
Abstract
This article presents findings from a grounded theory study, which investigated interactions between health professionals and consumers. The authors used Corbin and Strauss’s evolved version of grounded theory, which is underpinned by symbolic interactionism. The study sample included 23 consumers and nine health professionals. Data collection methods included demographic questionnaires, interviews, consumer diaries, digital storytelling, observations, and field notes. Data analysis was conducted using essential grounded theory methods. The resultant grounded theory consists of five categories: (a) Unexpected entrance, (b) Learning a new role, (c) Establishing a presence, (d) Confronting the dichotomy of “us and them,” and (e) Tailored care. Findings suggest that despite consumers and health professionals’ roles, consumers are outsiders in the social world of health care. Progress toward empowered consumers who are in control of their health and health care is slow and care that is truly consumer-centered is still the exception not the rule.
Introduction
Until the 1970s, a biomedical model of health predominated in Western health care systems. This model prioritized the impact of illness on the human body, over consumers’ experience of care. The introduction of Engel’s (1977) biopsychosocial model of health care in 1977 shifted the culture of health care to include consumers’ psychological and social contexts being considered in conjunction with their illness during treatment. As this cultural shift continued to evolve, the relationship between consumers and health professionals developed greater equality, and consumers’ rights to self-determination and autonomy were recognized (Deber et al., 2005; Will, 2011).
This cultural evolution has led to the concept and terminology of patient-centered care (also referred to as consumer-centered care or person-centered care) becoming mainstream. Although the concept of patient-centered care was introduced in the mid-1950s (Balint, 1969; de Haes, 2006; Groene, 2011), it did not gain traction until the release of a landmark report in the United States, titled Crossing the Quality Chasm (Committee on Quality of Health Care in America, 2001). The report names patient-centered care as one of six key improvements required in the U.S. health care system. In addition, the report provides the first definition of patient-centered care as “care that is respectful of and responsive to individual patient preferences, needs and values” (Committee on Quality of Health Care in America, 2001, p. 6). Around the same time, other definitions of patient-centered care took into account individuals’ “desire for information, sharing decision making and [experts] responding appropriately” (Stewart, 2001, p. 445). The Australian Commission on Safety and Quality in Health Care (ACSQHC, 2012) later extended the definition to include health professionals forming partnerships with consumers, their families and carers.
Despite models of health care shifting away from an illness focus, to the inclusion of consumers’ biopsychosocial contexts and more recently, to consumers being central to decisions about their health care, the representation of consumers as patients in the literature often categorizes people according to their illness or contextualizes them within specific health settings (see Ferri et al., 2015; Lammers & Happell, 2003; Mathur et al., 2013; Tobin et al., 2002). Interactions between consumers and health professionals are central to delivering health care that is patient- or consumer-centered. Yet research often focuses on interactions with specific health professionals only (Jangland et al., 2011; Stenhouse, 2011) or addresses interactions from methodological or conceptual perspectives (see Cahill et al., 2008; Drew et al., 2001; Sofaer & Firminger, 2005).
Consumer-centered care requires affected people to share power and responsibility for their health and health care with health professionals (Gluyas, 2015; Mead & Bower, 2000). Supporting people to become more involved in their own health and health care requires insight into their perceptions of interactions with health professionals. The aim of this study was to identify and explain processes of interaction between consumers and health professionals that are not bound by specific health professions, health settings, or health conditions (Chamberlain-Salaun, 2015). Gaining consumers’ insights and identifying and explaining processes of interactions between consumers and health professionals has the potential to inform the development of strategies to improve consumers’ health care experiences and their health outcomes.
Study Design
Method
Grounded theory is both a research design and a product. The researchers used Corbin and Strauss’s evolved version of grounded theory, which is underpinned by symbolic interactionism, as the methodological lens through which to conduct the study. A more detailed account of links between grounded theory methods and symbolic interactionism and the application of the former in light of the latter are presented in an earlier publication (Chamberlain-Salaun et al., 2013). Grounded theory provides a comprehensive and integrated approach for identifying dominant processes within an area of inquiry, with the aim of developing a theory that explains what is actually going on rather than “what should, could, or ought to be” going on (Glaser, 1999, p. 840).
Grounded theory research does not commence from the premise of a priori theories. Rather, the researcher begins with an area of inquiry, which is broad enough to allow the flexible application of essential grounded theory methods to guide the collection, generation, and analysis of data to construct a theory (Charmaz, 2014). The area of inquiry of the study reported in this article is the process of interaction between consumers and health professionals. The resultant product of a grounded theory research study is a theory that is recognizable to people familiar with internal processes relating to the area of inquiry (Hunter et al., 2011). The grounded theory Outsiders in the experts’ world incorporates five dominant processes: (a) Unexpected entrance, (b) Learning a new role, (c) Establishing a presence, (d) Confronting the dichotomy of “us and them,” and (e) Tailored care (Chamberlain-Salaun, 2015).
Definitions
In the context of the study and this publication, the authors use the terms consumer to define a person who accesses health service for their own care or on behalf of someone for whom they care. The use of the term consumer avoids the passive overtones of the term “patient” and acknowledges that consumers are actual or potential users of health care services (ACSQHC, 2011b). The use of the term experts in this publication refers to all health professionals. It was an in vivo term used by consumer study participants to acknowledge the expertise of health professionals.
Sample
A total of 32 participants from one Australian regional city were recruited to and participated in the study. The sample included 23 consumers (14 females and nine males) and nine health professionals (eight females and one male). Methods included purposive, theoretical, and snowball sampling (Birks & Mills, 2015). Generation and analysis of data from an initial purposive sample of consumers guided theoretical sampling of additional participants in an iterative process. Theoretically, sampling health experts resulted in snowball sampling of additional consumer participants. Similarly, the purposive sampling of consumers directed the sampling of additional health expert study participants. Consumers were eligible to participate in the study if they were 18 years of age and above and interacted with a range of health professionals. Experts from any health discipline were eligible for inclusion in the study.
