
Abstract
This study determined the status and outcomes of bioterrorism-related training programs for healthcare workers. While media-based education/training uses simulations, games, and web-based programs, evidence of their effectiveness and relevant systematic reviews remain scarce. This systematic review focused on articles published in PubMed, EMBASE, CINAHL, PsycINFO, Cochrane Library, and Research Information Sharing Service between January 1, 1990 and September 17, 2023. Among 2,592 identified articles, literature quality was assessed in 12 articles. In the most articles, bioterrorism-related knowledge and problem-solving ability significantly increased following interventions. However, quality assessment results provided insufficient evidence regarding improvement in healthcare workers’ preparedness to face bioterrorism after undergoing bioterrorism-related training programs. Developing easily accessible and regularly implemented bioterrorism training programs for healthcare workers could enhance their preparedness toward terrorism and provide high-quality evidence for effective bioterrorism responses.
Background
Since the anthrax bioterrorism incident that occurred in the United States (US) in September 2001, fear and awareness of bioterrorism have increased globally. Bioterrorism refers to an act intended to cause potential social disruption by causing death or disease to humans, animals, or plants using microorganisms or toxins derived from living organisms (National Center for Emerging and Zoonotic Infectious Diseases, 2020). The production, concealment, transportation, and dispensing of bioterrorism agents are easy; bioterrorism detection is difficult and takes time owing to the incubation period (Jansen et al., 2014). Moreover, bioterrorism can cause extensive damage by spreading beyond the original attack site, thereby causing secondary and tertiary infections. Failure to promptly respond in the early stage could instantly paralyze the public health system (Jansen et al., 2014). Therefore, bioterrorism is a significant national security issue that requires a predetermined emergency response system.
The most significant aspects of a bioterrorism response system are early detection, diagnosis, and prevention of the spread of the agent (O’Brien et al., 2021). Healthcare providers should accurately recognize bioterrorism-related signs and symptoms, including acute rash syndrome, acute neuropathy syndrome, acute hemorrhagic fever syndrome, and acute respiratory syndrome; conduct multiple detection kit tests; report positive results to authorities; and should isolate infected patients and initiate antimicrobial treatment to limit the spread of infection as much as possible (Centers for Disease Control and Prevention, 2020). Healthcare workers should possess competencies that allow them to accurately understand and quickly respond to bioterrorism. Therefore, enhancing bioterrorism response competencies professionally and systematically through constant training and education based on real-life situations is necessary.
Several resources for preparation and planning for bioterrorism emergencies are supplied by the US Centers for Disease Control and Prevention. This includes educational videos on Category A diseases (smallpox, anthrax, botulism, plague, tularemia, and viral hemorrhagic fevers) that have high potential for use as bioterrorist weapons (Center for Preparedness and Response, 2018). However, healthcare workers have been found to have low competencies regarding bioterrorism-related knowledge and response; moreover, a significant number of them have no bioterrorism training experience (Adithya Teja Prasad et al., 2020; Nofal et al., 2021). The Biological Weapons Convention was adopted by the United Nations General Assembly on December 16, 1971, and the development, production, and stockpiling of biological and toxin weapons are prohibited and obliged to be destroyed (United Nations, 2022). Currently, the Biological Weapons Convention has 185 States parties and four signatory states, whereas 10 countries have neither signed nor acceded to it (United Nations, 2022). The Korean government has established a bioterrorism countermeasure team, a response system and guidelines for each response stage, and implemented a mock drill centered on local governments (Korea Disease Control and Prevention Agency, 2021). However, North Korea did not sign the Convention, and South Korea faces massive threats of chemical, biological, radiological, nuclear, and high-yield explosive terrorism in the context of a divided Korea (Chun et al., 2012). Accordingly, investigating the status and effects of bioterrorism-related training programs for healthcare workers and establishing strategies for strengthening bioterrorism response competencies are necessary.
