
Abstract
Burnout is a mental, emotional, and physical exhaustion that affects many healthcare workers. However, there is a lack of information in Ethiopia. Therefore, this study aimed to assess the prevalence of burnout syndrome and identify the associated risk factors among healthcare professionals in Dessie Comprehensive Specialized Hospital, Ethiopia. A cross-sectional study was conducted on randomly selected 251 health workers at Dessie Comprehensive Specialized Hospital. The Maslach Burnout Inventory-Human Service Survey was used to assess burnout (MBIHSS). A multivariable logistic regression analysis was used to explore the potential determinants of burnout syndrome among the participants. A total of 251 healthcare professionals were included in this study making a response rate of 99.2%. The prevalence of burnout syndrome among healthcare professionals was 15.1% (95% CI [10.8, 19.9]). Being male (AOR = 3.22:95% CI [1.17, 8.87]), lack of interest in their profession (AOR = 2.66, 95% CI [1.84, 6.02]), experiencing physical violence (AOR = 3.52, 95% CI [1.32, 9.36]), unsatisfied with their job (AOR = 4.17, 95% CI [1.46, 11.90]) were variables found to be significantly associated with burnout syndrome. Burnout is a major problem among working in Dessie Comprehensive Specialized Hospital healthcare professionals. Being male, having no interest in their job, having physical violence, and not being satisfied with their job contributed to burnout syndrome. Interventions to increase interest in there in their job, improve physician-patient relationships, provide safer workplace environments, and increase job satisfaction may be promising strategies to reduce burnout syndrome.
Plain Language Summary
Abstract Background: Burnout is a mental, emotional, and physical exhaustion that affects many healthcare workers. However, there is a lack of information in Ethiopia. Therefore, this study aimed to assess the prevalence of burnout syndrome and identify the associated risk factors among healthcare professionals in Dessie Comprehensive Specialized Hospital, Ethiopia. Methods: A cross-sectional study was conducted on randomly selected 251 health workers at Dessie Comprehensive Specialized Hospital. The Maslach Burnout Inventory-Human Service Survey was used to assess burnout (MBIHSS). A multivariable logistic regression analysis was used to explore the potential determinants of burnout syndrome among the participants. Results: A total of 251 healthcare professionals were included in this study making a response rate of 99.2%. The prevalence of burnout syndrome among healthcare professionals was 15.1% (95% CI [10.8, 19.9]). Being male (AOR = 3.22:95% CI [1.17, 8.87]), lack of interest in their profession (AOR = 2.66, 95% CI [1.84, 6.02]), experiencing physical violence (AOR = 3.52, 95% CI [1.32, 9.36]), unsatisfied with their job (AOR = 4.17, 95% CI [1.46, 11.90]) were variables found to be significantly associated with burnout syndrome. Conclusion: Burnout is a major problem among working in Dessie Comprehensive Specialized Hospital healthcare professionals. Being male, having no interest in their job, having physical violence, and not being satisfied with their job contributed to burnout syndrome. Interventions to increase interest in there in their job, improve physician-patient relationships, provide safer workplace environments, and increase job satisfaction may be promising strategies to reduce burnout syndrome.
Background
Burnout (BO) is a state of emotional exhaustion, cynicism, depersonalization in professional interactions, and decreased personal accomplishment that can affect anyone as a result of excessive work under stressful circumstances (Weitzer, 2015). Emotional exhaustion (EE) is characterized by a loss of energy, emotional depletion, enthusiasm tension, and frustration. Depersonalization (DP) represents interpersonal relationships with others in the workplace that leads to negative interaction. The sense of reduced professional achievement (PA) is defined as a tendency for healthcare workers to negatively judge themselves, making them feel less competent, as a result, it displays unhappiness with their work performance (Cañadas-De la Fuente et al., 2015).
Healthcare professionals (HCPs) are commonly grouped into health professions such as nurses, general practitioners, anesthetists, pharmacists, and laboratory technicians. The primary responsibility of HCPs is to provide a wide variety of care to patients seeking healthcare services. They regularly work in hospitals, health centers, and additional service delivery points (WHO, 2010). Although burnout (BO) affects individuals of all ages and occupations, it is highly prevalent among HCPs due to the intense and continuous nature of contact with individuals receiving care (Ângelo & Chambel, 2015). The BOS has a major psychosocial problem that affects professionals from different areas such as impaired job performance, cause of medical illness (like hypertension and myocardial infarction), marital difficulties, high levels of absenteeism from sickness, dependence on psychotropic substances, psychological changes including headaches, fatigue, sleep disturbances, irritability, anxiety, and depression also frequently occur (Cañadas-De la Fuente et al., 2015; Toker et al., 2012). This usually could result in high absenteeism or quitting of their job, significant declines in a variety of quality-of-life areas, and even lead to suicide in extreme cases if left untreated (Vukojevič et al., 2015).