Data Generation and Collection
Data were generated and/or collected (Birks & Mills, 2015) via demographic questionnaires, interviews, consumer diaries, digital storytelling, observations, and field notes. Data generation refers to the process of generating data with participants via methods such as interviews. Data collection refers to collecting artifacts from participants or from other sources such as participants’ diaries, questionnaires, or digital stories. Table 1 presents an overview of the types of data generated and/or collected, the number of participants involved, and the quantity of data produced.
Data Generation/Collection Method and Quantity of Data by Participant Type.

Data Analysis
Data were analyzed using essential grounded theory methods as ascribed by Birks and Mills (2015). The methods are initial coding, concurrent data generation or collection and analysis, constant comparative analysis, intermediate coding, theoretical sampling, selecting a core category, advanced coding and theoretical integration, and writing memos and theoretical sensitivity.
Initial coding is the first step of the data analysis process. In this phase, data were scrutinized in units and labeled with codes. Concurrent generation or collection and analysis of data are “interrelated processes” (Corbin & Strauss, 1990, p. 419; italics in original) that underlay the operation of grounded theory (Glaser & Strauss, 1967). Using this method, each round of generated or collected data in the study was analyzed before the next round of data generation or collection commenced. The constant comparative analysis method uses inductive reasoning to extrapolate patterns across individual data units to form conceptual categories (Bryant & Charmaz, 2007), whereas abductive reasoning “bring together things which one had never associated with one another [in] a cognitive logic of discovery” (Reichertz, 2010, para 16). Using constant comparative analysis, intermediate codes were identified. During the intermediate coding process, the researcher moves iteratively between initial and intermediate coding to connect codes and categories into more conceptual-level categories.
Theoretical sampling is a method unique to grounded theory. The distinguishing characteristic of theoretical sampling is that it is an iterative process whereby future data collection is guided by concepts derived from analysis of data from the previous round of data collection or generation (Corbin & Strauss, 2008; Glaser, 1978; Glaser & Strauss, 1967). Theoretical sampling determines, where, how, and from whom to collect or gather further data to elaborate and refine categories in a developing theory (Birks & Mills, 2011; Charmaz, 2014).
A core category is the overarching category that links all the categories of a grounded theory; it reassembles the parts into a whole (Birks & Mills, 2011; Corbin & Strauss, 2008). Corbin and Strauss (2008) use the metaphor of an umbrella to explain the concept of the core category. The categories, or concepts, of a grounded theory resemble the umbrella’s spokes. Without the material covering the spokes, the spokes are just spokes and are of little use. The material links the spokes and gives the object form and use; it becomes an umbrella. Researchers can be assisted in identifying a core category by asking themselves how they would conceptualize their findings in a succinct way (Corbin & Strauss, 1990). A core category is central to the integration of a grounded theory because it encapsulates and connects all the components of a theory (Strauss & Corbin, 1990).
Theoretical integration of a grounded theory conceptually brings together the elements of the grounded theory process into a theory that explains phenomena (Strauss & Corbin, 1994). In this study, the use of the advanced coding technique of storyline (Corbin & Strauss, 1990; italics in original) enabled the integration of the grounded theory.
Theoretical sensitivity and writing memos are also key components of a grounded theory process. Theoretical sensitivity is a researcher’s ability to recognize nuances in the data, to extract data elements relevant to the developing theory and to reconstruct meaning from data generated with participants (Corbin & Strauss, 2008; Mills et al., 2006; Strauss & Corbin, 1990). Theoretical sensitivity is influenced by a researcher’s “personal and temperamental bent” (Glaser & Strauss, 1967, p. 46), their intellectual history, and their personal and professional experiences (Strauss & Corbin, 1990). Throughout the study, the writing of theoretical, analytical, and conceptual memos (Glaser, 2004; Thornberg & Charmaz, 2011) lubricates the cogs of the ground theory research process from the planning phase through to the end of a study (Birks & Mills, 2011).
Ethics
Ethical considerations were adhered to in accordance with the Australian National Statement on Ethical Conduct in Human Research 2007 (The National Health and Medical Research Council et al., 2014). The research study received ethics approval from the Cairns and Hinterland Human Research Ethics Committee (HREC) and the James Cook University HREC. All study participants were given a Study Information Sheet and provided written consent prior to participating in the study (Chamberlain-Salaun, 2015).
Findings
The grounded theory Outsiders in the experts’ world presents what happens when people enter the social world of health care and take on a consumer role and how processes of interactions between consumers and experts are enacted. The contingent relationship between what and how (Charmaz, 2014) addresses the question, “why are consumers outsiders in the experts” world? Regardless of the key roles of consumers and experts in the social world of health care, findings in this study suggest that consumers are outsiders in a world dominated by experts who drive the machinations of the social world of health care.
The grounded theory consists of five categories and their subcategories (Figure 1): (a) Unexpected entrance (Emotional fluctuations, Changing perceptions of self), (b) Learning a new role (Acquiring knowledge, Learning the language of health care, Confronting mortality, and Cultivating support), (c) Establishing a presence (Gaining confidence, Choosing a voice, and Establishing relationships, (d) Confronting the dichotomy of “us and them,” (e) Tailored care (Listening and acting; and Accessing experts). Each category is discussed in detail below and representative participant quotes are used to exemplify findings. Quotes are coded as participant (P) and artifact (A) number.
