioner, as well as to promote the acquisition of new health behaviors and habits (Uechi et al., 2018), which is essential to increasing life expectancy (Limpens et al., 2022; Sun et al., 2021). In this sense, gamification has been used to promote physical activity (Koivisto & Hamari, 2019), to improve nutrition (Kurtzman et al., 2018), to promote adherence to medication (Abdul Rahim & Thomas, 2017), and to encourage hand hygiene (Lapao et al., 2015). In addition, it has also been used to optimize clinicians’ performance by promoting awareness of and commitment to them (McKeown et al., 2016).
In other words, gamification represents an opportunity to facilitate patient involvement in the management of their disease and to promote healthy habits that improve their state of health. It should also be noted that gamification is closely linked to technology. While not necessary, gamification is often adopted through digital technology-based experiences (Qiao et al., 2023). The digitization of health care is a reality that has been accelerated following the COVID-19 pandemic (Al Knawy et al., 2022). Digital health care allows remote health monitoring and control (Mahajan et al., 2022), can improve the effectiveness of interventions (Ibrahim et al., 2022), and gamification can be implemented within these services.
Gamification is nowadays presented as a relevant aspect to improve the efficiency and quality of health care services management, representing an opportunity to involve the population in the care of their health. The impact of gamification can vary depending on whether the perceptions of the performer or the recipient of the service provided are being evaluated (Miranda et al., 2010; Zou, 2020). We must remember that technology is advancing rapidly, and as it continues to evolve, new opportunities will arise to adopt gamification through electronic devices such as mobile telephones or personal computers. Therefore, it is essential to know what is known about it so far in the health care field to direct future efforts to help improve the efficiency and quality of health system management. A relevant example in this context is the Corona-AI Project hosted on the Vodafone Foundation’s DreamLab platform created in collaboration with the Garvan Institute for Medical Research in Australia (Garvan Institute, 2021; Vodafone, 2020) and involving researchers from Imperial College London (Veselkov et al., 2019). Corona AI uses the potential of smartphones and distributed computing to examine the potential effect of molecules present in food and medicines on diseases caused by Covid-19 (Bueno Muñoz et al., 2022; Vodafone, 2020).
The elements of the game that define the framework of the gamification experience vary depending on the individuals, the environment in which they carry out their activity, and the objectives they seek to achieve with the gamification experience (Morschheuser et al., 2017). In health care management, these aspects present unique characteristics, which make it necessary to develop tools that provide comprehensive, objective and contrasting scientific information and thus avoid, as far as possible, the biases, contradictions and limitations that, as in any emerging field, the studies published to date present.
For this reason, this research aims to advance the understanding of gamification in health care management through a systematic review of the literature. The execution of a systematic review of the literature to establish a conceptual framework on which to develop a research agenda is a methodology that is widely used in medicine (Eden et al., 2011) and in other disciplines such as engineering (Dolgui et al., 2022) or business (Durach et al., 2021). In the health field, however, until now, only very general reviews on gamification and health care management that analyze few features in this regard (Al-Rayes et al., 2022; D. Johnson et al., 2016) or literature reviews on very concrete and specific aspects such as e-health (Sardi et al., 2017a) or physical activity (Koivisto & Hamari, 2019) have been published. Despite its relevance, there is, to date, no systematic review of the literature on the use of gamification in health care management following the approach specified in our study.
In addition, unlike others, our review is complemented by the collaboration of two independent experts. Thanks to their work, we identify the main attributes extracted from the systematic review, which, in addition, are evaluated by two focus groups of gamification and health care management professionals (Flick, 2022; Sim & Waterfield, 2019) which will be explained in detail in Section 3, Subsection 3.2 Phase 2: Focus groups. This allows us to advance our knowledge and get closer to the vision of professionals who develop their work in the field that concerns our research. Knowing what is being researched and where efforts should be directed is critical to guide future research on gamification in health care management, especially if we consider its potential to improve efficiency in this sector. To this end, we conducted a review to identify the attributes of gamification in the health care literature to guide the future research agenda (J. S. Kim & Chung, 2017) and provide policy-relevant results (Perkmann et al., 2013).
The concept of gamification used in this study is the one followed in the most relevant international literature, such as the work of Zichermann and Cunningham (2011), from which gamification could be understood as the application of the game to other fields and activities with humans interaction as could be the field of health care management. In this same line, we also have as an example of the definition of gamification used in this study, the one provided by Werbach (2014, p. 266), which defines gamification as “the process of making activities more game-like.”
With our research, therefore, we seek to provide a conceptual, objective and validated reference framework on which researchers and health policy makers can develop a research agenda aimed at more efficiently rationalizing the resources of the health system, improving the quality of health care management and increasing the satisfaction rates of health professionals and patients with the health service. To do this, we followed the multiphase analysis of Micheli et al. (2019). Professor Micheli, a Professor at the University of Warwick, is a renowned academic and consultant to multinational companies for over 20 years and has taught at a dozen European academic institutions. Professor Micheli and his research team have used the multiphase analysis in the past with robustness, publishing their results in a leading international journal. Through a multiphase analysis (Micheli et al., 2019), we first extract all the relevant bibliographic data for our research according to a methodology of data generation structured in six stages and a descriptive analysis oriented to the technical characterization of the data. Then, we codify all the information, identify the main attributes with the collaboration of two independent experts and check their validity by evaluating two focus groups of gamification and health care management professionals (Flick, 2022; Sim & Waterfield, 2019).