Globally, different published works of literature among healthcare professionals reported, in Western countries, the prevalence estimated burnout to have of Netherlands 21% (Prins et al., 2010), France 34.6% (Moukarzel et al., 2019), and Germany 34.1% (Dreher et al., 2019). Another systematic review conducted in the UK showed 43% and 39% of females and males experienced burnout respectively (Amoafo et al., 2015). Likewise, Asian countries, the prevalence of burnout was in Japan 49.2% (Higuchi et al., 2016), and China 76.9 % (Qiao et al., 2016). In addition, in Singapore, the prevalence of burnout in their category showed emotional exhaustion 39%, depersonalization 40%, and low personal accomplishment 59% (Ang et al., 2016). Studies showed in Africa, Malawi the prevalence of burnout syndrome was 62% (Kim et al., 2019). Also, in some studies from Ethiopia Jimma 82.8% (Biksegn et al., 2016), Mekelle 47.6% (Redae & Dai, 2019), and Gondar 13.7% (Bhagavathula et al., 2018). Furthermore, in Arab countries also the prevalence of burnout Emotional Exhaustion is 20%, Depersonalization 9.2%, and Personal Accomplishment communication at 13.3% (Elbarazi et al., 2017). Several factors are associated with the development of HCP burnout, including age, unmarried, gender, negative marital status, low income, years of practice, number of years in training, long working hours, low reported job satisfaction, working at night, high perception of workload, interpersonal conflicts, low interest in the profession, professional level, use of negative coping, styles long duration of employment, depression, low social support, high levels of distress, working night shifts, poor response to patient’s needs, poor communication while handing patients, presence of chronic disease, job dissatisfaction, poor quality of sleep, and exposure to physical violence/verbal violence are all variables that increase the risk of burnout syndrome (Amoafo et al., 2015; Ang et al., 2016; Bhagavathula et al., 2018; Dreher et al., 2019; Ebling & Carlotto, 2012; Elbarazi et al., 2017; Fernando & Samaranayake, 2019; Hamdan & Hamra, 2017; Mattei et al., 2017; Moukarzel et al., 2019; Qiao et al., 2016).
A high level of burnout among healthcare professionals could lead to a reduction in their numbers and challenges their physical and mental well-being, which could consequently affect the quality of healthcare. These issues could result in a severe effect on the country’s healthcare system. Few existing studies were conducted in Ethiopia, particularly at the University of Gondar Hospital (Bhagavathula et al., 2018) and Mekelle City Hospitals (Redae & Dai, 2019), but no study was done to determine the prevalence and associated factors of burnout among healthcare professionals in northeastern, Ethiopia. Therefore, the present study has aimed to assess the prevalence of burnout syndrome (BOS) and associated factors among all healthcare professionals working at Dessie Comprehensive Specialized Hospital, Dessie, Ethiopia. This study will help policymakers, future researchers, and health planners, serve as a foundation for future public health and mental health research in the area. Additionally, it contributes to the development of knowledge about burnout syndrome.
Methods and Materials
Study Setting and Period
The study was conducted in Dessie Comprehensive Specialized Hospital from May 14 to June 01/2021. The hospital was established in 1942 and served 5 million people in Amhara regional state and neighboring Afar, which is geographically located in Dessie town is situated 401 km away from Addis Ababa to the North-Eastern part of Ethiopia, and 482 km from Bahir Dar, the capital city of Amhara regional state. The hospital has been given various services such as medical, surgical, ANC, obstetric, pediatrics, orthopedics, and regular follow-up. It has 563 healthcare professionals.