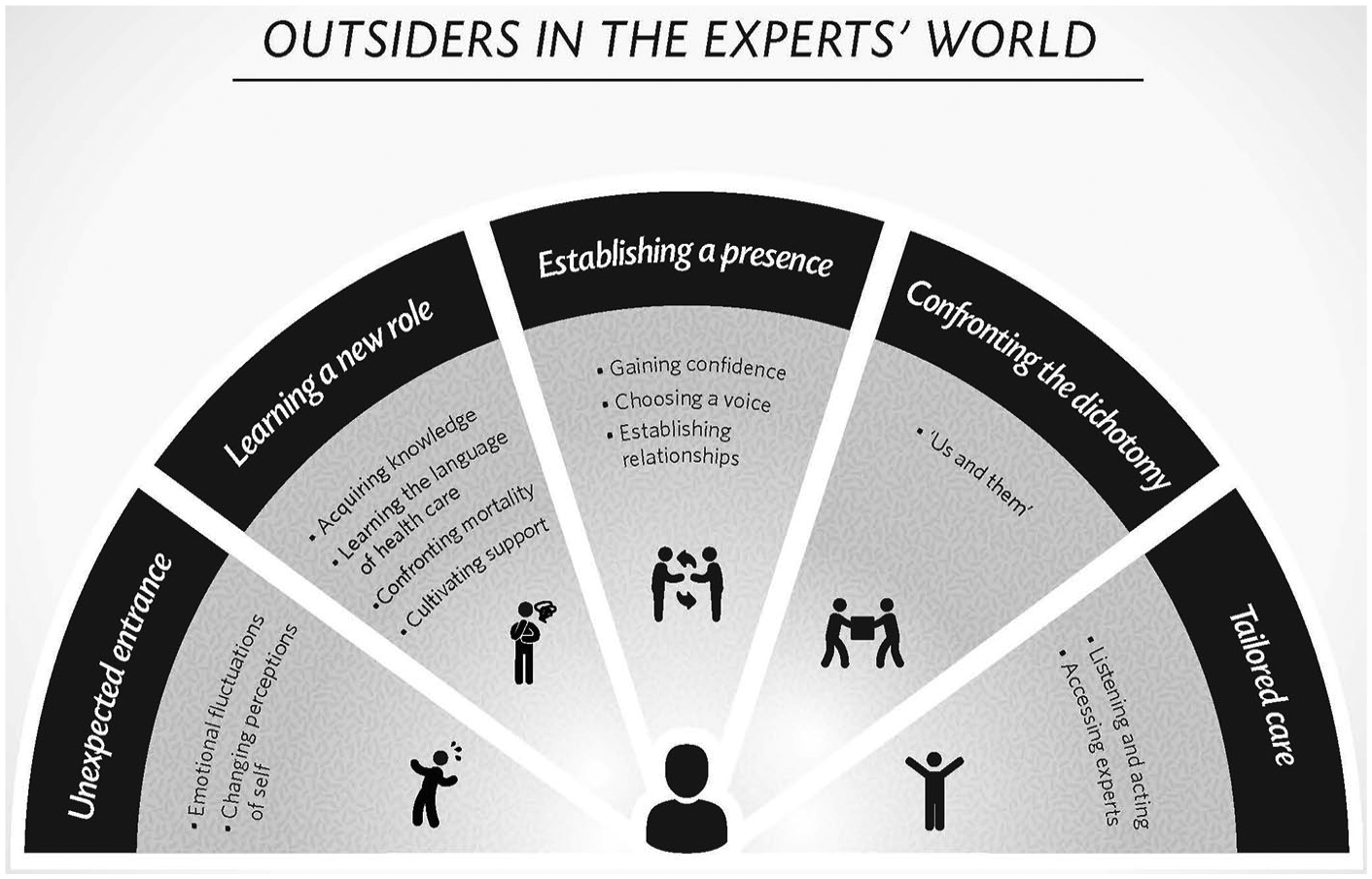
Grounded theory model of outsiders in the experts’ world.
Unexpected Entrance
People make unexpected entrances into the social world of health care and become consumers as a result of illness or injury. Illness can be either a diagnosed condition or a range of persistent symptoms that affect a person’s health and well-being but defy diagnosis. Becoming a health care consumer can also be experienced vicariously by those who are responsible for providing care or support to someone else experiencing illness or injury. Unexpected entrances are fraught with emotional fluctuations and changing perceptions of self that mark the beginning of “another chapter” (P5A26) in a person’s life.
Unexpected entrances into the social world of health care cause emotional fluctuations that exceed everyday emotional experiences. Before entering the social world of health care, people cannot imagine what it is like to wake up in hospital with a tube hanging out of [their] throat, looking at a ceiling and this nurse leaning over just saying, “Relax” [ . . . ] It is very scary to wake up like that, not moving, not knowing what’s going on. (P5A26)
The following consumer had not seen the inside of a hospital for 30 years before experiencing chest pain at home in the middle of the night and being taken to hospital by ambulance: I didn’t know what to expect and all the rest of it. You know what I mean. If you go there because you cut yourself open and you need stitches, then you know what’s going to happen. (P4A13)
Four hours later, this same participant was diagnosed with leukemia. His feelings of disbelief were emphasized in his retelling of the event. “I said to the doctor ‘it must be wrong, you’ve made a mistake with somebody’s blood, it’s not mine. I’m a regular blood donor, I just gave blood six weeks ago. Surely it would have been picked up then’” (P4A13).
Consumers with persistent but undiagnosed symptoms similarly experience the emotional fluctuations experienced by consumers who have received a diagnosis. They feel frustrated, isolated, and impatient; frustrated because they do not have a label to attach to their symptoms and isolated because they do not receive the same level of support and understanding from others that a diagnosis often attracts.
After the initial emotional fluctuations of an unexpected entrance, peoples’ perceptions of “self” change. Perceptions of both the internal self and the physical self are intertwined with how consumers perceive themself, how others perceive them, and how they think others perceive them. After being in hospital for extended periods of time, consumers are faced with the challenge of learning to reconnect with their previous perceptions of self and to trust themselves again. One consumer related the experience of returning home after 9 weeks in hospital. His wife was at work all day, so he was home alone: All of a sudden I was at home alone. It made no sense, because I was well or reasonably well, and I could look after myself. I could make myself tea and coffee and have lunch and all the rest of it. But it was just the fact that there was nobody here, when you’re used to having, you know, all the ward staff there at your call. (P4A13)
The consumer’s recount of his internal dialogue provides insight into his attempts to bring some perspective to the situation. I told myself, “stop being a bloody idiot and get on with it. What are you concerned about? You’re well” (P4A13).
The changed physical self of another consumer, who is in a wheelchair as a result of an accident, led him to think about his body in new ways. Without the sensory perception of his body from the stomach down, his diet and weight have become priorities for maintaining health because “you can’t tell when your belly’s full” (P5A26) and weight gain can lead to health complications.