In accordance with the above, this paper is structured into five sections. After this introduction, the second section is dedicated to compiling the relevant bibliographic data for our research and their descriptive analysis. The third section codifies and identifies the main attributes by relying on independent experts and specific focal groups of gamification and health care management. After the final synthesis developed in this third section, in the fourth section, we proceed to discuss the main attributes identified in the systematic review of the literature. The fifth section is dedicated to discussing and comparing our results with the existing literature. Finally, the sixth section presents the conclusions of our study.
Literature Review
A clear and rigorous methodology is critical in ensuring the reproducibility of results (Micheli et al., 2019; Silva et al., 2020; Verganti et al., 2021). To this end, we begin our analysis with a literature review structured in two sections. First, we gather bibliographic data related to the object of study of our research. In the second section, we implement a descriptive analysis aimed at characterizing the articles selected in the previous section.
Data Collection
This first phase of the search, in which we identify the bibliography that studies the two concepts, gamification and health care management, was developed following the methodology of Micheli et al. (2019), as shown in the six stages detailed in Figure 1.

Stages of the data collection process.
The first stage, which consists of an initial search for the selected terms, is carried out in five databases, namely, four multidisciplinary databases (Web of Science, Scopus, Science Direct, Springer Link) and one health-specific database (PubMed). In the second stage, we add to the located articles other articles located from their references, and in the third stage, we eliminate duplicated articles. The fourth stage consists of a selection of articles that meet the objectives of the review according to the titles and abstracts. Then, in the fifth stage, the articles are refined according to the quality of the complete articles. Finally, in the last stage, the final articles are generated. Later, by obtaining a series of attributes and codes, the scientific literature on gamification in the health field is reviewed.
Once introduced, we describe in more detail the most relevant aspects of each of these six stages. Within the first stage, oriented to the initial search of relevant terms, it is worth noting that the field of application of games and gamification in health is wide. For example, physical activity (Harris, 2018b), training professionals (Garnett & Button, 2018), or even connecting people to the advances of medical science (Novák et al., 2016) should be promoted. To favor the precision and conciseness of our analysis, in this work, we circumscribe the field of research to gamification and health care management. For this purpose, in this first stage, the following boolean operators are used: (GAMIF*) AND (HEALTHCARE OR MEDIC* OR PHARMAC* OR NURS*).
GAMIF* search criterion is used to limit the review to gamification, excluding terms related to serious games (Verschueren et al., 2019). The basis of both terms is the same, that is, the game to motivate and create engagement (Krath et al., 2021); however, although in both aspects there is a non-game purpose, in gamification, the game elements are part of the system along with others that are not games, while the serious games are completely built on these elements (Kasurinen & Knutas, 2018; Laamarti et al., 2014). Regarding the search criteria used in the health field, we have employed HEALTHCARE search criterion. According to the WHO (Shimkin, 1946), HEALTHCARE refers to a set of services to promote, protect or restore health, with gamification being a tool of health services, to achieve health goals. To introduce the main health areas, medicine, pharmacy and nursing, we also introduce MEDIC*, PHARMAC*, NURS* and so on, and the different phases of health care management, prevention, diagnosis, treatment, rehabilitation and care are also included.
We also use HEALTHCARE and not HEALTH because the concept of health, according to the WHO (Shimkin, 1946), refers to a “state of complete physical, mental and social well-being, and not merely the absence of disease.”
The search is carried out in June 2020 in the PubMed, Scopus, Science Direct, Web of Science and SpringerLink databases, which were selected based on their up-to-date, temporal and thematic coverage according to the study and their provision of links to the complete articles to facilitate the work of the researchers. In relation to the filters used, we apply the restrictions allowed by the databases (Table 1) and a time range of the years 2009 to 2020 because both the concept of gamification (Deterding et al., 2011a) and publications related to it (Kasurinen & Knutas, 2018) are recent in nature. In the end, we obtain a total of 2,989 results: 139 from PubMed; 1862 (Scopus); 6 (Science Direct); 167 (Web of Science), 815 (SpringerLink).
Databases and Search Criteria.

Once the first stage of our data collection process is concluded, then, in a second stage, in addition to these 2,989 articles collected, we add another 273 articles located in the bibliographic references of the first-stage search results, thereby generating a total of 3,262 references. In this way, we include other articles that make relevant contributions to the knowledge about the field of this study.
In the third stage, and through the Mendeley bibliographic manager, the 73 references that are duplicated in our results because they appear in different databases are eliminated. Then, the fourth stage consists of a phase of reviewing the articles, which entails the reading of the titles and the summaries for the elimination of those articles not relevant to the objective of this work by applying the rules detailed in Table 2. According to this procedure, at the end of this fourth stage, 358 results are eliminated.
Selection Criteria.

In the fifth stage, we perform a complete reading of the articles to exclude working papers, opinion articles, protocols and editorials to check that the methodology is adequate and that the individual, the problem, the intervention and the results all coincide with the objectives of this review.