Study Design and Participants Selection
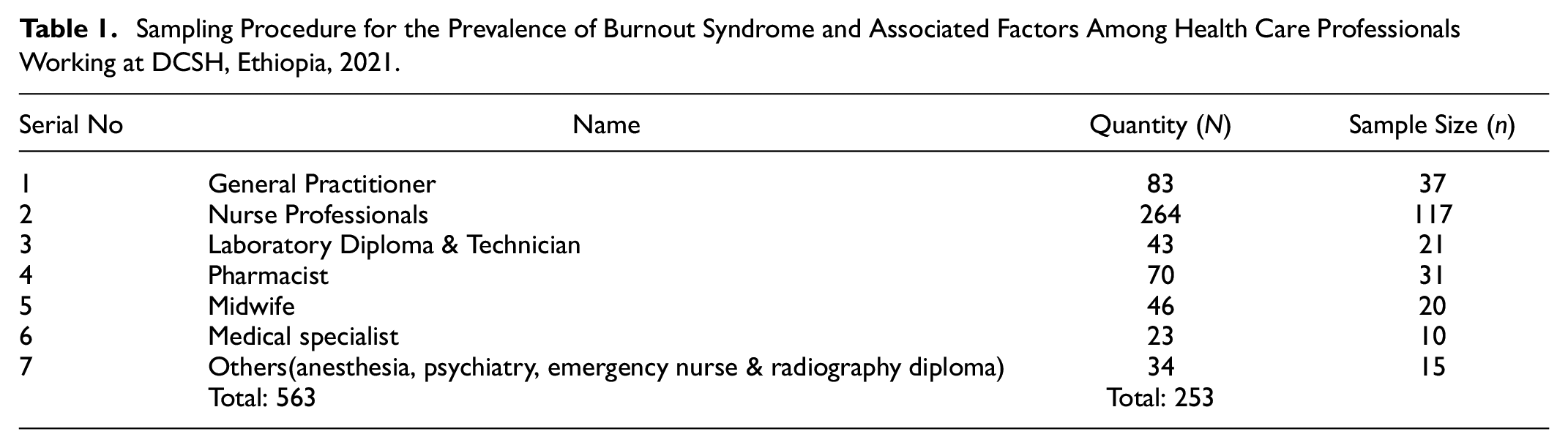
A hospital-based cross-sectional study design was employed. The actual sample size for the study was determined using the formula single population proportion by assuming a 5% degree of freedom and 95% confidence interval at alpha (α = .05) and the population proportion with a magnitude burnout was taken from a previous related study which is 47.6% (Holloway et al., 2007). The total sample size was 384. Since, the total population < 10,000, the finite population correction formula is used, and by adding a 10% non-response rate the final sample size was 253. All HCPs who were working in different departments, with working experience of > 6 months, and who were available during the data collection period and volunteered to participate in the study were included in the study, while healthcare professionals who were on vacation, sick leave, maternity leave, or away for professional training and are seriously ill, were excluded. A total number of 563 healthcare professionals (HCPs) are available in Dessie Comprehensive Specialized Hospital. Samples were taken proportionally distributed from each different department. To select the study unit from each group, we used a lottery method by using their record list at the human resource office of each category. After we had gotten their identification number from the office coordinators’ list document, we mixed numbers on a piece of paper, and then selected random numbers from mixed numbers via a lottery corresponding to a proportionally defined sample for each HCPs category (Table 1).
Sampling Procedure for the Prevalence of Burnout Syndrome and Associated Factors Among Health Care Professionals Working at DCSH, Ethiopia, 2021.
Data Collection Tools and Techniques
The burnout (BO) was assessed using the Maslach et al. Burnout Inventory-Human Service Survey (MBIHSS), which is widely used for measuring the burnout of healthcare professionals (Maslach et al., 1997). It is based on the Maslach Burnout Inventory (MBI), which was designed for human services professionals. The criteria proposed by Ramirez et al. (1996); Grunfeld et al. finding reliability values in the sub-scales, which permit observing that emotional fatigue is the strongest sub-scale (0.88), followed by personal fulfillment (0.81), and depersonalization (0.79).