Dichotomies between how consumers perceive themselves and how others see them are not uncommon. One participant related how an expert referred to her condition as “a significant physical disformity [sic]” (P7A32). This was in stark contrast to the way in which the consumer perceived her physical condition. She explained that she did not consider her condition to be “that bad” nor did she perceive herself as someone who “looked funny or walked funny” (P7A32).
Learning a New Role
The role of a health consumer is largely undefined. Similar to other undefined roles in life—parent, spouse, sibling—the consumer role is learned and refined through experience. Learning the role of consumer incorporates acquiring knowledge, learning the language of health care, confronting mortality, and cultivating support.
Consumers acquire knowledge through their sensemaking of information and through the experience of living with a health condition. They access information from a range of sources including experts, the Internet, and from members of their social networks. One consumer explained how she used the printed information about migraines, which her pharmacist provided, as a basis for collecting further information via the internet. The consumer then used her newfound knowledge of migraines and treatment options as a starting point for discussions with her general practitioner. Consumers use the internet in varying degrees to search for general health information, treatment and medication options, and for self-medicating via online medication purchases. Some consumers are more wary of this source of knowledge than others and approach with caution, recognizing that “there’s no guarantee of quality on the Internet” (P3A10).
Consumers who care for someone with a health condition acquire knowledge about their role through the experience of representing and advocating for another. These consumers explained how their experiences influence their interactions with experts. A mother explained that prior to giving birth her approach with doctors was “to tell them what the problem was, listen to what they’d say and not really enter into a discussion” (P11A46). Since becoming a parent, the consumer acknowledged that she no longer “just takes the doctor’s word” (P11A46). She attributed her increased assertiveness to a combination of knowledge gained over time, having a long-term relationship with her general practitioner and “just growing older” (P11A46).
To understand what is happening to them and around them, consumers must learn the language of health care, which includes new words and their meanings. Consumers also assign their own meanings to previously known words, and these meanings may change over time. For one study participant (P4A13), the word leukemia meant, “you’re dead” when he was diagnosed. His construction of meaning was based on what he had seen on television. Following initial discussions with his doctor, the meaning of the word leukemia morphed into “the fight of your life” and then as he met and heard stories from other patients living with leukemia, the word came to mean “remission” and the possibility of a fulfilling life.
Humor, as a component of language, is often used in consumer–expert interactions. Factors which influence when and how humor is used include the relationship between consumers and experts, how consumers are feeling on a particular day, and the point at which consumers are on the spectrum of their condition. An expert’s comment highlights how the use of humor changes as consumers adapt to their diagnosis, “a positive outcome diagnosis [is] not a joking matter [but] once [consumers] have got used to their diagnosis they’ll come in and have a joke with the staff” (P20A58). Similarly, a consumer who has a chronic condition recounted a frequent exchange that he has with one of his health experts: “Almost every time I see him, I walk in and he says, ‘So how are you?’ and I say, ‘I’m not dead yet’ and he says, ‘There’s a bonus we weren’t expecting’” (P4A13).
When the role of being a consumer is associated with a life-threatening or life-limiting illness, consumers are acutely confronted with their own mortality. Some consumers accept that the inevitability of dying is part of living and they acknowledge that this makes “the burden [of illness] easier to carry” (P8A27). Consumers who accept their mortality are more likely to speak openly about death, not to mask their fear of death but to “lighten” life. A general practitioner study participant recounted how one of her patient’s acceptance and openness about illness and death guided frank discussions between them (P22A60). The same participant added that speaking openly about death removes the proverbial elephant in the room and alleviates the “need for euphemisms” (P22A60).
Cultivating support includes consumers accepting unrequested support when it is offered and requesting support when it is needed. Family, friends, and social networks are sources of practical, financial, and emotional support. Consumer participants recounted instances of receiving overwhelming support, as the following interview excerpt highlights: My friend from church has been mowing my lawn and trimming my edges and cutting my trees since [I got sick]. He has never accepted any payment for it. He has just—he just took it on himself that that’s what he was going to do. [ . . . ] people would come over with home-cooked meals so that we didn’t have to do it, and yes, there was just so much support. When we got into financial problems, they whipped the hat around at church and came up with literally thousands of dollars over the last four years to help us out. (P4A13)
Consumers living with mental illness, or who are parents or carers of people living with mental illness, are often isolated in their journey prior to seeking professional support. For these consumers, seeking support from health professionals is often a “cry for help,” which is not always heard or does not meet their expectations. A consumer who participated in the digital storytelling workshop titled her story Invisible (P17A53). The digital story speaks directly to health professionals and tells the story of her family’s struggle of living with the “nightmare” of her son’s mental illness. The story opens with images of family photos, an eerily haunting soundtrack and the participant’s voice; “Invisible. Do you see us? Do you hear us? Do you know us?” (P17A53). Rather than meeting the family’s cry for help, seeking professional support amplified the family’s struggle. They felt even more isolated as they searched for health professionals “with heart and soul” (P17A53) and more often than not were unable to access this level of care.
Establishing a Presence
As consumers learn their, role they establish their presence in the social world of health care. To establish their presence, consumers must first gain confidence and choose a “voice.” Confident consumers assert their presence and provide feedback directly to experts. In choosing a voice, consumers make decisions about how they will interact with experts. The “voice” that a consumer chooses may be the result of their increased confidence, the influence of their individual personality, or it may reflect where they are on the spectrum of their illness or condition.