Finally, in the sixth and last stage, we obtain 118 articles, which, ultimately and following the previous phases and selective filters, we will use in our research. We will proceed to the in-depth analysis of these articles. These 118 articles are classified according to the analysis methodology they use in Appendix 1 and are marked with an asterisk (*) in the bibliographic references section of this research.
Descriptive Analysis
After obtaining the 118 previously mentioned articles, in this second section, we proceed to their characterization according to aspects such as the year of publication, their bibliographic references or the journals in which they are located. As seen in Figure 2 and because gamification is a recent term (Landers et al., 2018), in the first years of the search, the number of articles located is reduced but presents a continuously increasing trend. The first article appears in 2010, and it is not until 2013 that the constant increase in the accumulated percentage of publications in the field of research concerns us, that is, the gamification of health care management begins.

Publication year of articles on gamification and healthcare.
The 118 articles selected belong to 92 scientific journals (Figure 3) and have a theme that is directed mainly at public health (26) or medical clinics (22), although there are also references to computer science (18), health (12), and technology (9).
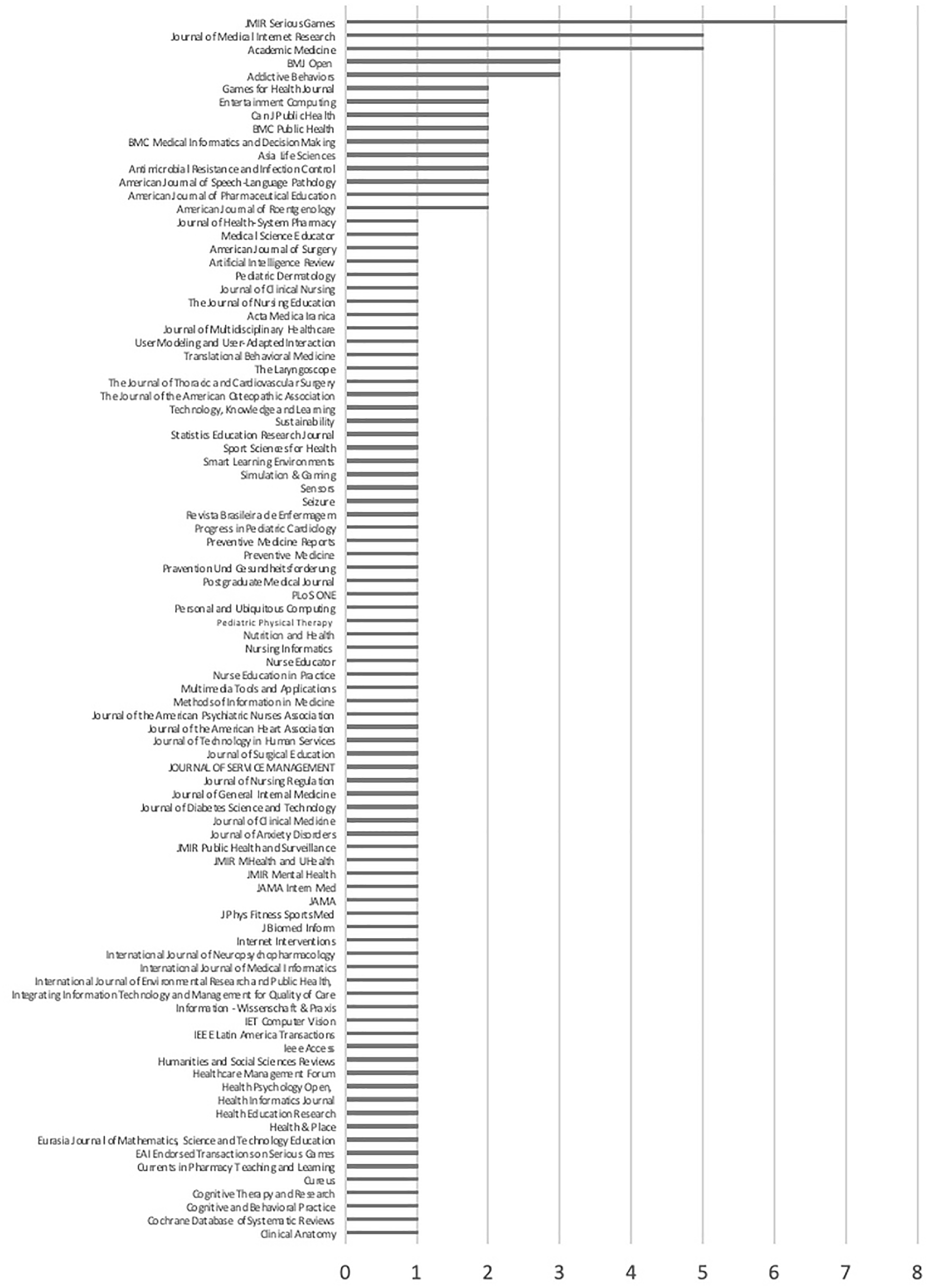
Scientific journals where the selected articles were located.