The questions evaluate three independent dimensions, including emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA). The symptoms of EE include feeling of emotional overextension brought on by one’s job, DP includes emotional indifference and the dehumanization of service users, and PA includes feelings of occupational stagnation, incompetence, and underperformance. According to the MBI manual’s cut-offs, scores for each of the three subscales were classified as high, average, or low. It has 22 items with eight items for (EE), five items for (DP), and nine items for personal accomplishment (PA), that ask respondents to show the frequency of numerous feelings experienced. Each question was answered on a 7-point ranging from 0 (never) to 6 (every day). The sum of each dimension was obtained from the MBI scoring scale, and the results were classified according to values established by prior studies (Campos & Maroco, 2012; Moreira et al., 2009; Wall et al., 2014). The MBI-HSS was self-administered, which was reliable and valid. A high level of BO corresponded to high scores for the EE and DP dimensions and low scores for the PA dimension (Wang et al., 2015). To say having a burnout, if the participants scored ≥ 27 on Emotional Exhaustion (EE), ≥13 on Depersonalization (DP) sub-scales, and ≤ 31 on Personal Accomplishment (PA) sub-scale of the MBI-HSS (Haile et al., 2019). A prior study has shown that even when used in another language (Spanish) the tool made high sensitivity 92.2% and specificity 92.1% (Haile et al., 2019). This assessment is the most often used and recognized tool for evaluating the major BO symptoms. The internal consistency (Cronbach alpha) of (MBI-HSS) in this study was 0.82.
CAGE contains four questions that indicate the problems of alcohol use disorder. Each question has a yes or no response (0: “no,” 1: “yes”). The criterion for alcohol use disorder is defined by ≥ 2 positive responses to the CAGE (Alem et al., 1999). The simple mnemonic CAGE makes the four questions easy for a busy practitioner to recall. The CAGE questionnaire was first created verbally at a meeting in Australia in 1970, and Ewing and Rouse, who devised this tool, were both clinicians who also conducted research (Ewing & Rouse, 1970). It was developed before the Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised (DSM-III-R), which was published in 1987, made alcoholism’s official diagnosis more accurate (Association AP, 1987). The CAGE questionnaire for a cut-off of 2 had a sensitivity of 77% and a specificity of 94% (Malet et al., 2005). The internal consistency (Cronbach alpha) of (CAGE) in this study was 0.89. The current substance use (Use of substances like khat use, cigarettes, cannabis/ hashish, benzodiazepine, pethidine, and other substances) in the last 1 month. The determinants included in this study were, workplace violence including physical violence (physical and sexual assaults) and nonphysical violence (verbal abuse, threats, and sexual harassment) was recorded into (Yes/No); Job satisfaction was measured by asking the question, “Are you satisfied with your current job” with the following response choices: “1 = satisfactory; 2 = moderately satisfactory, and 3 = unsatisfactory.”
Study Variables
Dependent Variables
Burnout syndrome: Yes/No
Independent Variables
✓
✓
✓
Data Quality Control
The questionnaire was prepared in English first, then translated into Amharic, and finally back to English to ensure consistency. Three data collectors (all with a BSc in psychiatry) and one supervisor (MSc in psychiatry) received 2 days of training. The pre-test was conducted in the Dessie Health Center with 5% (n = 13) of the participants to identify potential problems with data collection instruments and to modify the questionnaire. The supervisor and investigator provided regular oversight and support to the data collectors. During the data collecting period, supervisors and investigators evaluated the data for completeness and consistency on a regular bases.
Data Processing and Analysis
Epi-Data version 3.1 was used to enter the data, and SPSS 26.0 was used to analyze it. The results were presented using tables, and the data were summarized using mean, standard deviation (SD), or percentage. The researchers used binary logistic regression analysis, both bivariable and multivariable. To adjust for probable confounding effects, explanatory variables with a p-value < .25 in the bivariable model were included in the multivariable regression model. Hosmer and Lemeshow goodness inspected the fitness model. All factors in the multivariable model with a p-value < .05 were considered statistically significant, and the strength of the association was represented by an odds ratio with a 95% confidence interval.
Result
Socio-Demographic Characteristics of the Participants
A total of 251 participants were involved in this study, making the overall response rate of 99.2%. Among the study participants, more than half (59%) were males and nearly half (47.0%) were married. The mean age of the participants was 29.43 years (standard deviation (SD) ±5.31 years). The majority of participants (46.6%) were nurses and (65.7%) were < 5 years service years of experience. Similarly, the mean monthly income of the participants was 5223.12, (SD ± 3865.68 ETB) (Table 2).
Socio-Demographic Characteristics of Respondents at Dessie Comprehensive Specialized Hospital (DCSH), Ethiopia, 2021.