It is challenging for consumers to gain confidence in their interactions with experts when experts exclude them from discussions or when consumers perceive that their inclusion in discussions is tokenistic. The following comment reflects a consumer’s perceptions of mental health experts as noninclusive: “You see what you want to see, hear what you want to hear and know what you want to know” (P17A56). Over time, the lived experience of illness enables consumers to gain confidence. A participant who had been a consumer for about 4 years at the time of interview had spent numerous extended periods in hospital. His recount of a scenario demonstrates the ways in which confident consumers can change the course of interactions with experts: he [the registrar] would ask me a question and I would begin to answer, and only halfway through, he would talk over the top of me. I let him go, and he did that [for] probably six or seven minutes. This was in the ward, yes. Like, there was him and—because there’s usually a group of between three and five of them. Yes, there was him and two or three others, I forget how many. But he was doing all the talking. Eventually, I pulled it up and I said, “Listen, do you want to hear what I’ve got to say, or don’t you?” I said, “Are you actually interested?” He said, “What do you mean?” I told him. I said, “You asked me a question, I start to talk, and then you talk over the top of me. Now, do you really want to know, or don’t you?” I said, “Because if you’re just going to talk over the top of me and not bother listening to what I’ve got to say anyway, then I don’t want you treating me.” Actually, he was—he really changed his attitude after that. (P4A13)
To be heard, consumers have to find their voice and use it. Consumers use a range of “voices” or approaches when interacting with experts, including a “squeaky wheel gets more oil” approach, a warrior approach or a gentle, patient approach. Some consumers use “a squeaky wheel gets more oil” (P11A46) approach as their mantra. One consumer explained, “say what you need, what you think you need [because] no one’s going to come looking to help” (P11A46). The participant explained that before coming to this realization she would answer “I’m fine” (P11A46) anytime an expert asked her how she was feeling.
Using the “squeaky wheel” approach does not always produce desired results; external factors also influence outcomes. A consumer’s digital story tells of his experience of arriving at a hospital emergency department (ED) with severe back pain. The consumer used a “squeaky wheel” approach and repeatedly asked to have an ultrasound or an MRI (magnetic resonance imaging) so that the underlying cause of his pain could be ascertained and he could be given appropriate treatment. His requests were refused without explanation.
Taking a “warrior” approach is familiar to consumers who are carers. As carers for others, they “fight” for those who cannot advocate for themselves. In the digital story titled Invisible (P17A53), a consumer included an image of two dinosaurs fighting and the spoken words, “Then we came to you. Then we must become warriors” (P17A53). The image and the consumer’s words, symbolize the constant battle that carers face when they interact with the health system and experts.
Consumers with life-threatening health conditions tend to choose a gentle, patient approach in their interactions with experts. During interviews and observation, these consumers spoke with, and demonstrated, humility and patience in relation to their interactions with experts. One consumer explained, Attitude is everything. I’ve seen people in there who really treated the staff with disdain, you know, because they wanted attention and they wanted it now. Whereas, I was always patient, knowing that there’s more people in there than just me and some of them are in a worse condition than me. (P4A13)
Relationships between consumers and experts are often established over long periods of time. Of all the relationships that consumers have with experts, their relationship with their general practitioner is the most intimate. Consumers spoke about the changes in their lives that their general practitioner had seen them through: relationship break-ups, depression, the lowest point in their illness, and being close to death. Regardless of the experiences that consumers share with their experts, professional boundaries are maintained.
Sometimes experts will relax professional boundaries. For example, they may make exceptions in the last stages of a consumer’s life. In this situation, general practitioners might give their personal telephone number to a consumer, but not before considering “what [they] are willing to do for that person. Like go and visiting them at the drop of a hat” (P22A60).
Within doctors’ surgeries, power differences between consumers and general practitioners or medical specialists are less pronounced than in the hospital setting. The consultation space in doctors’ surgeries is generally limited to one-on-one interactions, except in instances where consumers are accompanied by a carer or family member. The duration of the professional relationship between a consumer and their doctor influences the structure of their relationship. The longer a “patient–doctor” relationship has been established, the more relaxed interactions are likely to be. In this scenario, the consumer is in a position of greater power than the patient in the hospital bed and is therefore more likely to establish their presence. In a doctor’s surgery, the consumer influences, to some degree, when an encounter will occur as they have usually initiated the appointment. The extent to which consumers maintain control of an encounter depends on how the situation unfolds and how each actor responds to the other.
Confronting the Dichotomy of “us and them”
The social world of health care dichotomizes consumers (us) and experts (them). In health care settings, the dichotomy of “us and them” is characterized spatially, physically and through the asymmetrical relationship between consumers and experts. The asymmetrical relationship is supported by social structural elements such as culture, systems, and decision-making powers engendered by consumers’ and experts’ roles. Some consumers and experts confront the dichotomy of “us and them” as they would in a battlefield in which a victor must emerge. These actors do not transcend social structural elements but wield them as weapons. Other consumers and experts are willing to transcend structural dichotomies of “us and them” to create and negotiate reciprocal interactions that meet each other’s needs and expectations.
Health care settings are spatially dichotomized into consumer spaces and experts’ spaces, although sometimes the two overlap. Consumers are generally spatially confined to hospital wards and hospital and medical practice waiting areas. Spaces designated for experts include offices and hospital ward stations. Consulting rooms and operating theaters are designated spaces into which experts invite consumers to enter.
The physical positioning of experts during interactions with consumers often represents a reality of the division between the two groups. In hospital settings, experts often stand above consumers who are laying or sitting in hospital beds. The asymmetrical positioning of consumers and experts in these scenes perpetuates a dichotomy of “us and them.” Although in hospital and private practice consulting rooms consumers and experts are physically positioned at eye-level, the expert’s desk and professional workspace are a physical cue of the dichotomy of “us and them.”