According to their analysis methodology, we identify four types of articles (Appendix 1): studies with participants, theoretical framework studies, literature review studies, and evaluation studies of apps and software. In the first group, the number of studies in which “N” exceeds 1,000 participants is scarce (Harris, 2019); only six randomized and controlled trials are included, and they do not measure health outcomes as often as they measure individual behavior. The studies that refer to the theoretical framework and the review of the literature address the use of gamification in a wide variety of fields, both clinical and educational. Finally, in the group of studies dedicated to app and software evaluations, expert analyses abound.
For the bibliographic references on the concept of gamification that are the most cited in the studies analyzed (Table 3), the most popular is that of Deterding et al. (2011b), which is present in 42% of these studies. This reference is followed by the meta-analysis of Hamari et al. (2014), which is cited in 22% of the cases studied.
Most Frequently Cited References on Gamification.

In light of these references, we can conclude that there is some consensus among researchers regarding Deterding et al.’s (2011b) definition of gamification as “the application of game elements in non-game environments.” This consensus is a good starting point for the research objectives of this article.
Construction of Coding and Attribute Identification
The coding of constructs consists of the extraction of certain words or concepts that reflect the main content of the articles examined. At this point, we exclude formal aspects such as the type of research, methodology, or data collection and instead focus on those characteristics that strictly refer to gamification and health care management. After a first identification, we unify the codes with similar meanings, for example, “old age,”“elderly,” and “senior citizens.” As a final result, we identify 183 codes associated with the current state of research on gamification in healthcare.
After the initial coding of constructs carried out by the research team, we proceed to the identification of attributes. This attribute identification is organized in three consecutive phases. In the first phase, we request the collaboration of two independent experts. Then, after verifying the reliability of the attributes obtained by the two experts through inter-rater reliability analysis, in a second phase, we check the validity of the code assignment by evaluating two groups of professionals using the focus group methodology (Kitzinger, 1995). Finally, after these two preliminary phases, the authors of this research proceed to make the final synthesis. In the following, we present in detail each of these three phases aimed at coding and identifying the main attributes of our research.
Phase 1: Independent Experts
Many of the codes extracted from the 118 articles selected for our research refer to concepts that are closely related to each other. Therefore, following the methodology of Micheli et al. (2019), two independent experts proceed to group these codes, according to their definitions, into higher-order attributes. To provide a multidisciplinary vision, experts are sought who have different professional and academic profiles. Thus, the first of the experts has a background in nursing, political science and sociology and has experience in the health care management field, health planning and inspection. The second expert is an industrial engineer and has worked in business management.
The two experts were previously informed by the research team of the objective, conceptual foundations and methodology of the work in which they were going to collaborate. They were provided with the list of codes so that they could independently generate a series of attributes, each of which identifies a set of codes. Following this procedure, the first expert identifies seven attributes, and the second identifies 10. Thus, the researchers compare the results of the two experts. For two of the attributes, that is, “psychology” and “behaviors,” the experts agree on the use of the same name. A correlation is also observed between the codes contained in the attributes of “technology” and “electronics” and “health/medicine” and “medical science.” Lower levels of coincidence, although some similarity, are also observed between the codes grouped by the experts as “activities” in one case and “life stages” in the other.
In any case, to check the quality of the analysis of the qualitative data, it is necessary to verify that the selected attributes are correct representations of the codes. This requirement is tested by calculating the interrater reliability or reliability indices among the evaluators (Gisev et al., 2013), with a result of 59%, which is a high score for an initial coding phase.
Finally, to improve the convergent and discriminant validity (Rosenthal & Rosnow, 1991) of our results, we proceed to assess the discrepancies and similarities, selecting a final set of attributes that show greater coincidence levels while modifying the definition and naming of some of them. As a final result, we obtain the seven attributes described in Table 4. The first group refers to health care users, the second alludes to aspects related to psychology, the third contains codes related to behavior, the fourth refers to activities in which these behaviors are developed, the fifth describes the health field, the sixth refers to the elements and other aspects of applied gamification, and finally, the last section of attributes describes the technology that defines the environment of application of the study.
Item Attributes.

Phase 2: Focus Groups
After categorizing the attributes, we proceed to confirm the validity of the analysis. For this purpose, we resort to the evaluation of professionals from the health and gamification sectors using the methodology of focal groups (Flick, 2022; Kitzinger, 1995). This technique represents the most flexible and adaptable methodology within the field of qualitative research analysis, which gives robustness to the analysis and enhances the validity of the conclusions derived from the results provided by our research in this particular aspect of our analysis (Chioncel et al., 2003; Vogt et al., 2004). Figure 4 shows the steps used to implement the methodology of the two focus groups used in our study. The health care management focal group is made up of four doctors, one nurse, and one pharmacist, both from the public sector (four doctors and one nurse) and the private sector (one pharmacist) and with experience in health care management (all of them), research (two of them), management (two of them) and health technology (one of them). The focus group of gamification professionals is made up of seven people, two from the field of education, four from consultancy, and one from video games. Of these seven people, five have publications, and six provide training on gamification.

Development of the focus group exercise.
Despite the different backgrounds and extensive knowledge and experience of the members of each of the two groups, the consensus in the assignment of codes is remarkable, confirming the validity of the results obtained initially. In fact, in one of the groups, only the change of the school and community codes from the health care users attribute to the activities attribute is proposed, and in the other group, the incorporation of the resilience code to the behavior attribute is proposed.