Previous studies on bioterrorism-related training programs for healthcare workers showed that online lectures have been developed in Korea; some local governments have been conducting their own bioterrorism response training (Park & Choi, 2020). However, as the existing literature reports lack such evidence, the effectiveness of these training programs needs to be reviewed (Park & Choi, 2020). Reviewing previous foreign studies showed that personal protective equipment simulation trainings were conducted for healthcare workers in Saudi Arabia (Abualenain & Al-Alawi, 2018); bioterrorism game simulations were conducted in the US for university students and nurses (Olson et al., 2010); and a web-based program was conducted in the US for physicians (Cosgrove et al., 2005), medical students (Silenas et al., 2008), and nurses (Nyamathi et al., 2010). For medical students and internal medicine interns, education and training programs through screen savers were implemented (Terndrup et al., 2005). However, evidence of their effectiveness and relevant systematic reviews are scarce. This review aimed to (i) examine the level of evidence in bioterrorism-related education studies and (ii) identify the characteristics and major outcomes of these studies. The review question is: What are the characteristics and major outcomes of bioterrorism-related training programs for healthcare workers? Hopefully, this review will provide an initial data source to aid future developments of effective training programs.
Material and Methods
Search Strategy and Selection Criteria
This is a systematic review study that aims to identify the characteristics and major outcomes of bioterrorism-related training programs for healthcare workers. The article search and selection process adhered to the systematic review protocol of Preferred Reporting Items of Systematic Reviews and Meta-Analysis (Moher et al., 2015) and Cochrane Collaboration’s guidelines for systematic reviews of interventions (Higgins & Green, 2011). Ethical approval exemption was obtained from the Institutional Review Board at Kyungpook National University (KNU-2020-0122). All methods were performed following the Declaration of Helsinki. In September 2020, before conducting the actual literature search, a brief search of the PubMed database was conducted to inform the search strategy. Based on the articles found, key questions were identified using the population, intervention, comparator, and outcome (PICO) framework. Keywords for each database were selected, and a search strategy using MeSH was established.
Articles were selected on the basis of the PICO–SD criteria, where SD stands for study design. The control group as comparator included those who did not receive any intervention. A comparator or control method is the preferred means of detecting disease states when the PICO framework is used in diagnostic studies. The following were the inclusion criteria: studies where participants consisted of healthcare workers, including doctors, nurses, emergency medical technicians, and students in medical/nursing/emergency medical technician fields, and studies that used bioterrorism training as an experimental intervention. Outcome variables included those indicating post-intervention effects, including knowledge, self-efficacy, problem-solving, performance, skill, ability, preparedness, satisfaction, effectiveness, and teamwork. Regarding study design, randomized controlled trials (RCTs) and quasi-experimental studies were selected. This review was limited to articles that were written in Korean or English. Therefore, all articles published in other languages were excluded from this review. Furthermore, the following articles were removed from this review: those published before 1990, dissertations, and conference papers.
Two researchers independently searched for and selected the articles in June and August 2021 and searched using the same method for an update in September 2023. The researcher teaches nursing microbiology, including bioterrorism-related contents in the undergraduate course, and has conducted special lectures and researches on bioterrorism-related healthcare providers’ preparedness. Bioterrorist threat response-related studies emerged in publications from the 1990s, mostly from the US (Kim, 2003). Therefore, the final search criterion for the publication period of articles was from January 1, 1990, to September 17, 2023. According to the Core Standard Ideal (COSI) search protocol (Bidwell, 2000), we searched for a suitable database. Based on the selection and exclusion criteria, articles written in English were retrieved from the following five databases that were commonly used in the healthcare field based on previous systematic review studies (Hanskamp-Sebregts et al., 2016; Witjes et al., 2019): PubMed, EMBASE, CINAHL, PsycINFO, and Cochrane Library. Articles published in Korea included those found in the Research Information Sharing Service. Search results from Google further revealed articles that were used in this study. The final literature search before the review was performed on September 18, 2023. Two researchers independently performed all study procedures, including the selection or exclusion of articles, data extraction, and analysis. Resolution was achieved through discussions until consensus was reached in case of disagreements. Analysis methods and inclusion criteria were not registered in PROSPERO. The complete search strategy for each database is presented in the Supplementary Material 1.
Data Extraction and Analysis
We identified 2,592 articles, including 2,584 articles from database searches and 8 additional articles from manual searches. Following manually removing duplicates, two researchers reviewed the titles and abstracts of 2,258 articles and subsequently excluded 2,236 articles. After reviewing the full text of the remaining 22 articles, 12 were included in the systematic review. The others were excluded for the following reasons: non-experimental studies (n = 2), studies not related to bioterrorism (n = 3), non-comparative studies (n = 3), duplicated dataset (n = 1), and qualitative research (n = 1; Figure 1).