Consumers appreciate experts’ attempts to break down common spatial and physical barriers. A consumer, who has a child with disabilities, emotionally recounted the following scene, which she observed between a medical specialist and her son: He [the doctor] made him sit on the bench so he could see him eye to eye, and explained everything. He wouldn’t even look at me, and I thought, this is great. He called him by name, and explained everything to him as a seven-year-old and he [my son] took it all in, you know. As a mother of a child with a disability, it just—it meant so much to me, you know, that someone would take the time. (P1A3)
Tailored Care
Tailoring care to meet individual consumer needs is a process—“a consultative thing” (P4A13)—in which consumers and experts listen to each other and act. Access to experts they know and trust also influences consumers’ receiving tailored care. Consumers feel valued within the expert–consumer relationship when experts listen and act: All I said to the first doctor was that I have a lot of difficulty with everyone being around me when I don’t have any control. I’d no sooner said it than sort of extraneous people were moved away. So, he heard every word that I said, and put the appropriate amount of action. (P8A27)
Tailoring care to meet consumers’ emotional needs is also important. An excerpt from a consumer interview provides insight into ways in which consumers and experts collaborate to ensure that consumers receive tailored care that meets their emotional needs. This consumer has a chronic life-threatening illness. Together, he and his general practitioner have constructed a scenario that they will play out when the consumer reaches a point where he wants to “give up” (A27r105): We have a code now. So I told him, “Well, when I get to the point—to that stage again, I’ll just tell you that I’m ready for a short trip to Switzerland.” He says, “Is there anything that I can do to help that I’m not doing?” I said, “Yes. When I come in and I look really bad—no matter what—I want you to tell me how well I’m doing. I promise you that I’m going to pretend that I believe you.” (A27r107)
When consumers feel that experts do not listen and therefore do not tailor their care, consumers’ needs are either not met or are not met in a timely manner. One consumer’s digital story includes an image of males in “slave gangs” followed by an image of the Australian Indigenous flag. The images are accompanied by the consumer’s voice over that refers to experts “not listening because they don’t have to” (P13A49). The symbolism of the images links the consumer’s cultural identity to concepts of oppression and exclusion, which are expressed in the consumer’s spoken words.
Consumers also revealed that sometimes experts hear and listen but do not act. During open discussions in the digital storytelling workshop, one consumer related to the group how experts on a hospital ward listened to him “crying, turning and screaming in pain” (P15A56) without acting.
The process of tailoring care also requires consumers to listen to and to act on experts’ advice. One consumer related a story of how when he was on holidays interstate, he needed to present to the ED of a public hospital. On arrival at the ED “the triage nurse was on the phone and the computer at the same time and said ‘Just take a seat, I’ll be with you in a few minutes’” (P8A41). The consumer then recalled previous advice given to him upon discharge from a hospital in his home city. The discharge doctor had advised, The next time you get sick, if you’re not here when that happens, you need to emphatically tell them how unwell you are, because you never look it. So those words came back to me when I was in Melbourne, and so I didn’t go and sit down. I just stood there for a few moments, and she [the triage nurse] was trying to get a bloody application to work on her computer, and that’s what was more important than triage. So, I finally said to her, when she stopped talking to the IT person—I said, “I’m 57 years old, I’ve had chest pain for 16 hours, and my pulse is so erratic I can’t count it.” So she finally looked up and said, “Just a minute,” and came rushing around and got a wheelchair. By the time my friend parked the car, you know, and got in, I was already in the resuscitation room and they had lines put in, and they already had defibrillated the first time by the time he came in. So, that’s how serious it was. Like, my pulse was hitting 250. So—so now I know to tell people. (P8A41)
Access to experts when consumers need it and to experts that consumers know and trust contributes to consumers receiving tailored care. Prompt access to experts is often limited to consumers whose condition requires immediate attention or who are in the final stages of life: Because of my condition, [the doctor is] very accessible. If I have any concerns at all, I can ring him. Usually, obviously, he’s not the one that answers the phone, and I tell the nurse or the receptionist, whichever one answers the phone [ . . . ] and he usually calls back within one to two hours at the most. (P4A13)
Another consumer, who was caring for a family member who was in the final stages of life, explained in her digital story how “the specialist had given me all of his contact numbers and I’m allowed to ring 24/7 if needed” (P16A52).
Access to experts is not always so readily available for other consumers. During consumers’ open discussions in the digital storytelling workshop, two participants, who are both mothers of adult children with mental illness, explained how they were excluded from participating in any aspect of their children’s care. It was unclear, from the conversation, what the mothers’ legal status was in relation to accessing information or being involved in their children’s care. Nonetheless, both mothers expressed concern for their children and were upset and angry that “the system took them [their adult children] away” (P17A56).
These consumers have no way of knowing whether their children are receiving tailored care and they are excluded from contributing in any way to their child’s care. One of the mothers described how she had asked for and needed help from experts when her son was admitted to the hospital psychiatric unit. “Nobody ever phoned me, nobody ever returned my calls” (P17A56). For this consumer, accessing an expert who had “passion, professionalism [and] intelligence” was important and akin to “finding a friend” (P17A56). The other mother explained that experts had told her, “we can control our patients better without the family around” (P17A56).
Accessing experts close to their home and in settings familiar to consumers supports tailored care. Sometimes consumers have to travel from regional or remote areas to capital cities or larger regional hospitals to receive care. Being away from family and support networks is isolating. Consumers prefer the familiarity of smaller regional hospital facilities, which they believe foster more personalized care: I can remember going into the ED one day and just walked through the door—and that’s all I did, was just walk through the door—and the girl behind the counter said, “Hi [consumer’s name], come on straight through.” It made it all bearable, for a start. It made me confident that I wasn’t just a number, I was being treated as a person. It made me glad that I was being treated in [ . . . a regional town], and not in a capital city where possibly I may have been just a number. Yes, as I said earlier, it made a really bad situation feel a lot better. (P4A13)
Discussion
Regardless of whether a consumer’s unexpected entrance is the result of an accident, a diagnosis, or being a carer of someone who has experienced either, consumers experience all stages of the grounded theory Outsiders in the experts’ world. Although consumers generally move sequentially through the stages of the grounded theory, the stages may overlap or be revisited. For example, a consumer who has received a diagnosis may experience each stage of the process only to find themself catapulted back to an earlier stage and assigned a new diagnosis. A new diagnosis has the effect of an unexpected reentrance and may occur at any stage of the process. A consumer’s previous experience gives them some familiarity with the process of being an outsider in the expert’s world but it does not change their outsider status.
The grounded theory Outsiders in the experts’ world explains the process that people experience when they unexpectedly enter the social world of health care and become health consumers. The theory emphasizes the outsider status of consumers in a context in which health professionals maintain their status as experts. The status of consumers as outsiders contradicts the central role that they are given in models of consumer-, patient-, and/or person-centered care. Key findings from this study relate to the culture shock that people experience when they unexpectedly enter the social world of health care and the social categorization of roles within that world that result in them having to learn a new role and establish a presence to receive tailored care.