Among the ideas contributed by these professionals, the health professionals express the lack of quantitative studies that measure the health outcomes of patients, while the professionals from the educational field suggest other attributes such as psychology and pedagogy and codes such as emotion, learning, and communication, among others. Other contributed ideas consist of the need to clearly identify the objective and the user in every gamification process, the need for co-creation with professionals from different fields, and the need of the health world to have tools for the motivation of patients and professionals.
Phase 3: Final Synthesis
After the codification of the articles, the preliminary analysis of the independent experts and the verification of professionals through the focus groups, we proceed to the final synthesis. The result of this synthesis appears in Table 5, in which we collect the ultimately identified and selected attributes, the number of articles in which these attributes are present, and the codes associated with each attribute, together with an example of the literature for each of them.
Codes, Attributes and Frequency of Occurrence.

In a first reading of the previous table, we check the different frequencies of the different attributes, which indicates that not all aspects have been the object of the same attention. Thus, in 99 articles, the health field is described; in 88 articles, behaviors are described; in 66 articles, technology is used; 43 articles describe the health care users; 31 articles describe psychological aspects; 62 studies focus on activities; and 34 articles mention elements of gamification. Similarly, we note that some attributes, such as technology, contain a small number of codes, although there are a high number of publications, and in others, such as the health field, the dispersion is much greater. This result may indicate that while the application of gamification is carried out with a series of very specific technologies (mobiles or apps), it is nevertheless applied in a wide spectrum of facets in healthcare.
Discussion of the Attributes of the Literature on Gamification in the Health Field
The current health system, in which public health, chronic diseases and patient empowerment have become very important, requires tools that promote the motivation of both patients and professionals. The work of Qiu (2017) notes the usefulness of gamification, a tool which, although not exempt from discussion (Hung, 2017), is very implanted in other areas such as education and business, in achieving this objective. Therefore, in this work, we analyze scientific articles related to gamification and health care management published from 2009 to 2020 with the aim of providing managers, professionals, and researchers a solid framework on which to base their practical application and identify those aspects where it is necessary to deepen their research.
This review is, therefore, a notable contribution to the literature for responding to the important need already indicated and for presenting several innovative aspects at both the conceptual and methodological levels. At a conceptual level, we can highlight that, first, gamification itself is a recent concept (Landers et al., 2018) and, second, its use in a context other than educational and business contexts, such as health, is also very novel and has a clear and constant upward trend. On a methodological level, this research presents an appreciable contribution by conducting a systematic review of gamification in the health field, in which only partial reviews have existed to date (m-Health, mental health, promotion or training). For this contribution, we have relied on the participation of independent experts according to the methodology of Micheli et al. (2019), thereby complementing it, in addition, with the participation of focal groups both in the health field and in that of gamification.
After this process, we observe, first of all, that there is a wide consensus in the specialized literature on the definition of the concept of gamification, being, in this sense, the most cited articles of Deterding et al. (2011b), Hamari et al. (2014), and Zichermann and Cunningham (2011). Regarding the type of publications, studies with participants are the most frequent, although only six randomized and controlled trials have been published. Most of these studies measure individual bebehaviors but there is a lack of studies measuring health outcomes. Other types of articles generally address the theoretical framework, conduct partial reviews of the literature, or evaluate programs and applications.
Second, in this work and as an additional contribution to the literature, we have determined that the most relevant aspects of the content of the research published to date in the field of gamification in the sanitary sector refer mainly to the following seven attributes: (i) the characteristics of the health care users to whom gamification is applied, (ii) its psychological aspects, (iii) the behaviors of these health care users that we intend to promote, maintain or avoid, (iv) the activities in which these behaviors are included, (v) the fields of the health field in which it is used, (vi) its relationship with technology, and (vii) the gamification elements used.
Health Care Users
The detailed and in-depth study of the healthcare users to whom the gamification experience is directed is a crucial step for its adequate implementation (Hamari et al., 2014) and for the effectiveness of the gamified experience (Orji et al., 2017). In this sense, our analysis shows that there are two main characteristics of the health care users on which most of the studies analyzed focus, namely, age and the role they play in the health system. In terms of age, the most frequent groups are adolescents and elderly individuals. The objectives of gamified experiences in these groups are encompassed in different areas identified within the Health field attribute. For example, activities aimed at adolescents are linked to promoting sexual health (Haruna et al., 2018) or nutrition (Wilson & McDonagh, 2014). Regarding elderly individuals, gamification in the health context seeks to promote physical activity (van Stralen et al., 2010) and adherence to and compliance with treatments (de Vette et al., 2015).
Regarding the role of the user in cases of gamification in the health sector, the most repeated occupations are those of students, with the purpose of promoting health habits (Earle et al., 2018) and their training in different health areas (Garnett & Button, 2018), and the occupation of resident doctors in contexts related to learning (Mokadam et al., 2015) and training (Nevin et al., 2014). This is in line with the results of general reviews about gamification, which point to education as its most important application sector (Kasurinen & Knutas, 2018; Klock et al., 2020).