Flowchart diagram of data extraction and analysis.
Data Analysis
Of nine selected studies, two were RCTs and seven were non-randomized studies. For literature quality assessment, the revised Cochrane risk of bias tool for randomized trials (RoB 2) was used for RCTs, and the risk of bias in non-randomized studies of interventions (ROBINS-I) version 2.0 was used for non-randomized studies (Higgins & Green, 2011). Two researchers independently performed quality assessment, following which their findings were combined. In case of disagreement between the researchers, consensus was reached through a discussion. Quality assessment results were presented using RevMan 5.0 version (Cochrane Community, Oxford, UK).
RoB 2 was used for assessing the risk of bias in terms of the following five items: “randomization process,”“deviations from intended interventions,”“missing outcome data,”“measurement of the outcome,” and “selection of the reported result.” ROBINS-I was used for assessing the risk of bias in terms of the following seven items: “bias due to confounding,”“bias in the selection of participants into the study,”“bias in the classification of interventions,”“bias due to deviations from intended interventions,”“bias due to missing data,”“bias in outcome measurements,” and “bias in the selection of the reported result.” RoB 2 and ROBINS-I are tools that assess each item’s risk of bias using five response options (“Yes,”“Probably yes,”“No,”“Probably no,” and “No information”). In RoB 2, the risk of bias for each domain was rated as low, some concerns, or high, according to the assessment algorithm for each domain. Meanwhile, in ROBINS-I, the risk of bias was rated as low, moderate, serious, critical, or no information.
This study used a qualitative approach to analyze the data. As the selected articles applied different types of intervention programs, and the study design and measurements were heterogeneous, meta-analysis was not performed. For data extraction, one researcher drafted the basic format, and the final format was established following a discussion between the researchers. Data were summarized by dividing them according to the country of study, participants, study design, follow-up period, duration and frequency of intervention, measurement tools, and study findings (Table 1). After one researcher organized the data, another researcher reviewed the original text to re-screen the compiled data.
Characteristics of Studies Included in the Systematic Review (N = 12).

Results
Of twelve articles included in the final analysis, seven were published between 2004 and 2010, and there was five article each from 2018 and 2023. Regarding the country of study, eight studies were from the US, two studies were from Iran, and there was one study each from Saudi Arabia, and Turkey. Five RCTs and seven non-randomized studies were noted (two with a control group and five with a solitary group pre–post design). Participants in five, four, and three studies included only medical students or doctors, only nurses or nursing students, and various healthcare workers, respectively. Regarding sample size, two, five, and five studies with sample sizes of ≤40, 41–<100, and ≥100, respectively, were observed; meanwhile, only four studies conducted follow-up tests.
Experimental interventions included web-based education (n = 4), simulations (n = 3), game simulations (n = 1), problem-based learning (n = 1), tabletop exercises (n = 1), and lectures and pamphlets (n = 2). Seven studies implemented their interventions in groups, and five opted to conduct them individually; moreover, seven and five studies implemented offline and online interventions, respectively. The duration of interventions was ≤2 day and 3 weeks in eight and one studies, respectively; it was ≤1 month, 11 months, and unspecified for the three remaining studies, respectively. Post-intervention outcome variables included bioterrorism-related knowledge (n = 8), skill or performance (n = 4), bioterrorism response attitudes (n = 3), self-efficacy or confidence (n = 2), and personal protective equipment donning and doffing checklists (n = 1). Ten studies reported a significant increase in knowledge or problem-solving ability in post-intervention outcomes compared with the control or pre-test results. In contrast, two study reported no significant difference in knowledge compared with the control (Table 1).