Culture Shock
Consumers experience cognitive responses to the shock of a diagnosis (Anderson et al., 2010) and the shock of suddenly being subjected to an unfamiliar culture (Edwards Lenkeit, 2014). Within the socially constructed world of health care, people who willingly assume the role of experts provide care to those who unwillingly assume the role of consumers. Being a health consumer is not a role that people voluntarily choose. A diagnosis or recurrent symptoms engender a reality that thrusts people into the role.
Anthropologists use the term culture shock to describe feelings of disorientation, frustration, and helplessness that people encounter when they are subjected to an unfamiliar culture (Edwards Lenkeit, 2014). Culture shock involves two key processes: contact with or immersion in an unfamiliar culture and loss of familiar social roles, cues, and practices (Irwin, 2007; Oberg, 1960). The environment of health care is a microculture consisting of physical objects, ideas, beliefs, and institutional processes, which are unfamiliar to consumers (Edwards Lenkeit, 2014). In addition, technical terminology is used, which may be difficult for consumers to understand (Zeng-Treitler et al., 2008). When people unexpectedly enter this microculture, they leave behind their expectations of everyday life and take on a consumer role (Plummer, 2012).
Unexpectedly entering the social world of health care is akin to “taking a first trip to a foreign country” (Ramsden, 1980, p. 289). The difference being that a person taking a first trip to a foreign country is better prepared for their experience than a person making an unexpected entrance into the social world of health care. A trip to a foreign country is usually planned; departure and return dates are chosen; some knowledge of the language, norms, and culture of the country are acquired and travelers will have an idea of what their budget will allow in relation to accommodation and other expenses. Consumers do not have the luxury of preparing for their entrance into the social world of health care but instead make an unexpected entrance into a new social world where they need to learn a new role.
Classifying individuals into social groups is a process of social categorization (Abrams & Hogg, 1990) in which individuals not only categorize others but also consider whether others belong to their own “in-group, or to some other, out-group” (Ward et al., 2001, p. 9). In the seminal work The Social System, Parsons (1951) states that categorizing people as “being sick” is a social condition because it involves people entering into the socially constructed “sick” role. Consumers, however, do not collectively form a subculture around the role because the undesirable state of being sick is not a motivating factor for joining this group (Parsons, 1951).
Since Parson’s (1951) work, the number of people with diagnosed illness has increased and the concept of consumer support groups has developed. The experience of being socially categorized as being sick is not, therefore, necessarily as isolating as Parson infers. Some consumers in the study, particularly parents of children with disabilities, cultivate support by seeking out and connecting with consumers experiencing similar situations. Findings in the literature show that joining a support group enables consumers to identify with others through shared experiences (Doran & Hornibrook, 2013; Thompson et al., 2014) and diminishes thier initial feelings of culture shock. Interacting with others and/or being a member of a support group creates a sense of belonging that alleviates these consumers’ feelings of isolation and “normalizes” their situation. This form of normalization helps consumers to establish a presence in the social world of health care and in turn confront the dichotomy of “us” and “them” that exists between consumers and experts.
It is widely recognized that the relationship between consumers and experts is important for individuals’ health and the course of illness (Murtagh, 2009; Tsai et al., 2015). The relationship, however, is complex. Consumers are essentially nonvoluntary participants in a relationship in which consumers struggle to define and learn their role. Although consumers may not define their role in terms of a collective consumer group, the consumer role is “universal” because the institutional and social expectations and obligations placed on consumers are applied to all consumers regardless of demographics such as age, gender, occupation, ethnicity, or status in other spheres (Morgan, 1982; Parsons, 1951). This notion of universal expectations leads to consumers exerting their presence through strategies that include choosing a particular voice and establishing relationships with experts that have the potential to transcend professional boundaries in a crisis, or at the end of life.
Unlike the consumer role, the expert’s role is “collectivity-oriented not self-oriented” (Parsons, 1951, p. 434). Collectively, experts form a culture that comprises subcultures of experts from individual professions (e.g., medicine, nursing, psychology). Membership into these groups is a selective process, and education, professional qualifications, and social categorization legitimize roles. Experts learn, develop, and maintain their professional identities through formal education, experience in their role and consumers’ expectations of their role (Biddle, 1986; Broderick, 1998; Haslam, 2014). Experts are proficient in separating their professional and personal identities. Consumers, on the contrary, do not have the luxury of separating their identities. The manifestation of illness in the physical body is not separate to consumers’ other social identities; body and self are inextricably entwined. As consumers confront the dichotomy of “us” and “them,” they learn how to manage the collective professional boundaries traditional to the social world of health care. Managing these professional boundaries does not automatically result in consumers having license to transgress; however, they can learn how to push the boundaries to the point of receiving a level of tailored care that meets their needs.
Social Categorization of Roles
When illness becomes the foundation for socially categorizing consumers, individuals’ perceptions of self cognitively shift (Charles et al., 1997; Mozo-Dutton et al., 2012). A cognitive shift means accepting and integrating illness into one’s life and “liv[ing] illness fully” (Frank, 2002, p. 3). Consumers in this study demonstrate living illness fully as evidenced by their responses to emotional fluctuations and changing perceptions of self during the unexpected entrance phase of the consumer experience. In a study of the impact of multiple sclerosis on perceptions of self, Mozo-Dutton et al. (2012) found that the onset of illness changed study participants’ perceptions of their body. Similarly, in the study reported here, changing perceptions of self attest to consumers viewing their physical body differently after an unexpected entrance into the social world of health care. Some consumers are more circumspect, however, and their perceptions of their physical self do not match the ways in which others perceive them.