Note. Others*:- Anesthesia, psychiatry, emergency nurse & radiography diploma. ETB = Ethiopian Birr
Work-Related Factors of Health Care Professionals
A substantial proportion of healthcare professionals (86.1%) have reported working >39 hr a week, (21.1%) on duty in their shift pattern and >one-third (38.2%) slept < 8 hr and 68 (27.1%) had one or more sick leave during the last year. Regarding violence history, (13.5%) had experienced physical violence, and (31.9%) had experienced non-physical violence. Of the participants, 16 (6.4%) had reported a history of mental illness, one-third (33.9%) had a worker’s intention to leave work, and 76 (30.3%) had no interest in owning a profession. One hundred seven (42.6%) of the participants worried about contracting an infections or illnesses. In terms of job satisfaction, (42.6%), (40.6%), and (16.7%) were satisfied, moderately satisfied, and unsatisfied with their job respectively (Table 3).
Work-Related Factors of Respondents at Dessie Comprehensive Specialized Hospital (DCSH), Ethiopia, 2021.

Lifestyle-Related Characteristics of the Participants
In terms of substance use, fewer than one-tenth had chewed khat (8% or n = 20), took pethidine (4% or n = 10, used benzodiazepine (2.8% or n = 7, smoked cigarettes (2% or n = 5), and used cannabis (hashish) (2% or n = 5) in the previous month before the survey study period. Among the study participants, 10.8% had AUD and 44.2% had regular exercise.
Prevalence of Burnout Syndrome Among HCPs
The overall prevalence of burnout syndrome among healthcare professionals was 15.1% (95% CI [10.8, 19.9]). The prevalence of emotional exhaustion, depersonalization, and, poor personal accomplishments in the study participants were 79(31.5%), 149(55.8%), and 211(84.1%) respectively (Table 4).
Prevalence of Burnout Syndrome Among HCPs Working in Dessie Comprehensive Specialized Hospital (DCSH), Ethiopia, 2021.

Factors Associated With Burnout Syndrome Among Healthcare Professionals
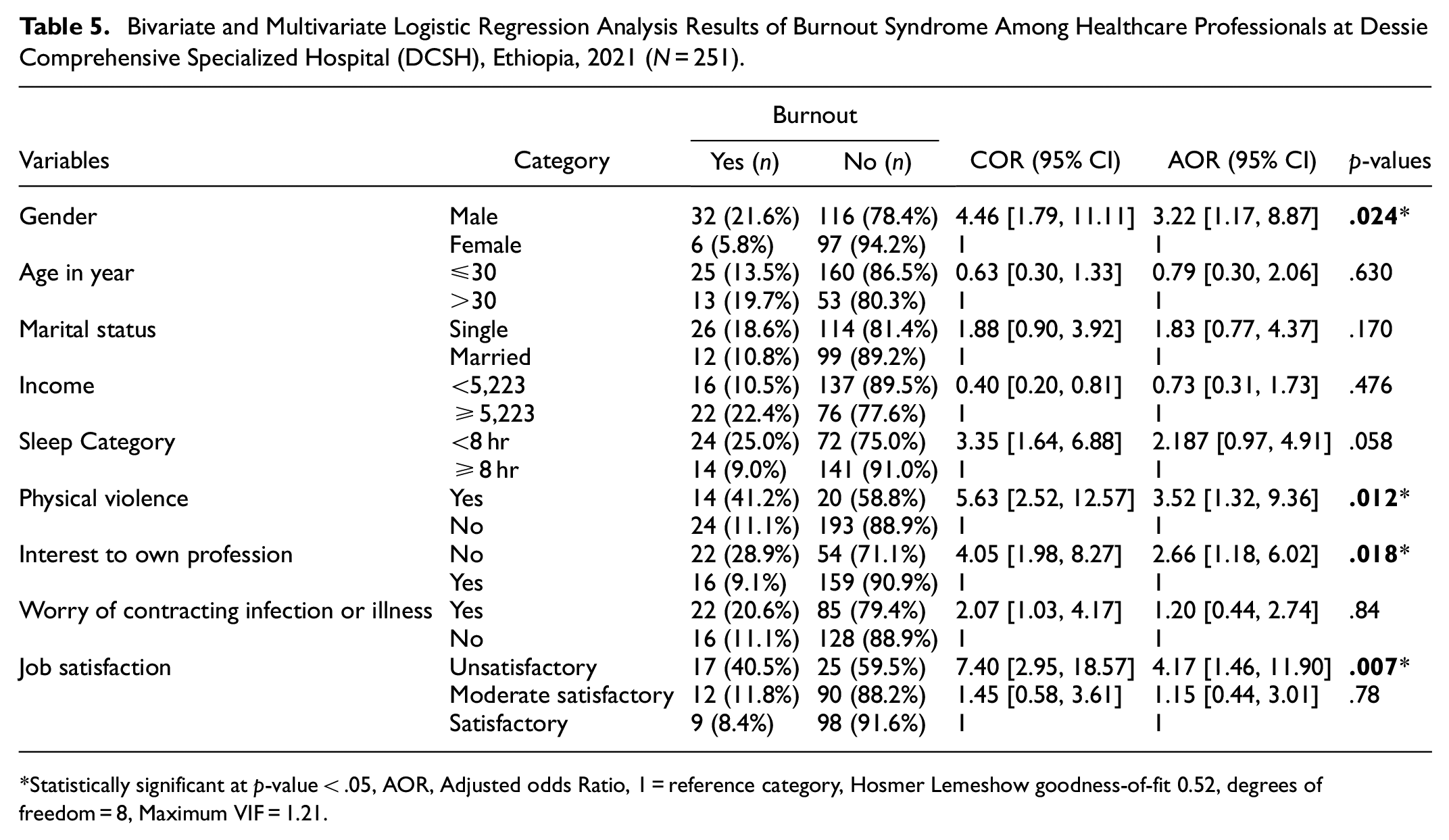
In the bivariate analysis: gender, age, marital status, income, poor sleep quality, physical violence, interest in own profession, worry of contracting infection, and work satisfaction were a candidate for multivariable analysis. In multivariable binary logistic regression variables; gender, physical violence, absence of interest to own profession, and job unsatisfactory were found to be statistically associated with burnout syndrome at a p-value < .05.