RoB 2 was used to assess the quality of the five RCTs. In the study by Chung et al. (2004), four domains were determined to have a low risk of bias. However, as the intervention outcome assessor had not been blinded to the intervention, the “measurement of the outcome” domain was determined to have a high risk of bias. The assessment had likely been affected by the knowledge about the intervention. Therefore, since one or more domains were noted with a high risk of bias, the final overall risk of bias was determined to be high. According to Nyamathi et al. (2010), the “selection of the reported result” domain was assessed to have a low risk of bias. While sociodemographic variables were investigated, there was no mention or adjustment of baseline homogeneity. Consequently, the “randomization process” domain was assessed as having some concerns. Moreover, owing to the higher dropout rate in the experimental group compared with that in the control group, and participants were not blinded to the intervention when reporting the results, the “deviations from the intended interventions,”“missing outcome data,” and “measurement of the outcome” domains were determined to have a high risk of bias. Consequently, the final overall risk of bias was also assessed as high. In the study by Tobin et al. (2020) and Huyar and Esin (2023), all domains were determined to have a low risk of bias, and the final overall risk of bias was also assessed as low. In the study by Ghahremani et al. (2022), four domains were evaluated as low risk and “randomization process” domain was assessed as having some concerns. While there was a significant baseline difference between the two groups in the pre-test, statistical adjustment for this was not accomplished. Consequently, the final overall risk of bias was some concerns (Figure 2).

Risk of bias in randomized controlled trials.
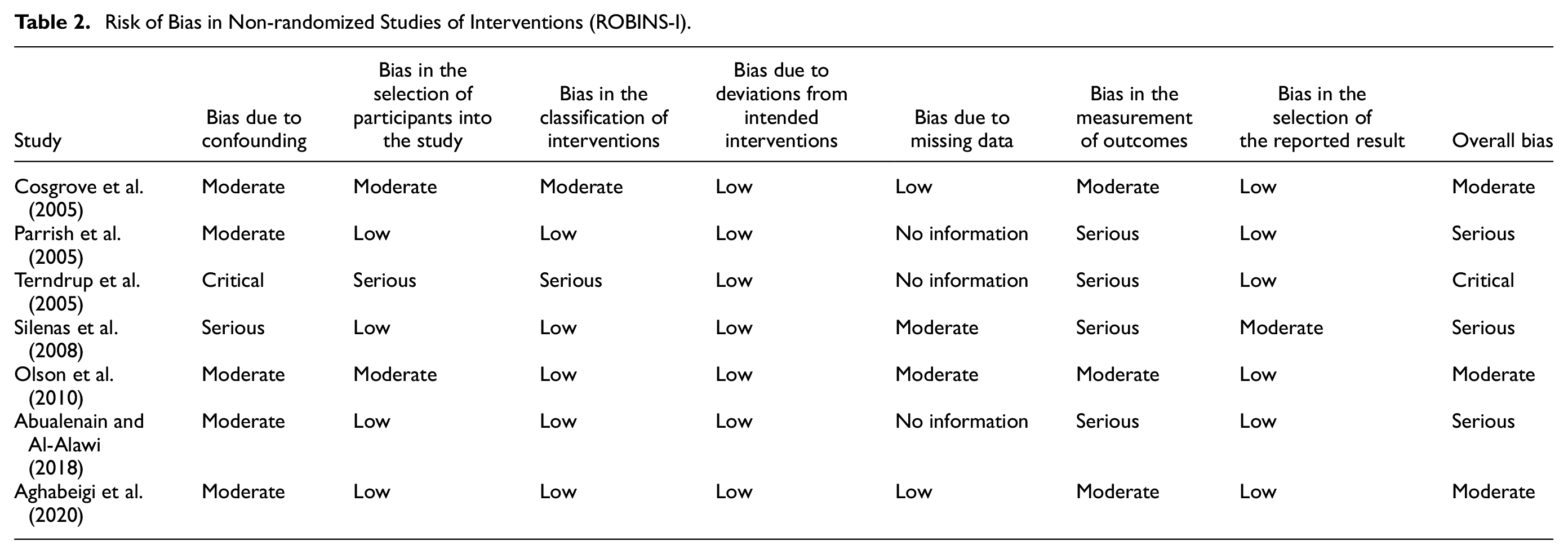
ROBINS-I was used to assess the quality of the seven non-randomized studies. As no domain with a serious risk of bias was noted, the overall risk of bias in three studies (Aghabeigi et al., 2020; Cosgrove et al., 2005; Olson et al., 2010) was determined to be moderate. In three other studies (Abualenain & Al-Alawi, 2018; Parrish et al., 2005; Silenas et al., 2008), most participants directly reported intervention outcomes; thus, no assessor was blinded. Accordingly, the “bias in the measurement of outcomes” domain and the final overall risk of bias were determined to be serious. In another study (Terndrup et al., 2005), no assessor blinding or correction related to participant selection was observed, and participants started the intervention at different time points; thus, its findings could not be used as reliable evidence of interventional effects. Thus, the final overall risk of bias was determined to be critical (Table 2).
Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I).
Discussion
This study aimed to identify the status and effects of bioterrorism-related training programs for healthcare workers. Twelve studies were selected, highlighting the scarcity of interventional studies on bioterrorism response training programs for healthcare workers. Of these 12 studies, 7 were published between 2004 and 2010 and conducted in the US. Potentially, owing to the anthrax terror attacks that occurred in the US in September 2001, the studies were concentrated in specific periods and countries. Subsequently, this became the impetus for bioterrorism-related studies. While previous studies were concentrated in the United States, studies conducted around 2020 were conducted in several countries, including the Iran (2), Saudi Arabia (1), Turkey (1), and US (1).
Of the seven studies conducted through 2010, five studies had doctors or medical students as participants, indicating that among different types of healthcare workers, the highest number of interventional studies focused on doctors. However, recently, the number of studies targeting nurses or nursing students has increased. Existing studies on healthcare workers, including doctors and nurses, have reported poor knowledge of bioterrorism response among participants (De Felice et al., 2008; Katz et al., 2006; Kerby et al., 2005; Rebmann & Mohr, 2010), which is almost similar to the findings of a recent study (Nofal et al., 2021). While healthcare workers mainly agree about the need for bioterrorism preparedness education or training, they rarely participated in relevant education or training programs (Katz et al., 2006; Nofal et al., 2021; Rebmann & Mohr, 2010). The bioterrorism preparedness competencies of healthcare workers varied according to workplace, department, profession, education level, and prior bioterrorism preparedness training (Nofal et al., 2021). Katz et al. (2006) supported these findings by stating that a significant difference was observed in performance according to the profession, work experience, education level, and prior training. Therefore, to increase the level of preparedness for bioterrorism among healthcare workers, it is necessary to develop practical training programs that help strengthen their competencies by considering previous work experience and educational attainment, as well as the specialty of each job type.
Among the non-RCTs that were included in this review, two studies used a control group pre–post design, and five studies used a single group pre–post design with no control group. Although adopting such a study design could lower the level of evidence, the implementation of any intervention program for healthcare workers requires active cooperation from the institution. Moreover, owing to the possibility of Hawthorne effects within the institution, conducting an RCT may be challenging (Abualenain & Al-Alawi, 2018). However, future studies should be better designed to obtain high-quality evidence to help identify the effects of bioterrorism training programs and ensure the generalizability of the findings. The 12 studies in the review analyzed various forms of bioterrorism training programs, including web-based education, simulations, game simulations, problem-based learning, tabletop exercises, lectures, and pamphlets. Experimental interventions were very diverse in terms of focus (individual vs. group), format (online vs. offline), duration (within 1 h to 11 months), and type. Owing to several intervention methods across different studies, comprehensively explaining or generalizing them is challenging. However, of note, bioterrorism training programs have occurred in such a large variety, and their effects have been assessed.
An analysis of the implications for future studies based on the strengths and weaknesses of applied training programs and assessment methods showed the following among the various articles. Terndrup et al. (2005) developed a screensaver and website containing detailed information regarding bioterrorism. The intervention was applied to fourth-year medical students and interns, and the effects of the intervention were analyzed. The intervention method, which allows the use of a screensaver and relevant website, when necessary, is considered efficient and effective. However, this study implemented the intervention between March 2001 and January 2004, which is a period before and after the 9/11 terror attack in the US. Therefore, bias may have been introduced in the assessment and interpretation of intervention effects.
Concerning medical students and interns in medical training, those who participated in the study during the latter part of their training, rather than the initial phase, may have had learning opportunities through other training programs. Therefore, the problem of participant maturation during the study cannot be disregarded. Moreover, an RCT by Chung et al. (2004) provided an educational website; however, the intervention did not enhance the knowledge of emergency department doctors. Particularly, most of the participants assessed that their knowledge of bioterrorism was inadequate following the intervention. Merely providing healthcare workers with access to educational websites may be insufficient to effectively enhance relevant knowledge and develop their competencies to respond to future bioterrorist attacks. The participants in the aforementioned intervention may have lacked the motivation to use the website because only few opportunities to encounter diseases caused by biological agents were presented (Chung et al., 2004). Therefore, ensuring that healthcare workers first understand and recognize the need for the development of bioterrorism response competencies is significant. Thus, the competency level should not be rated only by knowledge assessment. Training programs that consider various aspects of competencies, including awareness and attitudes, should be developed.