Although the onset of illness can change consumers’ perceptions of their body, this does not necessarily mean a loss of self (Mozo-Dutton et al., 2012). Rather elements of one’s former self can still be preserved and even enhanced through the experience of illness. This process is beautifully described in Ken Plummer’s (2012) account of his own illness in which he explains that although his body became a “thin body,” a “tired body,” an “encephalopathic body,” a “transformed body,” and a “new body,” he remained an “interactionist academic self.” Plummer’s preservation of self enabled him to reflect on, give meaning to, and write about his experience of illness.
Regardless of social categorizations associated with roles and illness, and changing perceptions of self, the quality of relations—at the interaction level—between consumers and experts is central to the delivery of health care. The delivery of health care is an interpersonal process (Soklaridis et al., 2016). Until the early 1970s, the traditional paternalistic model of health care dominated the “doctor–patient” relationship in Western health care systems. Within this model, the relationship is characterized by a dominant doctor interacting with a passive patient (Kaba & Sooriakumaran, 2007; Pilnick & Dingwall, 2011). Doctors act as consumer guardians and use their skills to determine the patient’s condition and to prescribe tests and treatments that they consider best for the patient, who passively consents (Ha & Longnecker, 2010). While some emergency situations may still justify the use of this model, health care models have since evolved to incorporate other health professionals and the role of consumers as active participants in their health (Janamian et al., 2016; Kaba & Sooriakumaran, 2007). Under evolved models of care, a range of experts, including nurses, psychologists, and allied health professionals, are now instrumental in delivering health care (Bury, 2004) and the traditional paternalistic doctor–patient relationship has, in theory, transitioned to a partnering relationship, which is patient-, person-, consumer-, or relationship-centered (Duggan & Thompson, 2011; Soklaridis et al., 2016). However, while findings in this study evidence these changes, the findings also highlight that achieving access to tailored care is not an easy process for consumers to engage in nor is it without challenges.
Current health policy attempts to bridge dichotomies between consumer outsiders and expert insiders by introducing strategies and models of care that seek to place consumers and their families at the center of care and to empower and support them to participate in their own health and health care (ACSQHC, 2011a; Mastro et al., 2014). Risk reduction is a key impetus for introducing such policies. Reducing the risk of adverse events and increasing consumer safety within the context of health care is a win-win for both consumers and experts and the health systems within which they interact. However, while a risk reduction approach is necessary, approaches are largely policy driven and generally fail to consider what consumers really need and want from experts.
Dichotomies fundamentally result from contradictory sets of underlying assumptions. Health systems are based on risk management and economic assumptions that favor transactional not relational interactions. Risk management strategies include evidence-based practices that are underpinned by positivist scientific knowledge, which favor a biomedical approach to interactions between experts and consumers. In contrast, consumer-centered approaches are based on biopsychosocial perspectives that combine ethical values, consumers’ preferences, psychotherapeutic theories, and negotiation theories (Bensing, 2000; Jensen et al., 2013). Economic imperatives to achieve more with less impose structures that reward experts and health service providers for quantity of interactions over quality of interactions. Although the importance of the quality of interactions between consumers and experts is recognized, it is often measured through quantitative means.
It is not all doom and gloom; however, there is a shift afoot. Current trends in research suggest that the human qualitative aspect of health is gaining momentum, particularly at the consumer–expert interaction level (The Beryl Institute, 2019; Brach, 2014; Johna & Rahman, 2011) and that consumers are participating in their health care (Entwistle, 2009; Rocque et al., 2019; Röing & Holmström, 2012). However, progress toward empowered individuals who are in control of their health and health care is slow (Foot et al., 2014) and care that is truly consumer-centered is currently the exception not the rule (Brach, 2014). Bridging dichotomies that exist between outsiders and insiders means acknowledging consumers’ and experts’ differing perspectives, knowledge, skills, needs, and desires in the process of improving consumers’ experience of health care.
Study Strengths and Limitations
A key strength of this study is the sample size and the variation and scope of the data set. Data were collected and generated from 32 participants representing 23 consumers and nine experts. The scope of the data set includes data collected and generated via a range of methods. Data generation/collection method and quantity of data by participant type are presented in Table 1. In addition, the lead author’s commitment to the essential grounded theory method of memo writing resulted in a “bank” of 120 memos. Having access to that quantity of decision-making records and thought patterns over the course of the study supported the development of the grounded theory.
Another key strength of this study is the potential transferability of the findings. The grounded theory Outsiders in the experts’ world is theoretically applicable across all health sectors and is transferable to other contexts in which consumers unexpectedly enter experts’ social worlds, for example, the justice system or the welfare system. The scope of this study does not provide the opportunity to extend the theory over and above the substantive area of the social world of health care. The applicability of a formal grounded theory to broader environments has not, therefore, been substantiated.
No serious flaws limited the study. It is noted, however, that data were collected from consumers and experts in one Australian regional city only. Also, information obtained from demographic questionnaires was incomplete. Five consumers and three experts did not complete demographic questionnaires. These participants were observed interacting with experts and consumers, respectively, and were given a study information sheet and provided consent prior to observation sessions being conducted. The lack of demographic data relating to these participants did not affect the quality of the grounded theory but would have provided additional information relating to variation in the total sample.
Conclusion
The grounded theory Outsiders in the experts’ world explains the process of interaction between consumers and experts across the continuum from consumers’ unexpected entrance into the social world of health care to receiving tailored care (Chamberlain-Salaun, 2015). As outsiders, consumers have to navigate and negotiate their way in the social world of health care to access required information and receive care that is tailored to their needs. Within this social world, consumers and experts act and interact in health care discourses and make meaning of their experiences.
Consumer-centered health care has strong policy support. Yet, the findings from this study establish that for participants, consumer-centered care is the exception not the norm. Understanding consumers’ needs and their perceptions and meaning making of interactions with experts is valuable. The theory contributes to understandings and knowledge of what it means to be a consumer of health care—not a consumer who is categorized according to their illness or condition, or by the setting in which they receive care or according to the specific health professionals with whom they interact. Gaining insight into the substantive area of inquiry enables improved efficiencies in the delivery and quality of health care. Importantly, gaining insight into consumers’ experience of interacting with experts also provides a foundation for considering relationships and ways of interacting between consumers and experts that acknowledges and respects each other’s humanness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.