However, our research highlights the marginal treatment, to date, by the experiences of gamification developed in the health field, of both the user in his or her role as a patient (Caliskan et al., 2018) and in his or her role as an employee of the health sector (Hammedi et al., 2017). In addition, regardless of the role played, we have noted a lack of studies that typify health care users from the point of view of their relationship with the elements of the game (Marczewski, 2015). This is an important handicap in regard to successfully applying gamification techniques in any context, including health.
Psychology
The aim of gamification is to activate the motivation mechanisms of the participant in the gamified experience, and this activation, from the point of view of psychology, is achieved through emotion and cognition (Mullins & Sabherwal, 2020). According to our research, we have verified that many articles refer to aspects such as psychology (Harris, 2018b), cognition, or memory (Savulich et al., 2017). They also study the positive emotions generated by competition (Kawachi, 2017) and well-being (D. Johnson et al., 2016) and negative emotions such as apathy (Savulich et al., 2017) or boredom (Lumsden et al., 2017). In any case, our research shows that many of these investigations lack a systematic, structured analysis with quantitative empirical evidence of the relationships between the use of gamification in the health sector and its effects on motivation, engagement and behavioral change of the end user to whom the gamification experience is directed. Quantitative research on these aspects is essential to better understand the effects of gamification in specific healthcare environments and to be able to design effective gamified experiences that achieve the objectives for which they were created.
Behavior
Another central attribute that our systematic review of the literature has identified in the field of gamification in the health field is behavior, with 88 references. Not in vain, the ultimate aim of all gamified experiences is to favor the change of behaviors related to the health of the user who participates in the mentioned experience, as well as its maintenance in the time of new acquired health habits (Seaborn & Fels, 2015). In numerous articles, the codes of behavior (Schoech et al., 2013), engagement (Wilson & McDonagh, 2014), motivation (Wollmann et al., 2016), and encouragement appear. Healthy behaviors are encouraged, such as compliance (Leinonen et al., 2017), collaboration or responsibility, as well as the abandonment of harmful behaviors, such as mistakes, neglect, variability, and violence (Savulich et al., 2017).
Activities
Our research also shows the existence of a clear tendency in the most recent specialized literature to analyze the relationship between gamification, the population’s lifestyle and its formation. All these aspects are included in the general attribute of Activities. The most effective interventions to improve health are related to one’s lifestyle (Kraft et al., 2009), and within this health determinant, the most numerous activities where gamification is applied are related to physical activity (Steinert et al., 2018) and food (Jones, Madden, Wengreen, Aguilar, & Desjardins, 2014). Activities related to training range from patient education (Theng et al., 2015) and health education in schools (Haruna et al., 2018) to training professionals either at universities (Lemermeyer & Sadesky, 2016) or in their practice as resident physicians (Nevin et al., 2014). Additionally, although to a lesser extent, gamification practices in the literature appear to promote other professional activities, such as handwashing (Lapao et al., 2015) and research (Sardi et al., 2017b). From our point of view, there are other activities in the healthcare field that could be gamified. For example, as mentioned in the health care users attribute, our research highlights the marginal treatment of the user in his or her role as an employee of the health sector. However, employees in the health sector represent potential health care users of gamification. In other sectors, gamification improves employee satisfaction and engagement (Silic et al., 2020); which, in the health care sector, can lead to an improvement in service quality (Perreira et al., 2018).
Health Field
Health care management, which is the object of analysis in this research, constitutes a very broad and diverse field of knowledge with a large number of different sectors, levels of care, pathologies and professions. Therefore, it is vital to determine those contexts where gamification becomes more relevant. Preventive medicine and chronic disease are the areas in which much of the current research in the gamification of health care management is focused. Preventive medicine is reflected in codes such as promotion (Horstmann et al., 2018) or prevention (Lapao et al., 2015). This is consistent with the results previously discussed in the Activities attribute, in which we have pointed out that the activities identified as most relevant are those related to physical activity and food, which are two aspects closely linked to a healthy lifestyle and health promotion.
Chronicity (Giunti et al., 2018), which is currently a priority for health systems at the global level (Madrid & McGee, 2019), is visible in articles related to the chronically ill, adherence to treatment (Leinonen et al., 2017), rehabilitation (Kontadakis et al., 2020), or relapses (Vervaeke et al., 2018). Regarding the predominant pathologies, chronic diseases such as diabetes (Priesterroth et al., 2019), obesity (Van Lippevelde et al., 2016), or mental health (Brown et al., 2016) are common.
Technology
Another attribute identified in this systematic review of the literature shows that, as in education (Tsay et al., 2018) and business (Adornes & Muniz, 2019), in the health field, there is also a close relationship between gamification and new technologies. Technology, with a frequency of 66 references, represents the third attribute with the greatest presence in the articles included in this review. Precisely, it is placed behind the Health field (99 references) and Behavior (88 references). This highlights the close relationship between gamification and technology in its application in the healthcare field. Authors from other disciplines have pointed out the link between both concepts and note that, although gamified experiences can be created in a non-technological context (See, 2020), technology facilitates their application (Murillo-Zamorano et al., 2019; Parapanos & Michopoulou, 2019).