Tobin et al. (2020) reported that web-based or web-enhanced programs had greater effects on education than conventional offline lectures and were more effective when they included interactive elements. In particular, since it shows the effectiveness of online simulation as an educational program for novice trainers, it can also be considered an educational method to train novice trainers efficiently. Olson et al. (2010) demonstrated that training through game simulations was significantly associated with better performance. Cosgrove et al. (2005) highlighted that not measuring long-term knowledge retention was a study limitation and emphasized that repeated and frequent education methods for strengthening the knowledge of healthcare workers are one of the advantages of Internet-based modules. Moreover, improved scores among intervention participants could be attributed to computer skills (Nyamathi et al., 2010). Individuals who possess greater computer skills were more likely to demonstrate greater acceptance of Internet-based programs and recognize such content to be useful (Creedy et al., 2007). The coronavirus disease 2019 (COVID-19) has led to the Fourth Industrial Revolution based on 5G network acceleration (Baek et al., 2020). The changing times have ushered in the age of full-fledged remote learning (Baek et al., 2020; Kumar et al., 2021). This is significant as healthcare workers or college students, who are born between the late 1990s and early 2000s and are commonly referred to as “Zoomers” or “Generation Z,” represent a digitally native generation (Merriam-Webster, 2021); therefore, the active use of web-based training programs with interactive elements should be considered. Healthcare workers have indicated that the scarcity of information about available programs and the lack of easily accessible programs are barriers to bioterrorism education (Nofal et al., 2021). Therefore, developing programs with better accessibility that promote healthcare worker participation and provide relevant program-related information is significant. However, regarding the lack of educational motivation, attaining the benefits of training programs would be challenging if only a website is provided (Chung et al., 2004). Thus, motivation-enhancing strategies that can promote active participation in training should also be prioritized.
Of the 12 studies, most evaluated pre- and post-intervention outcomes, and six performed follow-up tests. Nyamathi et al. (2010) highlighted the need for the assessment of long-term effects, as retaining the effects of such training programs is significant for healthcare workers to build competencies to effectively prepare for bioterrorism. Although bioterrorism is a highly rare and unique situation, it can be fatal when prompt accurate diagnoses and treatments are not implemented. Therefore, having a continuous training system that enables the demonstration of trainees’ competencies at any time before an actual situation occurs is imperative. Thus, while developing training programs for healthcare workers, one should consider not only the enhancement of competencies immediately following training but also strategies for continued retention of the developed competencies. Moreover, developing training programs that help gain competencies through practice in real-life situations, as opposed to mere knowledge acquisition, would be ideal.
Ensuring an effective educational system for undergraduate programs to prepare future healthcare workers for bioterrorism is essential. In modern society, disaster response education for healthcare professionals is significant (Parrish et al., 2005). As diverse and complex problems stemming from a disaster cannot be managed by specific expertise, the basic contents of the educational curriculum for disaster response should comprehensively include various fields, including medicine, public health, and health policy. Further, an educational system focusing on merely acquiring knowledge regarding responses to unavoidable disasters should be transformed into one that improves clinical competencies. In this regard, Silenas et al. (2008) highlighted the significance of having faculty members who can train other healthcare workers. Faculty members who have in-depth knowledge of multi-disciplinary integrative disease responses are lacking, whereas the need to develop competencies of instructors who can provide effective disaster response education has not received much attention. Therefore, ensuring that healthcare faculty members provide practical disaster response education while training healthcare workers in their specialty fields is necessary. In addition, recent RCT studies (Huyar & Esin, 2023; Tobin et al., 2020) have shown that simulation-based education is widely implemented and has high educational effectiveness. It is necessary for healthcare workers to have sufficient experience through simulation training for disasters such as bioterrorism, which have a low probability of occurrence but have a high risk.