The odds of burnout among participants with a male were three times higher as compared to females (AOR = 3.22, 95% CI [1.17, 8.87]). Those experiencing physical violence were 3.52 times more likely to have burnout syndrome as compared with respondents who don’t experience physical violence (AOR = 3.52;95% CI [1.32, 9.36]). Similarly, those healthcare professionals who have no interest in their profession were about three times more likely to have burnout syndrome than their referent groups (AOR = 2.66:95% CI [1.84, 6.02]). Finally, the odds of burnout syndrome among HCPs who were not satisfied with their job was about 4.17 times higher as compared with the satisfaction with their job (AOR = 4.17:95% CI [1.46, 11.90]) (Table 5).
Bivariate and Multivariate Logistic Regression Analysis Results of Burnout Syndrome Among Healthcare Professionals at Dessie Comprehensive Specialized Hospital (DCSH), Ethiopia, 2021 (N = 251).
Discussion
The study showed that 15.1% (95% CI [10.8, 19.9]) of healthcare professionals at DCSH had symptoms of burnout syndrome. This finding on the magnitude of burnout is in line with the study conducted at Gondar University Hospital, Ethiopia which was 13.7% (Bhagavathula et al., 2018). In contrast, our result was lower than the prevalence report among healthcare professional workers in the Netherlands, France, Germany, Japan, China, Malawi, and Ethiopia, reporting burnout rates ranging from 20% to 83% (Biksegn et al., 2016; Dreher et al., 2019; Higuchi et al., 2016; Kim et al., 2019; Moukarzel et al., 2019; Prins et al., 2010; Qiao et al., 2016; Redae & Dai, 2019). The possible variation might be in the Netherlands, it was a national study conducted among 2115 resident doctors (Prins et al., 2010). In France, the study included 379 professionals working in the Emergency department (ED), who are more exposed to burnout syndrome due to extreme workload and high demands for care. Also, this variation might be due to the screening tool difference in which a previous study GHQ-12 was used in Japan (Higuchi et al., 2016), whereas Maslach Burnout Inventory Human Service Survey (MBI-HSS) was used in this study.
Another discrepancy in China, burnout was assessed among 501 HIV/AIDS healthcare workers, this is due to HIV/AIDS healthcare workers having an excessive workload, higher levels of stress, and worse working conditions because of the particularity of HIV, which includes infectivity, stigma, and discrimination than other health professionals staff. Furthermore, another possible reason for the variation may be relatively attributable to the respondent’s socio-demographic factors for example; age, gender, professional type, marital status, work-related factors: such as healthcare system, inadequate income, working time, career progression, and social support.