The most commonly used technological device for the implementation of gamification experiences in health care management is the cell phone. Numerous articles refer to mobile phones (Kontadakis et al., 2020), smartphones (Kurtzman et al., 2018), mobile health (Gremaud et al., 2018), and apps (Hightow-Weidman et al., 2018). Other areas of technology also detected in our research are e-Health (Uechi et al., 2018) and the use of social networks (Ahola et al., 2013) or the Internet (Horstmann et al., 2018). Concerning the healthcare areas of application of technology and gamification, gamification is used in the following areas both training through simulation (von Barnekow et al., 2017) or MOOC course platforms (Steinert et al., 2018) and in the treatment or diagnosis of patients through physical activity (Uechi et al., 2018), rehabilitation, telemedicine (Giunti et al., 2018), virtual reality, and wearables (Steinert et al., 2018).
Gamification Elements
Gamification elements represent the second least present attribute in the selected articles. We consider it convenient to emphasize within this section of the discussion that gamification is not effective per se. The use of one or more elements in the design of the gamification experience leads to different results (Sailer et al., 2017) because each element satisfies different needs (R. M. Ryan & Deci, 2000). It is therefore crucial to identify and use the elements of the gamification experience that best contribute to the achievement of the behavioral objectives set (Murillo-Zamorano et al., 2021). Despite this need, our research shows that the number of articles in which these elements and their interactions are studied in depth is limited. Some articles, such as Berger and Schrader (2016), refer to the mechanics of Werbach and Hunter (2012), while others allude to the elements of gamification in a nonspecific way (Edwards et al., 2016); finally, some, in even smaller number, allude to specific but disjointed elements such as feedback (Wollmann et al., 2016), rewards (Zuckerman & Gal-Oz, 2014), badges (Garnett & Button, 2018), levels (Afyouni et al., 2017), or points (McAuliffe et al., 2020).
It is necessary to note in the future research agenda both the theoretical concretion of these elements and the empirical contrast of their interactions with the objectives and health behaviors pursued by the gamification experience. It should also be noted that theoretical frameworks included in this review, such as those of Janssen et al. (2017) and M. D. Lee (2016), point out the need for collaboration between game designers and health care professionals to create appropriate gamified experiences. In this sense, they recommend that health care professionals know the game principles and participate in creating gamified designs framed in this sector.
Discussion
In recent years there has been increasing interest in gamification in the health care sector. We have conducted this systematic review to provide a conceptual, objective and validated reference framework on which researchers and health policy makers can develop a research agenda aimed at more efficiently rationalizing the resources of the health system, improving the quality of health care management and increasing the satisfaction rates of health professionals and patients with the health service. In the following, we discuss the results of our research and compare them with those obtained in other reviews on gamification in health care.
Our review includes a larger number of articles (118 articles, as of June 2020) than previous reviews conducted by Brown et al. (2016) in mental health (61 articles), D. Johnson et al. (2016) in health and wellbeing (19 articles), Sardi et al. (2017a) in e-Health (46 articles), Cheng et al. (2019) in mental health (70 articles), Martinho et al. (2020) in elderly care (103 articles), Tran et al. (2022) in medication adherence (11 articles), and Al-Rayes et al. (2022) in healthcare (22 articles), among others.
The most recent and general is the review by Al-Rayes et al. (2022) on gamification in healthcare. However, their review, unlike ours, only focuses on three aspects: which are the most employed elements, the main areas of application and the challenges it represents. Sardi et al. (2017a) carry out a systematic review of the literature on the use of gamification and serious games in e-Health. In their work, they perform a joint analysis of gamified designs and serious games, despite the existing differences (Krath et al., 2021). In this way, they analyze the domains within health where these resources are used, the research types of the studies and the benefits found. Other reviews have been conducted in specific domains within health care such as mental health (Brown et al., 2016; Cheng et al., 2019) and medication adherence (Tran et al., 2022). Some similarities and differences are found between our findings and those of previous reviews:
First, regarding health care users, our analysis shows that there are two main characteristics of the health care users on which most of the studies analyzed focus, namely, age and the role they play in the health system. Regarding age, D. Johnson et al. (2016) point out that the participants of most studies are adults, although some also target children and adolescents. In contrast, our review shows that studies focus on adolescents and elderly individuals. In the most recent literature, we can even find a review focused on the use of gamification in elderly care (Martinho et al., 2020). In reference to the role of the participants in the health care system, our review points out that students are the predominant ones. Education is the main area of gamification application (Kasurinen & Knutas, 2018; Klock et al., 2020). Moreover, in the literature we can even find reviews about the employment of gamification in health professions education (S. V. Gentry et al., 2019; van Gaalen et al., 2021).
Second, regarding the health field attribute, according to the study by Sardi et al. (2017a), the most analyzed topics are chronic disease management and physical activity, followed by nutrition, mental health and hygiene. According to the review by Al-Rayes et al. (2022), the most important application areas are physical fitness, chronic disease management, rehabilitation and physical therapy. D. Johnson et al. (2016) derive from their review that physical health and, in particular, the promotion of physical activity is the area with the highest concentration of studies. According to our review, the health fields with the highest number of studies are preventive medicine and chronic diseases. It should also be noted that in our study we identified many more codes within the health field attribute (70 codes) than in reviews by other authors.