Intervention effects were assessed on the basis of bioterrorism-related knowledge and problem-solving skills. Significant increases in these outcome variables were observed in most studies. However, quality assessment results indicated that the level of evidence that bioterrorism training programs can enhance the bioterrorism response competencies of healthcare workers is inconsistent and low. However, it is encouraging that the recent studies are RCTs, and their risk of bias was also evaluated as low. The bioterrorism response competencies of healthcare workers were not clearly defined. To measure the major outcome variables, several studies used self-developed tools or checklists. Studies that used tools or assessment methods with proven reliability and validity were minimal. Bioterrorism response competencies were expressed as disaster response competencies (Silenas et al., 2008), knowledge and attitudes concerning disaster responses (Parrish et al., 2005), and bioterrorism and emergency readiness (Olson et al., 2010). However, the bioterrorism response competencies that healthcare workers should possess were not clearly defined; most studies assessed the level and enhancement of such competencies based on the knowledge level of participants. To investigate the bioterrorism preparedness of healthcare workers or the general population, a tool developed by Katz et al. (2006) has been used in various studies (Nofal et al., 2021); however, the tool only made use of knowledge-based questions (Katz et al., 2006). Therefore, it is necessary to clearly define bioterrorism preparedness competencies and develop tools that enable objective measurements and comparisons to properly assess the bioterrorism preparedness competencies of healthcare workers and develop training programs that will enhance such competencies.
Implications
While several healthcare workers agree that bioterrorism preparedness education or training is necessary, they have yet to have much experience participating in related education or training programs. Considering the need for knowledge of healthcare workers on bioterrorism preparedness in previous studies, developing and applying various educational programs for improving bioterrorism preparedness-related competencies is necessary. However, it should be considered to improve not just knowledge but also various contents and methods for strengthening competencies. There have been few studies on the development and effectiveness evaluation of bioterrorism-related training programs; therefore, conducting studies to develop interventions and verify their effects is significant. As previously discussed, the key is to develop effective intervention programs for healthcare workers by fully considering the strengths and weaknesses of existing programs. Conducting these additional studies will increase the level of evidence.
Limitations
This study had some limitations. First, because the training modes applied in each study and the assessment of the effects of such training varied between studies, a meta-analysis could not be performed; therefore, a quantitative synthesis of the training effect was not possible. While articles with a high risk of bias were excluded from the analysis based on quality assessment results, the included articles exhibited bias in assessing the effects of the intervention. Therefore, there are limitations to generalizing the findings. Second, the studies were conducted in a few countries, thereby limiting global generalizability. Lastly, high-quality RCTs targeting healthcare workers were still lacking, and some non-RCTs had some risk of bias. Thus, when interpreting the effects of the interventions, caution is needed. Despite these limitations, this is the first study to identify the status of the development and implementation of bioterrorism-related intervention programs. Moreover, the study presents future research directions by confirming that the previously developed programs were not evidence-based; they did not consider causal factors, instead, focused on personal factors.
Conclusion
While bioterrorism is a low-likelihood event, a lack of preparedness could cause irreversible damage and loss. The COVID-19 pandemic has completely altered daily life, causing countless deaths, and has revealed the limitations of the current healthcare system in handling such a crisis. Individuals increasingly realize the significance of disaster preparedness competencies. This study confirmed that interventional studies on enhancing the competencies of healthcare workers for bioterrorism response have been consistently conducted. However, several inadequacies in the content or delivery mode of training programs and competency assessment methods are noted. This indicates the need for future studies focused on delivering a higher level of evidence. Bioterrorism training programs that are easily accessible and available at any time and educational methods that allow knowledge to be applied in actual situations through appropriate interactions and simulations of bioterrorism scenarios could be effective in strengthening the bioterrorism-related competencies of healthcare workers. Additionally, to improve the disaster response competencies of healthcare workers, thereby leading to stronger national crisis response competencies. government support and interest are needed.
Supplemental Material
sj-xlsx-1-sgo-10.1177_21582440231211373 – Supplemental material for Bioterrorism-Related Training Programs for Healthcare Workers: A Systematic Review
Supplemental material, sj-xlsx-1-sgo-10.1177_21582440231211373 for Bioterrorism-Related Training Programs for Healthcare Workers: A Systematic Review by Yujeong Kim and Haeyoung Lee in SAGE Open
Footnotes
Author Contributions
Study design: Y Kim, H Lee
Data collection: Y Kim, H Lee
Data analysis: Y Kim, H Lee
Manuscript writing: Y Kim, H Lee
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), which is funded by the Ministry of Education [grant number NRF-2020R1I1A3068740].
Ethical Approval
Ethical approval exemption was obtained from the institutional review board at Kyungpook National University (KNU-2020-0122).
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.