However, the current study is higher than the report from China in which the prevalence of burnout was 2.46% (Gan et al., 2019). A possible explanation for this variation might be the difference in the healthcare worker to patient ratio, which is the low ratio in Ethiopia and enhances the workload on HCPs. The differences may be due to focusing on a specific group of HCPs (general practitioners) in China and the nature of the healthcare system. In addition, other possible reasons could be socioeconomic variation across the study settings and the tools and sample size may contribute to this difference.
Regarding factors associated with burnout syndrome, in the current study; the odds of burnout among male participants were three times higher as compared to females. This finding is confirming the results of previous studies from Malawi (Kim et al., 2019), Brazil (Ebling & Carlotto, 2012), and Gondar University Hospital (Bhagavathula et al., 2018). The possible reason for this variation has been clarified by the differences in cultural beliefs and attitudes. In the healthcare scenario, the idea of a stronger or easier involvement of women with the care and well-being of others continuing to be more prevalent in males (Maslach & Jackson, 1985).
That health professional who was exposed to physical violence was 3.52 times more likely to experience a high degree of burnout as compared with respondents who don’t experience physical violence last year. Studies conducted by Palestinian (Hamdan & Hamra, 2017) and Jimma (Biksegn et al., 2016), which showed exposure to physical violence by teammates and patients was significantly associated with having a high degree of burnout. The possible clarification might be that exposure to trauma in physical, social, and psychological situations had bad implications that left people disgusted with their work and inept to have job-related satisfaction.
Similarly, another factor associated with burnout syndrome was the absence of interest in their job. Those healthcare professionals who do not have an interest in their profession were 2.66 times more likely to have burnout syndrome than their referent groups. This finding is supported by a study conducted in Jimma (Biksegn et al., 2016). The possible explanation might be due to high patient flow, low payment or/and imbalance between work demands and the capacity to cope with such demands and little interaction with their colleagues which can easy to feel demotivated and will cause for loss of pleasure in their job (Tsai & Liu, 2012).
Moreover, the odds of burnout syndrome among HCPs who were not satisfied with their job was about 4.17 times higher than compared those satisfied with their job. In our study, 42 (16.7%) of healthcare professionals were unsatisfied with their job. This finding and previous researchers have identified a negative correlation between job satisfaction and burnout syndrome. It is supported a survey from Brazil (Ebling & Carlotto, 2012), and two studies from China (Gan et al., 2019; Qiao et al., 2016). It suggests that low in job satisfaction could serve as a less effective way to prevent or minimize burnout, and provides new insights for future studies on ways to improve the job satisfaction of HCPs and indirectly address burnout syndromes (Gan et al., 2019).
Limitations
The temporality and causality of the observed associations could not be assessed because of the cross-sectional study methodology. This is why we recommended longitudinal studies should be conducted to confirm the present conclusions. Recall bias was unavoidable because data were collected from participants’ self-reports. Due to job satisfaction being assessed using a single question, future researchers it is better to use a standard tool assessment for investigating job satisfaction. Finally, because the study was limited to DCSH, the results may not be generalizable to other populations. However, we attempted to mitigate the effect by clearly stating the study’s goal and value to the participants, as well as employing a standardized questionnaire to assess BS, including from all fields of healthcare professionals, could be taken as a strength of the study.
Conclusions
Burnout syndrome (BS) is a significant problem among healthcare professionals working in Dessie Comprehensive Specialized Hospital. Being male, loss of interest in their job, physical violence, and job dissatisfaction were significant determinant factors of burnout syndrome. To alleviate public health problem, interventions concentrating on building a stress management program, as well as strengthening interpersonal relationships and working circumstances to promote job satisfaction among HCPs, are critical. Also, Administrators could also account for the value of personality profiling, in order to allocate resources to prevent burnout among healthcare workers in valuable personality traits.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to the Participants
The researcher obtained ethical clearance from the Ethical Review Board. Moreover, we strived to protect and respect the privacy, secrecy, and well-being of participants under these conditions. All collected data were used for this study only. The respondents were informed about the aim of the study from the study participants before the data collection. Confidentiality and privacy of the respondents were maintained. Written informed consent was obtained from all participants. Those who did not want to take part in the study were allowed not to participate or to withdraw from the study at any time they want.
Consent for Publication
Not applicable
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.