Third, with regard to technology, our review indicates that the most important device through which gamification is implemented in health care is the smartphone. This is not surprising given that the smartphone has become an indispensable device that allows us to be connected to the Internet from anywhere and whose number of health care users has increased substantially in the last decade (Li et al., 2022). Edwards et al. (2016) analyzed the use of gamification in apps for health promotion and only 4% of the apps included in their study had a gamified design. However, it should be noted that, according to the review by Martinho et al. (2020) on the use of gamification in elderly care, the most commonly used technologies are self-management systems, portable devices, physical robots, consoles and wearable technologies.
Fourth, regarding gamification elements, the most employed according to the study by Sardi et al. (2017a) are feedback/rewards and social connection, followed by progress bars and challenges/quests. Martinho et al. (2020) point to feedback, progession/levels and rewards as the most important. Al-Rayes et al. (2022) find that the most important are points, leaderboards, levels, feedback and challenges. Brown et al. (2016), on the contrary, point out that story/theme is the most present element in mental health, while levels are not used in this field. However, the review by Cheng et al. (2019) in mental health reveals that the most important elements are levels/progress, points, rewards, narrative/theme, personalization and customization. In other words, the results differ between both studies conducted in the same field. In any case, as we have argued in the previous section, it is necessary to carry out more empirical research that explores the relationship between the elements and the effectiveness of the gamified experience. This research will help to gain a deeper understanding of how gamification works in this context and to develop guidelines or recommendations on which to base the gamification design process.
Finally, it should be noted that the attributes psychology, behavior and activities do not appear in the reviews carried out by other authors, or are encompassed within other attributes. For example, D. Johnson et al. (2016) differentiate between health care users with prior motivation and those without, concluding that in most studies participants had no prior motivation. In our case, we encompassed motivation within the behavior attribute. This lack of attention to psychology, behavior and activities is surprising given that gamification has been widely studied from a psychological basis in other fields of knowledge, being essential that its application is based on a theory of motivation (Landers et al., 2015). Likewise, through gamification, motivation is influenced to achieve a change in user behavior (Seaborn & Fels, 2015). In our review we have identified different behaviors present in the literature on gamification in health care such as the promotion of healthy behaviors such as compliance, collaboration or responsibility, as well as the abandonment of harmful behaviors.
As mentioned in the previous section, our research shows that there is a lack of systematic, structured analysis with quantitative empirical evidence of the relationships between the use of gamification in the health sector and its effects on motivation, engagement and behavioral change of the end user to whom the gamification experience is directed. Unlike the health care field, the relationships between motivation, engagement and behavioral change have been extensively studied in other fields of knowledge (Khodabandelou et al., 2023; Oliveira et al., 2023). Finally, we would like to point out that like any scientific work this one also has limitations. In our case, we have followed the methodological approach of Micheli et al. (2019) for the systematic literature review. There are other approaches in the literature, such as Domenico et al. (2021) or James et al. (2021), that propose alternative scenarios that could be considered in future research.
Conclusions
Healthcare, a sector in which public health, chronic diseases and patient empowerment have now taken on a central role, requires tools that promote motivation, engagement and behavioral change, both from the patient (L. C. M. Johnson et al., 2021) and from healthcare professionals (Veenstra et al., 2020). Gamification, which is understood as the application of game elements in non-playful environments, is a tool in continuous growth and expansion that can be very useful for these purposes.
The potential of gamification, which has already been effectively proven in the fields of education (Manzano-León et al., 2021) and business (Merhabi et al., 2021), does not, to date, have a theoretical frame of reference based either on its elements or on the interactions of these elements with the health objectives and behaviors demanded by the health care management sector. To the best of our knowledge, our research is the first to offer a systematic review of the literature on gamification in the field of health care management following the approach specified in our study.
The novel and systematic research methodology developed in this work has allowed us to introduce objectivity criteria, based on which we have identified the existence of a growing research interest in gamification in health care management, focused mainly on chronicity, lifestyle, preventive medicine and the training of professionals. To identify the codes and attributes present in the literature on gamification in healthcare management, we conducted a systematic review of the literature and then carried out a three-phase process. In these, two independent experts and, subsequently and based on their results, two focus groups contributed their vision in determining and grouping the codes and attributes. With this, we also provide clarity regarding the knowledge of professionals and health managers about the usefulness and applications of gamification in health care management.
Our research also reveals the existence of gaps that must necessarily be taken into account in the development of the research agenda for the coming years. On the one hand, there is a lack of studies that measure final results in the health of the population. On the other hand, there is a need for quantitative empirical evidence on the existing relations between the use of gamification in the health sector and its effects on user motivation, engagement and behavior change. Furthermore, it is necessary to go deeper into the typification of patients and professionals, as well as into the preliminary identification of those elements of gamification that are more effective in each particular context.
Our purpose with this study has been to provide a conceptual, objective and validated framework on which researchers and health policy makers can develop the agenda for future research in the gamification of health care management. In our opinion, the execution of this agenda will contribute to a more efficient rationalization of the resources of the health system, improve the quality of health care management and increase the satisfaction quotas of health professionals and patients in regard to health services.
Footnotes
Appendix
General Description of Selected Articles According to Methodology.

Author Contributions
All authors contributed equally to the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.